
Abstract
Nature-based interventions (NBIs) in healthcare settings have the potential to enhance physical and mental wellbeing of patients, healthcare staff, and visitors but are often underutilized. Knowledge about factors influencing effective implementation of NBIs in healthcare settings is scarce. This study aimed to develop a framework for identifying implementation factors relevant to NBIs in hospitals, long-term care facilities for elderly, and rehabilitation centers. A two-round Delphi study was conducted. In the first round, potential implementation factors were identified based on input from 33 experts from the following groups: healthcare managers, landscape designers, nature and health consultants, and healthcare staff. These factors were then supplemented with additional factors identified from previous studies and the Consolidated Framework for Implementation Research (CFIR). In the second round, 21 experts rated the importance of these factors. The items that reached expert consensus were included in the new implementation framework. In the first round, an initial set of 99 implementation factors was identified. Most factors derived from experts and literature were design related. These factors were complemented with factors derived from the CFIR. In the subsequent round, 98 implementation factors were considered important by experts and retained. These factors were incorporated into a new framework, the Green Implementation Framework (GreenIF). The GreenIF provides an overview of factors that contribute to the successful design and implementation of NBIs in healthcare settings and can be used to enhance their usage and maximize their benefits.
Highlights
Nature-Based Interventions (NBIs) in healthcare settings are underused Knowledge about effectively implementing NBIs in healthcare settings may solve utilization issues A Delphi study was used to develop a by experts supported implementation framework for NBIs Key factors to consider during NBIs implementation are included in the new framework
In recent years, Nature-Based Interventions (NBIs; see Box 1 for a definition) have gained increasing recognition for their potential in healthcare settings. NBIs can offer a range of benefits to healthcare staff, patients’, and visitors’ physical and mental well-being (e.g., Din et al., 2023; Yeo et al., 2019). Studies have, for example, shown that gardens in healthcare settings can contribute to improvements in emotional exhaustion in nurses (Cordoza et al., 2018) or improvements in quality of life and reductions in agitation and depression in residents with dementia (Edwards et al., 2013).This paper focuses on three healthcare settings: hospitals, long-term care facilities for elderly, and rehabilitation centers.
While NBIs in healthcare settings hold great promise, their practical implementation has encountered numerous challenges. Reported challenges hindering the use of NBIs have included limited accessibility (Tseung et al., 2022; Weerasuriya et al., 2019), safety concerns (Idris et al., 2021; Shi et al., 2019), uncomfortable seating (Blaschke et al., 2017; Idris et al., 2021; Tseung et al., 2022) and a lack of resources and staff support (Blaschke et al., 2017; Bray et al., 2022; Evans et al., 2019). Addressing these challenges can enhance the utilization of NBI in healthcare settings. However, there may be a range of other factors that influence the effective utilization of NBIs in healthcare settings.
Research on the evaluation and enhancement of NBI utilization has predominantly concentrated on the design aspect of NBIs (Cervinka et al., 2014; Cohenmansfield, 2007; Cutler & Kane, 2006; Davis, 2011; Gonzalez & Kirkevold, 2016; Heath & Gifford, 2001; Jaffe, 2020; Jiang et al., 2018; Senes et al., 2012). However, the field of implementation science, which focuses on gaining a better understanding of utilization challenges, has shown that the success of interventions in healthcare relies on identifying and addressing a range of factors that might affect their utilization (Bauer & Kirchner, 2020). Besides design-related aspects, also implementation barriers and facilitators pertaining to the context, users, and implementation processes need to be identified (Damschroder et al., 2022). Implementing strategies should be developed that effectively address implementation barriers while reinforcing facilitators (Bauer & Kirchner, 2020).
Thus far, only a limited number of studies have specifically addressed the implementation of NBIs in healthcare settings (Steensma et al., 2025). They have focused, for instance, on identifying barriers and facilitators of an NBI (Bray et al., 2022; Buist et al., 2018), developing and testing a training program to enhance the implementation of an NBI in practice (Chapman et al., 2007), and evaluating an NBI and extracting learning lessons from the implementation process (van der Velde-van Buuringen et al., 2021). While the studies discuss implementation, only one of these studies (Buist et al., 2018) incorporated knowledge derived from implementation science theories, models, or frameworks to guide their approach. Consequently, these studies may have overlooked key factors or missed important implementation steps, which can impede intervention success.
In conclusion, there is limited knowledge available about factors influencing the implementation of NBIs in healthcare settings, which may negatively impact their utilization and integration, and ultimately successful implementation into healthcare practices.
To address this gap, we aimed to acquire a more profound understanding of the factors influencing NBI implementation in healthcare settings by consulting experts with practical experience in both developing and implementing NBIs within healthcare settings using the Delphi method (Okoli & Pawlowski, 2004). The objective of this study was to develop a framework for identifying implementation factors relevant to NBIs in hospitals, long-term care facilities for elderly, and rehabilitation centers.
This framework can support future implementation research and help users identify context-specific factors, assess the current status of an NBI's implementation, and determine which aspects require further attention. Such a framework has the potential to strengthen the adoption of NBIs in healthcare practice.
Concepts and Definitions
We define NBIs in healthcare settings as intentional initiatives that engage patients, residents, healthcare staff, and visitors with real nature to promote health, well-being, and enhance the quality of care (World Health Organization, 2017; Shanahan et al., 2019). More specifically, NBIs encompass initiatives, strategies, or programs ranging from integrating nature—such as gardens, living walls, plants, flowers, or water features—into the in-or outdoor environment to therapeutic, care, and other work-related practices that engage users with nature (Shanahan et al., 2019).
NBIs can be used actively, where users have “intentional, direct, and tactile interaction with real forms of nature”, and passively, where they “can observe forms of real nature, without influencing or manipulating them” (Yeo et al., 2019, p. 188).
Implementation is defined as “the process of putting to use or integrating evidence-based interventions within a setting” (Rabin et al., 2008, p. 118). An implementation process is considered to contain the following stages: development, communication, exploration, installation, operation, and sustainable integration and use in practice (Moullin et al., 2015).
Implementation domains are groups or levels that influence implementation outcomes (Moullin et al., 2015; Nilsen, 2020). Following the Consolidated Framework of Implementation Research (CFIR) (Damschroder et al., 2009; Damschroder et al., 2022), five primary domains are considered: (a) Innovation domain, (b) Outer setting domain, (c) Inner setting domain, (d) Individuals domain, and (e) Implementation process domain as the main domains related to implementation.
Implementation Factors
Implementation factors are defined as variables that can positively (i.e., facilitators) or negatively (i.e., barriers) affect the implementation process or directly influence the use of NBIs (S. A. Flottorp et al., 2013). Identifying these factors in relation to both the intervention and its context enables the selection of tailored implementation strategies.
Implementation strategies are specific approaches designed to address identified implementation factors and facilitate the successful adoption and integration of interventions (Moullin et al., 2015).
A distinction can be made between:
The intervention itself, which is the “product” that remains in use after implementation. For NBIs, this could involve the physical intervention (e.g., green elements, green spaces, gardens) or activities that make use of green elements or are conducted within green spaces (e.g., horticultural therapy or work meetings). The implementation process, which refers to the steps and strategies used to introduce the intervention, ending once implementation is complete (Damschroder et al., 2022).
Method
Study Design
We employed a two-round Delphi study. The design of this study was approved by the ethical committee of the Faculty of Behavioral and Movement Sciences (VCWE-2021-058). Delphi is a method characterized using a series of questionnaires in which experts are asked for their opinion on a certain issue, aiming to clarify positions and delineate differences between experts (Barrett & Heale, 2020; Gustafson et al., 1986). This technique is often applied in areas where knowledge is uncertain or imperfect (Kaynak & Macaulay, 1984). As there is limited scientific evidence available about the factors important for the implementation of NBIs in healthcare settings, we used the Delphi method to first collect all potential factors and then examine consensus among experts for the inclusion of these factors in the new implementation framework. The study design and process are visually presented in Figure 1.
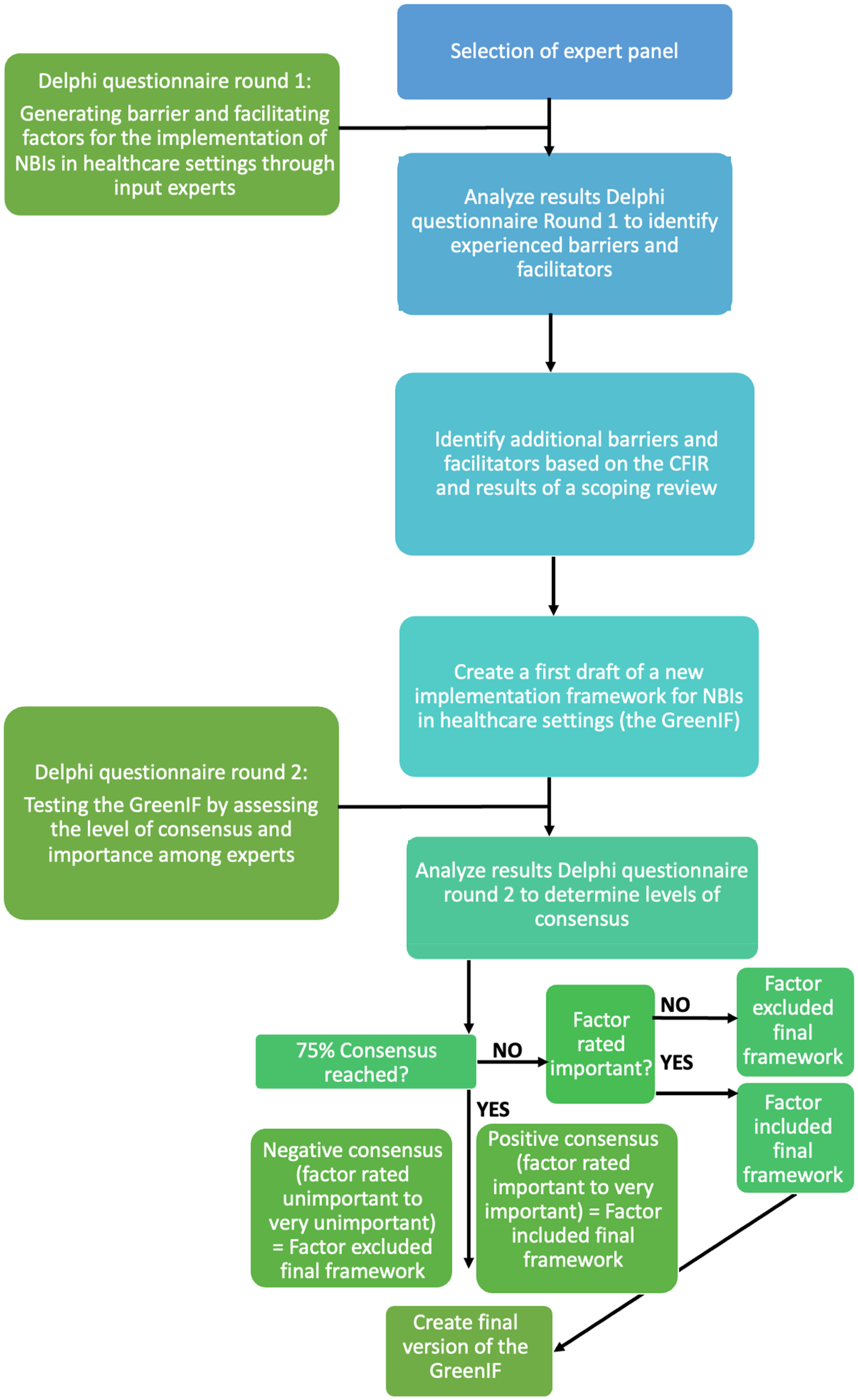
Study overview. Note. NBIs = Nature-Based Interventions; CFIR = The Consolidated Framework for Implementation Research (Damschroder et al., 2009), Scoping Review (Steensma et al., 2025).
Selection and Recruitment of the Delphi Panel
Our first step in the selection of the Delphi panel was to identify Dutch experts involved in the implementation of NBIs in hospitals, long-term care facilities for elderly, and rehabilitation centers where patients and residents are admitted or stay primarily because they require physical medical care. Experts that worked in healthcare settings providing care for mental health, psychiatric care, individuals with intellectual disabilities, palliative care, or those living at home, partially independently, or only attending day care were not included. This decision was made because the primary healthcare needs of patients/residents in these excluded settings can deviate significantly from the focus of the chosen healthcare settings in our study. Five key expert groups in these settings were identified: (a) managers in healthcare settings (e.g., healthcare managers, project leaders, unit leaders, and facility managers), (b) healthcare professionals, (c) patients/residents from healthcare settings, (d) landscape designers, and (e) nature and health advisors. Given that expert panels typically consist of five to 10 participants per group (de Villiers et al., 2005), we aimed to include a minimum of 30 participants, ensuring at least five individuals in identified expert group. Additionally, experts had to meet the following inclusion criteria (a) have knowledge about and experience with the implementation of NBIs in healthcare settings in the Netherlands, and (b) be able to provide relevant input on this topic.
From January 2021 to July 2021, experts were recruited by telephone or e-mail through purposive sampling (Gray, 2021). This Delphi study is part of a larger nationwide project with partners from (applied) universities, the healthcare sector and the green industry, which has the goal of improving the utilization of NBIs in healthcare environments. Therefore, first, partners of the research project were contacted since they are all experts in this field. Second, potential experts were recruited by contacting healthcare settings that implemented an NBI in recent years. Third, experts were recruited through the snowball sampling technique (Gray, 2021), in which experts were requested to recommend other potential experts to the researchers.
To promote patient/resident involvement, healthcare professionals were also requested to assist in distributing the questionnaire to patients or residents who had been involved in implementation efforts. Additionally, they were asked to support patients in accessing the online questionnaire, getting started, and providing guidance if needed.
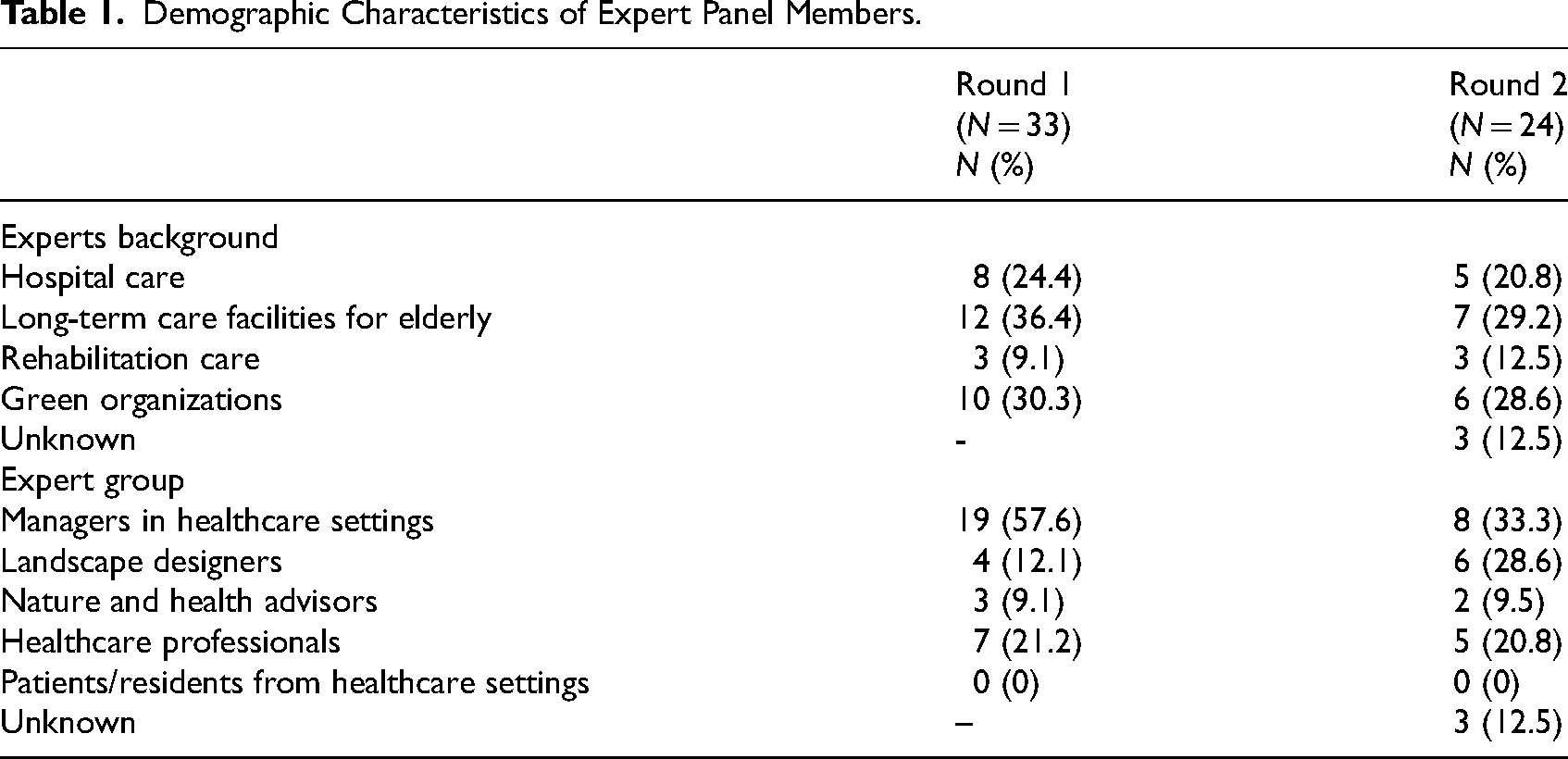
A total of 54 potential experts were identified and invited via email to participate in the questionnaires of the first and second Delphi round. In Round 1, 33 experts participated, resulting in a response rate of 61%. In Round 2, 24 experts participated, resulting in a response rate of 44.4%. In both rounds, respondents represented four different expert groups, with managers of healthcare settings being the predominant representation in both rounds (Table 1). Most participants worked in elderly care and had experience with the implementation and execution of an outdoor NBI. No patients or residents were recruited in this study because experts did not identify patients or residents with experience in implementing NBIs. Not all experts participated in both rounds. For example, in Round 2 there were nine experts who did not participate in Round 1.
Demographic Characteristics of Expert Panel Members.
Delphi Round 1: Generating Implementation Factors
Following a classic Delphi structure (Keeney et al., 2001; Okoli & Pawlowski, 2004), the first Delphi round was used to generate a first list of barriers and facilitating factors. In this round, experts were asked a series of open-ended questions to gain insights into barriers and facilitators to the implementation of NBIs in healthcare settings. This open approach was used to encourage the panel to generate as many ideas, concepts, and factors as possible based on their own experiences and knowledge, without the risk of potential influence from other sources.
Questionnaire Round 1
The first Delphi questionnaire was distributed between March and April 2021. It started with information about the study and included an online informed consent form. After giving informed consent, participants were asked about their occupation and the healthcare setting in which they worked, stayed, or lived. To ensure a shared understanding of the terminology used in the study, participants were then provided with an accompanying document that clarified the concepts of NBIs and implementation (see Appendix 2). After reading this document, participants were asked to describe the NBI they were involved in and what they experienced as barriers and facilitators to the implementation and use of NBI in healthcare settings. After describing the barriers and facilitators, experts could provide a qualitative response to further explain their suggestions.
Analysis Round 1
The responses of Delphi Round 1 were thematically analyzed using the approach of (Braun & Clarke, 2006). This was done independently by two researchers (RS and WM). First, the researchers familiarized themselves with the data by reading and re-reading the answers given by experts. Second, each researcher independently coded each answer and labeled each as a barrier, facilitating or neutral factor. Next, the researchers utilized the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2009) to systematically organize the coded factors. The CFIR is a widely utilized framework in implementation research and frequently applied to support implementation processes in healthcare settings (Kirk et al., 2016). The CFIR is designed to identify potential barriers and facilitating factors that may influence the success of an implementation. It comprises five domains: the intervention itself, the outer setting, the inner setting, the individuals involved, and the implementation process. Within these domains, implementation factors are categorized into constructs and subconstructs. The CFIR provides valuable insights that support tailoring implementation strategies, identifying necessary adaptations, and effectively interpreting implementation outcomes (Damschroder et al., 2022; Nilsen, 2020). For this analysis, we deductively grouped each code under thematic categories, facilitating a systematic comparison of these themes with the CFIR's domains, constructs, subconstructs, and related factors.
By incorporating this framework into this stage of the analysis, we aimed to prevent unintentionally overlooking implementation factors indicated by experts, and we aimed to identify potential new NBI-specific factors not addressed by the CFIR. During the deductive analysis, the research team (JM, RS, WM) discussed the analyzing process and the data multiple times. When disagreements arose among researchers, codes and themes were debated until a consensus was reached. If a code did not fit into any of the CFIR (sub)constructs, a new (sub)construct was created. Finally, a first list of summarized (sub)constructs and related factors was created.
Identifying Additional Barriers and Facilitators
Between Delphi Round 1 and 2, the list of barriers and facilitators resulting from Round 1 was complemented. This expansion included factors from the CFIR that were not explicitly mentioned by experts in Round 1, along with preliminary findings from a scoping review on implementation barriers and facilitators for NBIs in hospitals, long-term care facilities for elderly, and rehabilitation centers (Steensma et al., 2025). This led to the initial version of an implementation framework, titled the Green Implementation Framework (GreenIF). This framework included all barriers and facilitators identified by experts during the Delphi Round 1, the literature on NBIs (scoping review) and the CFIR. This first version served as input for Delphi Round 2.
Delphi Round 2: Validation of the First Draft of the NBI Implementation Framework
In Delphi Round 2, we aimed to investigate to what extent the factors integrated into the first version of the GreenIF were perceived by the panel as important for the implementation of NBIs in healthcare settings. In this round, the results from the first round were aggregated across all expert groups. Participants were then asked to review whether their input from Round 1 had been accurately incorporated into the list of factors. This process functioned as an indirect member check, enabling us to validate the accuracy and completeness of our analysis, thereby enhancing the overall validity of the research (Creswell & Creswell, 2017).
Delphi Questionnaire Round 2
The questionnaire of Delphi Round 2 was sent by email to the panel in July 2021. Like Round 1, the questionnaire started with an information letter, informed consent, demographic information, and information about the terminology. The first version of the new implementation framework was used as the starting point for the remainder of the questionnaire. The panel was asked to rate on a five-point Likert scale (not important at all—very important) how important each individual item in the framework was to the implementation of NBIs in healthcare settings. For each factor, the experts were asked to substantiate their answer in a textbox. By asking participants to substantiate, we aimed to offer deeper insights into the diverse perspectives and contextual nuances associated with the factors being examined.
Analysis Round 2
The data of Delphi Round 2 were analyzed on a quantitative and qualitative manner. First, the relative importance of factors was calculated based on the median scores of the responses of the experts. Only if the median importance score was ≥4 the factor was considered as important. Additionally, the interquartile range (IQR) was calculated to give further insight into the variability of the expert ratings. Consensus was set at 75%. Meaning that if ≥75% of the panel rated the item as “important” or “very important” on the five-point Likert scale, it was considered an item on which the panel agreed. A factor was included in the final framework when consensus was ≥75% and the median score ≥4. If an item did not reach the 75% consensus, but did have a median score ≥4, it was still included in the final framework along with a brief summary of expert explanations. The expert's substantiations were utilized to provide more insight into the diverse perspectives and contextual nuances associated with the factors where the experts lacked consensus (see Appendix 3). This approach aimed to clarify the reasons behind the absence of consensus and can provide more insights into what to consider during the implementation when utilizing the framework. If an item did not reach consensus (<75%) and had a median score ≤3, it was removed from the framework.
Results
Delphi Round 1
In Round 1, 33 experts generated a total of 236 suggestions for factors important for the implementation of NBIs in healthcare settings. After merging duplicate suggestions, 198 unique suggestions were identified, including 155 suggestions for facilitators and 43 for barriers (Appendix 1). Many suggestions were similar in content and could be combined into factors.
The 198 suggestions were summarized into 62 separate factors. Twenty-two of these factors could be directly classified to the five existing domains and related (sub)constructs and factors of the CFIR (Damschroder et al., 2009). The remaining 40 factors could not be directly translated to the original CFIR (sub)constructs as they were unique to the NBI. They were therefore added as new factors under new (sub)constructs to the CFIR to create the implementation framework for NBI in healthcare settings. Seven new constructs were created: Activities and Use, Maintenance, Vision, Plan, Goals, Design, and Continuity and Sustainability. In addition, 10 new subconstructs were created under the existing CFIR construct “Design Quality and Packaging.”
In terms of content, a significant portion of the factors mentioned by experts related to (fostering) stakeholder support by, for instance, providing (scientific) knowledge about the significance of the NBI and involving stakeholders early in the implementation process. Additionally, various design-related recommendations and practical considerations were highlighted, such as the importance of making an NBI accessible and ensuring proper maintenance and creating a replacement plan that takes into account possible turnover of volunteers. In addition, experts highlighted aspects related to the implementation process. For example, they mentioned specific examples of models that can be used to evaluate NBIs and stressed the importance of developing a clear vision for NBIs.
Integration of Additional Barriers and Facilitators
The integration of factors derived from the CFIR, expert input In Delphi Round 1, and relevant literature has culminated in the development of a first version of the implementation framework, hereafter referred to as the GreenIF. This first version of the framework comprises 99 discrete implementation factors, categorized into 5 domains, 32 constructs, and 19 subconstructs. Among these, 7 constructs, 10 subconstructs, and 51 factors were not present in the original CFIR and were newly added. The remaining new constructs, subconstructs, and other factors thus emerged from a combined input of experts and literature. Of these, 3 subconstructs and 14 factors were exclusively from experts and 2 subconstructs and 11 factors were exclusively from the literature. For an overview of factors and their corresponding sources, please refer to Appendix 1.
Results Delphi Round 2
In Round 2, 24 experts rated the level of importance of 99 implementation factors included in the first version of the GreenIF. Table 2 shows all 99 factors and their rated importance, the IQR and consensus. The experts rated 98 out of the 99 suggested implementation factors as important (median score ≥4). Of these 98 important factors, 88 factors also reached positive consensus (≥75%). Hence, 10 factors were rated as important, but did not reach consensus (<75%). Given their perceived importance, these factors were retained in the framework (Figure 1). Appendix 3 provides a summary of the experts’ substantiations for the items for which consensus was not reached.
The GreenIF: Overview of Factors Important for Implementing Nature-Based Interventions in Healthcare Settings.

Note. NBIs = nature-based interventions, CFIR = The Consolidated Framework for Implementation Research (Damschroder et al., 2009).
 Full consensus 100%
Full consensus 100%
 Consensus ≥75%
Consensus ≥75%
 No consensus <75%
No consensus <75%
 No consensus <75% and low importance ≤3
No consensus <75% and low importance ≤3
Factor 59: “there are reward systems within the organization that promote the implementation and use of the NBI” was rated as unimportant and did not reach consensus and was, therefore, omitted from the framework. Consequently, the final version of the GreenIF comprised out of 98 factors. Below we summarize per domain which construct and subconstructs are included in the GreenIF (Figure 2).
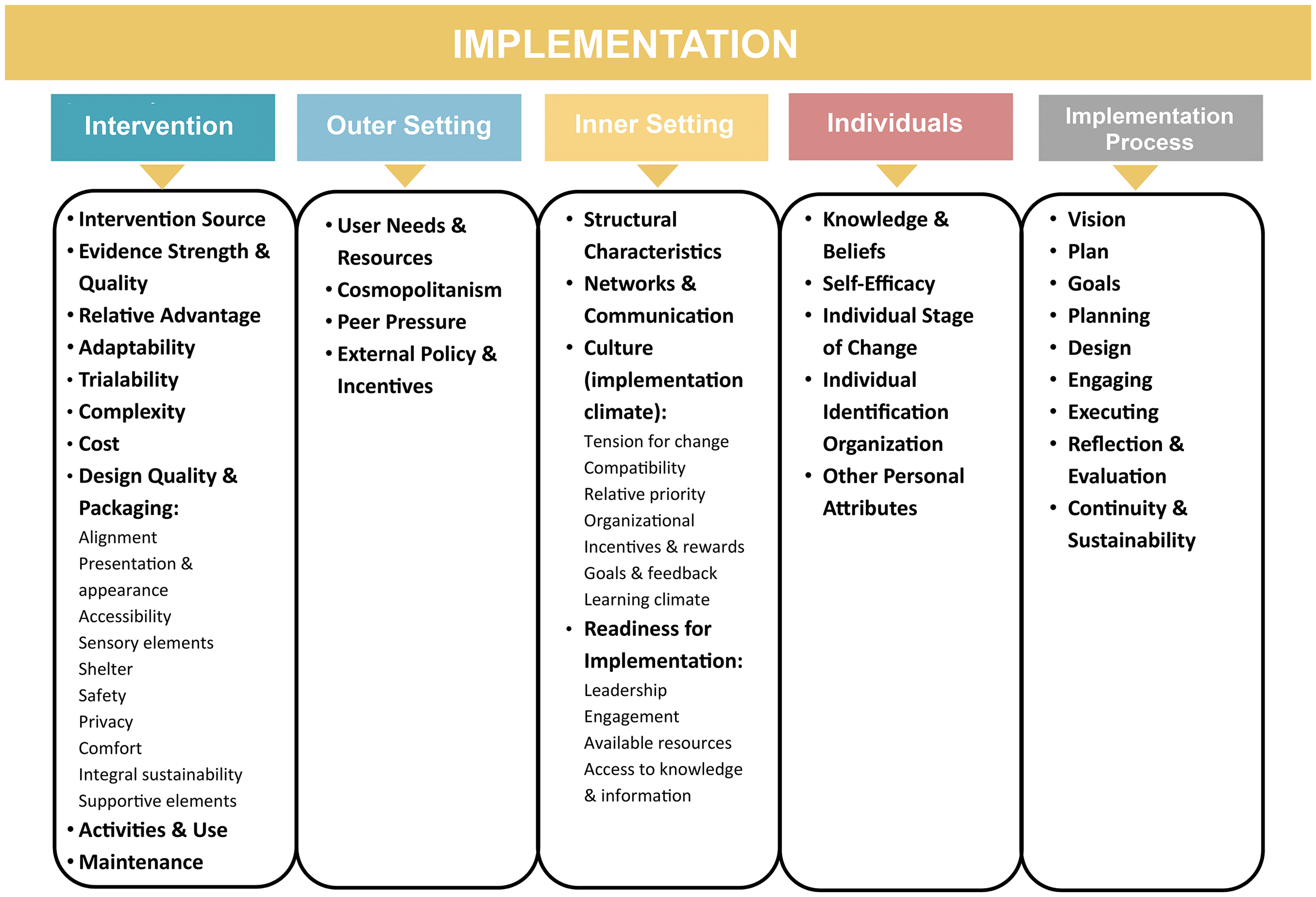
Domains included in the GreenIF.
Discussion
The objective of this study was to get an overview of barriers and facilitators relevant to the implementation of NBIs in hospitals, long-term care facilities for elderly, and rehabilitation centers, to provide content for a comprehensive implementation framework for NBIs, the GreenIF. This framework can support future implementation research and practice by helping identify relevant implementation factors, enabling the selection, tailoring, execution, evaluation, and optimization of effective implementation strategies. Utilizing a two-round Delphi study, information from previous studies on implementation factors for NBIs in healthcare settings, and the CFIR (Damschroder et al., 2009), an overview of 98 factors grouped into 5 domains important for the implementation of NBIs in healthcare settings was developed and included into the GreenIF.
Results of Round 2 revealed that the experts collectively scored most suggested implementation factors in the first version of the GreenIF as important. These findings indicate that the experts generally recognize the importance of a variety of factors. It also suggests that the GreenIF is well-supported by experts in the field and, thus, its intended users. The GreenIF serves as a valuable extension to the original CFIR tool by Damschroder et al. (2009), as it integrates additional factors drawn from both the practical expertise of experts and literature collected from diverse studies. While the CFIR provides essential general guidelines for implementing general healthcare interventions, the GreenIF offers more in-depth insights into specific factors relevant for NBIs.
The input from experts appeared to be important for the creation of the GreenIF. Experts identified elements that contribute to successful implementation of NBIs that were not mentioned in CFIR or literature. Factors put forward by experts, which were not mentioned in the existing CFIR and therefore are additional, often related to the design, the implementation process and other practical aspects. This underscores how experts, drawing from their experience with NBIs in healthcare settings can contribute additional value to existing implementation knowledge. Interestingly, the experts also emphasized the importance of using sustainable materials to promote sustainable implementation and to promote biodiversity. This aspect did not appear in either the CFIR (Damschroder et al., 2009) or the literature. We believe that, especially given the current issues related to climate change (Masson-Delmotte et al., 2021), this factor is a valuable addition to the new framework.
Experts did not mention a part of the CFIR factors in the first round but later acknowledged their importance in the second round when these were presented in the framework. This suggests that certain factors may not immediately come to mind when considering implementing NBIs. This highlights a potential lack of initial awareness regarding the full spectrum of implementation factors, underscoring the value of using CFIR as a foundational input for this study. The newly developed implementation framework aims to address this lack of awareness by highlighting potentially important factors for the implementation of NBIs in healthcare.
Strengths and Limitations
A strength of this study is that it is the first that developed and evaluated an implementation framework (the GreenIF) specifically tailored for implementing NBIs in healthcare settings. The framework goes beyond general implementation frameworks such as the CFIR by providing more in-depth insights into factors drawn from experts and the literature that are particularly relevant for NBIs. These insights, especially those regarding the design and process of implementing NBIs, enhance its practical applicability. As a result, the GreenIF aligns more closely with the specific implementation needs of NBIs in healthcare settings compared to the CFIR alone. Besides the importance of experts' practical experience and knowledge in tailoring the framework to NBIs within healthcare settings, their input and validation of this framework are fundamental. Research has shown that non-academic professionals are more likely to use scientific knowledge in their work and policies when they are actively involved in creating that knowledge (Huzzard, 2021). This is particularly important because the utilization of implementation knowledge seems to be primarily limited to researchers rather than the individuals who need to apply it in practice (Westerlund et al., 2019). This aspect is addressed for this specific framework by the involvement of experts in its development, enhancing its practical applicability in real-world settings. However, further research is needed to evaluate the GreenIF in real-world settings, focusing on its effectiveness, refining its components, and assessing its user-friendliness. Such initiatives will help establish the frameworks validity and demonstrate its broader applicability.
Another strength of this study is the inclusion of multiple expert groups, which provided insights into factors relevant to diverse contexts and types of NBIs. This approach ensures that the framework can be broadly applied to identify implementation factors across a wide range of applications. This also means that not all factors within the framework will be relevant in every specific situation. For instance, the type of NBI (see Textbox 1) influences the level of user involvement and the behavioral changes required for its use, which, in turn, determine the relevance of certain factors and the complexity of implementation efforts needed. Interventions intended for more passive use such as incorporating plants or views of nature, may involve fewer factors and therefore implementation efforts may be less extensive. Nevertheless, factors such as user-centered design, organizational resources, and a clear maintenance plan remain important. For interventions designed for active use, such as therapeutic activities in nature, these factors continue to be important. However, other factors—such as stakeholder involvement, activity coordination, and knowledge in effectively integrating NBIs into work tasks—become increasingly significant. By providing a comprehensive overview of potentially important factors, the framework allows users to identify those most critical for their specific context and needs, which is similar to the flexibility provided by the CFIR. Providing such an extensive list is particularly beneficial for users who may not initially recognize which factors require attention. This approach broadens their understanding of potential considerations and supports the development of implementation strategies that are well-suited to their unique context, enhancing the likelihood of successful integration into practice.
A limitation of our study is the absence of patient participation and the involvement of only three experts from rehabilitation centers in the Delphi rounds. Although factors from their perspectives were incorporated into the framework based on literature, their direct input is still missing. To further develop the framework, it is important for these expert groups to provide their insights on the included factors and potentially suggest new ones.
Another limitation of our study is the number of rounds employed to develop the content of the framework. While a substantial portion of the framework underwent thorough review and evaluation by experts in Round 2, a valuable enhancement to our study could have involved having experts re-assess the final version. This would focus on seeking more clarity on factors where consensus was lacking and on the extent to which the framework aligns with their preferences. We opted not to pursue this additional step to prevent imposing unnecessary time commitments on the experts. Therefore, we do not consider this version of the framework as the final product, especially because we believe that testing the framework during the implementation of NBIs in real-world settings is necessary for its refinement.
Implications
The GreenIF can be used by multiple stakeholders for different purposes. The framework can be useful for supporting researchers in the design, monitoring, and evaluation of implementation studies as it allows for a more detailed investigation of the impact of context-specific implementation factors and corresponding strategies on the enhancement of usage. The framework can be used in healthcare practice by healthcare managers, decision-makers, policymakers, healthcare designers, green designers, healthcare professionals to inform and evaluate the design, and implementation processes of NBIs in healthcare settings. The framework can facilitate conversations among multiple stakeholders about the current implementation context and raises awareness of potential challenges.
The framework can also be included in various stages of implementation. During the pre-implementation phase, it can be used to identify key barriers, facilitators, and select corresponding implementation strategies. In the implementation phase, the framework can be used as a base for an implementation plan, where identified factors could be elaborated into context-specific implementation strategies, related task assignments, and schedules. In the post-implementation phase, strategies can be evaluated and optimized, and the framework can be reapplied to identify remaining factors that require attention. One could also specifically examine the extent to which usage improves when focusing on context-specific implementation factors and related implementation strategies. Moreover, the framework could also be employed in evaluating existing interventions to examine whether differences in the utilization of existing NBIs can be explained by the implementation factors.
A limitation of implementation frameworks, and thus also of the GreenIF, is that they do not facilitate the implementation process step by step (Westerlund et al., 2019), and do not offer guidance on the methodologies required (Lyon & Koerner, 2016). Therefore, we believe that this framework, when used in isolation, may not be the ultimate total solution for implementing NBIs in the healthcare environment but can be used to support the process.
Future Directions
The GreenIF provides a comprehensive overview of implementation factors. However, we believe that a potential step in the refinement of the GreenIF could be to test the usability of this framework within various contexts in combination with a structured implementation approach. This includes assessing the applicability of its factors in other healthcare settings. Although we think many of the factors in the framework could still be relevant to other healthcare settings, it remains important to validate them in practice. Such studies will provide evidence of the framework's validity and broader applicability.
To enhance the practical application of the GreenIF, the framework could be further developed into an interactive tool. For example, incorporating features that guide users through the factors and, akin to the approach by S. Flottorp et al. (2013), allow them to indicate the extent to which each factor has been properly addressed and identify those requiring further attention. Based on this input, such tool could generate a prioritized list of barriers, enabling users to focus on critical areas and take actionable steps.
To further enhance the applicability of the GreenIF, a feature could be integrated that links identified barriers to relevant implementation strategies, enabling users to develop comprehensive implementation plans. A similar feature already exists for the CFIR—the Expert Recommendations for Implementing Change (ERIC) match tool. However, as the authors themselves note, it should be used with caution due to the lack of consensus on the best strategies for specific factors (Waltz et al., 2019). Further implementation research could be helpful to improve our understanding of effective strategies specifically tailored to implementing NBIs in healthcare settings. and enrich the current offerings of the GreenIF.
Conclusion
The GreenIF is a new step in advancing the professionalization of implementing NBIs in healthcare settings. It brings together knowledge from Dutch experts, literature, and an existing implementation framework into a comprehensive overview of factors that could play a critical role in successful implementation of NBI in healthcare settings. While further refinement remains important, this framework can be used in healthcare, in policy and design practices and by researchers to inform and evaluate design and implementation processes, ultimately optimizing the implementation, use and benefits of NBIs. Thus, only Green IF all factors of the GreenIF are considered.
Implications for Practice
General implication: The Green Implementation Framework (The GreenIF) can offer users valuable insights into important factors to consider when implementing nature-based interventions (NBIs) in healthcare settings.
Supporting research: The GreenIF can help researchers design, monitor, and evaluate implementation studies, with a central focus on measuring the impact of implementation factors on the utilization of NBIs.
Informing healthcare practice: Healthcare managers, decision-makers, policymakers, healthcare designers, green designers, and professionals can use the GreenIF to support and evaluate the design and implementation processes of NBIs in healthcare settings.
Facilitating stakeholder conversations: During implementation processes the GreenIF can facilitate discussions among multiple stakeholders about the current implementation context and can provide insights into potential challenges.
Guiding implementation phases of new NBIs: During the pre-implementation phase, the GreenIF can identify barriers and facilitators specific to the healthcare settings, aiding in the development of design and implementation plans. In the implementation phase, the framework can monitor the progress of the implementation process and adjust it if necessary. In the postimplementation phase, it can assist in evaluating the process and identifying any remaining factors that require attention.
Evaluating existing interventions: The GreenIF can be used to evaluate if design and implementation factors explain usage differences of existing NBIs. When comparing various NBIs, the framework can provide broader insights into which specific factors are important for a successful implementation of NBIs in healthcare settings in general, thereby enhancing the effectiveness and efficiency of current practices.
Supplemental Material
sj-docx-1-her-10.1177_19375867251331105 - Supplemental material for Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings
Supplemental material, sj-docx-1-her-10.1177_19375867251331105 for Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings by Rosanne Steensma and Nicole van den Bogerd, Karin Dijkstra, Wendy Meijboom, Maryska Janssen-Heijnen, Lydia Krabbendam, Jolanda Maas in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-2-her-10.1177_19375867251331105 - Supplemental material for Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings
Supplemental material, sj-docx-2-her-10.1177_19375867251331105 for Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings by Rosanne Steensma and Nicole van den Bogerd, Karin Dijkstra, Wendy Meijboom, Maryska Janssen-Heijnen, Lydia Krabbendam, Jolanda Maas in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-3-her-10.1177_19375867251331105 - Supplemental material for Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings
Supplemental material, sj-docx-3-her-10.1177_19375867251331105 for Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings by Rosanne Steensma and Nicole van den Bogerd, Karin Dijkstra, Wendy Meijboom, Maryska Janssen-Heijnen, Lydia Krabbendam, Jolanda Maas in HERD: Health Environments Research & Design Journal
Footnotes
Authors Contributions
RSS did conceptualization, methodology, formal analysis, writing—original draft, visualization.
NVDB did conceptualization, methodology, formal analysis, writing—review and editing, supervision.
KD did writing—review and editing, supervision.
MJH did writing—review and editing, funding acquisition, supervision.
LK did writing—review and editing, supervision.
JM did conceptualization, methodology, formal analysis, writing—review and editing, supervision, project administration, funding acquisition.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The manuscript “Development of the GreenIF: A Framework to Identify Implementation Factors for Nature-Based Interventions in Healthcare Settings” presents original findings that have not been published elsewhere and is not currently under review by any other journal. This study was approved by the ethical committee of the Faculty of Behavioral and Movement Sciences (VCWE-2021-058).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Provincie Overijssel, Medisch Centrum Leeuwarden, Topsector Horticulture and Starting materials, Revalidatie Friesland, Isala Zwolle, Pennemes, VieCuri Medical Centre (grant number LWV-19222-08).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.