
Abstract
Objectives:
This research describes the physical environments of and equipment in Aotearoa New Zealand (NZ) general practices in relation to available standards for big-bodied people (BBP) seeking healthcare.
Background:
The prevalence of BBP both in NZ and globally has increased over the last 30 years and is expected to increase further. As the first and most utilized point of contact for patients in NZ and many countries, it is essential that general practices provide suitable environments to cater for and meet the needs of big-bodied patients seeking healthcare.
Methods:
An exploratory study utilizing an environmental investigation was undertaken in three diverse general practices. Data collection consisted of direct observation and physical measurements of practice layout and equipment. Findings were compared to the existing guidelines or standards for the healthcare of BBP.
Results:
The analysis identified most environmental facets and equipment in all three general practices did not meet published guidelines for the care of BBP.
Conclusions:
In the global context of increasing and sustained prevalence of BBP, this exploratory study highlights it is crucial that general practices and similar community-based facilities review their physical environments and equipment and consider modifications to improve accessibility, inclusivity, and comfort for BBP.
Keywords
Introduction
Primary care (general practice, family doctor, or physician), as the first and most utilized point of contact for patients in many countries (Cumming & Salmond, 2018; Goodyear-Smith & Ashton, 2019; Pedersen et al., 2012; Tenbensel et al., 2017; Turner, 2023), needs to provide suitable environments to cater for and meet the needs of patients, including big-bodied people (BBP) seeking healthcare. The prevalence of BBP globally has markedly increased over the last 30 years and further increases worldwide are expected (Noncommunicable Diseases Risk Factor Collaboration [NCD], 2016; Ortiz et al., 2021). BBP are described as those weighing 150 kg (331 lb) or more, have a body mass of 40 kg/m2 (8.19 lb/sqft) or more, or who have large physical dimensions (Accident Corporation Company [ACC], 2011). In Aotearoa New Zealand (NZ), the NZ Health Survey reports that 5.9% of adults were identified as having a body mass of 40 kg/m2 (8.19 lb/sqft) or greater, with indigenous Māori (13%), Pasifika (24.5%), and those living in high deprivation areas (11.9%) being disproportionately represented (Ministry of Health, 2021a, 2021b).
It is well-documented that BBP experience societal and environmental stigma relating to size- and weight-based prejudice (Lee & Pausé, 2016; Phelan et al., 2015). The latter includes not being able to fit in seats at cinemas, public transport, or on aeroplanes (Lewis et al., 2011), and compared to direct forms of stigma (such as verbal insults), environmental stigma has been described by BBP in a recent Australian study as having the greatest impact on their well-being due to their inability to respond (Lewis et al., 2011). However, little is known about the barriers created by public physical environments for BBP such as healthcare buildings that are not ergonomically designed to accommodate them (Masson et al., 2019a, 2019b; Owen, 2012). Of the limited international empirical studies that have examined the adequacy of healthcare environments for BBP, most have been undertaken in high-acuity environments such as hospitals. These studies have reported equipment (such as imaging scanners, beds, stretchers, and wheelchairs) and spaces that are inadequate for BBPs’ size and weight (do Lucio et al., 2008), which lead to injury, delays in care, and embarrassment for BBP (Kukielka, 2020). A lack of suitable equipment and facilities to cater for BBP have similarly been identified in NZ hospitals (Hales et al., 2018; Yee et al., 2022) and residential aged care facilities (Hales et al., 2020). In a recent study exploring BBPs’ lived experience of public hospitalization in Australia, BBP expressed that a lack of timely provision of appropriate equipment necessary for their basic care resulted in a loss of personal dignity and increased pain and dependence (Pazsa et al., 2022).
In contrast, ambulatory clinical service delivery in healthcare environments, such as general practice, is usually short (under an hour) but the throughput higher. Research examining the adequacy of primary care physical environments for BBP is scarce; however, qualitative studies and case reports have indicated that BBP struggle to use the spaces and clinical equipment and other amenities (such as chairs, gowns, and blood pressure cuffs; Ahmed et al., 2002; Merrill & Grassley, 2008). Further, BBP have reported that the inadequate equipment, lack of privacy (such as weight scales being situated in open areas), and the associated sense of shame are the key barriers to their engagement with primary care, where preventative healthcare measures such as regular screening are important (Forhan et al., 2013; Merrill & Grassley, 2008). Lack of suitable equipment has been noted by family physicians as being a significant barrier to undertaking breast and cervical cancer screening examinations in BBP (Ferrante et al., 2010).
However, overall, very little observational research has directly examined the adequacy of general practice environments for BBP. This study set out to observe, measure, and describe the physical environments of three diverse NZ general practices and compare with the available standards for BBP seeking healthcare (shown in Table 1).
Design Standards for Bariatric Healthcare Settings.
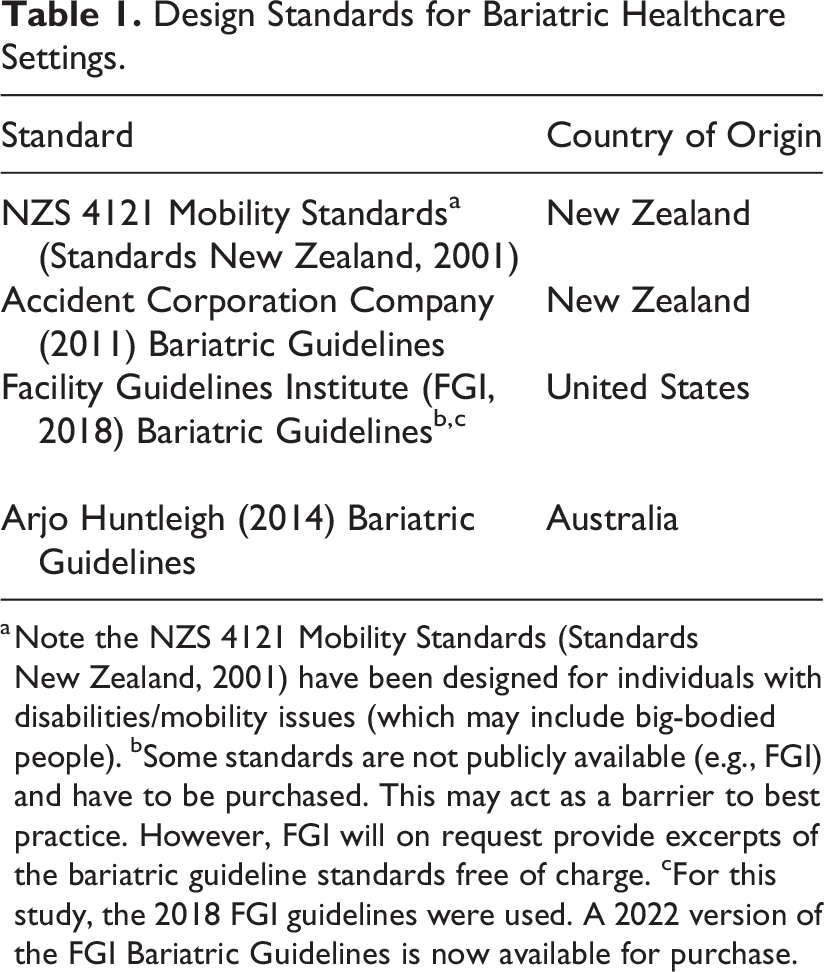
a Note the NZS 4121 Mobility Standards (Standards New Zealand, 2001) have been designed for individuals with disabilities/mobility issues (which may include big-bodied people). bSome standards are not publicly available (e.g., FGI) and have to be purchased. This may act as a barrier to best practice. However, FGI will on request provide excerpts of the bariatric guideline standards free of charge. cFor this study, the 2018 FGI guidelines were used. A 2022 version of the FGI Bariatric Guidelines is now available for purchase.
Method
Study Design
This exploratory study utilized an environmental investigation method (Park et al., 2020). Direct observation and physical measurements were undertaken in three diverse general practices and findings were compared to the existing guidelines for healthcare of BBP. Data collection took place in late 2021 and early 2022 during the COVID-19 pandemic when mitigations for infection control were being implemented (plexi-screens at reception, masks, and entry procedures). This study was approved by the University of Otago Human Ethics Committee (ref D21/04).
Setting and Participants
General practice buildings in NZ range from converted residential homes to purpose-built facilities (Morgan et al., 2021). Three practices were purposively selected for the study to include a range of practice size, building type (age of building, converted residential, or purpose-built), location, and practice population (to include Māori, who have a higher prevalence of BBP). Two practices were in the lower North Island of NZ, and the third was in the east coast of the North Island. Practice recruitment was completed via existing contacts and snowball network techniques. A description of the participating practices is provided in Table 2.
Description of Participating General Practices.
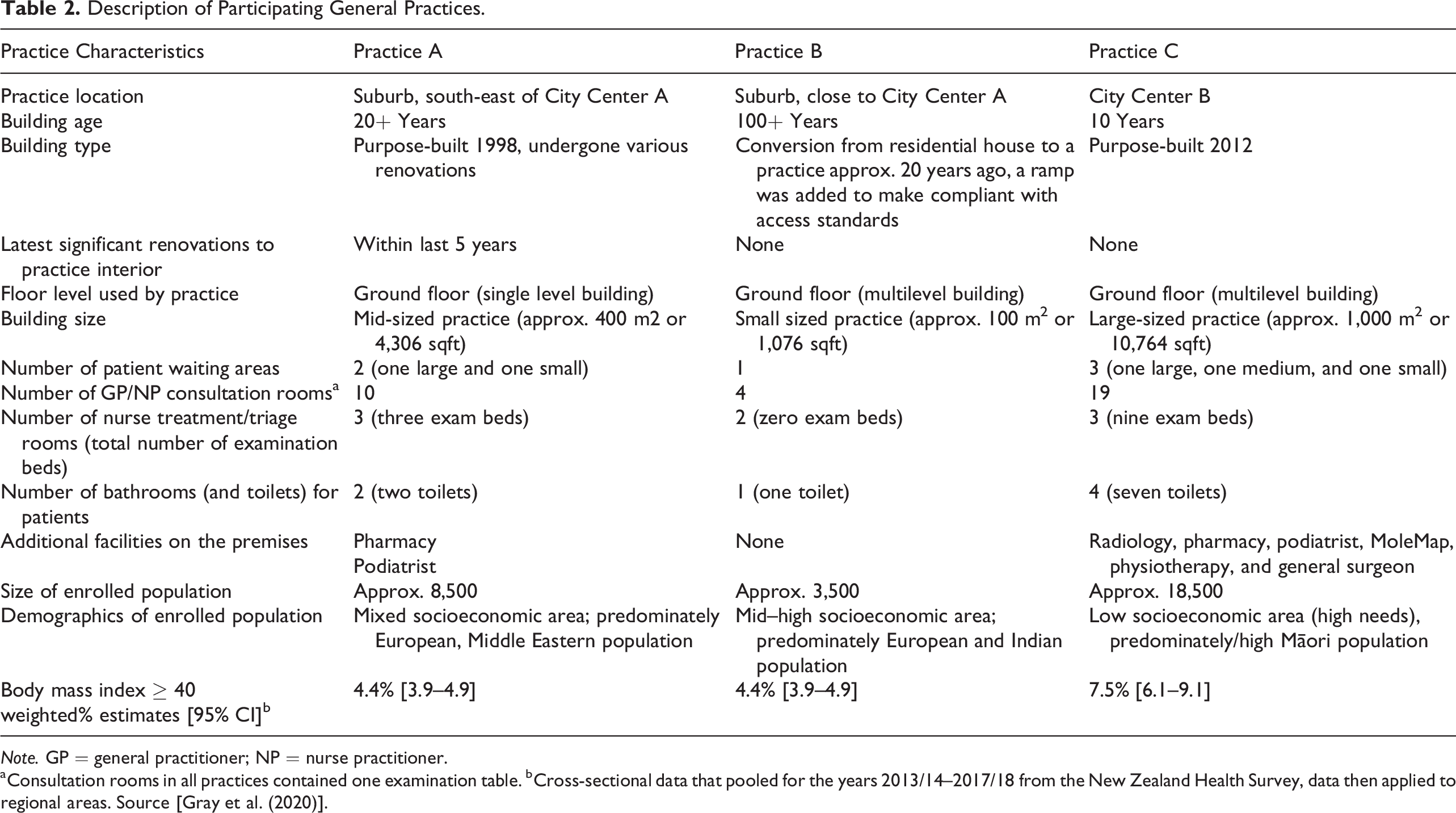
Note. GP = general practitioner; NP = nurse practitioner.
aConsultation rooms in all practices contained one examination table. bCross-sectional data that pooled for the years 2013/14–2017/18 from the New Zealand Health Survey, data then applied to regional areas. Source [Gray et al. (2020)].
Data Collection
Practice recruitment and data collection were undertaken sequentially. In each practice, direct observation consisted of a practice visit where a research fieldworker 1 observed, photographed, and measured selected spaces and equipment, when patients were not present. Floorplans and other relevant information about the practice building and equipment were also obtained from practice staff. Observations were recorded on a structured paper-based tool informed by international and NZ-based guidelines for healthcare services (ACC, 2011; Arjo Huntleigh, 2014, 2023; Facility Guidelines Institute [FGI], 2018), and measurements were undertaken using an electronic measuring tool. Unstructured field notes were also taken.
Analysis
Data recorded on the paper-based observation tool were converted into an Excel spreadsheet and field notes converted to electronic form. All data collected from each separate practice were collated and reviewed. Physical environment data for each practice were compared to published guidelines or summaries of guidelines for the design of outpatient (FGI, 2018) and general healthcare facilities providing care to BBP (ACC, 2011; Arjo Huntleigh, 2014, 2023) and standards for making facilities accessible for people who have disabilities (see Table 1). With no guidelines specific to general practice settings, observations were also compared to more general guidelines or recommendations for creating inclusive general practice environments for BBP (Ahmed et al., 2002; Freihoefer et al., 2013; National Task Force on the Prevention and Treatment of Obesity, 2002; Ortiz et al., 2021; Royal New Zealand College of General Practitioners, 2022).
Results
The analysis identified environmental features in each of the three general practices where accessibility, inclusivity, and comfort for BBP could be improved. Practice observations confirmed the physical practice environments and equipment had not been designed in terms of any best practice standards for addressing the specific needs of BBP in healthcare settings (see Table 3 for summarized results and Supplementary File A for complete table of results). The observations compared to published guidelines are described in the following according to the main physical spaces BBP experience when accessing a general practice: the access/entrance, reception and waiting areas, corridors and entranceways, consultation/treatment rooms, and bathrooms.
Selected Practice Observations Compared to Available Standards and Recommendations for General Practices to Accommodate Big-Bodied People (BBP).a,b,c
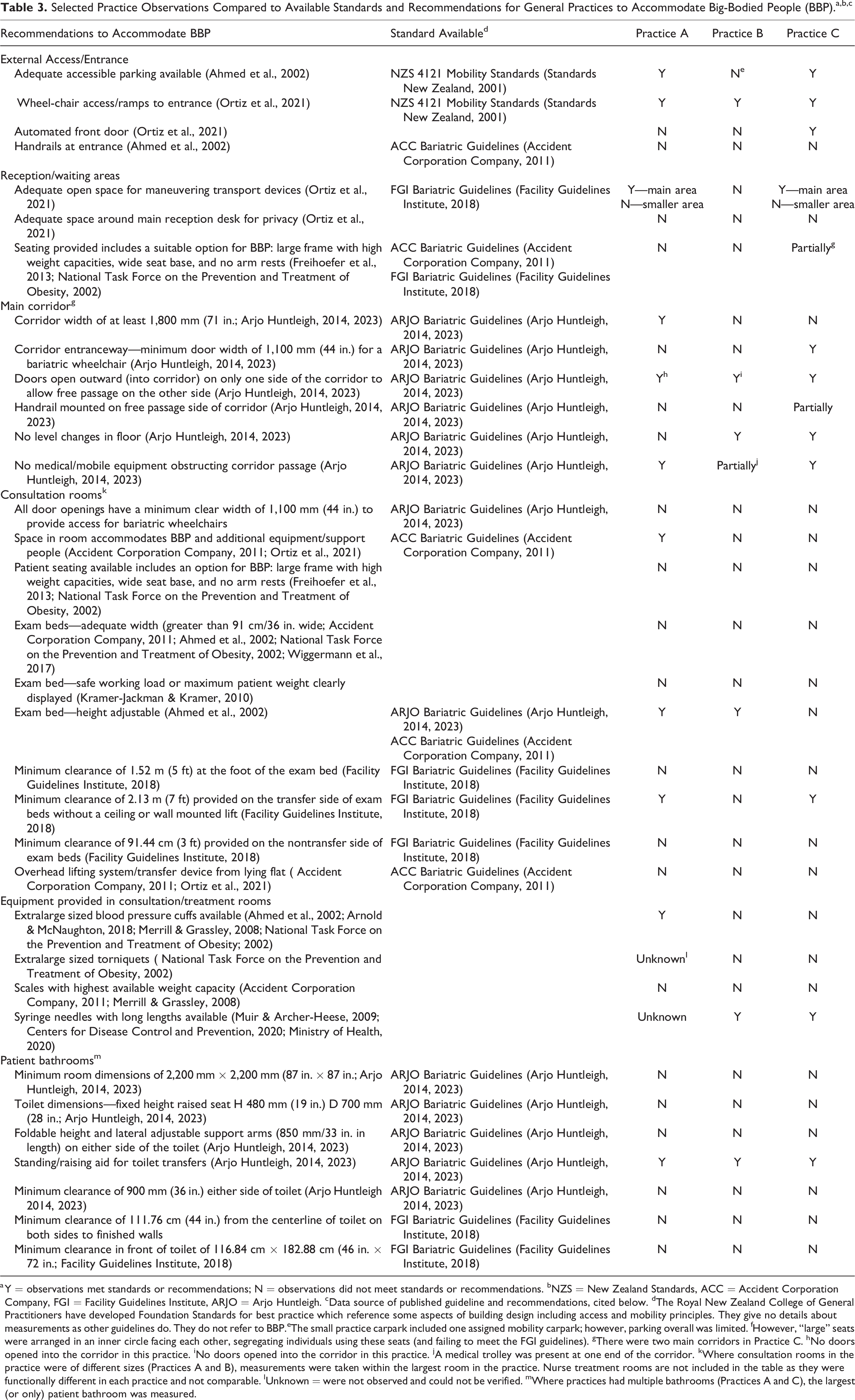
a Y = observations met standards or recommendations; N = observations did not meet standards or recommendations. bNZS = New Zealand Standards, ACC = Accident Corporation Company, FGI = Facility Guidelines Institute, ARJO = Arjo Huntleigh. cData source of published guideline and recommendations, cited below. dThe Royal New Zealand College of General Practitioners have developed Foundation Standards for best practice which reference some aspects of building design including access and mobility principles. They give no details about measurements as other guidelines do. They do not refer to BBP.eThe small practice carpark included one assigned mobility carpark; however, parking overall was limited. fHowever, “large” seats were arranged in an inner circle facing each other, segregating individuals using these seats (and failing to meet the FGI guidelines). gThere were two main corridors in Practice C. hNo doors opened into the corridor in this practice. iNo doors opened into the corridor in this practice. jA medical trolley was present at one end of the corridor. kWhere consultation rooms in the practice were of different sizes (Practices A and B), measurements were taken within the largest room in the practice. Nurse treatment rooms are not included in the table as they were functionally different in each practice and not comparable. lUnknown = were not observed and could not be verified. mWhere practices had multiple bathrooms (Practices A and C), the largest (or only) patient bathroom was measured.
Practice External Access/Entrance
Sufficient parking and wheelchair accessible entrance ways that facilitate access for BBP are important for those with high weight and decreased mobility (Ahmed et al., 2002; Ortiz et al., 2021). In NZ, there have been Access and Mobility Standards since 2001, with requirements for car parking and access to buildings (Standards New Zealand, 2001). Two of the participating practices had adequate parking, with large numbers of parks available either within practice parking lots or nearby on the street. However, one practice was located on a busy street with limited dedicated practice parking within the parking lot. All practice parking lots included at least one mobility park and had good wheelchair access to the main entrance, yet the accessibility of the entranceway itself varied between practices. In one practice, the main entrance had automatic doors, and in the other two practices, entrance doors were opened manually. There were no handrail supports available at any practice entrance ways.
Reception and Waiting Areas
As “front-of-house” public spaces, it is essential the reception and waiting areas are welcoming, provide adequate privacy for checking-in, and include appropriate furniture for BBP (Ahmed et al., 2002; Ortiz et al., 2021). The 2018 Facility Guidelines Institute (FGI) guidelines for the design and construction of outpatient facilities note that sufficient space is required for maneuvering or parking wheelchairs or other transport devices. There was variability in all of these aspects in the study practices and none sufficiently attended to all these standards. None of the practices included fully private areas for patient check-in. Clearance space around the reception desks in the two larger practices was observed to permit quiet conversation to take place out of the range of patients seated in the adjacent waiting areas; however, space for private conversation in the small practice was insufficient. All three practices featured one main open waiting area space with a central reception desk; the two larger practices both had additional small waiting area(s) in other parts of the building. The main waiting areas in the two larger study practices provided adequate space for the use of transport devices and/or caregivers/support people, but maneuvering transport devices in the small practice’s waiting area would have been difficult.
Seating available within patient waiting areas is known to be a key factor influencing BBPs’ comfort and experience (Ahmed et al., 2002; Merrill & Grassley, 2008; National Task Force on the Prevention and Treatment of Obesity, 2002; Pazsa et al., 2022). It is important there is enough furniture for BBP in these spaces and that it is large and sturdy to support BBP as they wait for treatment (Ahmed et al., 2002; Freihoefer et al., 2013). The 2018 FGI guidelines stipulate that furniture in waiting areas should support higher weight body types without segregating or highlighting the individual, and 5% of seating in these spaces should accommodate individuals who weigh up to 272.16 kg (600 lb). Suitable chairs for BBP have larger frames with high weight capacities and wider seat dimensions with no arm rests or moveable arm rests (Freihoefer et al., 2013; National Task Force on the Prevention and Treatment of Obesity, 2002). The types of seating provided in all three study practices’ waiting areas were found to not meet these guidelines. Although all practices provided at least two different seat options in waiting areas (including at least one seat option without arm rests), none of the practices’ waiting areas included a seating option that would effectively and comfortably meet the needs of BBP. For example, in two of the study practices, seats provided without arm rests did not have sturdy frames or wide bases that would accommodate BBPs. Although one or two “standing-assistance chairs” (designed for use in medical or aged care settings with high or adjustable seat bases and high weight capacities) were available in some practice waiting areas, they had nonmovable arm rests. Only one practice provided larger seats to comfortably accommodate most BBP (with wide bases, solid frames, and no arm rests). These seats for BBP were arranged in an inner circle facing each other, segregating individuals (and failing to meet the FGI guidelines). See Figure 1 for an example of inadequate waiting room seating.
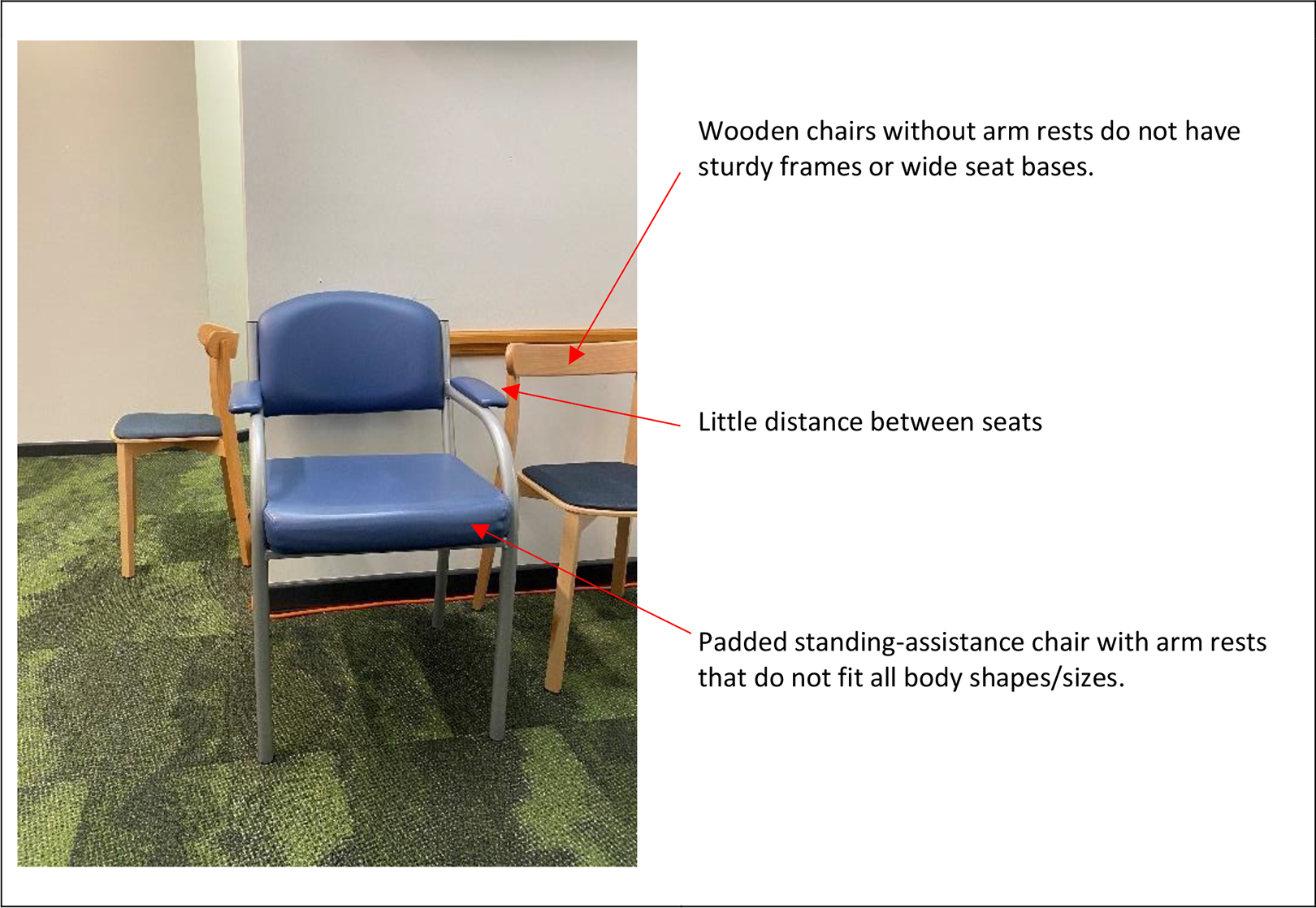
Example of waiting room seating options that are not adequate for big-bodied people. Image authorship: author.
Corridors and Internal Entranceways
Facilitating BBPs’ safe navigation from the reception to consultation or treatment rooms or other areas of the practice requires corridors and doorways of adequate width for mobility devices and additional caregivers/support people. The Arjo Huntleigh (2014, 2023) guide for architects and planners designing healthcare settings recommends that all corridors should be a minimum width of 1,800 mm (71 in.) and that doorways have a minimum width of 1,100 mm (44 in.) for expanded width and weight capacity wheelchairs (also known as bariatric wheelchairs). The guidelines further stipulate doors opening outward into corridors should only do so on one side of the corridor; handrails should be mounted on the free passage side of the corridor; no thresholds or doorways should be present in corridors and no level changes of floor; any doors which open into a corridor must be denoted with clear contrasting colors on the floor; and there should also be no mobile equipment stored in corridors.
The width of corridors in two of the three study practices did not meet the Arjo Huntleigh (2014, 2023) standards (see Figure 2 for an example). None of the three practices’ corridors included handrail supports, and in one practice, a section of the corridor floor was sloping (this was signposted). In all three practices, corridors were fairly free of obstructions and doors did not open into the corridor on both sides.

Example of a narrow corridor without handrails. Image authorship: author.
Consultation Rooms and Equipment
Patient treatment rooms such as general practitioner, nurse practitioner, nurse, practice pharmacist, and other staff consultation and treatment rooms must be accessible, of adequate size and layout, and include appropriate equipment to allow BBP to be safely and comfortably treated with dignity (Ortiz et al., 2021). All consultation rooms measured in study practices 2 did not meet most standards for providing care to BBP. Doorways into consultation rooms in the three practices were less than the minimum recommended width of 1,100 mm (44 in.) for bariatric wheelchairs (Arjo Huntleigh, 2014, 2023). The layout of consultation rooms was similar across practices (see Figure 3). All consisted of a desk with computer for staff on one wall, one-three patient/support person seats positioned to the side of the desk, an examination bed positioned against a wall, a hand washing basin, storage cabinets/trollies, and various other medical equipment items. The largest consultation rooms in each practice were approximately 18 m2 (194 sqft), 14 m2 (151 sqft), and 11 m2 (118 sqft). The configuration of furniture in most consultation rooms did not provide adequate space for BBP and additional equipment/support people. Most consultation rooms (excluding some large rooms in one practice) had minimal clearance space around furniture items for BBP to access seats without furniture being physically moved. Seats allocated for patients/caregivers often had little distance between them. Generally, one of these seats had no arm rests; however, seat dimensions were of standard size (neither bariatric or standing-assistance varieties).

Example of a standard consultation room with limited space for big-bodied people, mobility devices, or caregivers/support staff or whānau (family). Image authorship: author.
To provide safe assessment of BBP, examination beds in consultation rooms need to be of sufficient width, load-bearing capacity, and height adjustable (ACC, 2011; Ahmed et al., 2002; National Task Force on the Prevention and Treatment of Obesity, 2002; Wiggermann et al., 2017). Research shows patients with a body mass index greater than 35 kg/m2 (7.17 lb/sqft) have insufficient space to be turned side to side for examinations on standard hospital beds of 91 cm (36 in.) width (Wiggerman et al., 2017). In all study practices, consultation room examination beds measured were observed to be too narrow for BBP, with beds ranging from 74.5 cm (29.3 in.) to 89.4 cm (35.2 in.) wide. It is recommended that bed weight capacity should be labeled on all beds (ACC, 2011; Kramer-Jackman & Kramer, 2010), and the Independent Living Centre (2021) recommends all equipment should have a minimum load capacity of 10% above the user’s weight. Clinic examination beds in study practices’ consultation rooms were not labeled with safe working loads and practice staff did not know the weight capacities. Due to the age of some of the examination beds and with changes to model codes, it proved impossible to locate the original specifications, and so, we were unable to ascertain maximum weight capacities. 3 Only one practice had adjustable examination beds in all of the consultation rooms observed, and in one practice, beds in all consultation rooms were nonadjustable. 4 No consultation rooms provided mobile or ceiling hoists for bed repositioning or transfers as recommended for the moving and handling of bariatric patients (ACC).
The FGI (2018) recommends patient examination rooms also incorporate clearance space around examination beds for additional equipment and caregivers. Although most consultation rooms in study practices were observed to provide clearance space on the transfer side of examination beds, due to all examination beds being placed against walls, no clearance was provided on the nontransfer side of examination beds. In all practices, there was very little space, if any, at the end of the examination bed either due to other physical structures (such as sinks or desks) or the placement of furniture (such as trollies or seats) at the end of the examination bed. Other treatment/triage rooms in all study practices exhibited similar accessibility limitations for BBP in terms of room layout, clearance space, furniture, and equipment (see Figure 4 for an example).
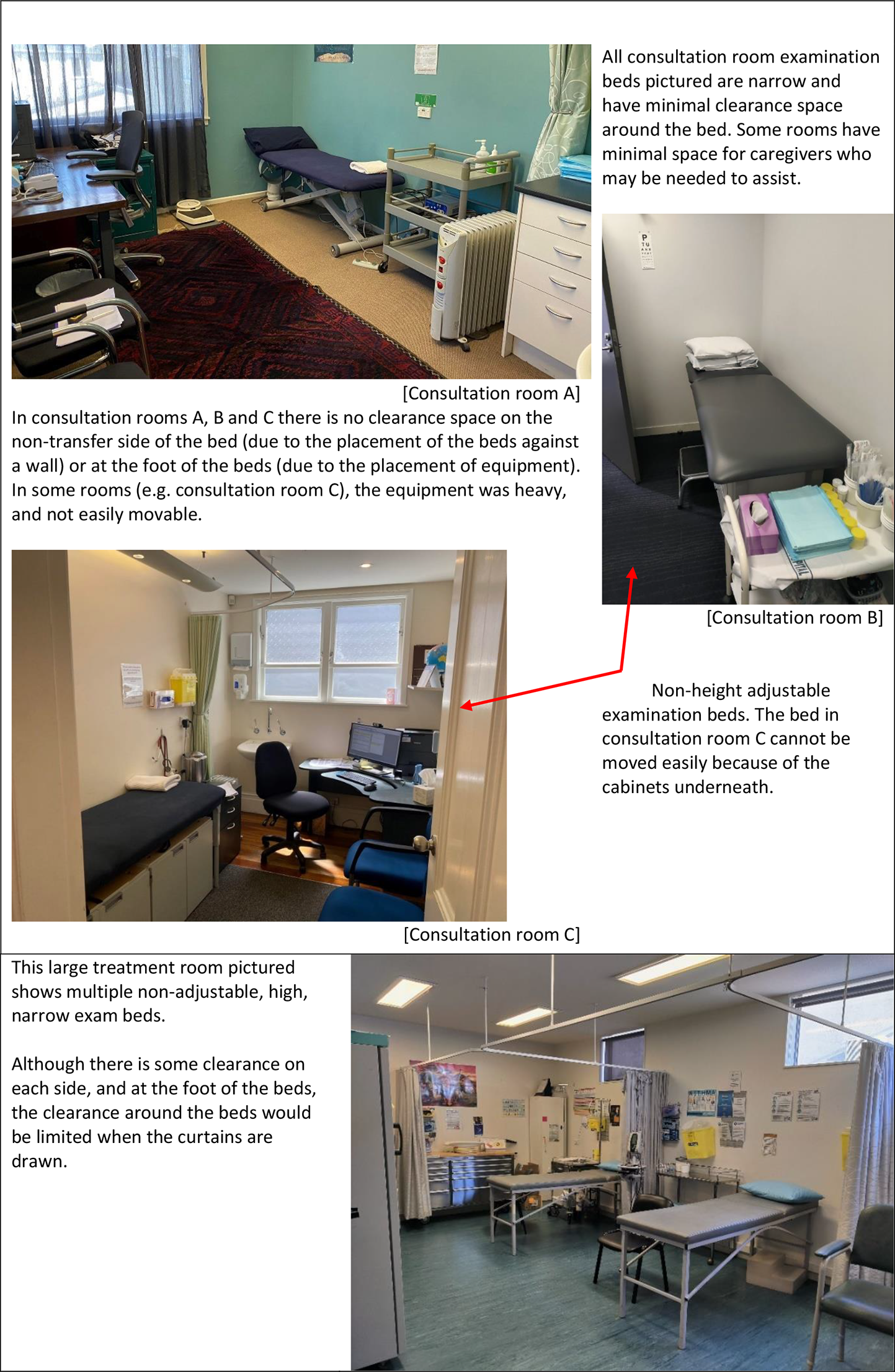
Examples of practice examination beds not suitable for big-bodied people. Image authorship: author.
Equipment Provided
Adequately sized diagnostic equipment for BBP is essential for accurate assessment and comfort (National Task Force on the Prevention and Treatment of Obesity, 2002; Phelan et al., 2015). However, equipment routinely provided in all the study consultation and treatment rooms was standard sized. Staff could not locate extralarge-sized blood pressure cuffs (Ahmed et al., 2002; Arnold & McNaughton, 2018; Muir & Archer-Heese, 2009) in two practices. Torniquet sizes (National Task Force on the Prevention and Treatment of Obesity) were noted to be regular sized in all practice consultation/treatment rooms. The maximum weight capacity of weighing scales available in study practices ranged from 150 to 220 kg (330–485 lb). Bariatric scales are commercially available up to 453.6 kg (1,000 lb) and often have a wider platform than regular scales and should be situated in spaces that allow for privacy (ACC, 2011). Syringe needles with long lengths as recommended for BBP for intramuscular deltoid vaccination (Centers for Disease Control and Prevention, 2020; Ministry of Health, 2020) were available in two study practices.
Bathrooms
Safe access to an appropriately sized bathroom and toilet is a basic human right (Faktor, 2011). The Arjo Huntleigh (2014, 2023) guidelines recommend the minimum dimensions of bathrooms to be 2,200 mm × 2,200 mm (87 in. × 87 in.), with a doorway entrance width of at least 900 mm (36 in.). The number of bathrooms for patient use in study practices ranged from one in the smaller practice to four in the largest practice. The size of all bathrooms measured in study practices did not meet the guideline’s minimum dimensions including the space between door openings and toilets. Some of the bathroom doors in two of the practices opened inward, restricting clearance space. The guidelines stipulate toilets should be a minimum of 480 mm (19 in.) height and 700 mm (28 in.) depth to facilitate sitting down and getting up from the toilet and include lateral adjustable support arms—850 mm (33 in.) in length on either side of the toilet that are securely attached to the wall. Standing and raising aids for toilet transfers are also recommended. None of the toilets measured met recommended dimensions. There were however grab bars fixed to the wall on one side of the toilet in most practice bathrooms.
Bathrooms that accommodate BBP require increased clear space around toilets (ACC, 2011; Ahmed et al., 2002). The Arjo Huntleigh guidelines (2014, 2023) require a clearance of 900 mm (36 in.) on either side of the toilet, and the FGI (2018) guidelines stipulate toilets should be mounted 111.76 cm (44 in.) from the finished wall on both sides. The FGI also recommends a clear floor area of 116.84 cm × 182.88 cm (46 in. × 72 in.) wide at the front of the toilet. None of the bathrooms measured in study practices met any of the Arjo Huntleigh or FGI guidelines pertaining to clearance space around the toilet (see Figure 5).
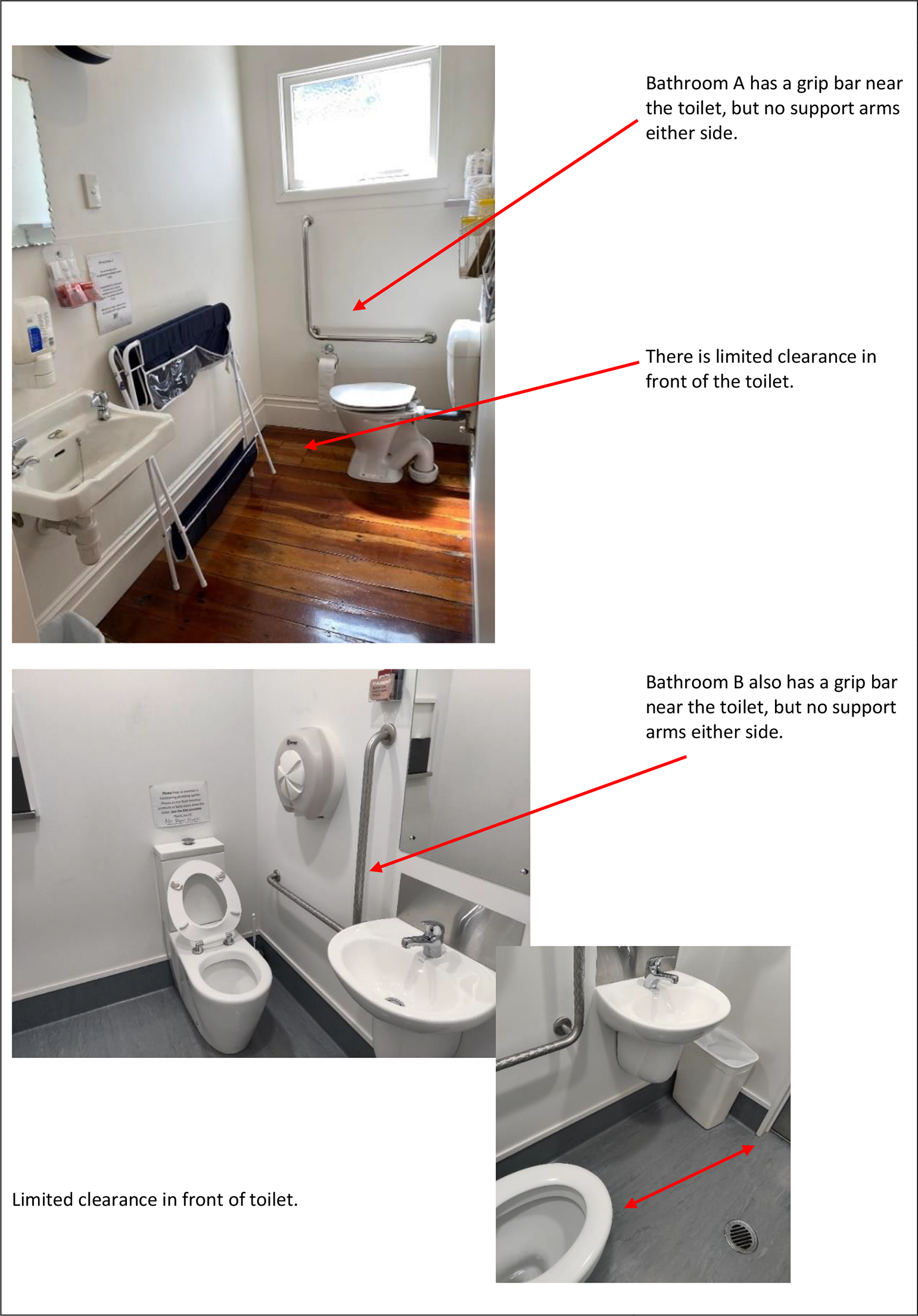
Examples of different patient bathrooms and limitations for big-bodied people. Image authorship: author.
Discussion
This study is the first that we are aware of to describe the physical environments of general practices in relation to best practice standards/recommendations for health facilities providing care to BBP. Except for car parking and wheelchair access covered by the NZ Access and Mobility Standard (NZS 4121), most environmental facets in all three practice environments failed to meet international published guidelines/recommendations in relation to BBP. Similarly, equipment used to measure clinical parameters was either not available or in limited supply (weight scales, large sizes of blood pressure cuffs, and torniquets).
It is perhaps unsurprising that the three study general practice premises did not meet international and national best practice standards for the healthcare of BBP as standards referenced in Table 1 are not all publicly available and some need to be purchased, and the cost for individual practices is prohibitive. Knowing specific standards for BBP exist would be helpful for other agencies developing their own. For example, the recently updated United Kingdom Health Building Notes for the National Health Service does not mention requirements for BBP (Department of Health, 2021). Similarly, the NZ Standard for Access and Mobility (Standards New Zealand, 2001), despite mentioning “extremes of physical size” (section 1.5.1.k), does not specifically include accommodations for BBP and the toilet specifications are smaller than the minimum recommended by the Arjo Huntleigh guidelines. The Royal New Zealand College of General Practitioners Foundation Standards (2022) similarly state there should be adequate space and equipment in practices but give no specification or particular guidance for how this should apply for BBP. Having a suitable physical environment with appropriate equipment in general practice is important as it is often the first point of contact for BBP into the health system and/or acts as a gatekeeper for access to hospital-based care (Cumming & Salmond, 2018; Goodyear-Smith & Aston, 2019; Pedersen et al., 2012; Tenbensel et al., 2017; Turner, 2023). BBP may delay or avoid seeking care if the environment is unwelcoming (Amy et al., 2006, Ingraham et al., 2014, Lee & Pausé, 2016, Merrill & Grassley, 2008, NCD Risk, 2016; Zuzelo & Seminara, 2006).
None of the study practices mentioned they had specifically considered renovations, alterations, or equipment upgrades to improve accessibility or comfort for BBP. The observations and measurements show that there are environmental and physical factors that act as barriers. These findings align with the negative experiences BBP have reported about inadequate healthcare spaces and equipment internationally in both hospital (Do Lucio et al., 2008; Kukielka, 2020) and primary care settings (Forhan et al., 2013; Merrill & Grassley, 2008) . However, our study extends previous research by revealing specific features in the different areas of the study practice environments and equipment, including many aspects that have not been reported before, that were directly observed to be inadequate for BBP, and did not meet published standards. This information could be used by general practices to review these aspects and if needed improve the accessibility, inclusivity, and comfort of their practices for BBP.
Strengths
This study is a starting point for further research with a larger sample of general practices and including staff and BBP’s views. Published standards or guidelines on building design for BBP were used to audit the observations and measurements of the physical environment and equipment with clarification by staff.
Limitations
The three NZ general practices in our study were chosen to represent a range of building size, configuration, age, and practice population and each was examined in detail, but they will not be typical of the full range of general practices across NZ or globally. Measurements were undertaken of the largest consultation rooms. Some measurements were unable to be collected either due to COVID-19 restrictions, limited access to practices, or due to the age of equipment. The views of BBP about the environment and equipment in general practices were not sought in this study.
Implications
In the global context of increasing and sustained prevalence of BBP, it is crucial that general practices and similar community-based facilities review their physical environments and equipment and consider ways, in which their practice environments can be redesigned or altered to improve accessibility for BBP. General practice environments differ in function and form to hospital and outpatient facilities. In the absence of specific standards for BBP in general practice settings, our results are based on international and national standards or guidelines for BBP predominantly developed for hospital healthcare and/or outpatient settings.
Recommendations
Establish a standard for new or upgraded general practice buildings accounting for the following aspects and needs of BBP, but recognizing that retrofitting is expensive and may need to be staged over time. Once undertaken, this will improve the accuracy/quality of care practices are able to provide and increase comfort and dignity for BBP. accessible access into the practice (parking, ramps/no stairs, and automatic opening doors), additional clearance space for easy movement, mobility devices, and support people in all key areas of the practice, seating options of an appropriate size and weight rating dispersed throughout practice waiting areas, treatment room furniture (such as examination beds and chairs) of an appropriate size and weight rating, and measuring equipment (such as scales, needles, and blood pressure cuffs) to accommodate larger sizes/weights.
Implications for Practice
Not all general practice buildings are physically welcoming to BBP. Given the increasing prevalence of BBP worldwide, it is crucial that general practices and similar community-based facilities review their physical environments and equipment and consider ways in which these can be redesigned or altered to improve accessibility for BBP.
Guidelines exist for creating inclusive hospital and outpatient facilities for BBP, but future research is needed to develop standards specific to general practice.
Key considerations include: accessible access into the practice; additional clearance space to accommodate BBP, mobility devices and support people in all key areas of the practice; seating options of an appropriate size and weight rating dispersed throughout waiting areas; consultation and treatment room furniture including examination beds that are of an appropriate size and weight rating; and measuring, weighing, and clinical equipment to accommodate larger sizes/weights.
Improving general practice accessibility for BBP is important because general practice is recognized to be the front line to providing healthcare and inadequate physical environments and equipment are known to contribute to BBP delaying or avoiding seeking care.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867241238442 - Sizing Up General Practice Environments for Big-Bodied Patients: An Environmental Assessment of Three Facilities in Aotearoa New Zealand
Supplemental Material, sj-pdf-1-her-10.1177_19375867241238442 for Sizing Up General Practice Environments for Big-Bodied Patients: An Environmental Assessment of Three Facilities in Aotearoa New Zealand by Sonya Morgan, Sheharazade Mihlar, Emily Wood, Eileen McKinlay, Helen Gibbs, George Parker and Lesley Gray in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors sincerely thank the participating general practices and staff participants who gave their time to participate and kindly provided access to premises and floor plans. They would like to thank Priscilla Smalley, who contributed to data collection in their final year of medical school as part of their Elective placement. They acknowledge the late Dr Cat Pausé who was to be part of this study and gave tremendous encouragement to the project from the outset. They also acknowledge and appreciate the support of Megan Ferris, Reference Librarian, Wellington Medical and Health Sciences Library University of Otago, Wellington.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Royal New Zealand College of General Practitioners. The University of Otago Wellington provided additional funding to complete the study, impacted by delays during the COVID-19 pandemic.
ORCID iDs
Notes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.