
Abstract
Window views, indoor plants, and room décor can potentially improve restoration and healing in a hospital room environment. Preferences for these attributes and their individual effect on physiological and cognitive outcomes remain understudied. This study investigated the extent to which visible green nature in window views, plantscapes, and green colored decor in virtual reality hospital rooms, affected restoration outcomes of simulated acute care patients. First, 12 room environments were developed in virtual reality where window views, plants, and green-colored room decor variables relevant to Stress Recovery Theory were systematically manipulated. Next, participants in a simulated patient acute-injury scenario (N = 188), which induced an external stress process, rated the environments on how much they perceived the room contributed to their sense of feeling relaxed and ability to clear their mind of stressful thoughts. Ratings for each environment were aggregated and used in full-profile and moderated conjoint analyses. Indoor plants produced the highest utility score on physical relaxation, while nature window views had the highest utility score for mental clarity. Utility scores for indoor plants were significantly higher on physical relaxation and mental clarity for the respondents with higher scores of acute cognitive stress, induced from the external stressor process. The verdant elements (e.g., green nature views, indoor plants, and green room décor) were associated with the highest restorative utility. Buildings obstructing nature views were associated with negative utility scores on the restoration outcomes. Findings highlight the individual and combined effects of: (1) indoor plants; (2) unobstructed views from the window of green nature; and, (3) green-colored décor in hospital room design.
Keywords
Introduction
Hospital patients commonly spend extended periods of time during their convalescence indoors, over time, they can realize benefits from restoration through window views and immersion in nature attributes (Holte et al., 2011; Raanaas et al., 2012, 2016). Restoration entails physical and psychological resources that are depleted due to stress from illness and challenges healing in a hospital environment (Andrade & Devlin, 2015). Hospitals have traditionally varied in the degree to which they support patient restoration through environmental design interventions, and the hospital room is a critical space on which people rely for healing (Andrade & Devlin, 2015). Namely, attributes of nature in window view, plants, and room décor including wall color and art appear to support restorative processes, in addition to other forms of aesthetic fascination and visual complexity from architectural and deisgn features that redirect attention (Masoudinejad & Hartig, 2020; Michels et al., 2022; Totaforti, 2018).
Namely, window views have been found to promote patient well-being (Grinde & Patil, 2009; Van den Berg et al., 2016). Specifically, a window view with high proportions of green nature and visible trees has been found to significantly reduce patient stress (Honold et al., 2016; Van den Berg et al., 2016). Also, the proximity to the nature and the size of a window that increases connection between the patient in the interior and the outdoors, effectively reduces stress (Ozdemir, 2010; Raanaas et al., 2012, 2016). The aesthetic characteristics of the type of nature observed through a window seem to be important, such as mountains, sky, lakes, trees, green landscapes, and other natural elements (Astell-Burt et al., 2022; Klompmaker et al., 2022; Yin et al., 2022), however, green-colored nature has predominantly been credited for fostering higher levels of restoration compared to other color themes (Bratman et al., 2019, 2021; Frumkin et al., 2017; Markevych et al., 2017; Mygind et al., 2019). Second to green nature, there is evidence that exposure to blue sky can positively impact psychological restoration and well-being, reduce stress, and promote feelings of calm (Masoudinejad & Hartig, 2020).
Relatedly, several studies have provided evidence of healing benefits to patients from an immersion in plants and indoor gardens (Marcus & Sachs, 2013; Raanaas et al., 2010). Architecture and building facades have also been identified as altering window views and compared with nature views on influencing relaxation and stress reduction (Lindal & Hartig, 2013; Ulrich, 1993). While some studies have demonstrated the relaxing effects of soft focus on building facades and building textures (de la Fuente Suárez & Martínez-Soto, 2022), visual preferences for natural landscapes over building or urban scenes have long been confirmed (Ulrich, 1993), and particularly associated by hospital patients with restoration and healing outcomes.
The extant literature indicates that hospital room window views of nature, plantscapes, and green-colored decor play a critical role in fostering restorative experiences among patients. However, while extensive research exists on their individual effects, studies comparing the influence and analyzing the combined influence of these hospital room features remain limited (Raanaas et al., 2012; Van den Berg et al., 2016). Moreover, research has shown that hospitalized patients in high-stress medical conditions often experience heightened sensitivity to environmental stressors, making the visual comfort of their surroundings even more significant (Huisman et al., 2012; Ulrich, 1984, 2001). Acute-care patients are individuals receiving short-term, intensive medical treatment for severe, sudden-onset conditions that require immediate medical attention and close monitoring. Unlike patients in chronic care, rehabilitation, or long-term hospital stays, acute-care patients often experience intense and immediate stressors due to the urgency and severity of their conditions. Further research utilizing multivariate techniques to understand how acute-care patients perceive multiple attributes of the hospital room is therefore warranted, as it can inform hospital administrators and designers to optimize visual surroundings for patient recovery, offering both theoretical insights and practical applications to reduce stress which in turn promotes healing.
To this end, the objective of this study was to assess the influence of hospital room environments on restoration outcomes of acute-care patients, with a particular focus on visual attributes. To achieve this, we employed conjoint analysis to evaluate how individual and collective environmental factors in virtual reality hospital room scenarios influence the perceived experiences of simulated acute-care patients.
Participants were exposed to 12 hospital room environments presented in virtual reality following an acute stressor induced through a transportation narrative experience of a severe injury and recovery process in a hospital room, allowing for controlled evaluation of the relative impacts of systematically varied window view, plantscape, and green decor attributes on restoration outcomes. We specified two levels of green nature window views, visibility of adjacent buildings through the window, the extent of the hospital building's enclosure obstructing window view, depth of sky in window view, indoor potted plants, outdoor window planters with plants, and green-colored room décor in a fractional factorial design. Participants evaluated a total of 12 hospital room environments in virtual reality, modeled based on the fractional factorial design to measure the extent to which they perceived each room contributed to restoration, including their sense of feeling relaxed and their ability to clear their mind of stressful thoughts.
Conjoint analyses of the scores revealed the relative contribution of each level of the attribute to those perceptions as well as produced overall attribute importance scores. Additionally, we explored whether the attributes had differential effects on participants reporting higher scores of stressful thoughts invading their mind as induced by the external stressor, predicting how much more window view, plantscape, and green attributes may contribute to restoration outcomes as levels of acute stress increase.
However, it is crucial to acknowledge that actual hospitalized acute-care patients may not react to environmental stimuli in the same way as simulated patients undergoing a narrative transportation process and exposed to virtual reality hospital room environments. Extrapolating these findings to real-world settings requires further validation. Our study on a nonhospitalized, simulated acute-care patient population aims to provide broad insights into the potential collective restoration benefits of various window view, plantscapes, and green room décor attributes in a hospital room and tests preliminary assumptions about the distinct differences in the relative influence of the individual attributes on physical relaxation and mental clarity. Moreover, this study's research aims to add to the experimental literature testing hypotheses based on the tenets Stress Recovery Theory (Sonnentag & Fritz, 2007). Stress Recovery Theory (SRT) suggests that natural environments help reduce stress and promote recovery by lowering both stress-related physiological and psychological markers.
Theoretical Framework Guiding the Study
Stress RecoveryTheory (Sonnentag & Fritz, 2007) provides a foundation for understanding how individuals recuperate from stress and highlights the role of specific activities and environmental conditions that facilitate relaxation, psychological detachment, mastery experiences, and resource replenishment. According to Ulrich (1993) nature exposure can be expected to relax psychological and physiological stress, enhance cognitive functioning, and improve healing outcomes. Achieving stress relief requires individuals to disengage from external stressors that contribute to cognitive and physiological strain. Accordingly, visual elements play a crucial role in this recovery process, promoting low-arousal positive states to support psychological restoration (Ulrich, 1981; Ulrich et al., 1991).
Thus, Stress Recovery Theory is particularly relevant when examining the restorative benefits of biophilic design, which integrates natural elements into built environments to enhance well-being. This framework supports the notion that immersion in natural surroundings fosters physical relaxation, mental rejuvenation, and emotional stability (Kellert & Wilson, 1995). The Psychoevolutionary Theory (PET) closely linked to Stress Reduction Theory (Ulrich, 1983) suggests that humans inherently respond positively to natural environments due to evolutionary associations with safety, survival, and refuge. Additionally, Prospect-Refuge Theory (Appleton, 1996; Stamps III, 2008) provides further insight into the significance of natural settings and survival, emphasizing the human tendency to seek landscapes that offer security and protection. Features such as dense vegetation, trees, and enclosed natural spaces historically served as protective shelters, contributing to a sense of safety and psychological comfort (Kellert et al., 2011). Applying these principles to interior design, SRT suggests that exposure to biophilic environments within built spaces can function as a stress-buffering mechanism, promoting relaxation and stress recovery (Gaekwad et al., 2022, 2023).
In healthcare design, SRT has been widely examined as a framework for integrating biophilic elements to support stress recovery in terms of physical and cognitive restoration among hospital patients. Research indicates that hospitalized patients with access to nature-inspired environments—such as window views of green landscapes, indoor plants, and natural light—experience lower stress levels, reduced anxiety, and improved psychological well-being (Dijkstra et al., 2008; Ulrich, 1984; Ulrich et al., 1991).
Studies by Ulrich (2008) and Raanaas et al. (2016) demonstrate that hospital rooms featuring biophilic elements contribute to faster physiological recovery, including lower heart rates, decreased blood pressure, and reduced cortisol levels. Similarly, patients recovering in rooms with windows offering views of nature report higher relaxation levels and improved emotional states compared to those in windowless or enclosed environments (Pati et al., 2016; Raanaas et al., 2012; Verderber & Reuman, 1987).
Additionally, research on biophilic hospital spaces has shown that patients in environments incorporating natural elements, such as plants, trees, gardens, or nature-inspired artwork, exhibit improved cognitive clarity and emotional resilience (Dijkstra et al., 2008; Masoudinejad & Hartig, 2020). These findings reinforce the therapeutic potential of biophilic design in clinical settings, emphasizing its visual role in enhancing attention restoration, mental clarity, and stress reduction.
However, gaps exist in the literature regarding the visual perceptual factors of views through windows to green nature, and how multiple elements including view of green nature through a window, indoor and outdoor plants, green-colored interior design elements, openness and depth sky views, alteration of views from building enclosure and adjacent buildings affect restoration (Lindal & Hartig, 2013; Masoudinejad & Hartig, 2020; Van den Berg et al., 2016). Filling the gaps is of theoretical importance and contributes to recommendations for more effective design of hospital buildings and rooms that optimize visual surroundings for restorative outcomes of patients. Particularly, acute-care patients undergoing stressful procedures and facing challenges during the healing and recovery process.
The purpose of the present study was to explore how acute-care patients experience a hospital room environment; specifically, what they see through the window (i.e., proportion of green nature and adjacent buildings), architectural embodiment (the extent to which they see the hospital building's envelope in view), how much they see outward (i.e., depth of view to the horizon and sky), plant immersion (indoor plants and outdoor window box plants), and green-colored interior décor (green wall color and artwork). The conceptual framework is shown in Figure 1.
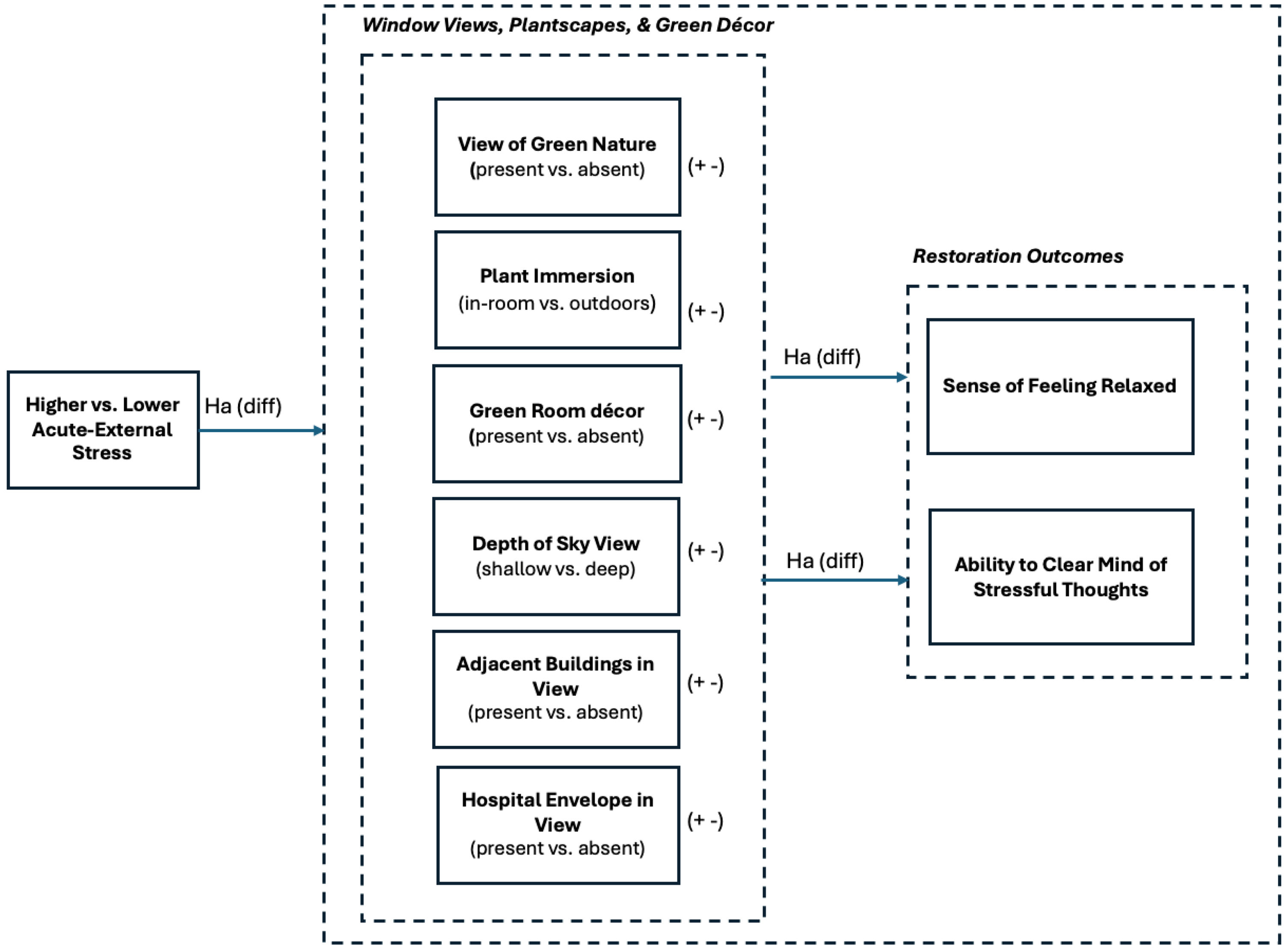
Hypothesized Framework of Stress Recovery in a Hospital Room from Window Views, Plantscapes, and Green Decor.
A multistage procedure to test the propositions of the restorative effects of window views, plantscapes, and green-colored décor elements in a hospital room (Figure 1) was conducted.
Methods
Study Design and Procedure
The first part of the study involved specification of six hospital room window view, plant, and green decor attributes based on the tenets of Stress Recovery Theory and elements tested on relaxation and cognitive enhancement outcomes in past literature. Fractional factorial design methods were used to systematically vary attributes across 12 hospital room scenarios that were then developed using 3D visualization software for experienceing in virtual reality. The second part of the study involved 12 hospital room scenario evaluations (n = 188). The third part of the study involved testing evaluations using conjoint analysis techniques and interpreting attribute part-worth estimates and importance scores.
Specification of Room Attributes
The present study identified an initial list of six hospital room attributes related to window views, plantscapes, and green-colored décor based on a thorough review of prior academic literature (e.g., Masoudinejad & Hartig, 2020; Van den Berg et al., 2016). The selection process was guided by SRT, which underscores the role of specific environmental conditions in fostering relaxation, psychological detachment, mastery experiences, and resource replenishment (Hartig & Kahn, 2016; VandenBerg et al., 2003) with particular consideration for the acute-care context and environmental stressors affecting hospital patients.
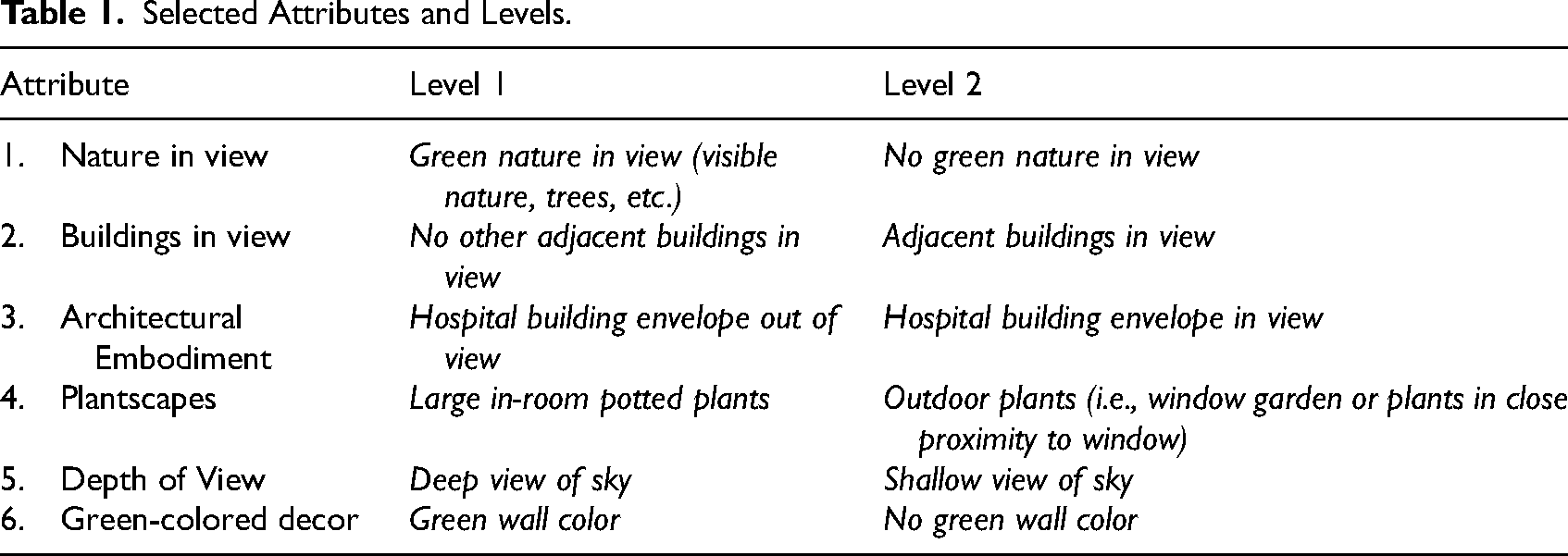
To ensure academic rigor and relevance, a systematic expert review process was undertaken with several senior academics specializing in environmental psychology, public health, healthcare interior design, and architecture. This process consisted of several key steps. An initial set of hospital room attributes was extracted from peer-reviewed studies focusing on biophilic design, isovist theory, stress recovery, and healthcare environments. The attributes were then cross-validated against empirical evidence supporting its influence on patient restoration outcomes, including stress reduction, and cognitive restoration. A structured review process ensured that the six selected attributes were theoretically sound, empirically supported, and contextually relevant for testing within an acute-care hospital setting. Faculty members provided structured feedback on attribute clarity, specificity, and operationalization, ensuring that each factor was distinct, measurable, and meaningful for patient recovery outcomes. Following expert review, the six attributes were explicitly defined with multiple levels for subsequent testing in conjoint analysis. The attributes and respective levels are summarized in Table 1.
Selected Attributes and Levels.
Virtual Reality Scenario Development
A fractional factorial design reduced the number of scenarios from a full factorial design (128) while maintaining orthogonality and ensured each level of the six attributes appeared the same number of times throughout 12 profiles. The number of profiles was determined based on the parameters needed to derive stable part-worth estimates for full-profile conjoint analyses. Conjoint analysis has been used in prior studies in consumer behavior literature to measure the degree of importance of a product's attribute both individually and combined with other attributes in a bundle, on consumer choice (Millar & Baloglu, 2011). Notably, studies by Suess and Mody (2017), Suess et al. (2024) and Guzzo et al. (2022) adapted the full-profile conjoint method to visualizations of hospital and biophilic attributes including architectural and interior design features, products, and services, in the form of 3D renderings. Following these studies, we incorporated the hospital room attributes specified in each of the 12 scenarios by the factorial design into 3D models, systematically varying one or the other level of the six attributes based on the method recommendation by (Xu & Yuan, 2001). 3D models were developed in Rhino v.7.0 software. The base hospital room model before the addition of attributes was created from exact dimensions and assets in a hospital room at the Clinical Learning Resource Center at Texas A&M University Health Science Center. The models were transferred to a custom-built dual-display port Dell gaming desktop computer and rendered in Enscape v. 3.4 (a software plug-in to Rhino v.7 that renders hyper-realistic 360-degree building information models) in real-time while participants viewed them using a Varjo XR-3 virtual reality headset. All the hospital room profiles were set from the point of view of a semireclined patient, in a bed. Participants could look around completely as well as sit up to elevate the space. To increase representativeness of hospital room views, the 12-room profiles were developed on both upper and lower floors. Examples of the hospital room scenarios used in the study are included in Appendix A.
Experimental Study
The study consisted of three primary stages: the introduction of an external stressor and measurement of self-reported stress measure and galvanic skin device measures, evaluation of the 12 hospital room scenarios in virtual reality, and answers to questions on a self-administered survey on an iPad.
Adults over 18 were recruited to participate in the study using the Human Behavior Lab at Texas A & M Universitys SONA system. Recruitment of participants was stratified across age, gender, and race categories in the local surrounding communities using quota sampling. A total of 188 subjects fully participated in the study by evaluating the 12 hospital room scenarios in virtual reality and completing a self-administered survey. Study time ranged from 29 to 54 min. Data were collected from October to December 2022.
Prior to evaluating the scenarios, respondents were asked to sit on a chair and a galvanic skin response device was placed on their nondominant hand and calibrated. To establish self-reported baseline stress levels, participants were asked to indicate the extent to which they felt their mind was invaded by stressful thoughts on a 5-point Likert-type scale (1 = “Do not feel stressful thoughts at all” to 5 = “Feel extreme stressful thoughts”), a measurement of acute cognitive stress adapted from Memari et al. (2021).
Next, an external stressor was introduced, in the form of a five-minute video showing a roller-coaster accident. This approach aimed to induce an acute-stress response in the participant and simulate an experience as a patient with severe injury. The video included a combination of an animation of a person falling from a roller coaster and stock film of a trauma center, surgery, and hospitalization of a paralyzed patient. Loud, ominous, music was added to the film to enhance affective stress (Yehuda, 2011). While watching the video, participants were prompted by narrative subtitles to imagine that they fell victim to the accident, were rushed to the hospital by ambulance, and then woke up recovering from a major orthopedic rehabilitative surgery. The roller-coaster accident sceneario was adapted from Memari et al. (2021) which was selected over other more realistic accidentor hospitalization contexts (i.e., car crash, occupational accident) to minimize recall and psychological harm. Videos have been proven to be effective as external stressors in studies exploring environmental preference in terms of restoration from stress (e.g., Memari et al., 2021; Park et al., 2020; Van den Berg et al., 2003).
Immediately after viewing the video, a second measurement of the extent to which respondents felt “stressful thoughts were invading their mind” was taken. In addition to the self-reported cognitive acute stress measurement, a galvanic skin response device measured participants’ stress levels before, during, and after the external stressor and evaluations of hospital rooms.
Next, respondents were exposed to 12 hospital room profiles in virtual reality and asked to indicate the extent to which they perceived each of the hospital room scenarios to be restorative. The extent to which the room was restorative to the respondent was measured by two indicators, including physical relaxation and mental clarity. Respondents were asked by an interviewer who entered their responses to a questionairre on an IPad “Please indicate on a scale of 0 to 10, with 0 being not at all and 10 being extremely, the extent to which you feel the room you are seeing now contributes to your sense of feeling relaxed” and “Please indicate on a scale of 0 to 10, with 0 being not at all and 10 being extremely, the extent to which you feel the room you are seeing now helps you to clear your mind of stressful thoughts.” The order in which scenarios were shown was also randomized for each respondent. Participants were assigned to either lower or upper floor level in the hospital randomly. The variation in the viewer's position from lower to upper floor manipulation introduced variation in the amount of sky seen, the height of treeline, grass and pathways, building rooftops and facades which helped to enhance ecological valdiity.
Following evaluation of the hospital rooms, a measurement of sense of presence in virtual reality captured the extent to which participants perceived they felt present in the virtual reality environment on a scale of 1–5, with 0 being not at all and 5 being very strong, which helped gauge whether the scenarioseffectively simulated a real-life hospital room (M = 3.68). Demographics questions included age, income, education, gender, race, and employment were also collected.
Conjoint Analysis
The scores for extent to which the 12 hospital room scenarios were relaxing and helped to clear the mind of stressful thoughts were analyzed using full-profile conjoint analyses. Part-worth estimates indicated the magnitude of the level of each attribute's influence on physical relaxation and ability to clear the mind, in addition to their ranking of importance relative to physical relaxation and mind clearing among the other attributes. Further, to compare the effect of the external stressor inducing an acute level of stress, the data were divided into two separate samples using a cluster analysis procedure on the means of the “extent to which stressful thoughts invaded mind.” Self-reported stress level was validated by galvanic skin response confirming respondents experienced higher or lower peaks in stress from the external stress process. Biometric responses were compared to self-reported cognitive stress scores. Conjoint analysis was conducted for each subsample “more stressful thoughts” and “less stressful thoughts” to understand the differences among the restorative responses associated with hospital room attributes for those with particularly higher levels of acute stress. The conjoint part-worth estimates were assessed for significant differences using pairwise comparison tests.
Results
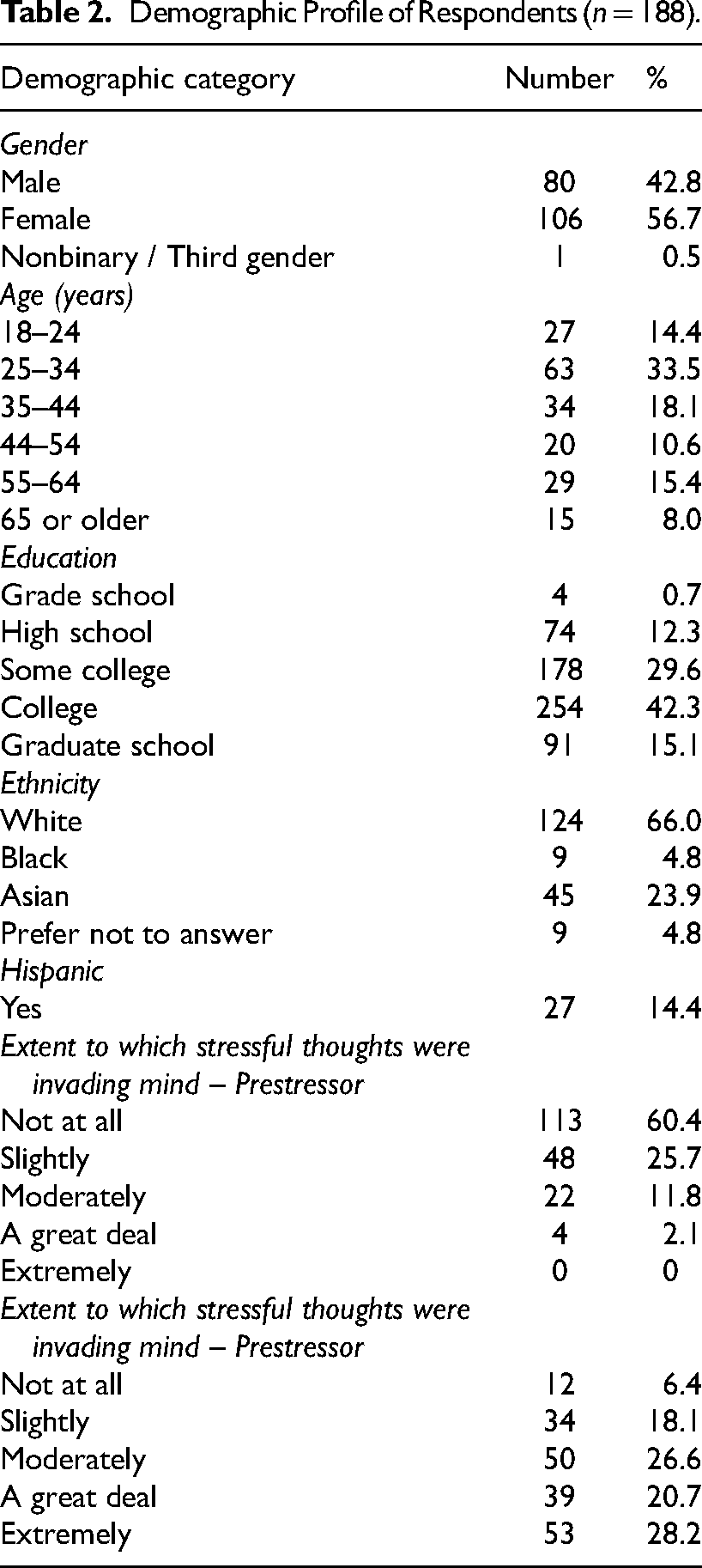
Table 2 includes the demographic information of the sample. Of the 188 participants, (56.7%) were women. Most participants were either 26–34 years old (33.5%) or 35–54 years old (18.1%). Almost half of the participants (45.7%) indicated their income was $60,000 or less. The majority had either a college (42.3%) or graduate school (15.1%) level of education. Most of the participants (66.5%) sustained at least part-time employment; 66.0% of the participants indicated they were White, 5.0% Black, and 24.0% Asian; 14.4% of the sample identified as having a Hispanic background.
Demographic Profile of Respondents (n = 188).
Hospital Room Attributes Contribution to Physical Relaxation and Mental Clarity
Sufficient goodness-of-fit for the conjoint full-profile models was indicated by Pearson's R and Kendall's tau statistic indicated for physical relaxation (.994 and .970, p < .001) and mental clarity (.997 and .970, p < .001), indicating consistent prediction of the set of attribute evaluations for both physical relaxation and mental clarity (Hair et al., 2010). The part-worth utility scores for 12 levels across the six attributes on the extent to which the hospital room contributed to the sense of physical relaxation and the extent to which the hospital room helped clear the mind of stressful thoughts are presented in Table 3. Where a higher positive value indicated that particular attribute level was perceived as contributing more to the overall hospital room's effect on either physical relaxation or mental clarity.
Part-Worth Scores.
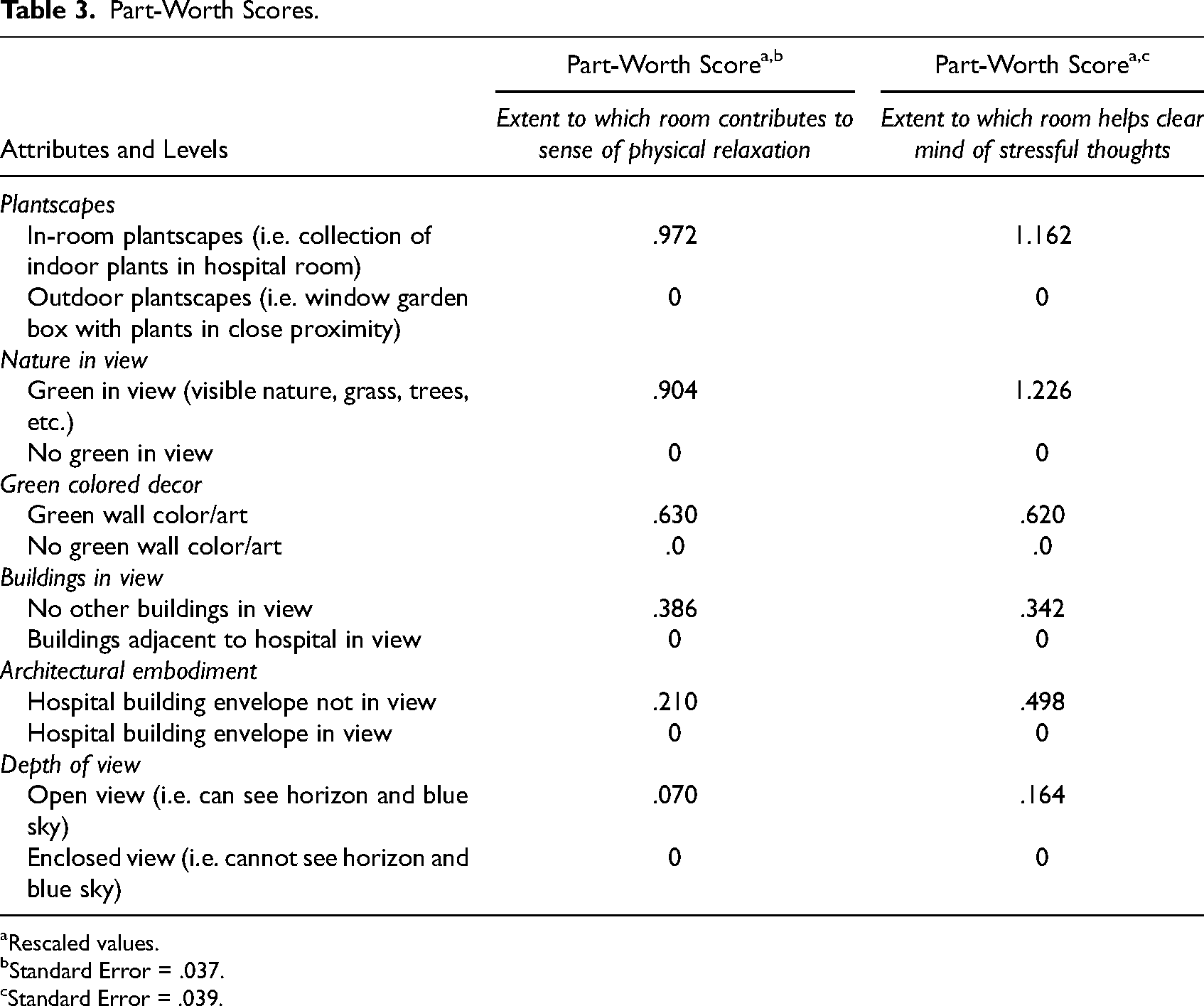
Rescaled values.
Standard Error = .037.
Standard Error = .039.
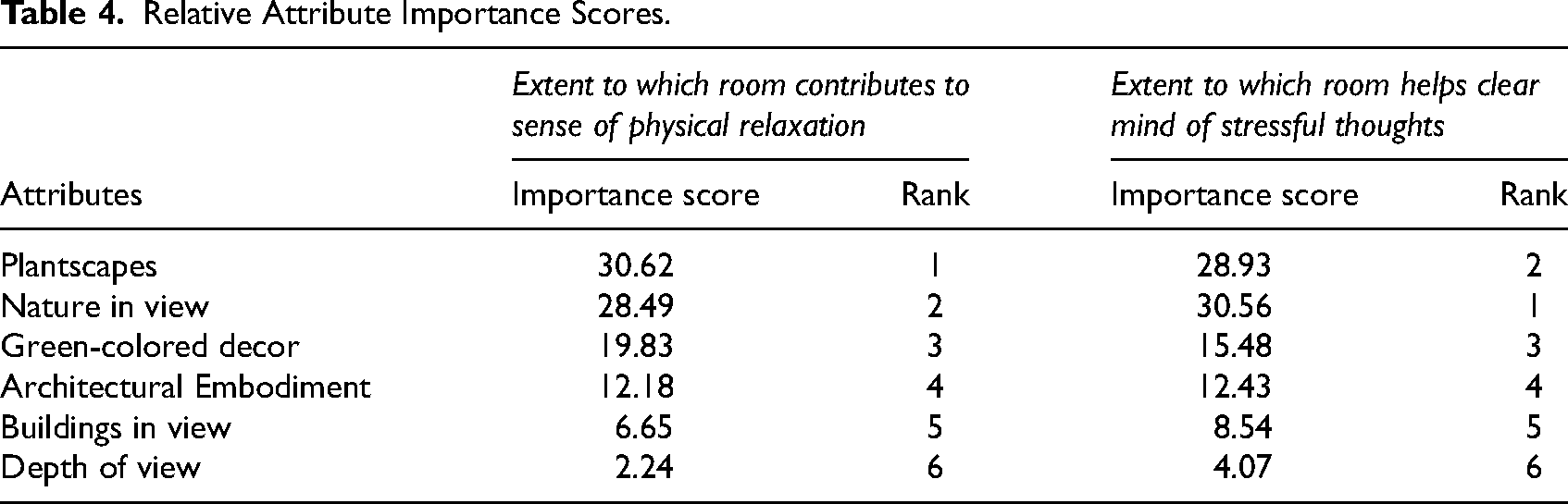
In terms of plantscapes, respondents indicated high physical relaxation utility from the indoor plantscapes (physical relaxation score = .972), followed by green nature in view (physical relaxation score = .904) and green wall color and art (physical relaxation score = .630). Relative to the ability to clear the mind of stressful thoughts, green views of nature from the window had the highest influence on ability to clear their mind (mental clarity score = 1.226), followed by the presence of indoor plants (mental clarity score = 1.162) and green wall décor and art (mental clarity score = .620). The absence of the building envelope in view was strongly preferred over partial view relative to both physical relaxation and mental clarity (mental clarity score = .498). Views unobstructed by adjacent buildings had a higher impact than adjacent buildings visible in the window view (physical relaxation score = .386), and views unobstructed by the building envelope views (physical relaxation score = .210) had higher utility on physical relaxation than a window view with the hospital building envelope creating visible enclosures. Finally, respondents indicated physical relaxation utility associated with a more open view with deeper view to the horizon and visible sky (physical relaxation score = .070) in addition to mental clarity utility from a greater depth of view to horizon with visible sky (mental clarity score = .164). Based on an absolute comparison to interpret utility scores without a fixed scale; attributes were calculated relative to the other attributes in the study. Given scores range from .07 to 1.226, the scores above 1.0 indicate a very strong preference, and that the attributes had more utility in reducing cognitive stress compared to enhancing relaxation (green views of nature = 1.222, presence of indoor plants = 1.162).
Relative Attribute Importance Scores.
Moderating Effect of External Stressor
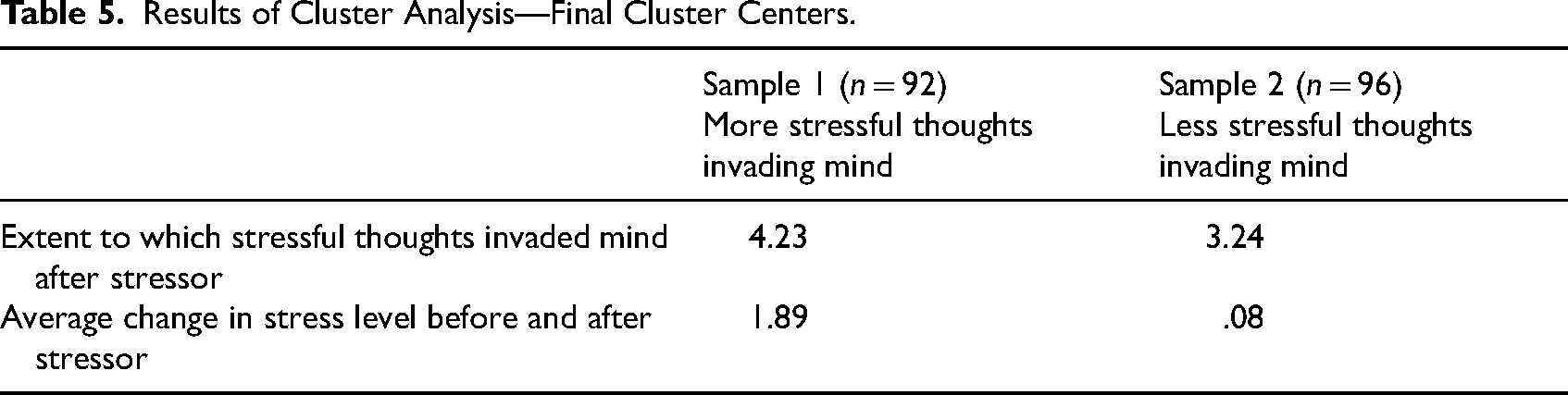
The sample was split into two separate samples on the basis of the extent to which stressful thoughts invaded their mind after viewing the external stressor using a k-means cluster method on the physical responses and self-reported responses. The information regarding the group split is presented in Table 5. The first sample comprised 92 respondents who perceived their mind was invaded by more stressful thoughts (M = 4.23) compared to 96 respondents who had perceived their mind was only somewhat invaded by stressful thoughts (M = 3.24).
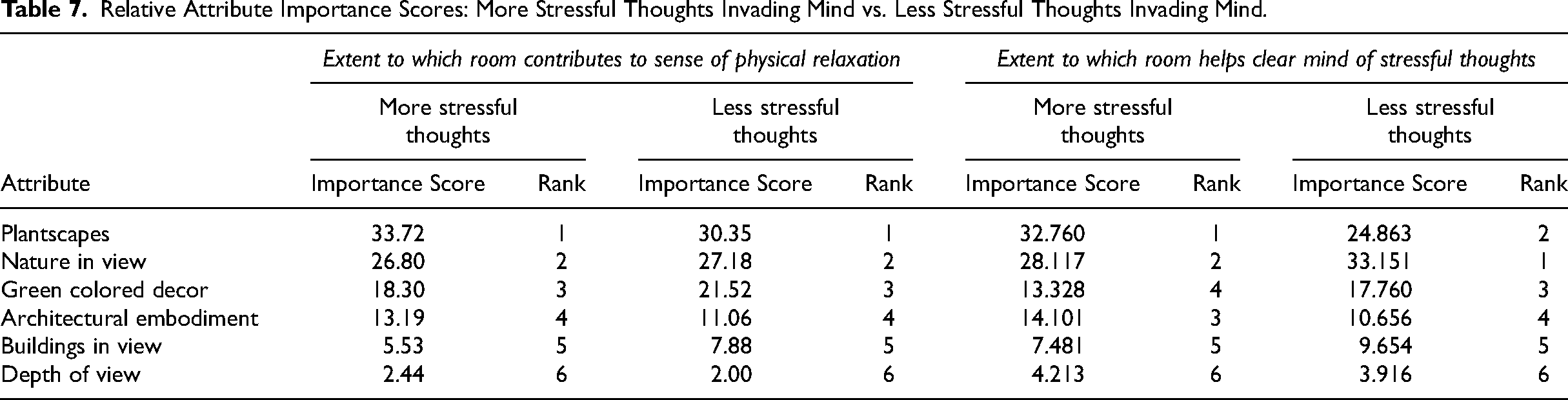
A conjoint analysis was conducted on each group. The values for the Pearson's R and Kendall's tau statistics indicated that the conjoint model demonstrated good fit and consistently predicted restorative evaluations of the attributes in both groups (Hair et al., 2010). “More stressful thoughts invading mind” were .996 and 983 and the “Less stressful thoughts invading mind” .990 and .970, respectively, and significant (p < .001). Table 6 includes rescaled part-worth scores for the 12 levels across the six attributes. Four significant differences were determined by pairwise comparisons on the part-worth score value between the extent to which attributes were perceived to be restorative for the two groups. The group with “more stressful thoughts” (i.e., those who indicated that more stressful thoughts invaded their mind from the external stressor)-had significantly higher physical relaxation scores associated with indoor plants (difference in part-worth score = .346; t = 7.26, p < .001) than those who had less stressful thoughts invading their mind. A view unobstructed by the building envelope was also significantly more important to physical relaxation for those with more stressful thoughts invading their mind (difference in part-worth score = .124; t = 2.29, p < .001). In terms of mental clarity, those with more stressful thoughts invading their mind derived significantly more help in clearing their mind from indoor plants (difference in part-worth score = .117; t = 2.46, p < .001), green nature in view (difference in part-worth score = .233; t = 4.90, p < .001) and a view unobstructed by the building envelope (difference in part-worth score = .188; t = 3.97, p < .001) than those with less stressful thoughts. In addition, the differences in scores are shown in the relative importance scores on physical relaxation or mental clarity of each overall attribute are represented in Table 7. Those who experienced more stressful thoughts most valued the attributes of indoor plants, green views and nature, with higher relative importance scores for mental clarity and physical relaxation on all the attributes, compared to those who were not experiencing stressful thoughts. It is interesting to note that the rankings reflect the overall sample (see Table 3), with a notably higher importance score for green views of nature than indoor plants on the room's contribution to the ability to clear mind from stressful thoughts.
Results of Cluster Analysis—Final Cluster Centers.
Part-Worth Scores: More Stressed vs. Less Stressed
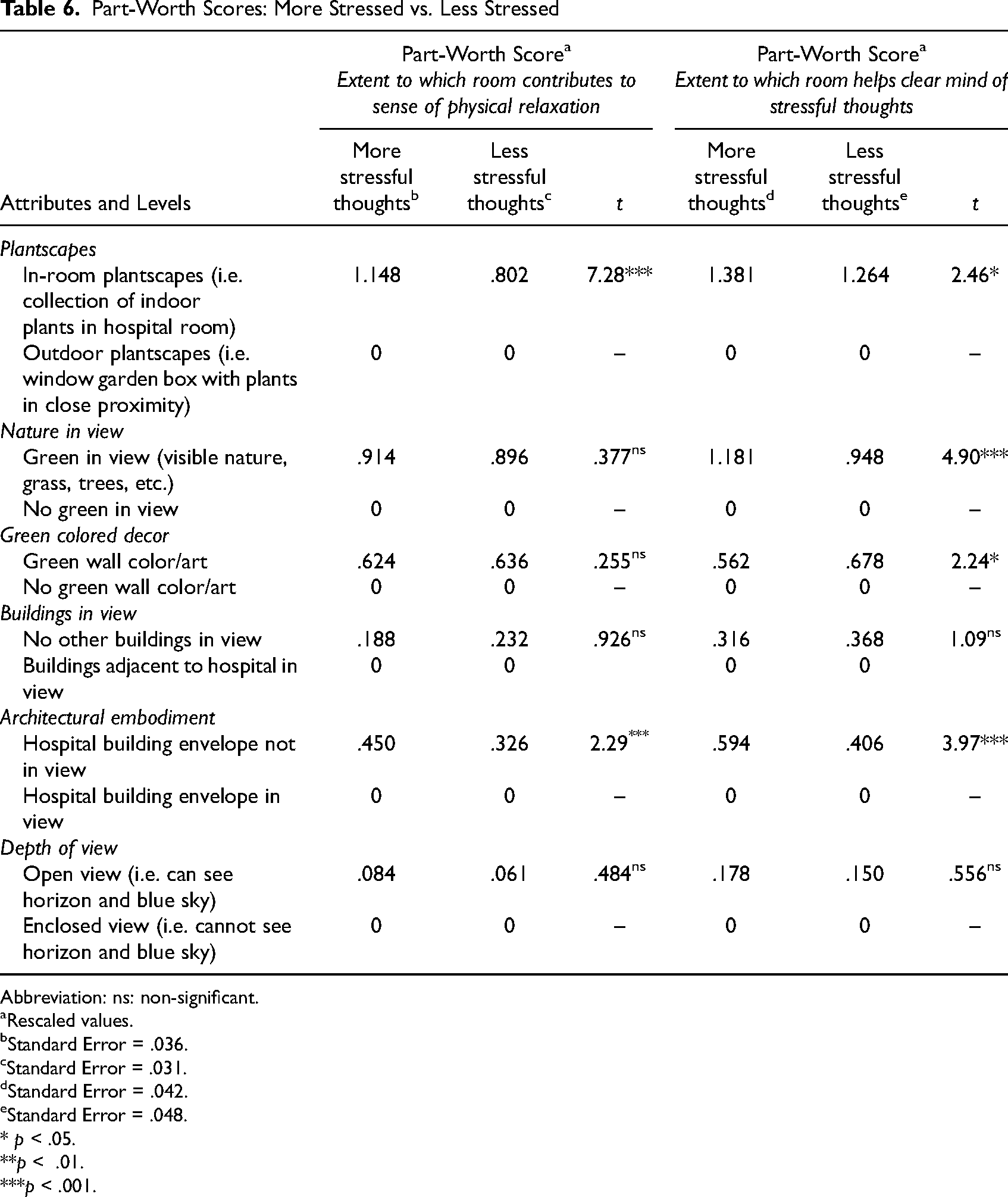
Abbreviation: ns: non-significant.
Rescaled values.
Standard Error = .036.
Standard Error = .031.
Standard Error = .042.
Standard Error = .048.
* p < .05.
**p < .01.
***p < .001.
Relative Attribute Importance Scores: More Stressful Thoughts Invading Mind vs. Less Stressful Thoughts Invading Mind.
Discussion and Conclusion
The findings of the present study contribute to the environmental psychology and evidence-based design literature in the context of restorative hospital rooms. As hospitals and rehabilitation centers increasingly adopt patient-centric environmental design with a focus on biophilic design, there remains a need to holistically test the combined effects of nature and experience of window views on patient convalescence in acute-care hospitals, as well as target specific critical-care patient groups at out-patient care facilities such asmedical hotels (Chesterton et al., 2021), perioperative care (Huzell et al., 2015), rehabilitation (Han & Hyun, 2014), and residential facilities (Park, 2006). In fact, patients with long-term stays in confined settings and with limited mobility have been found to rely heavily on visual and indirect environmental stimuli for psychological relief (Dijkstra et al., 2008; Marcus & Sachs, 2013).
While studies specific to acute-care settings confirm that natural window views and various biophilic design elements positively influence stress reduction, pain perception, and overall well-being (Huisman et al., 2012; Pati et al., 2016; Raanaas et al., 2012, 2016) and literature in the context of healthcare and SRT and PET (e.g., Hartig et al., 2011; Masoudinejad & Hartig, 2020; Van den Berg et al., 2016, Ulrich, 1981, 1984, 1993) provided the basis of the selection of various attributes with restorative qualities including nature in view, sky, building window view content, indoor plants, and green color interior design for this study, it is likely among the first to systematically design multiple attributes into high-resolution photorealistic hospital rooms in virtual reality for simulated acute-care patients to evaluate. The conjoint method allowed for simultaneous testing of individual attributes presented collectively in a holistic room environment. Unlike prior studies that assess these elements using multivariate techniques, this study used an integrated-design and visual approach to examine how 12 combinations of hospital room attributes influence restoration perceptions capturing a larger sample size for an experiment (n = 188). Moreover, the external stressor narrative transportation enhanced ecological validity, ensuring that participants had consistent elevated levels of cognitive stress, to serve as a proxy for actual acute-care hospital patient responses.
Although translating cognitive stress levels to acute-care settings requires careful validation. Research has shown that hospitalized patients in high-stress medical conditions often experience heightened sensitivity to environmental stressors, making the quality of their surroundings even more significant (Huisman et al., 2012; Ulrich, 1984, 2001). Thus, findings from this study that provide insights on hospital design strategies also rely on supporting evidence from the body of healthcare-specific studies and improvements in actual patient recovery experiences.
The integration of attributes into the experimental hospital room scenarios, based on the tenets of SRT and with PRT theoretical perspectives, represents a notable theoretical contribution of the present study. Stress Recovery Theory suggests that natural environments help mitigate stress responses and promote psychological restoration. Prior studies have established that biophilic hospital environments can improve mental well-being, pain perception, and stress reduction (Raanaas et al., 2016; Ulrich, 2008). Restoration, in the PET context, implies that the process of regaining physical and psychological capacitates from natural surroundings is a result of how humans have evolved (Grinde & Patil, 2009). Plants were critical to human survival during the earliest phases of evolutionary history; they served as a food resource, held medicinal properties, provided shelter, refuge from predators, signified seasonal changes and were an important indicator of wayfinding (Ulrich, 1991). As such, most early humans were adapted to live, idealy, in green foliage environments (Grinde & Patil, 2009). Even in typically nonvegetated regional areas, archeologists have found that humans incorporated green-nature elements into the design of their living environments (Lewis, 1996).
In the present study, the provision of indoor plants had the highest importance score compared to other attributes on physical relaxation (30.62) and was even higher for the group of participants reporting the higher levels of stressful thoughts invading their mind (33.72). Plants also had the highest relative importance in helping mental clarity in the group of participants experiencing more stressful thoughts (32.76). The importance, specifically, of plants was also demonstrated by Park and Mattson's (2008) study on the therapeutic benefits of plants to abdominal surgical patients, and Park et al.'s (2004) study on flowers and foliage in a hospital room reducing reported pain levels. Studies by Fjeld (2000), Hall and Knuth (2019), and Han and Ruan (2019) have also found that, in general, plants can reduce stress and anxiety, combat depression, counteract physical discomfort, improve mood, attention, and cognitive performance. Collectively, the findings of these studies and the present study implicate that plants have measurable benefits in a hospital room and are a tangible attribute that can be inexpensively and easily placed in a room for the majority of patients (excluding those in intensive care or with allergen restrictions).
Although the importance of a view of green nature as part of a hospital room's design for patient restoration has been established, it may not be entirely viable for hospitals to provide substantial and pleasant nature views to all patient rooms. The present study emphasizes the need for pragmatic landscape elements that maximize opportunities for views of green nature. A variety of potted plants in the room and plants and flowers in a window box (or gardens on building rooftops and balconies) have been shown in prior research to enhance well-being in the absence of a broader view of natural landscape (Masoudinejad & Hartig, 2020; Peters & Masoudinejad, 2022).
From an interior design standpoint, the findings of the present study confirm the importance of selecting interior design features—green wall color and artwork; particularly green is aesthetically stimulating and symbolic of the color of nature. Green wall décor had the third highest importance score for the participants in the present study reaffirming Thorpert et al. (2023) study on the relaxing effects of green color schemes and Suess and Mody's (2017) finding of colored walls and artwork as significant environmental contributors to perceived physical and mental well-being in hospital room evaluations. While green-colored décor overall had high utility to the sample participants, interestingly, the sub-sample of participants who indicated they had relatively less stressful thoughts seemed to derive slightly higher utility from green wall color and decor. While many studies in the evidence-based design literature have provided support for the findings of the present study regarding the restorative properties of green color and symbolism of verdant nature (Briki & Majed, 2019; Joye & Van den Berg, 2011; Memari et al., 2021), green has also been found to be associated with feelings of nausea and sickness (Kaya & Epps, 2004). More study is needed; there are different kinds of green.
In sum, the present study developed propositions and tested a framework based on the tenets Stress Recovery Theory to assess how simulated acute-care patients evaluate the restorativeness associated with the provision of window views, plantscapes, and green room decor attributes in virtual reality hospital rooms. As an increasing number of hospital planners intentionally design views from hospital rooms and landscape architects and interior designers recommend green nature interventions, the framework can be applied to research testing the patient experience in a hospital room in situ. Given the established relationship between contact with nature and improved patient healing and other clinical outcomes, one can use the model to isolate the effects of the patient experience of architectural attributes of the kind described in this study.
Limitations and Future Research
The framework was developed to test propositions of SRT in the present study as a broad framework of window views, plantscapes, and green-colored décor that can be intentionally designed into a restorative hospital environment. The attributes specified encompassed green nature views and did not discern between nature characteristics and vistas. The density of the nature depicted in the visualizations for the purpose of the present study may not reflect, in general, typical hospital landscaping and surrounding vegetation. The 3D hospital room scenarios were developed for the purpose of evaluating the variables specified and theoretical propositions of the present study. The propositions, conceptual framework, methods, and results provide a foundation upon which future research can build, with further considerations for regional factors and landscape types, building characteristics, and urban density.
The most limiting factor of the present study inherent to the conjoint analysis method was the selection of six attributes. Because participants cannot realistically evaluate more than 20 profiles before becoming fatigued, the number of attributes in a conjoint analysis typically is set to less than 10 (Suess & Mody, 2017). The number of attributes in the present study was restricted to six, within the recommendations for number of attributes by Hair et al. (2010) for a traditional full-profile conjoint analysis. Further, atmospheric features in a hospital room, including nature-based soundtracks and music, bird sounds, animals, soft lighting, and technology/media-based nature stimuli should be included in experimental designs (Harris et al., 2010; Pati et al., 2016; Ratcliffe et al., 2013).
While the present study used virtual reality technology to enhance the visualization and evaluation for the hospital rooms with attributes, future research can potentially utilize more dynamic, higher resolution, and interactive virtual reality environments to review hospital room designs (Browning et al., 2020; Shin et al., 2022; Verzwyvelt et al., 2021). Although studies have evidenced exposure to simulated and virtual natural landscapes and stimuli have influences that are comparable (but of lesser effect) to their actual settings (Browning, Shipley, et al., 2020; Frost et al., 2022; McMahan & Estes, 2015; Yin et al., 2022), future research would benefit from testing patients in actual hospital room contexts. Moreover, testing additional responses with biometric devices that measure more comprehensive physiological and emotional responses and pain reduction could be useful (Ulrich-Lai & Herman, 2009; Van Den Berg & Custers, 2011). It is important to recognize that acute care patients may not respond to environmental stimuli in the same manner as the simulated patients in this study. Although research on nonhospitalized populations offers useful insights into the psychological benefits of nature exposure, applying these findings to acute care settings necessitates thorough validation.
Implications for Practice
Where possible, hospital rooms should be constructed to maximize views of greenspace and unobstructed skylines, in addition to providing an abundance of indoor plants and green-colored décor should be incorporated into hospital rooms.
When indoor plants and views of nature are not possible, plants in window boxes outside the hospital room may offer green in window views and immersion in plants.
Supplemental Material
sj-docx-1-her-10.1177_19375867251344626 - Supplemental material for Understanding the Influence of Window Views, Plantscapes, and Green Décor in Virtual Reality Hospital Rooms on Simulated Acute-Care Patients’ Stress Recovery and Relaxation Responses
Supplemental material, sj-docx-1-her-10.1177_19375867251344626 for Understanding the Influence of Window Views, Plantscapes, and Green Décor in Virtual Reality Hospital Rooms on Simulated Acute-Care Patients’ Stress Recovery and Relaxation Responses by Courtney Suess and Jay Maddock in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
This manuscript is based on the research conducted for Dr. Courtney Suess’ masters’ thesis at the University of Texas at Austin, School of Architecture. Professor Micheal Benedikt is acknowledged for his isovist perspectives related to testing openness and enclosure and overall review and feedback on the design and execution of virtual reality research. Victor Franz Traubman, Jeff Pool, Arpit Shah, and Sarayu Chandramouli are thanked for their technological support and assistance with data collection.
Authors' Note
Courtney Suess is currently affiliated with Cornell Institute for Healthy Futures, Cornell University, Ithaca, NY, USA. Jay Maddock is currently affiliated with Houston Methodist Research Institute, Houston Methodist Hospital, Houston, TX, USA.
Data Availability
Data will be made available by written request to the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Texas A&M University's IRB approved all study procedures.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Presidential Tranformation Grants (T3) at Texas A&M University.
Informed Consent
All participants provided written informed consent prior to participation. Texas A & M University Approved IRB ID: IRB2022-0337D Reference Number: 139137.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.