
Abstract
Keywords
Introduction
Pediatric healthcare design has shifted from a focus on functionality toward a more holistic approach that prioritizes the well-being of young patients and their families. The physical environment plays a critical role in shaping health outcomes, with evidence demonstrating that well-designed spaces—incorporating natural light, calming colors, and access to nature—can reduce stress, improve clinical outcomes, and shorten hospital stays (Acosta et al., 2017; Bevan et al., 2019; Felippe et al., 2017; Fricke et al., 2019; Nourmusavi Nasab et al., 2020). This evolution reflects broader trends emphasizing patient- and family-centered care, particularly in pediatric settings, where family engagement is fundamental to the healing process (Flynn et al., 2019; Hill et al., 2018; Williams et al., 2021).
In recent years, design strategies for pediatric healthcare have emphasized creating adaptable, patient-centered spaces that integrate therapeutic elements to enhance engagement and comfort (Bogaert, 2022; Kim, 2023; Payam et al., 2023; Seniwati et al., 2023; Smith, 2018; Vollmer & Koppen, 2021). Biophilic and sustainable principles, incorporating natural materials, greenery, and daylight, have been shown to promote psychological and physiological well-being (Kellert et al., 2011). Concurrently, emerging technologies such as virtual reality (VR) and artificial intelligence (AI) are transforming healthcare design by enabling immersive visualizations, therapeutic applications, and operational efficiencies (Bailey & Bailenson, 2017; Eijlers et al., 2019; Pallavicini & Bouchard, 2019; Topol, 2019). Biometrics, capturing physiological and emotional responses to environmental stimuli, provides data-driven insights for design strategies (Bower et al., 2019; Kim & Kim, 2022; Valentine, 2024). Despite the potential, these technologies pose challenges related to privacy, ethics, and cost (Chen et al., 2020; Montreuil et al., 2021).
Systemic barriers, such as infection control requirements and operational inefficiencies, also limit the implementation of patient-centered and participatory approaches in healthcare design (Montreuil et al., 2021; Sathyanarayanan & Caldas, 2022). Participatory Design, also known as User-Centered Design or Co-Design, is a collaborative approach that involves stakeholders—including patients, families, and healthcare professionals—in decision-making processes (Robertson & Simonsen, 2012). By incorporating user perspectives, this method ensures spaces address functional, emotional, and cultural needs. In pediatric healthcare, participatory approaches can create environments that reflect the unique needs of children and their families, fostering engagement and well-being.
Designing for neurodivergent children and those with behavioral health challenges requires sensory-friendly, inclusive environments (Williams et al., 2023). Spaces must accommodate diverse needs while fostering comfort and belonging, incorporating design elements such as noise control, tactile-friendly surfaces, and biophilic features to reduce stress and promote recovery (Higuera-Trujillo et al., 2020; Lauwers et al., 2024). Addressing these multifaceted demands requires interdisciplinary collaboration among designers, clinicians, and patient advocates. Culturally sensitive features—such as multilingual signage, storytelling spaces, and family-oriented areas—can further enhance the patient experience (Kaihlanen et al., 2019).
This study explores how pediatric healthcare design can address these challenges and leverage emerging technologies to advance patient outcomes and family engagement. By synthesizing insights from experts, the research aims to fill critical knowledge gaps and provide actionable recommendations for the creation of adaptable, inclusive, and technologically integrated healthcare spaces. Specifically, the study addresses the following research questions:
How do experts describe current trends and the evolution of patient-centered care in pediatric healthcare environments? What barriers do professionals identify in implementing patient-centered and participatory design strategies in pediatric healthcare environments? How are emerging technologies, particularly immersive technologies, being utilized in the design process for pediatric healthcare environments, and what impacts do experts anticipate from their integration? What are the anticipated future directions for pediatric healthcare environments, and how are these expected to influence design practices and enhance patient and family engagement?
Methods
This qualitative study explored expert perspectives on trends, barriers, and opportunities in pediatric healthcare design using purposive and snowball sampling (Palinkas et al., 2015). Participants were selected based on direct experience in designing, managing, or researching pediatric healthcare environments. This phase focused on expert insights, with complementary studies addressing patient and caregiver perspectives to ensure a comprehensive research framework.
Fifteen experts were recruited based on their recognized expertise and direct experience in pediatric healthcare design. Five others did not respond to the invitation, an architect specializing in pediatric healthcare design, design researchers, and a healthcare owner. Physicians were initially considered, but were excluded due to scheduling challenges and limited availability during the COVID-19 period. Selection criteria prioritized diverse professional roles, including pediatric nurses, architects, healthcare administrators, child life specialists, psychologists, and researchers, with substantial experience in practice, research, or policy. Participants were identified through analysis of published works, professional networking platforms such as LinkedIn, direct outreach via email, and observations from industry webinars and conference presentations. Snowball sampling was subsequently employed to expand participation and capture a wider range of perspectives. No prior professional affiliations or collaborations existed between the study authors and the interviewees before recruitment. Table 1 outlines participant roles, with several experts possessing dual expertise: P1–P4 were Pediatric Registered Nurses and researchers, P5 and P11–P12 combined architectural and research expertise, and P10 was a Psychologist and Pediatric Researcher.
Participant Characteristics.
The study, conducted between June 2020 and June 2021, invited experts via personalized emails detailing the study's scope and significance. One-on-one interviews (∼60 minutes) were conducted on a secure Zoom platform using a semi-structured interview protocol (see Supplemental Material). Topics included pediatric healthcare design trends, patient-centered strategies, integration of emerging technologies (e.g., VR and AI), and barriers to implementation. All interviews were audio and video recorded and transcribed using Otter.ail. The lead researcher reviewed and corrected transcripts for accuracy before proceeding with thematic analysis.
Data were analyzed using Braun and Clarke's (2006) six-phase framework for thematic analysis, which included familiarization, coding, theme identification, and iterative refinement (Figure 1). MAXQDA, a qualitative data analysis software program (VERBI Software, 2021), was initially used for early coding and codebook development. Subsequently, the dataset was manually coded in Excel. The lead researcher and a research assistant independently coded a subset of interviews, generating approximately 200 codes that were reconciled into broader categories through discussion. A collaboratively developed codebook guided the subsequent analysis, which the lead researcher applied iteratively to the full dataset from 2020 to 2021. In 2024, the dataset was revisited to refine themes for publication, aligned with the original research questions.
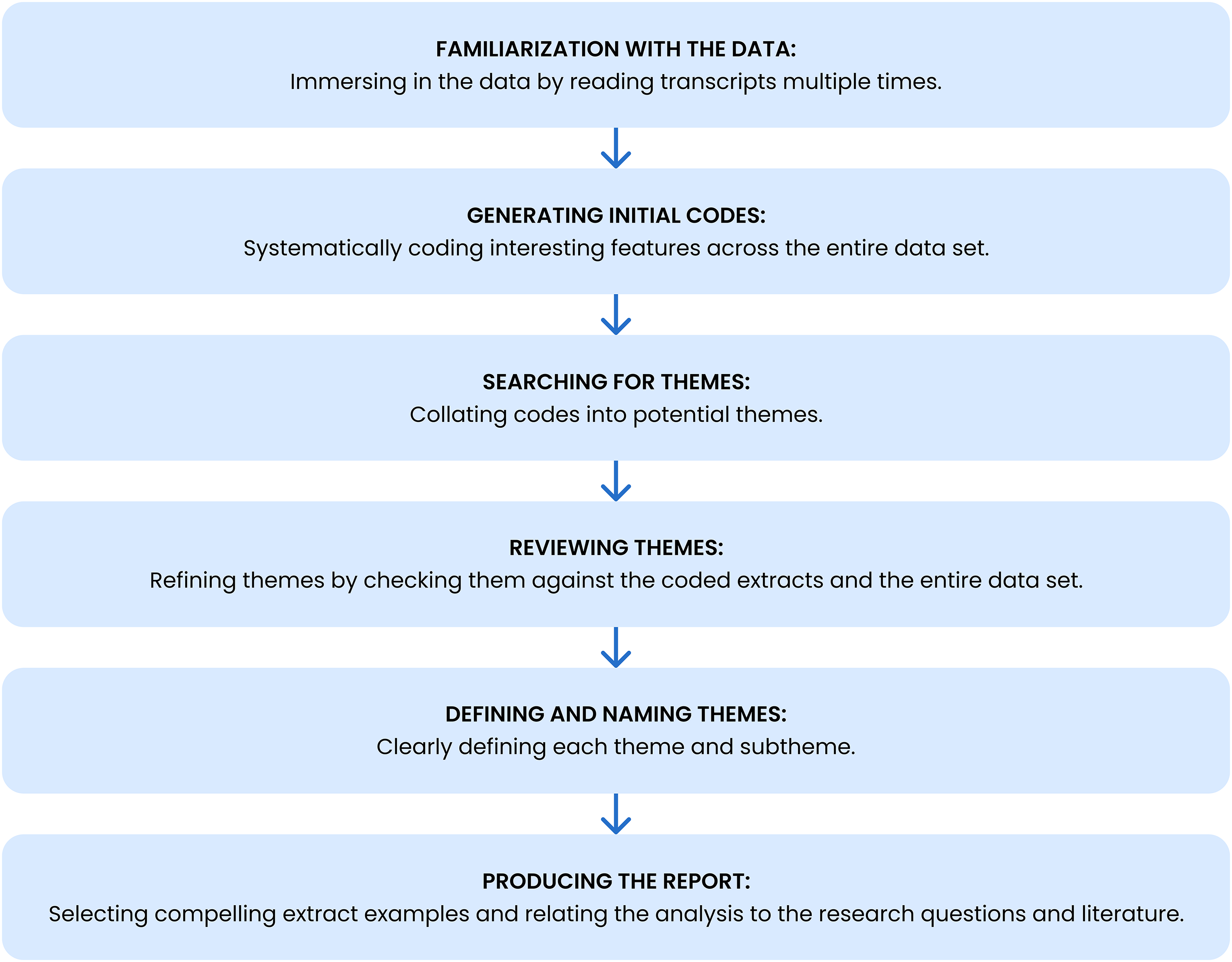
Thematic analysis framework based on Braun & Clarke's six-phase approach (adapted from Braun & Clarke, 2006).
Examples of identified themes included “Design and Trends” (subthemes: Patient Room Design, Private vs. Semi-Private Rooms) and “Technology Integration” (subthemes: VR for Pain Management, AI in Clinical Decision-Making) (see Table 2 for a full list of themes and subthemes). The final analysis identified 55 themes and 266 subthemes. To ensure accuracy, all themes and subthemes were systematically cross-checked against raw transcripts by the lead researcher through an iterative process, ensuring alignment with participant's original narratives.
Summary of Themes and Subthemes Addressing Research Questions on Pediatric Healthcare Design.
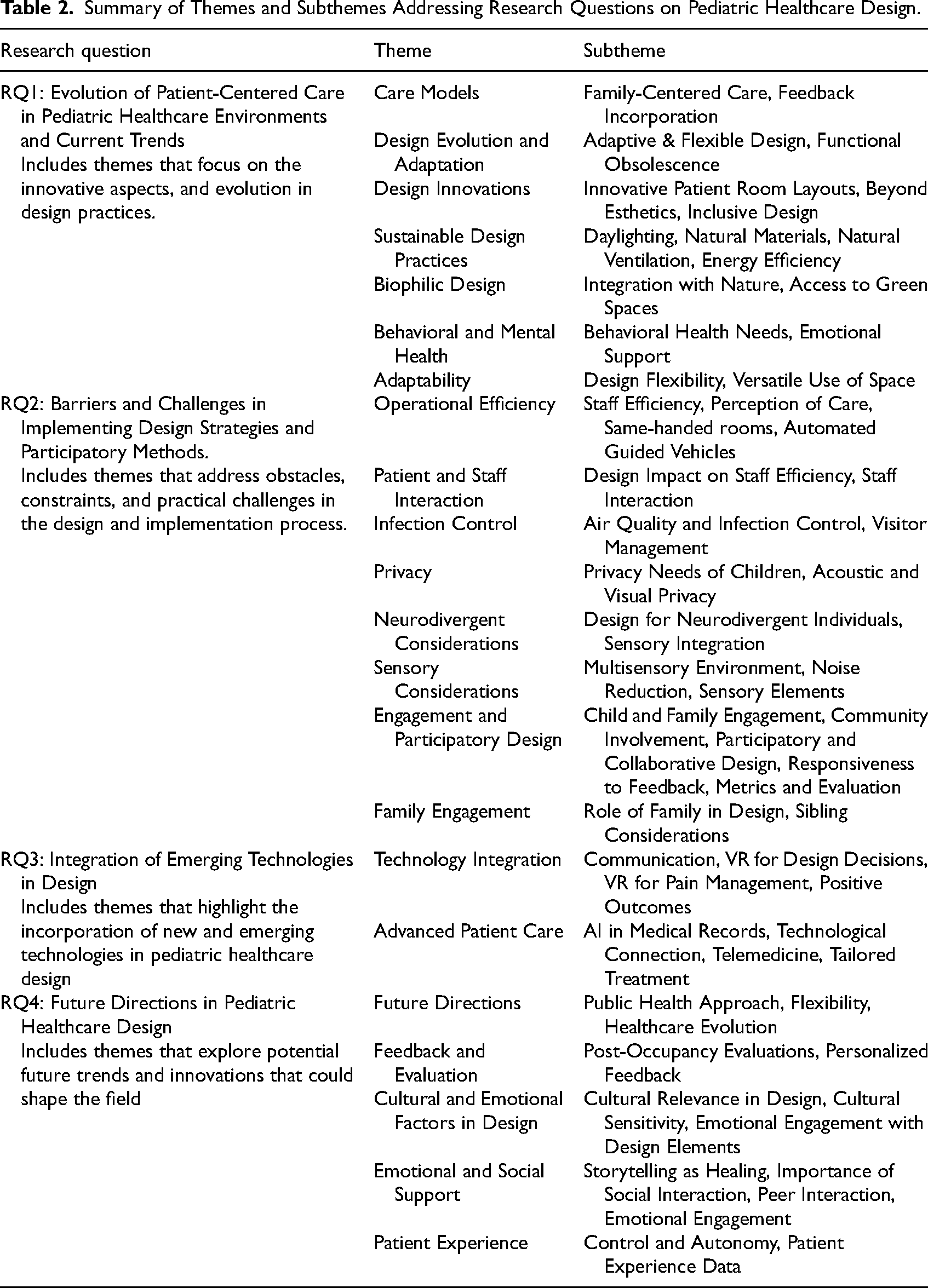
Participant responses were categorized by professional role to facilitate a structured synthesis of perspectives, allowing for a comparative understanding of role-specific priorities and challenges in pediatric healthcare design. Themes and subthemes were analyzed to identify unique and overlapping viewpoints across groups, ensuring alignment with RQ1 (trends), RQ2 (barriers), RQ3 (technology integration), and RQ4 (future directions). The lead researcher synthesized role-based responses, identifying both profession-specific insights and interdisciplinary overlaps. This structured approach strengthened the robustness of findings while maintaining alignment with the research questions.
Although inter-coder reliability was not calculated, credibility was ensured through collaborative codebook development, iterative coding, and revisiting data. Reflexivity—the process of critically examining one's own role, assumptions, and potential biases—was an integral part of the analysis process, with detailed documentation maintained to ensure transparency and consistency (Blair, 2015).
Ethical approval was obtained from the Committee for the Protection of Human Subjects at University of California, Berkeley (CPHS Protocol #2020-04-13200). Informed consent was obtained, and confidentiality was maintained through anonymization and secure data storage.
Results
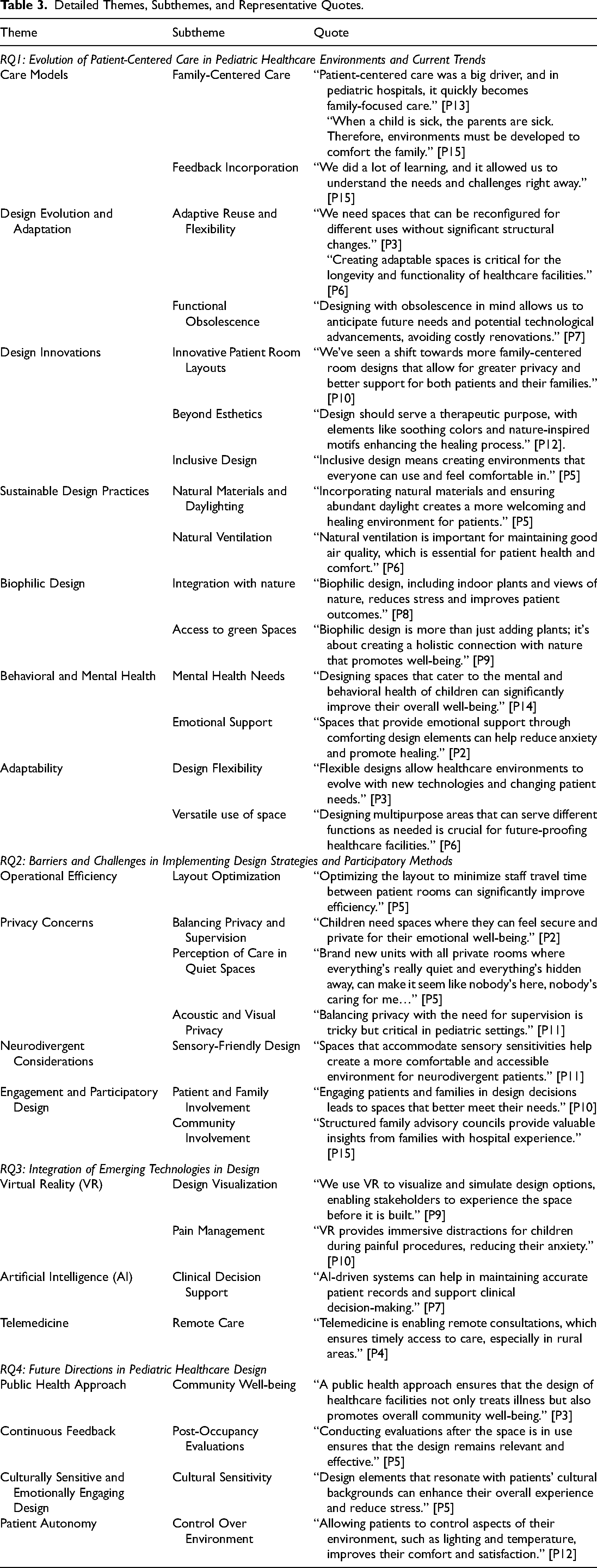
The expert interviews revealed key themes and subthemes in pediatric healthcare design, aligned with the four research questions. These findings included insights shared across roles and profession-specific priorities, reflecting the diverse expertise of participants. Figures 2 and 3 illustrate these trends, barriers, technology integrations, and future directions (Table 2). Table 3 presents representative quotes that deepen understanding of these themes.
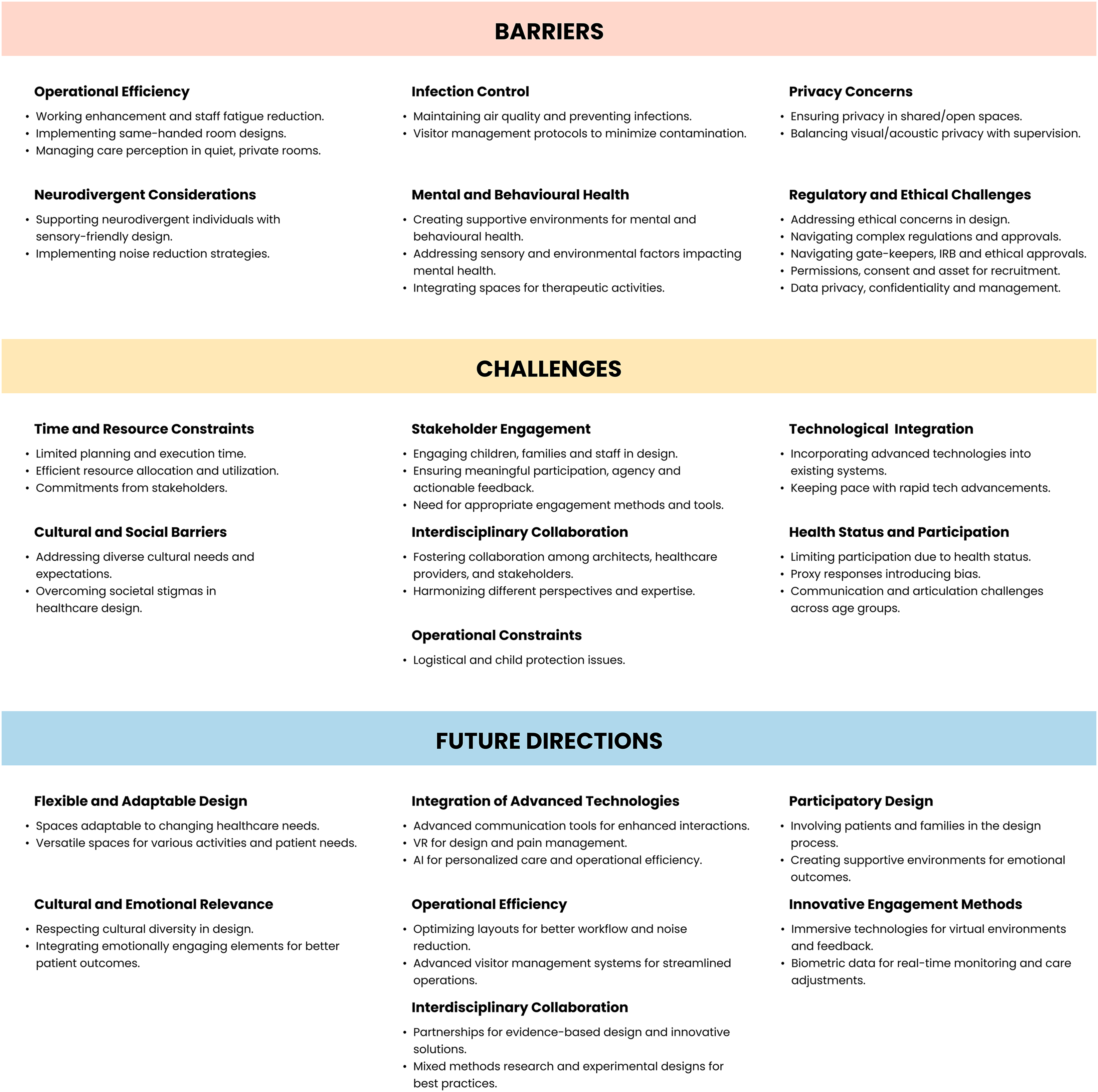
Barriers, challenges, and future directions in pediatric healthcare design.
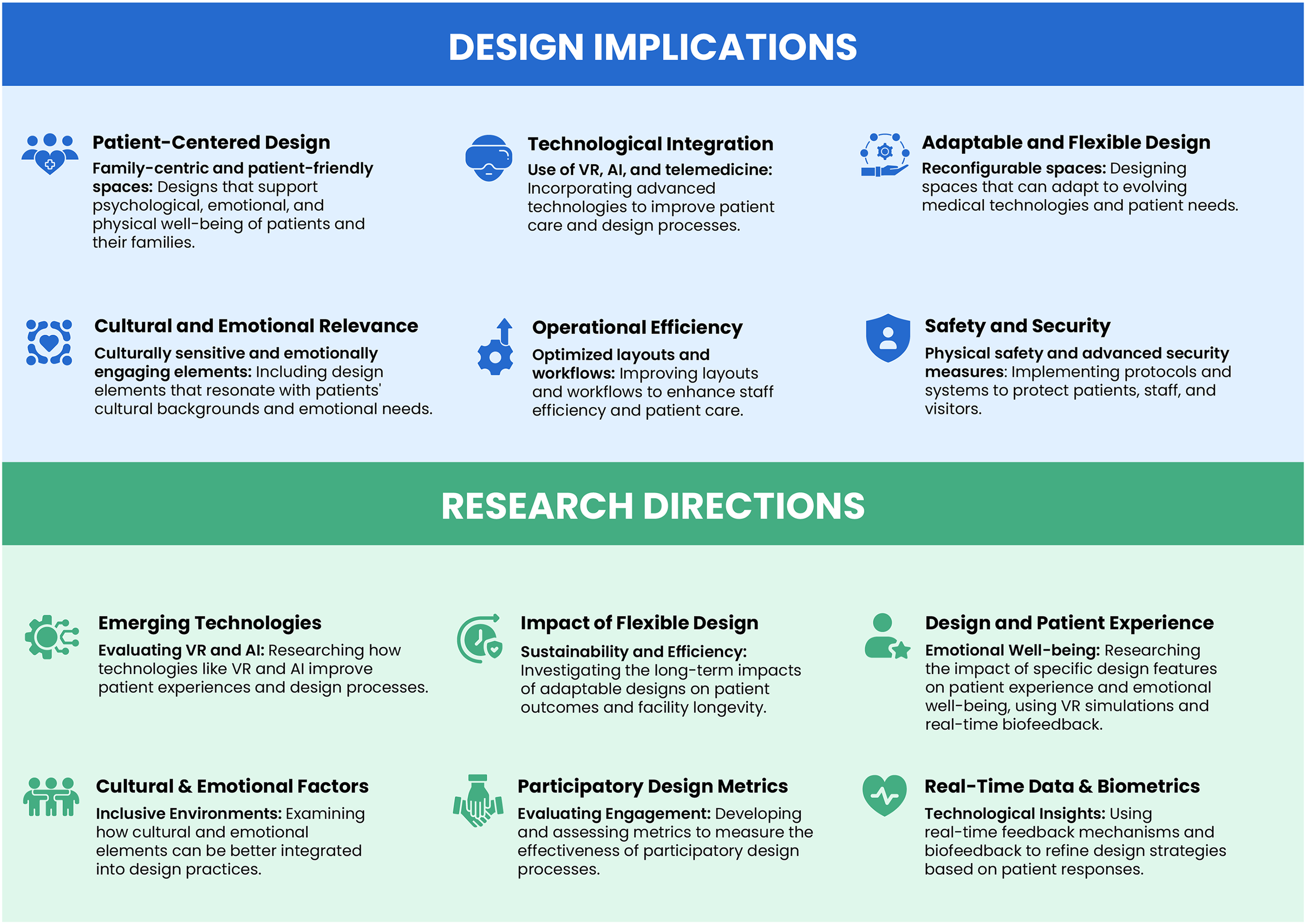
Design implications and research directions in pediatric healthcare environments.
Detailed Themes, Subthemes, and Representative Quotes.
In this study, barriers are defined as systemic or structural constraints, such as privacy concerns, operational inefficiencies, or infection control requirements. Challenges, on the other hand, are process-oriented or interpersonal difficulties, such as engaging diverse stakeholders or addressing the specific needs of neurodivergent patients. This distinction provides a framework for understanding the multifaceted obstacles identified by experts.
Experts emphasized the shift towards family-centered care and the importance of involving families in the healing process. The need for adaptable and flexible design strategies was highlighted to accommodate changing needs and technologies. Innovations in design, including therapeutic elements and inclusive practices, were considered essential for enhancing patient comfort and engagement. Sustainable and biophilic design practices, which integrate natural elements to promote physical and psychological well-being, were recognized for their positive impact on patient well-being. “Family-centered care, paired with adaptable design, is essential for creating pediatric environments that can flexibly support diverse and evolving needs of children and families” (P15, Hospital Owner).
Experts identified barriers such as operational inefficiencies from poor layout designs and privacy constraints in balancing patient supervision with acoustic and visual privacy. Process-oriented challenges included engaging patients and families in the design process and addressing the sensory needs of neurodivergent individuals. These findings underscore the need for systemic solutions alongside participatory approaches to improve design outcomes. “Balancing privacy with supervision remains a major design challenge in pediatric settings” (P12, Pediatric Healthcare Architect & Researcher).
Systemic barriers such as layout inefficiencies and privacy constraints must be addressed in tandem with participatory processes to improve pediatric care outcomes.
Systemic barriers such as layout inefficiencies and privacy constraints must be addressed in tandem with participatory processes to improve pediatric care outcomes.
The integration of emerging technologies such as VR and AI was identified as a key factor in transforming pediatric healthcare design. VR is currently used for design visualization and enhancing patient engagement, while AI supports clinical decision-making and improving operational efficiency. Table 3 shows how experts foresee the practical application of these technologies in healthcare environments. Telemedicine was noted for its role in providing remote consultations and timely medical advice. “VR and AI are driving innovation in pediatric design by enhancing patient engagement and operational efficiency” (P11, Pediatric Healthcare Architect & Researcher).
Future directions include addressing systemic barriers, such as operational inefficiencies, while adopting a public health approach to design that promotes community well-being. Continuous feedback mechanisms, such as post-occupancy evaluations, were emphasized as critical to refining design elements. Incorporating culturally relevant and emotionally engaging design elements was highlighted to enhance patient experience, along with providing patients with greater control over their environment to improve autonomy and satisfaction (Figure 2). “Culturally and emotionally supportive design enhances patient experience and well-being” (P13, Hospital Owner).
While core priorities such as operational efficiency, family engagement, and emerging technologies were widely shared, the emphasis placed on specific design challenges and strategies varied by professional group.
Analysis of Pediatric Healthcare Design Insights by Professional Role
This analysis (Table 4) highlights the unique contributions, focus areas, and challenges identified by different professional groups in pediatric healthcare design.
Analysis of Themes in Pediatric Healthcare Design by Professional Group.
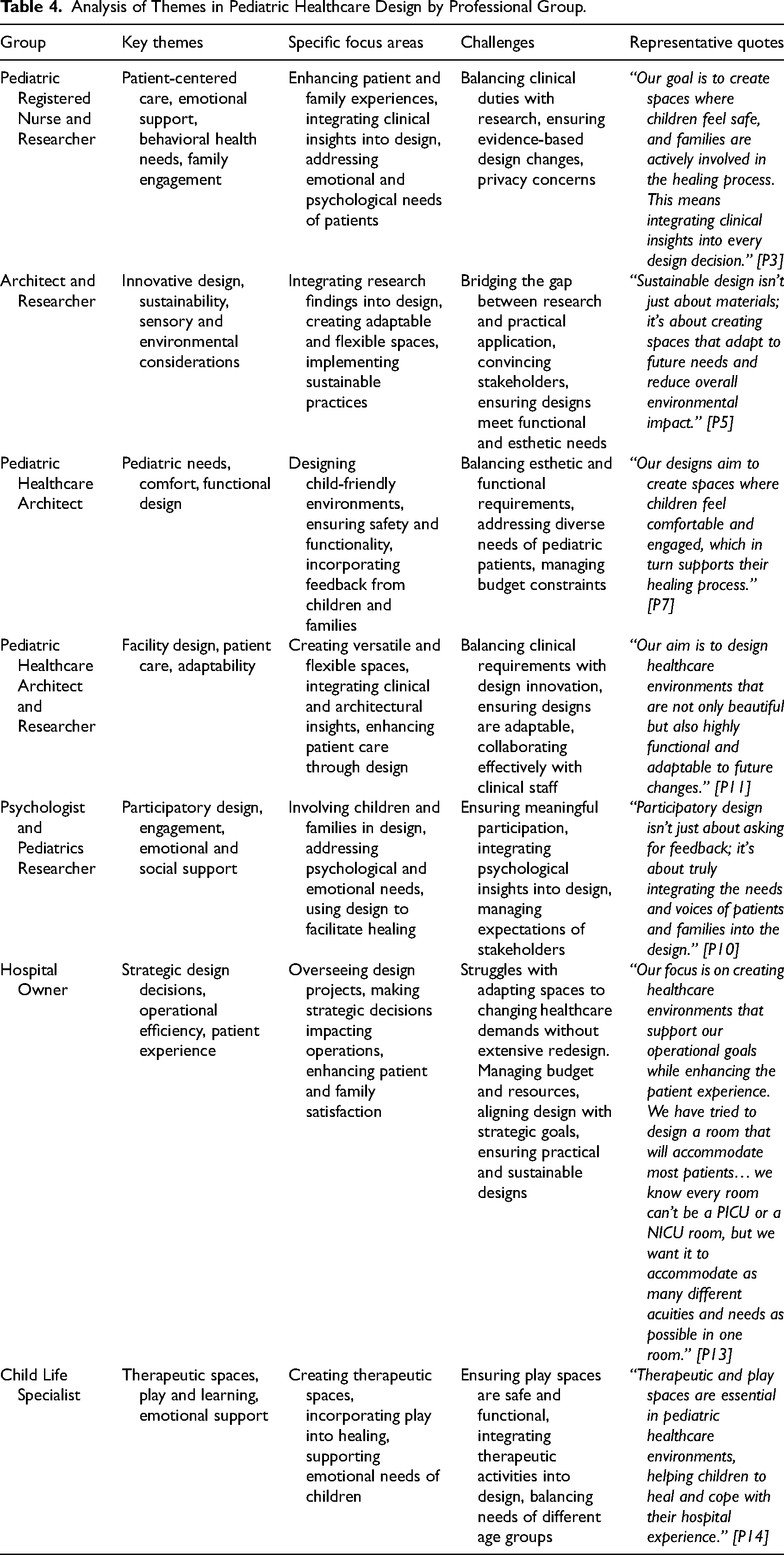
Pediatric nurses and researchers emphasized family engagement and the integration of emotional support within clinical workflows. Their insights highlighted the dual need to address both physical and emotional well-being in pediatric environments. Architects and researchers focused on innovative and sustainable solutions, emphasizing adaptable spaces and biophilic principles to improve patient outcomes while balancing systemic constraints. Pediatric healthcare architects concentrated on child-friendly environments that balance esthetics with functionality, ensuring designs are both engaging and practical for young patients. Psychologists and researchers underscored participatory design and emotional support, advocating for the meaningful involvement of children and families in the design process to align spaces with user needs. Hospital owners prioritized operational efficiency and strategic design decisions to enhance patient experiences while addressing institutional goals. Child life specialists emphasized the importance of therapeutic spaces and play environments in supporting emotional and psychological recovery, particularly through sensory-friendly and engaging designs.
The profession-specific insights highlight the need to bridge operational priorities with emotional and developmental needs in pediatric healthcare environments. A collaborative, interdisciplinary approach is critical to designing spaces that are adaptable, inclusive, and supportive of both clinical outcomes and patient well-being.
Discussion
Findings from this study highlight expert perspectives on key priorities in pediatric healthcare design, including adaptable and flexible environments, integration of emerging technologies, and culturally and emotionally supportive spaces, for positive patient and family experiences. Experts identified a growing shift toward family-centered care, biophilic and inclusive design, and the use of emerging technologies such as VR and AI to enhance healthcare outcomes (Ahmadpour et al., 2024; Yu et al., 2024). However, significant implementation barriers persist, particularly concerning privacy, infection control, and financial constraints, including systemic resource limitations that affect the delivery of pediatric care (Babbu & Haque, 2023; Kucukkaya et al., 2025). These insights contribute to the ongoing discourse on how pediatric healthcare environments can balance clinical efficiency with patient-centered principles, reinforcing the need for interdisciplinary collaboration between architects, clinicians, and administrators to ensure holistic, evidence-based design solutions.
Adaptability and Family-Centered Design
A key theme identified was the increasing emphasis on flexible and adaptable environments, which allow healthcare facilities to accommodate shifting patient demographics, evolving medical technologies, and regulatory changes. The study findings highlight the importance of reconfigurable spaces that can be modified based on patient needs, aligning with universal design principles that support diverse populations, including specialized equipment requirements (Nourmusavi Nasab et al., 2020). Implementing adaptable designs in pediatric healthcare remains complex, requiring coordination across operational, technical, and user-centered priorities, often constrained by organizational protocols and budget limitations (Kipps & Erdman, 2025). This finding supports prior research demonstrating that while flexible designs enhance patient experience and staff efficiency, they require strong institutional commitment for successful execution (Halawa et al., 2020).
Family-centered care and flexible design strategies are essential to creating pediatric environments that adapt to changing clinical, developmental, and technological needs.
Family-centered care and flexible design strategies are essential to creating pediatric environments that adapt to changing clinical, developmental, and technological needs.
Embedding family-centered care spatially within pediatric hospital environments emerged as a key recommendation, highlighting the need to align family engagement strategies with clinical workflows. The benefits of family-centered care are well documented, including improved patient satisfaction, reduced stress, and better clinical outcomes (Hodgson et al., 2024). However, findings from this study suggest that implementation remains inconsistent due to spatial, cultural, and operational constraints. Prior literature indicates that family-centered design features such as family sleep accommodations, communal spaces, and interactive patient rooms support caregiver engagement, but these features must be effectively integrated into clinical workflows to avoid disruptions (Okoniewski et al., 2022). The findings reinforce the importance of designing spaces that allow families to participate in care while maintaining a balance between privacy and supervision.
Integration of Emerging Technologies
The adoption of VR, AI, and telemedicine emerged as a transformative opportunity in pediatric healthcare design. The study findings reinforce how VR is increasingly valued for its roles in immersive design visualization, therapeutic applications, and patient engagement, aligning with prior research demonstrating its benefits for alleviating anxiety and supporting pediatric care experiences (Eijlers et al., 2019; Jansen et al., 2023). AI was identified as a critical tool for optimizing clinical decision-making, streamlining workflows, and personalizing care, reinforcing broader trends toward technology-enabled healthcare delivery (Pallavicini & Bouchard, 2019; Topol, 2019). Despite enthusiasm for emerging technologies, the findings underscore persistent challenges related to privacy, ethical concerns, and high implementation costs, which continue to limit broader adoption (Fustino et al., 2019; Montreuil et al., 2021). Successful integration requires interdisciplinary collaboration among designers, healthcare professionals, and technologists to ensure their effective, ethical, and sustainable implementation (Bosch & Lorusso, 2019). One significant barrier to technology integration is the lack of spatial readiness in existing hospital infrastructures.
Integrating technologies like VR and AI into pediatric environments demands alignment with developmental appropriateness, emotional safety, and workflow integration.
Integrating technologies like VR and AI into pediatric environments demands alignment with developmental appropriateness, emotional safety, and workflow integration.
While telemedicine has expanded access to pediatric critical care, designing hybrid physical-digital consultation spaces remains challenging due to infrastructure demands, care coordination needs, and variations in implementation outcomes (O’Brien et al., 2024). The need for flexible consultation rooms equipped with integrated digital infrastructure emerged as a significant design priority, reflecting the growing role of hybrid physical-digital healthcare delivery models. Research suggests that while hybrid models improve healthcare accessibility, they require spatial and technological investment to ensure user-friendly implementation (Chen et al., 2020). Future pediatric healthcare environments must proactively incorporate these technologies into early-stage design processes to maximize their benefits.
Balancing Infection Control, Privacy, and Sensory Considerations
Privacy concerns, operational efficiency, and infection control remain significant barriers to implementing patient-centered and participatory design strategies. Balancing patient privacy with supervision, particularly in open or shared spaces, emerged as a critical and complex design challenge, with experts highlighting the trade-offs between visibility, acoustic control, and emotional well-being (Yu et al., 2024). Prior research suggests that adolescents and neurodivergent patients require greater control over environmental factors, including lighting, noise levels, and spatial boundaries, reinforcing the importance of sensory-friendly and customizable spaces (Higuera-Trujillo et al., 2020). Solutions such as sound-absorbing materials, strategic partitioning, and advanced ventilation systems are essential to maintaining privacy while optimizing workflow and ensuring air quality (Litwin et al., 2023). Adjustable lighting, temperature control, and sensory design elements—including tactile-friendly surfaces and biophilic motifs—can enhance patient comfort and promote emotional and psychological well-being (Shepley et al., 2016). The prominence of Participatory Design in expert perspectives reinforces the need for early and continuous engagement of patients, families, and healthcare professionals to create inclusive, adaptable healthcare environments. Prior studies confirm that early stakeholder engagement improves the usability and effectiveness of pediatric healthcare spaces, leading to more responsive and patient-centered environments (Coyne & Carter, 2018; Larsson et al., 2018). Infection control protocols, while necessary for patient safety, often conflict with emotional and social needs. Single-patient rooms reduce hospital-acquired infections, yet they also limit opportunities for social interaction, increase caregiver burden, and contribute to patient isolation (Sathyanarayanan et al., 2025). While supporting private patient rooms for infection control, experts advocated complementary design strategies that also foster social interaction, emotional support, and flexibility within pediatric environments (Ulrich et al., 2020). Strategies such as biophilic design, smart air filtration, and modular partitions could provide a more holistic approach, balancing clinical safety with social engagement and emotional comfort.
Culturally Sensitive and Emotionally Supportive Environments
Culturally sensitive and emotionally supportive design emerged as central priorities in shaping pediatric healthcare environments that promote belonging, reduce stress, and support recovery. Research confirms that incorporating cultural elements into hospital design can reduce patient stress, foster a sense of belonging, and improve health outcomes (Kaihlanen et al., 2019; Lauwers et al., 2024). Healthcare environments that reflect patients’ cultural backgrounds through design motifs, language accessibility, and familiar spatial layouts can contribute to a more inclusive and welcoming experience. Culturally responsive spaces should go beyond language-inclusive signage to integrate storytelling areas, community gathering spaces, and interactive design elements that reflect the diverse identities of pediatric patients and their families. Prior research suggests that nature-inspired motifs, social interaction areas, and play-driven engagement zones can reduce anxiety and stress in pediatric patients, reinforcing the therapeutic value of emotionally supportive environments (Higuera-Trujillo et al., 2020; Jiang, 2020). Neurodivergent children and those with mental or behavioral health needs require tailored design approaches. Emphasizing the importance of sensory-friendly environments, the findings highlight the need to prioritize noise control, lighting adjustments, and tactile considerations to create more inclusive spaces for children with sensory sensitivities (Shepley et al., 2016). Biophilic design, which includes access to natural light, greenery, and calming color schemes, has been shown to enhance patient recovery and overall well-being (Litwin et al., 2023). Pediatric hospitals should integrate flexible and patient-controlled settings that allow children to personalize their surroundings, reinforcing autonomy and comfort.
Designing for neurodivergent and behaviorally complex pediatric populations requires inclusive, sensory-responsive, and customizable spatial strategies.
Designing for neurodivergent and behaviorally complex pediatric populations requires inclusive, sensory-responsive, and customizable spatial strategies.
These findings align with broader research advocating patient-centered care and participatory design principles in pediatric healthcare environments. The emphasis on flexibility, technology integration, and inclusive design reflects current shifts in healthcare design research, which recognize the need for dynamic and adaptable spaces that support both clinical needs and patient well-being. This study extends existing knowledge by highlighting expert perspectives on emerging design approaches, particularly how cultural sensitivity, sensory integration, and participatory strategies can enhance pediatric healthcare spaces.
Limitations
This study involved experts primarily from the United States, potentially limiting the diversity of perspectives as cultural and regional factors influence applicability. Experts’ professional backgrounds may have introduced bias, and reliance on self-reported data limits objectivity. The exclusion of direct input from patients or families restricts insights into their experiences and preferences. While focusing on VR and AI, the study offered limited exploration of other technologies, such as telemedicine, which could enhance healthcare design insights. Thematic analysis by a single coder may be a limitation. To address this, iterative re-coding and reflexive practices were applied to reduce bias, supported by detailed documentation to ensure transparency and data-driven findings. The absence of formal inter-coder reliability may reduce interpretive variability achieved through collaborative coding. While the interviews provided rich qualitative insight into priorities and strategies across professional roles, the format did not elicit direct trade-off decisions or explicit recommendations on what to de-prioritize.
Recommendations for Future Research
Future research should include pediatric patients and families to capture their needs and preferences in healthcare environments. Their direct input offers perspectives not covered in this study. Expanding research across cultures and regions would provide a more comprehensive understanding of how cultural and regional factors influence design preferences and outcomes. A mixed-methods approach, integrating quantitative and qualitative methods, could enrich studies by examining design impacts on recovery times, anxiety levels, and satisfaction. Longitudinal studies should assess the long-term effectiveness of adaptable designs and emerging technologies such as AI, VR, and telemedicine. Research should also focus on balancing infection control with patient-centered design by exploring strategies like modular partitions, hybrid private-social spaces, and smart ventilation systems. Further studies on design strategies for neurodivergent populations, including children with autism and developmental disorders, are needed to create inclusive and supportive healthcare environments. Cost-benefit analyses should evaluate the financial feasibility of adaptable spaces and technology-driven patient engagement tools to inform healthcare investment decisions. Future research could incorporate structured decision-making methods, such as conjoint analysis or discrete choice experiments, to examine how experts prioritize among competing design considerations under resource and operational constraints.
Conclusion
This study provides a comprehensive examination of pediatric healthcare design, synthesizing expert perspectives to identify current trends, systemic barriers, and actionable pathways for future innovation. By integrating insights from architects, pediatric nurses, psychologists, and healthcare administrators, it highlights the value of interdisciplinary collaboration in creating adaptable and inclusive healthcare environments tailored to the needs of diverse populations. The findings emphasize the critical role of flexible and culturally sensitive design strategies that respond to technological advancements, shifting demographics, and the specific needs of neurodivergent children and vulnerable populations. Emerging technologies, such as VR and AI, are positioned as transformative tools for enhancing patient engagement and operational workflows, provided their integration addresses challenges like privacy and ethical concerns.
This research uniquely contributes to the field by emphasizing participatory design methods, sensory-friendly environments, and the need for expert-driven solutions to systemic challenges like operational inefficiencies and infection control. It underscores the importance of tailoring design features to individual patient needs, including sensory and emotional considerations, as a foundation for future healthcare environments. Future research should integrate patient and family perspectives to complement expert insights, ensuring that healthcare environments holistically address lived experiences alongside systemic requirements. Expanding research across cultural and regional contexts will further enrich the understanding of pediatric healthcare design and its role in supporting community well-being. Actionable recommendations for healthcare designers and policymakers include fostering interdisciplinary collaboration, leveraging emerging technologies responsibly, and prioritizing inclusivity to create environments that comprehensively support young patients and their families.
Implications for Practice
Flexible Design Approaches: Emphasizing adaptable design solutions is essential to accommodate technological advancements and shifting patient demographics, supporting the long-term functionality of pediatric healthcare facilities.
Integration of Emerging Technologies: Thoughtful incorporation of technologies like VR and AI in the design process and patient care can enhance patient engagement, improve workflow efficiency, and support positive health outcomes.
Balancing Privacy With Operational Efficiency: Addressing privacy concerns while maintaining efficient healthcare operations is crucial, necessitating design strategies that protect patient confidentiality without compromising visibility and supervision.
Culturally Sensitive and Emotionally Supportive Environments: Creating healthcare spaces that reflect the cultural backgrounds and emotional needs of patients and families can reduce stress, promote belonging, and improve overall patient experience and satisfaction.
Interdisciplinary Collaboration in Design: Engaging a multidisciplinary team—including healthcare professionals, designers, patients, and families—in the design process can result in environments that meet the complex and diverse needs of pediatric populations.
Supplemental Material
sj-docx-1-her-10.1177_19375867251353733 - Supplemental material for From Challenges to Innovations: Expert Insights in Pediatric Healthcare Design
Supplemental material, sj-docx-1-her-10.1177_19375867251353733 for From Challenges to Innovations: Expert Insights in Pediatric Healthcare Design by Haripriya Sathyanarayanan and Luisa Caldas in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors extend sincere appreciation to the expert participants for their invaluable contributions to this study, and to The Beryl Institute for supporting this work through the Patient Experience Scholar Program. Special thanks to Shraddha Ramakrishnan, Graphic Designer, for assistance with the development of the figures, and to Jahara Cayabyab for support with the initial coding of interview transcripts.
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by The Beryl Institute's 2020 Patient Experience Research Grant for Scholars.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.