
Abstract
Objective:
The aim of this study is to analyze the consistency, variability, and potential standardization of terminology used to describe architectural variables (AVs) and health outcomes in evidence-based design (EBD) studies.
Background:
In EBD research, consistent terminology is crucial for studying the effects of AVs on health outcomes. However, there is a possibility that diverse terms have been used by researchers, which could lead to potential confusion and inconsistencies.
Methods:
Three recent large systematic reviews were used as a source of publications, and 105 were extracted. The analysis aimed to extract a list of the terms used to refer to the unique concepts of AVs and health outcomes, with a specific focus on people with dementia. Each term’s frequency was calculated, and statistical tests, including the χ2 and the post hoc test, were employed to compare their distributions.
Results:
The study identified representative terms for AVs and health outcomes, revealing the variability in terminology usage within EBD field for dementia-friendly design. The comparative analysis of the identified terms highlighted patterns of frequency and distribution, shedding light on potential areas for standardization.
Conclusions:
The findings emphasize the need for standardized terminologies in EBD to improve communication, collaboration, and knowledge synthesis. Standardization of terminology can facilitate research comparability, enhance the generalizability of findings by creating a common language across studies and practitioners, and support the development of EBD guidelines. The study contributes to the ongoing discourse on standardizing terminologies in the field and provides insights into strategies for achieving consensus among researchers, practitioners, and stakeholders in health environmental research.
Keywords
Introduction
Evidence-based design (EBD) is a field of research that has been attracting significant attention over the years, particularly in the healthcare field, due to its potential to improve health outcomes in the built environment (Mahmood, 2021). EBD studies have been conducted to investigate how the built environment can affect the physical and psychological health of its users (Evans, 2003). In the past few decades, numerous studies related to EBD and healthcare have been published, examining various aspects of how the built environment impacts its users. One important area of study has been the effect of healthcare facilities on people with dementia, which is a subset of EBD known as dementia-friendly design. This field focuses on improving the built environment for people with dementia (Brambilla et al., 2019; Marquardt et al., 2014; Waller & Masterson, 2015). It is important to note that among healthcare facilities, the research base of dementia-friendly design is more robust in long-term care facilities than in other types of healthcare facilities such as acute care (Hebert & Scales, 2019). This is due to the fact that in most countries, more than 80% of people in long-term care facilities (e.g., nursing homes) have dementia (Sanford et al., 2015).
The increase in dementia-friendly design studies in recent years as part of EBD has led to a fragmentation of knowledge, by introducing diverse methodologies, terminologies, and contextual variations, making it difficult to apply the results to practical design solutions (Gan et al., 2022; Marquardt et al., 2014). It is crucial to organize and consolidate the knowledge gained from these studies to create a more comprehensive understanding of how the built environment can be designed to support people with dementia. This effort could lead to a more coherent and effective approach to designing healthcare facilities for people with dementia, ultimately improving their health and quality of life.
Dementia-friendly design is a multidisciplinary field that involves experts from a range of disciplines. Architects and designers play a crucial role in creating environments that support people with dementia, researchers contribute to the understanding of how design features can support health outcomes, medical specialists and caregivers provide valuable insights into the needs of people with dementia (Røsvik & Rokstad, 2020). Gerontologists provide insights into the aging process and how it relates to the needs of people with dementia (Day et al., 2000), and psychologists offer valuable input by examining the cognitive and emotional aspects of the built environment and how it affects people with dementia (Oatley & Johnson-Laird, 2014). Collaboration among these professionals is crucial in the development and implementation of dementia-friendly design strategies. Moreover, policy makers and healthcare providers can have a significant impact on the adoption and implementation of such strategies in healthcare facilities (Lin, 2017). As a result, by working together, these experts can create more effective and inclusive environments for people with dementia.
The multidisciplinary nature of dementia-friendly design highlights the criticality of having a common language and agreed-upon terminology. However, researchers in EBD, especially in dementia-friendly design, have utilized diverse terms to describe the architectural variables (AVs) and health and care outcomes (HCOs) when investigating the relationship between the built environment and health outcomes. Furthermore, the use of a wide range of terminology in health environments research has resulted in some ambiguity in the interpretation of terms (Battisto et al., 2023). This poses a significant challenge, as consistent and standardized terminology is crucial for effective communication and understanding among the various specialists involved in EBD (Anåker et al., 2017; Peavey & Vander Wyst, 2017).
There is widespread agreement among researchers who specialize in standardized terminologies that a wide variety of inconsistent and diverse terminologies hinder the conduct of evidence syntheses, communication, collaboration, and knowledge of research findings in diverse settings. Standardized terminologies are particularly important in the healthcare industry and health environmental research, as they have the potential to improve patient care and safety (Battisto et al., 2023; Fennelly et al., 2021; World Health Organization, 2006). The use of standardized terminologies in clinical practice can enhance communication, quality of care, and interoperability and facilitate value-based healthcare and knowledge generation (Fennelly et al., 2021). For example, an international working group was established in 2012 to explore the development of a common terminology and a comprehensive framework for knowledge translation interventions that integrate evidence into health practices, systems, and policies (Colquhoun et al., 2014).
Standardized terminology is also critical to the development and access of nursing knowledge. Without consistent terminology, the nursing knowledge base may be hindered, thereby delaying the integration of evidence-based healthcare into nursing practice (Andrews et al., 2016; Hardiker, 2011). Several pervious efforts have focused on the importance and effectiveness of standardized nursing terminologies for nursing practice and healthcare outcomes (Andrews et al., 2016; De Groot et al., 2020; Strudwick & Hardiker, 2016; Tastan et al., 2014; Zhang et al., 2021). Furthermore, a literature review has provided evidence for the usefulness of standardized nursing terminologies in various fields of application (Törnvall & Jansson, 2017). Additionally, incorporating the input of nurses into the design process can further enhance the development and implementation of standardized terminologies that are relevant and useful to nursing practice.
To tackle these challenges, enhancing the uniformity of terminology can be an effective solution (De Groot et al., 2020; Fennelly et al., 2021; Hardiker, 2011; Törnvall & Jansson, 2017; World Health Organization, 2006). Furthermore, there is growing recognition that standardized information can support statistical reporting, decision making, outcome and performance measurement, and cost analysis. Therefore, various dimensions of terminology must be accurately captured and standardized (World Health Organization, 2006). Recognizing the potential limitations of a purely positivist view on the relationship between the built environment and human outcomes, it is important to acknowledge the diverse perspectives and nuances that exist in the field. While this article aims to analyze the consistency and variability of terminology in EBD studies, it recognizes the need to consider a broader research paradigm encompassing qualitative and mixed-methods approaches to capture the complexity of the relationship.
In light of the aforementioned considerations, this article addresses the following question: What are the most commonly used terms to describe the AVs of healthcare facilities and the HCOs of people with dementia in EBD studies?
Material and Methodology of Terminology Analysis
The methodology for identifying representative terms consists of four main sections: identifying relevant empirical studies, extracting terms through a concept-based approach, generating datasets with term modifications, and conducting frequency analysis with statistical tests. The goal is to identify key concepts and provide a summary of the most commonly occurring and statistically significant terms. This is illustrated in Figure 1.
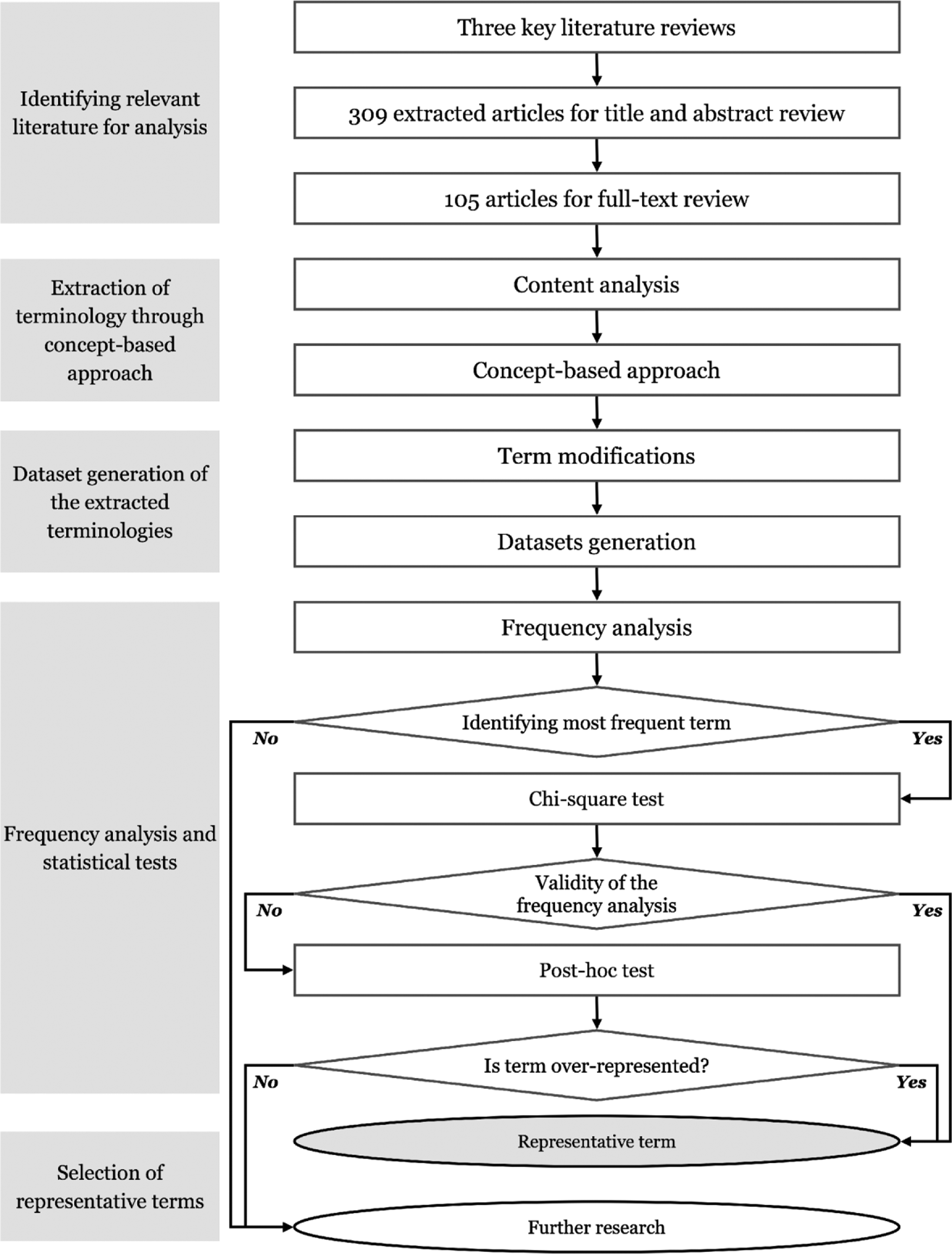
Schematic flowchart of the methodology sections.
The search strategy for this review involved conducting a comprehensive search of relevant literature reviews related to EBD and dementia-friendly design. Three key recent literature reviews were selected and used for this study (listed below). Then, the previous reviews (105 studies) were retrieved for full-text review: The Influence of the Physical Environment on Residents with Dementia in Long-Term Care Settings: A Review of the Empirical Literature (Chaudhury et al., 2018). From Research to Application: Supportive and Therapeutic Environments for People Living with Dementia (Calkins, 2018). Design and the Built Environment for People Living with Dementia in Residential Aged Care (Fleming et al., 2020).
The selection of three key recent literature reviews was based on specific criteria to ensure a comprehensive overview of dementia-friendly design in long-term care facilities. The chosen reviews, all conducted in 2018 or later, were considered the most recent to cover a spectrum of studies, including those featured in previous reviews and the latest publications. Additionally, the reviews were considered comprehensive as they addressed all aspects of dementia-friendly design, distinguishing them from those focusing solely on specific aspects. This selection process aimed to provide the audience with a robust and up-to-date synthesis of research in the field.
Identifying Relevant Empirical Studies for Analysis
To identify relevant empirical studies for analysis, 309 references were retrieved from the three key systematic literature reviews. The title and abstract of each reference were screened based on inclusion and exclusion criteria. Studies were included if they investigated quantitatively the impact of AVs on HCOs for people with dementia, were published in English, and were conducted in long-term care settings or residential aged care facilities such as nursing homes. These types of healthcare facilities are well-investigated in the context of the impact of AVs on HCOs for people with dementia. This could mean that there is a larger body of research, consequently, more data available for analysis in these specific settings. After applying the criteria, 105 studies were selected for full-text review and critical evaluation of the terms applied to AVs and HCOs. Any duplicate studies were removed at this stage.
Terminology Extraction Through a Concept-Based Approach
For terminology extraction, a content analysis was conducted to identify key concepts presented within the empirical studies. A concept-based approach was then applied, which involved identifying and categorizing terms based on their conceptual relevance and relationship to each other. This approach ensured that relevant terms were identified and analyzed in the context of the broader themes and concepts within the literature.
Conducting Content Analysis of Selected Studies
To conduct the content analysis, each of the 105 selected studies was reviewed in detail to identify relevant terms related to the AVs and HCOs investigated. These terms were extracted and recorded in a spreadsheet for further analysis. The content analysis was conducted in two steps: first, each study was reviewed to identify terms used to describe the AVs and HCOs, and these terms were recorded alongside a unique study code. Second, the extracted terms were organized into categories based on their conceptual similarity.
Application of a Concept-Based Approach
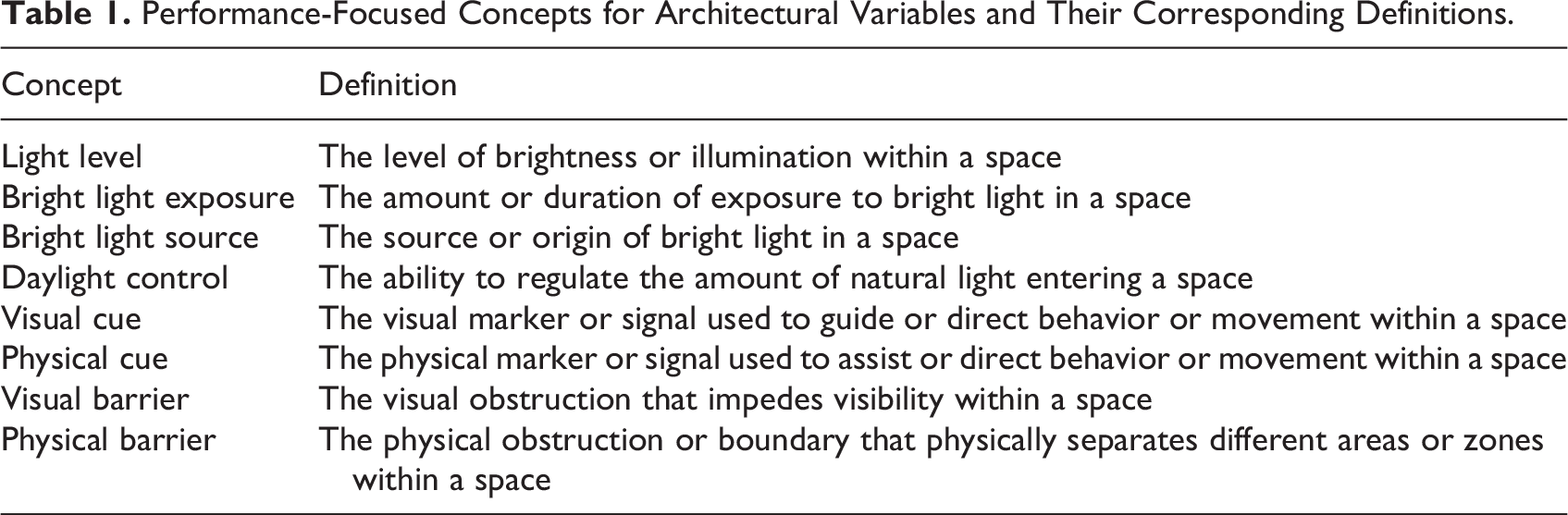
A concept is a general idea or category that encompasses specific instances or variations. For example, the concept of “light level” includes specific instances such as “amount of light,” “indoor light levels,” or “light.” This approach involved identifying the main concepts related to AVs and HCOs examined in the reviewed studies and compiling a list of different terms used by researchers to refer to each concept. Two separate tables were created for AVs and HCOs, listing the concepts along with their corresponding definitions (The list of concepts is presented in Tables 3 and 5, and the list of concepts with their definitions can be found in Tables A2 and A3 in the Supplementary Material). For each concept, a definition and a compilation of various terms used across different studies were established. The concepts were organized into different clusters and presented accordingly. As an illustration, Table 1 demonstrates the cluster of performance-focused concepts for AVs and their corresponding definitions.
Performance-Focused Concepts for Architectural Variables and Their Corresponding Definitions.
Dataset Generation of the Extracted Terms
To create datasets of the extracted terms related to AVs and HCOs, a review process was conducted to refine and clarify the terminology. This review revealed certain sources of variability in terminology. Several modifications were made to the extracted terms to obtain corresponding pure terms to standardize the scope of each concept and reduce variation. Three primary modifications were employed: replacing plural forms with singular forms, using the redundancy argument (i.e., eliminating terms that were found to be redundant or overlapping), and applying the variable-value distinction.
The use of singular and plural forms of terms was recognized as a source of variability. To reduce this variation, plural forms were converted to their corresponding singular forms (e.g., “outdoor environments” was changed to “outdoor environment”). Redundancy refers to the use of multiple terms or phrases to describe the same concept. In the reviewed studies, researchers may have used different words or phrases to describe a particular concept related to AVs and HCOs. To remove redundancy, for instance, the term “salient environmental cues” was simplified to “environmental cue,” while “assisted devices used” was changed to “assisted device.” Another example is the streamlining of “supportive wayfinding features with information necessary for the decision-making process” to “wayfinding feature.”
Another source of variability was the use of variables versus values to describe key concepts. Therefore, a variable-value distinction approach for each concept was applied to enable comparing and synthesizing findings across studies. In empirical research, “variable” refers to an attribute or characteristic that can vary across individuals or contexts. Variables refer to concepts that can change or vary, whereas values refer to specific observations or measurements of those variables (Babbie, 2016; Creswell, 2014; Maxwell, 2012). In this study, the concepts of AVs and HCOs can be considered variables. For example, the concept of “level of light” is a variable because it can be measured using a standardized metric and can vary depending on factors such as the time of day and the location of the light source. On the other hand, a “value” refers to a specific level of a variable, representing a particular measurement at a given point in time or space. Thereby, “high level of light” is a value because it represents a specific level of its variable. Values can also be classified into nominal values (those that represent categories or labels) and ordinal values (those that represent a rank order or hierarchy; Shreffler & Huecker, 2023).
Frequency Analysis Along with Statistical Tests
In the previous sections, the terms for AVs and HCOs have been extracted. Then, through previously described modifications, a dataset of pure terms was generated. This dataset includes a list of terms for each concept and the number of times that researchers used a term in the reviewed studies. Table 2 shows the dataset of pure terms for the concept of “light level” as an example.
Dataset of Pure Terms for the Concept of “Light Level.”
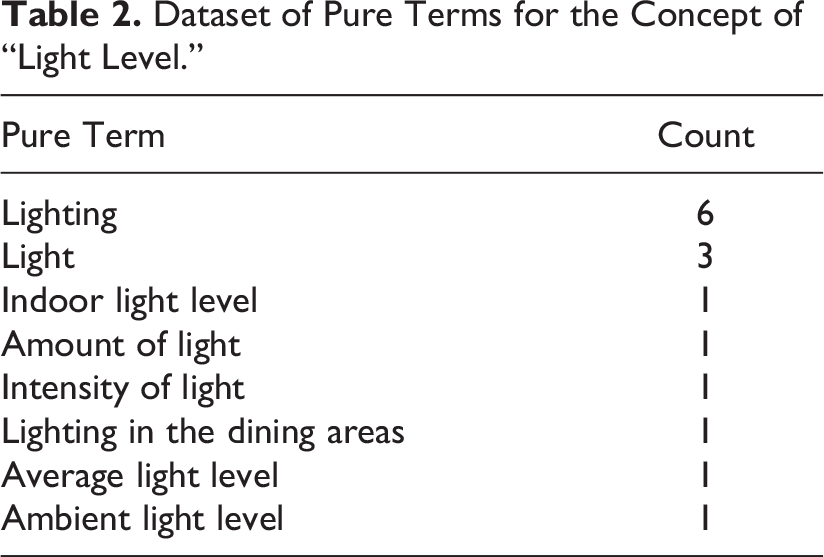
In this table, the “pure term” column lists the individual terms that researchers used to refer to the concept of “light level,” and the “count” column shows the number of times each term was used in the reviewed studies. The table provides a clear and concise way to organize the data and compare the usage of different terms for each concept.
The table is used as a basis for conducting a frequency analysis to identify the most commonly used term for each concept in the reviewed studies. However, relying solely on the observed frequency count is not enough to determine the representative term, as it may be due to chance. Statistical tests are necessary to confirm the results of the frequency analysis. The process involves calculating the observed frequency, relative frequency, and expected frequency of each term, followed by conducting a chi-square (χ2) test to determine if the observed frequencies differ significantly from the expected frequencies.
In this study specifically, the χ2 goodness-of-fit test is used to assess whether the observed frequency distribution of terms differed significantly from the expected distribution. Specifically, to determine whether any terms are significantly more or less frequent than others within the concept, a χ2 goodness-of-fit test with the following hypotheses is performed:
Using the observed and expected frequencies, the χ2 test statistic is calculated for each concept as follows:

where OF is the observed frequency and EF is the expected frequency.
Then, the χ2 test is used to determine if there is a significant difference between the observed and expected frequencies of each term, and the null hypothesis is either accepted or rejected based on the calculated χ2 value and the critical value at a significance level of 0.05. When a significant difference is identified, post hoc tests such as residual analysis are conducted to investigate which specific terms are contributing the most to the significant difference.
The residual analysis, specifically Pearson’s residual, is used to identify which terms are significantly over- or underrepresented in the dataset, aiding in the interpretation of the results. This analysis helps to determine which specific terms have the largest discrepancies between observed and expected frequencies. In this study, the residual analysis was conducted to determine which terms had the most significant discrepancies between observed and expected frequencies in cases where the χ2 test showed a significant difference.
By using Pearson’s residual, which is a common method for residual analysis in contingency tables, as well as calculating the critical value using the following formulas, the post hoc test has been applied:


In this formula, α represents the level of significance (significance level of 0.05), where z(α/2) is the z-score for the desired level of significance (α/2) and sqrt (OF) is the square root of 2 for the observed frequency.
The z-score is a statistical measure that indicates how far an observation is from the mean of a distribution in terms of standard deviations. It is calculated by subtracting the mean from the dataset and dividing the result by the standard deviation. The formula for the z-score is:

where OF is the observed frequency, mean is the mean of the distribution, and SD is the standard deviation of the distribution. By utilizing the above formulas, where the absolute value of Pearson’s residual for a term is greater than the critical value, that term is considered to be significantly different from what would be expected by chance and may be contributing to the overall significant χ2 result. In the following, the results of frequency analysis along with statistical tests that led to the selection of representative terms are presented separately for the concepts of AVs and HCOs. However, for some other AVs and HCOs, it was not feasible to introduce the representative term based on the available datasets. Therefore, further research has been suggested for those concepts.
Results
Representative Terms for the Concepts of AVs
Table 3 presents a list of representative terms for the concepts of AVs. This table was developed based on the selection criteria of frequency analysis, the χ2 test, and a comparison with the critical values for each concept.
Selection of Representative Terms for Architectural Variables.
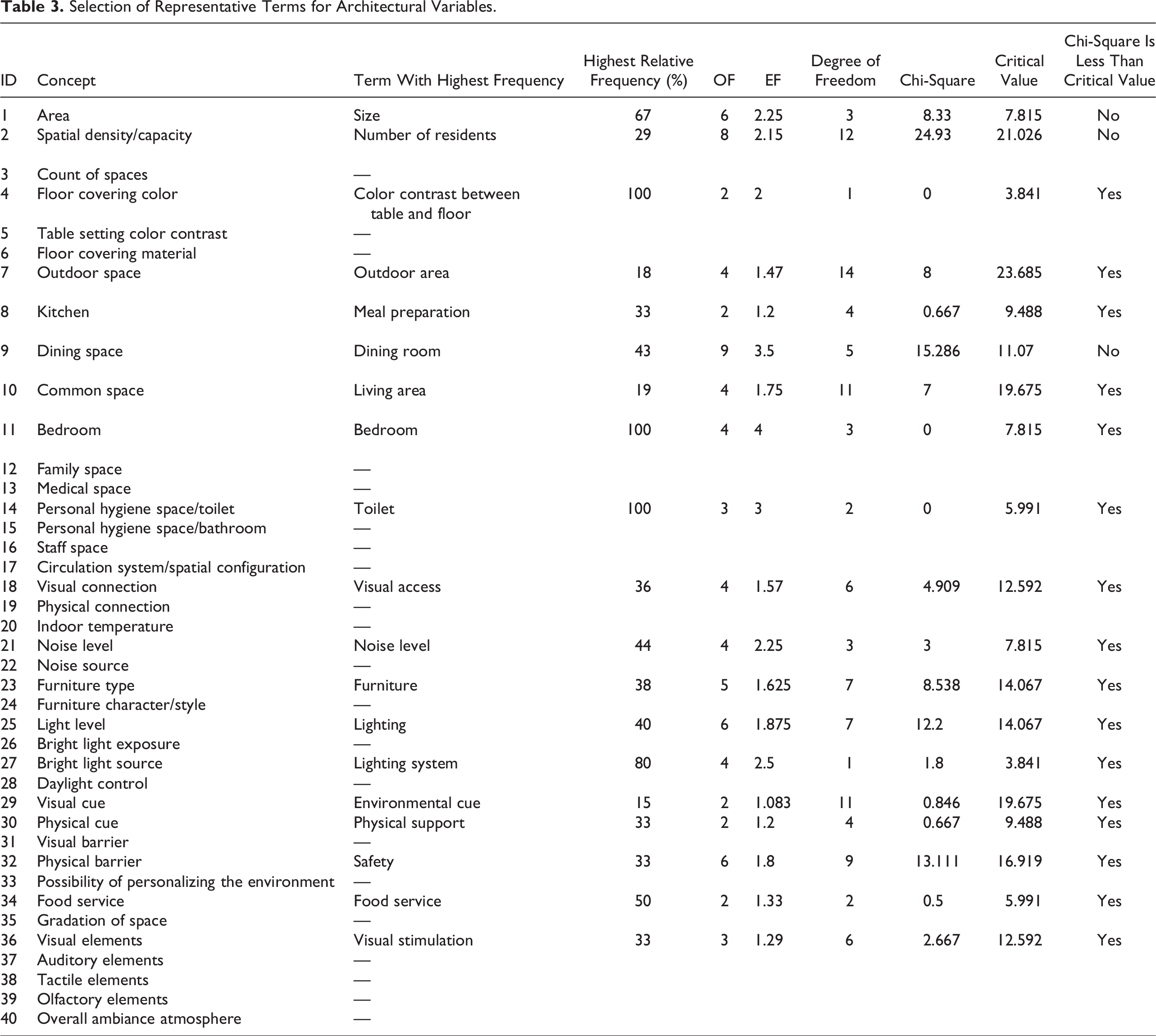
Table 3 presents 40 concepts related to AVs, many of which have representative terms with a high frequency and a positive result in the χ2 test confirming the frequency analysis. However, despite having representative terms, three concepts showed a significant difference between observed and expected frequency according to the χ2 test. These three concepts were further analyzed through a post hoc analysis, and the results are presented in Table 4.
Frequency Analysis and Post Hoc Test Results for Selected Concepts.
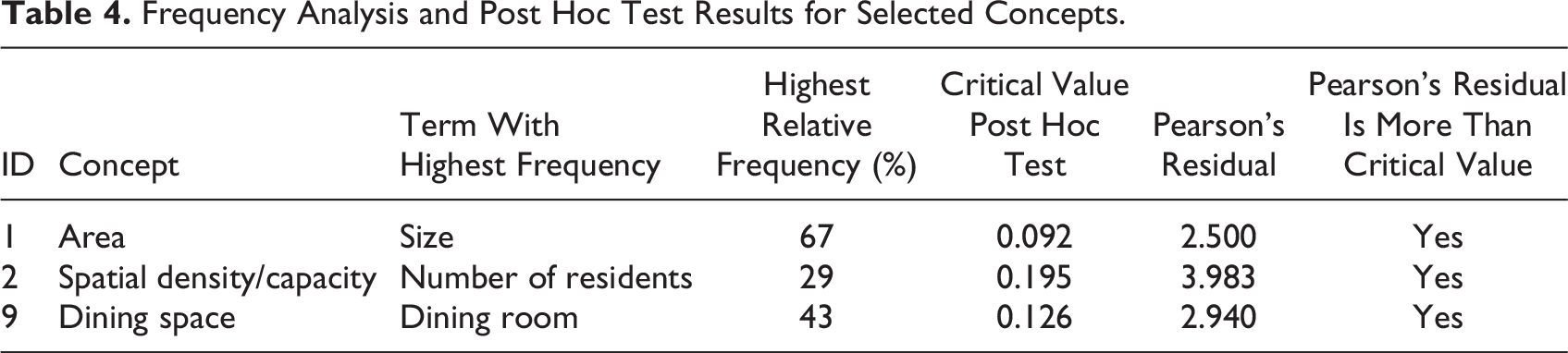
Table 4 presents the post hoc analysis results for three concepts: “area,” “spatial density or capacity,” and “dining space.” The results emphasize the importance of conducting post hoc tests to ensure the validity of the representative term. For example, the term with the highest frequency for the “area” concept was “size,” with a significant Pearson’s residual of 2.500. Similarly, the terms with the highest frequency for the “spatial density or capacity” and “dining space” concepts were “number of residents” and “dining room,” with significant Pearson’s residuals of 3.983 and 2.940, respectively.
Representative Terms for the Concepts of HCOs
The list of representative terms for the HCOs’ concepts is presented in Table 5. This table was generated using selection criteria such as frequency analysis, the χ2 test, and a comparison with critical values for each concept.
Selection of Representative Terms for Health and Care Outcomes.
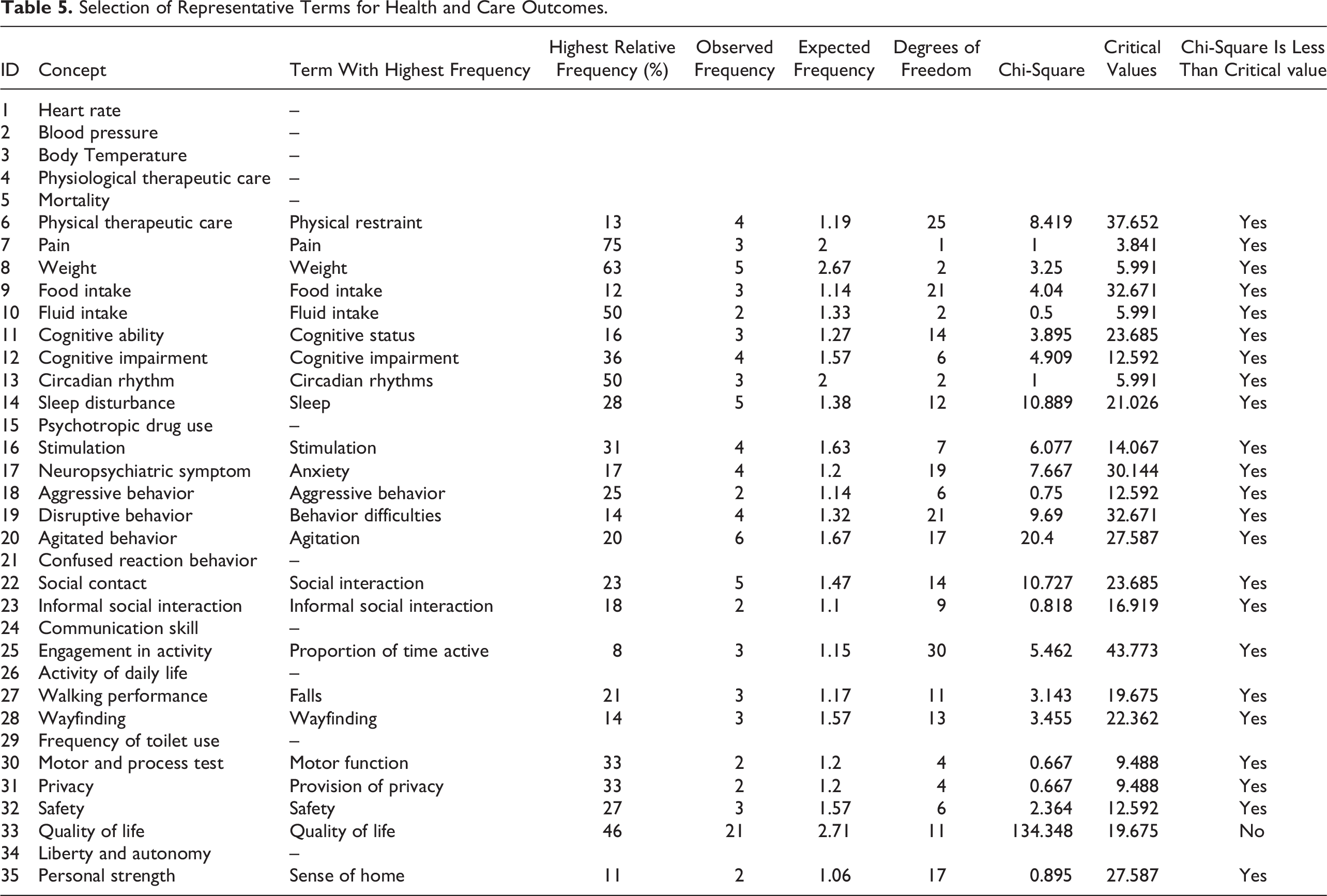
Table 5 displays 35 concepts associated with HCOs, where numerous concepts have representative terms with a high frequency and a positive χ2 test result that supports the frequency analysis. This table also shows that only one of the concepts, “quality of life,” has a significant χ2 test value, indicating that the frequency of the term “quality of life” is significantly higher than expected by chance. The post hoc test also confirmed that this term significantly contributed to the significant difference and is overrepresented in the data. Thus, it can be concluded that “quality of life” is the most frequent term for this concept.
Discussion
The results of the study indicate that there are a variety of terms used in EBD and dementia-friendly design studies to refer to the concepts of AVs and HCOs. This research determined the most commonly used term for each unique concept of AVs and HCOs by selecting terms with the highest frequency. The frequency analysis and χ2 tests provided valuable insights into the terms used to describe AVs and HCOs in the revniewed studies to identify standardized terminologies. The representative terms identified in this study could serve as a valuable resource for future researchers. These standardized terminologies not only ensure consistency in future studies but also facilitate more effective communication and collaboration among researchers.
Contribution to Efforts to Standardize Terminologies
In the field of EBD, there have been previous efforts to standardize terminology. One study critically examined and compared the conceptual meanings and underlying assumptions of EBD and research-informed design to facilitate practical use and theoretical development (Peavey & Vander Wyst, 2017). Ulrich and colleagues proposed a conceptual framework based on literature reviews (Ulrich et al., 2010). Additionally, the Center for Health Design’s Research Coalition initiated a project to create a standardized glossary of environmental terms and healthcare outcome measures. Phase I of this glossary development identified priority areas and common variables linking design elements to healthcare outcomes (Battisto et al., 2023; Quan et al., 2011). Another study aimed to increase awareness of the concept of “design quality” in healthcare architecture and resulted in a taxonomy of themes and terms used in the literature. This taxonomy provides a comprehensive understanding of how researchers, architects, and designers use the concept of design quality in healthcare architecture, with a focus on environmental sustainability, social and cultural interactions, and resilient construction. The study emphasizes the need for clear and explicit definitions of design quality to meet the complex needs of healthcare stakeholders (Anåker et al., 2017).
Just as Anåker et al. (2017) emphasized the need for standardized terminology in referring to design quality, the use of consistent terminology is also crucial in the emerging field of EBD in healthcare facilities, especially in relation to dementia-friendly design. By establishing standardized terminology, this effort aims to promote a more comprehensive and systematic approach to enhance the health and quality of life of people with dementia. One significant contribution of this standardization is facilitating easier interdisciplinary communication and the implementation of research findings into practice. Additionally, it provides a foundation for various practical applications, including the development of an assessment tool. An assessment tool can serve as a valuable resource for designing and evaluating the built environment, specifically in relation to the AVs that influence HCOs and their interrelationships (Calkins et al., 2022; Elf et al., 2017; Golgolnia et al., 2023; Mangili & Capolongo, 2022). The development of standardized terminology, as introduced in this study, lays the groundwork for further analysis, practical applications, and interdisciplinary collaboration in the field of EBD for dementia-friendly environments.
Advantages of Using Variable-Value Distinction Approach
Previous research has employed the variable-value distinction approach to standardize terminology and enhance the consistency of data analysis. By employing pure variables without values, this approach minimizes errors in statistical analysis and enables researchers to concentrate on the core concepts being measured rather than specific measurement values. The findings of Gelman and Hill (2007) and Schwarz and Oyserman (2001) indicated that consistent terminology usage resulted in more reliable and accurate outcomes, particularly in the context of cross-cultural research.
The use of pure terms for variables without values allowed for greater flexibility in analyzing the data and provided a common language for researchers to describe and compare the various concepts related to AVs and HCOs. This approach also enables researchers to easily add new terms to the list of pure terms as new technologies and design innovations emerge in the field. The use of operational definitions, which clarify the meaning of key concepts and distinguish between variables and values, is essential for ensuring the reliability and validity of research findings (Babbie, 2016; Creswell, 2014). The variable-value distinction approach proved valuable in standardizing terminology and reducing variation in the language used to describe AVs and HCOs in the reviewed studies.
Scenarios for Establishing Comprehensive and Standardized Terminology
Based on the result of frequency analysis in this article, Figure 2 in the following shows the number of concepts with unique highest frequencies, the same highest frequencies, and the concepts with the lack of data.
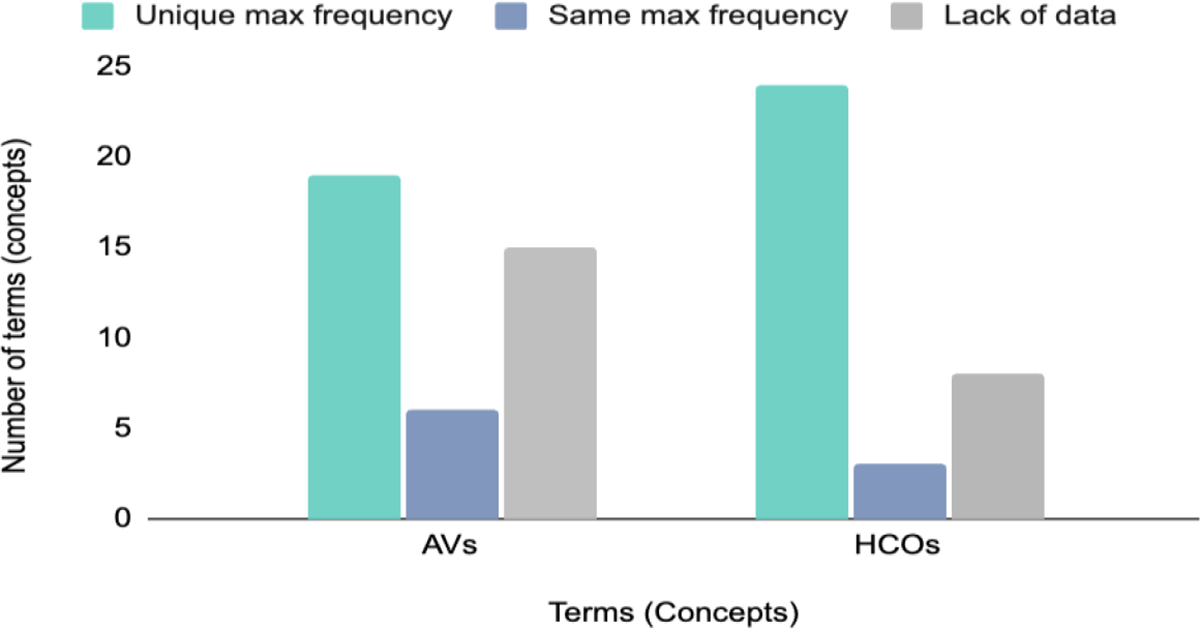
Distribution of frequency analysis results for architectural variables and health and care outcomes concepts.
Although the majority of concepts in both AVs and HCOs groups have representative terms, Figure 2 shows a significant lack of data for some concepts, which is a challenge that needs to be addressed. To address this challenge and develop a comprehensive and standardized terminology for AVs and HCOs, the findings of this study can be used to inform future research. Figure 3 illustrates the entire process of developing a standardized terminology, which includes the part of the process done in this article and the part suggested for future research.
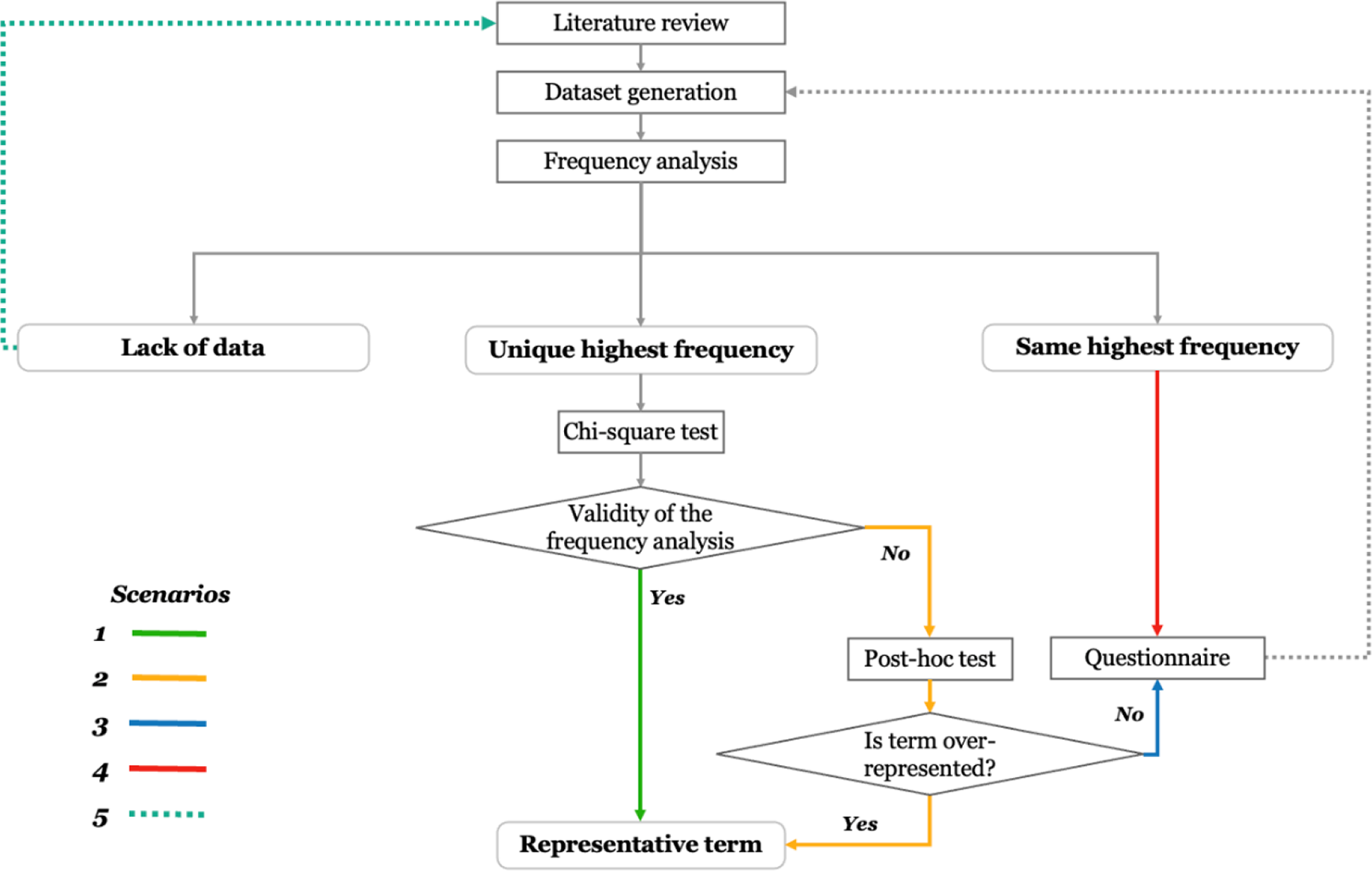
Proposed process for achieving comprehensive standardized terminology for architectural variables and health and care outcomes.
As Figure 3 illustrates, it is required to identify the representative terms for each concept based on their frequency of occurrence in the literature. However, some concepts may have more than one term with the same highest frequency. In such cases, it is proposed to collect additional data from experts’ opinions through a questionnaire and perform a second frequency analysis to determine the most representative term among the terms with the same frequency. Moreover, some concepts may not have enough data to conduct a frequency analysis in the first place. For these concepts, it is suggested to conduct the new literature review with a specific focus area (focusing on the specific concept or a specific cluster of concepts) and generate a new dataset that allows for frequency analysis and finding representative terms.
Figure 3 also outlines how to identify a representative term for each concept based on the frequency analysis conducted in this article. For this purpose, five scenarios can be considered for drawing conclusions based on the result of frequency analysis to identify the most representative term for a given concept.
The first scenario involves identifying a unique highest frequency. If the χ2 test confirms the validity of the frequency analysis, the representative term can be introduced without a post hoc test. A post hoc test is necessary in the second scenario if the χ2 test reveals a significant difference between the observed and expected frequencies. The third scenario suggests conducting further research using a questionnaire if the χ2 and post hoc tests do not confirm the frequency analysis result. The fourth scenario involves multiple terms sharing the same highest frequency, and experts’ opinions are recommended to identify a representative term. Lastly, in the fifth scenario, a lack of data prevents the identification of a representative term, and conducting a further literature review is suggested. In this case, conducting a review in medical literature could be a way to come across with the representative terminologies for HCOs. This process allows for a more robust and statistically rigorous analysis of the frequency distribution of terms for each concept, providing insight into the terms commonly used in the literature on the impact of AVs on HCOs for people with dementia.
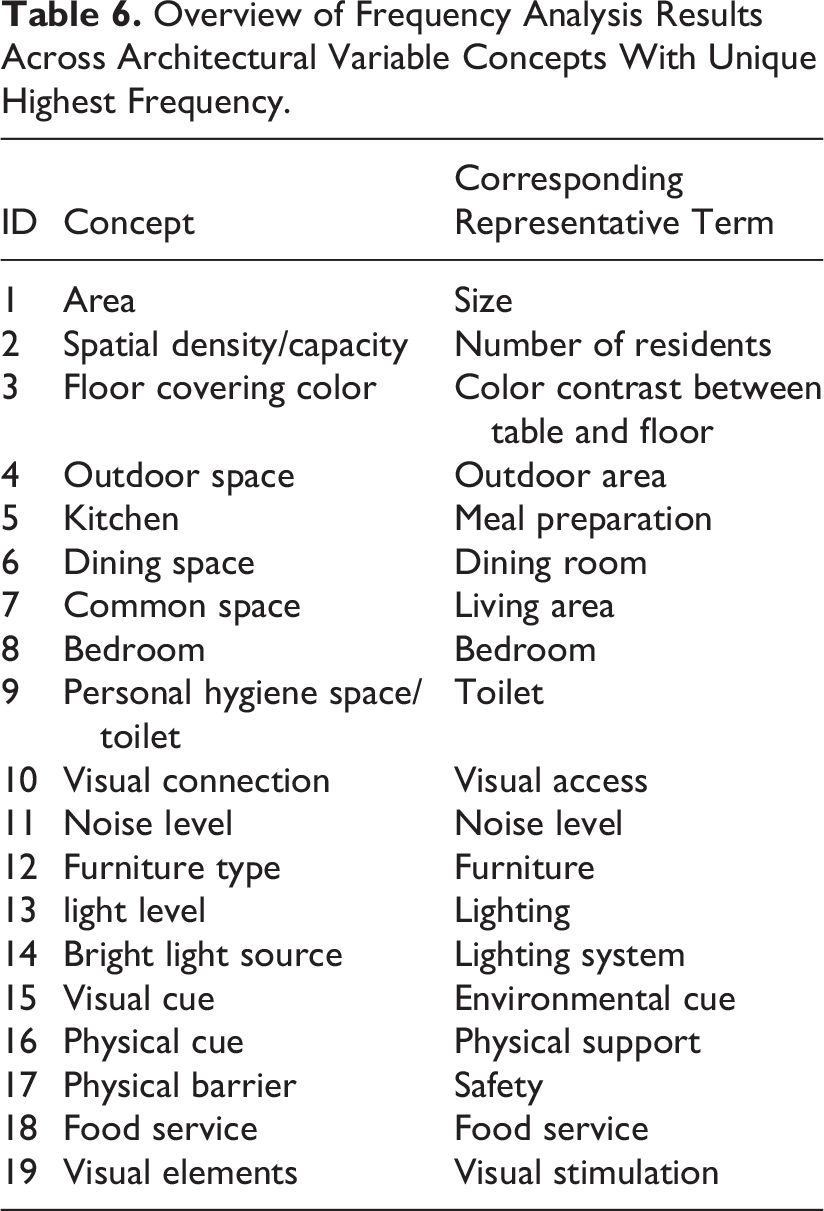
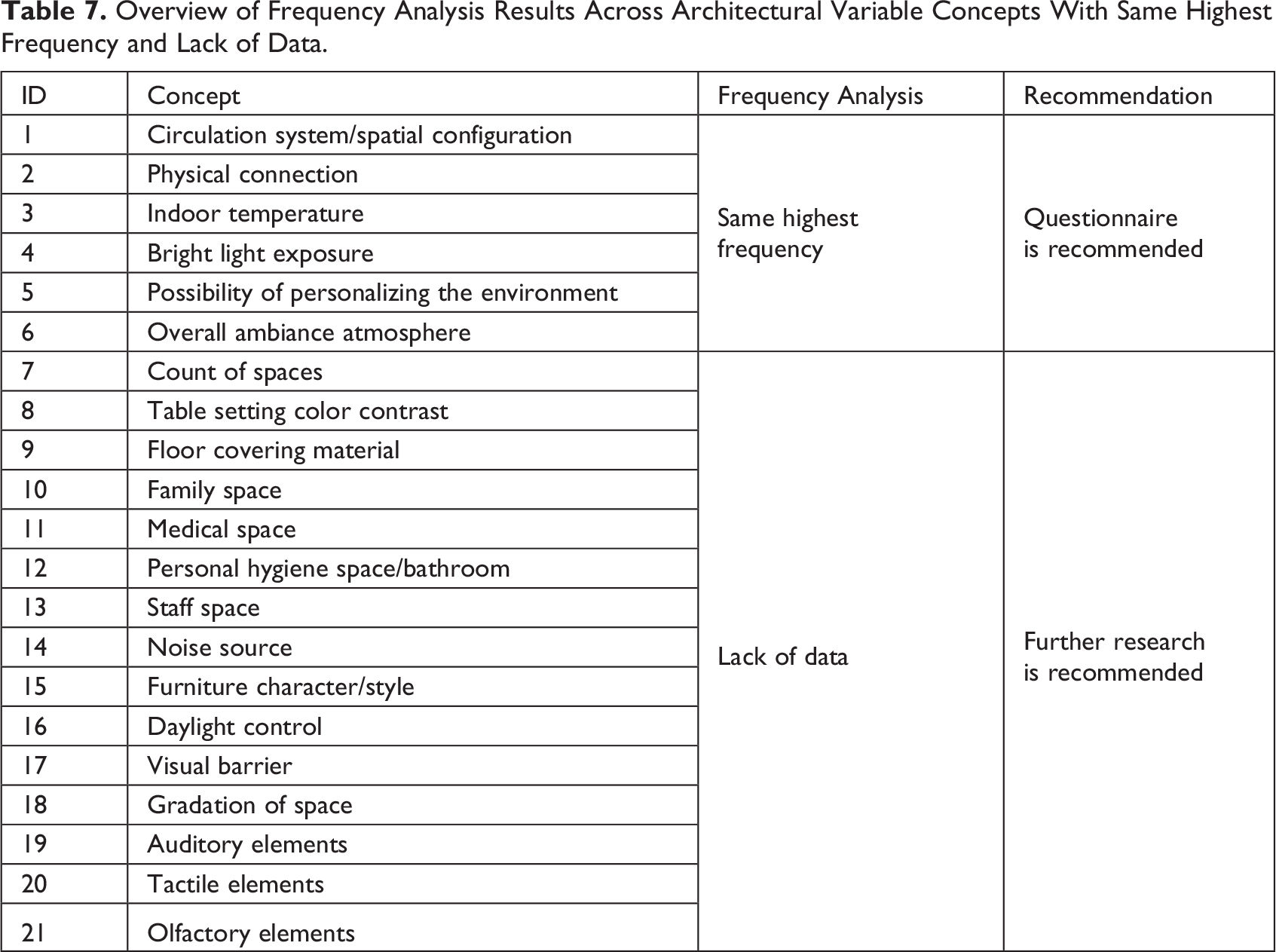
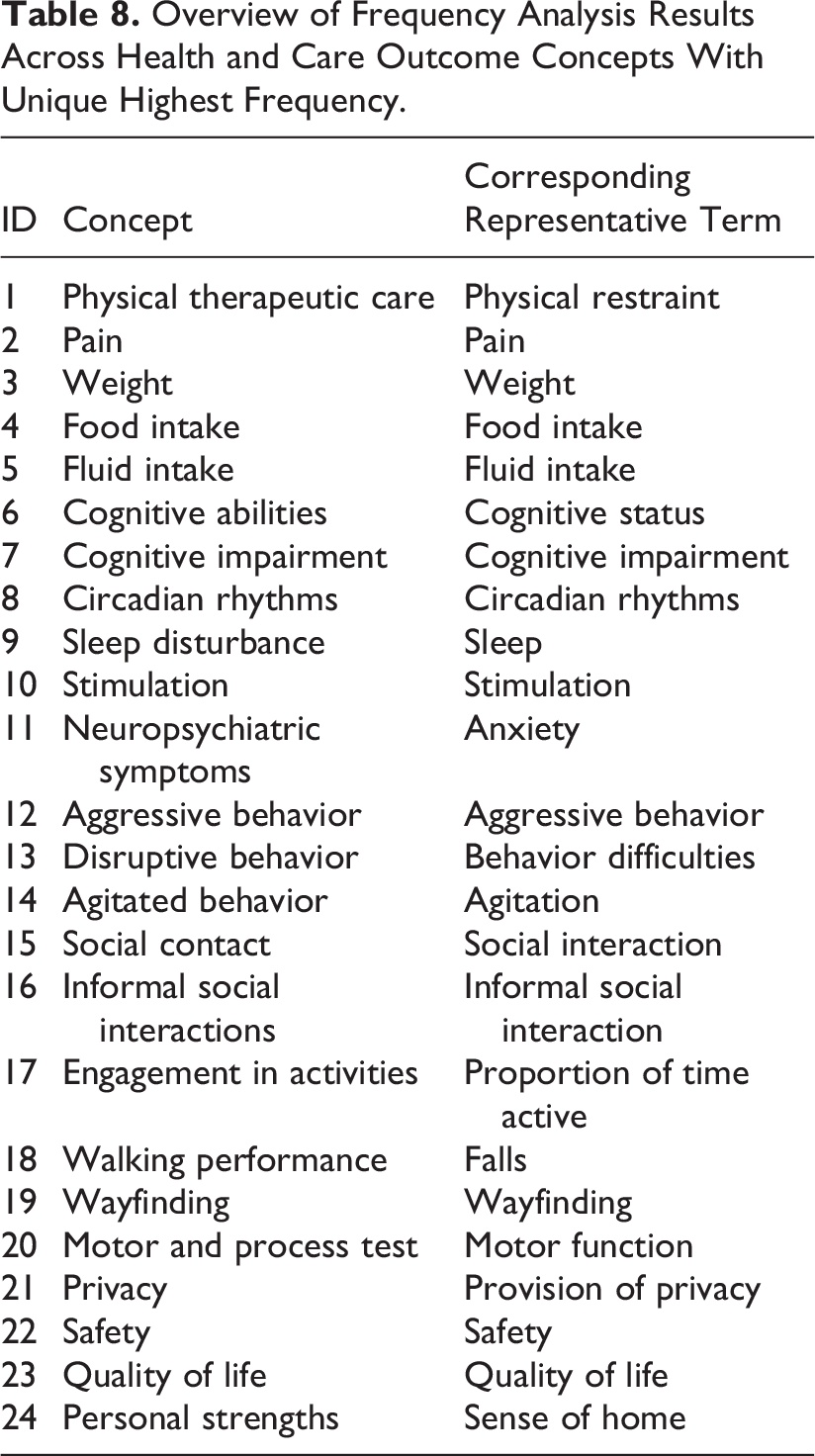
The identification of representative terms for 40 AV concepts and 35 HCO concepts was carried out, suggesting the five-scenario process. The results of this process are summarized in Table 6 and 7 for AV findings and Table 8 and 9 for HCO findings.
Overview of Frequency Analysis Results Across Architectural Variable Concepts With Unique Highest Frequency.
Overview of Frequency Analysis Results Across Architectural Variable Concepts With Same Highest Frequency and Lack of Data.
Overview of Frequency Analysis Results Across Health and Care Outcome Concepts With Unique Highest Frequency.
Overview of Frequency Analysis Results Across Health and Care Outcome Concepts With Same Highest Frequency and Lack of Data.
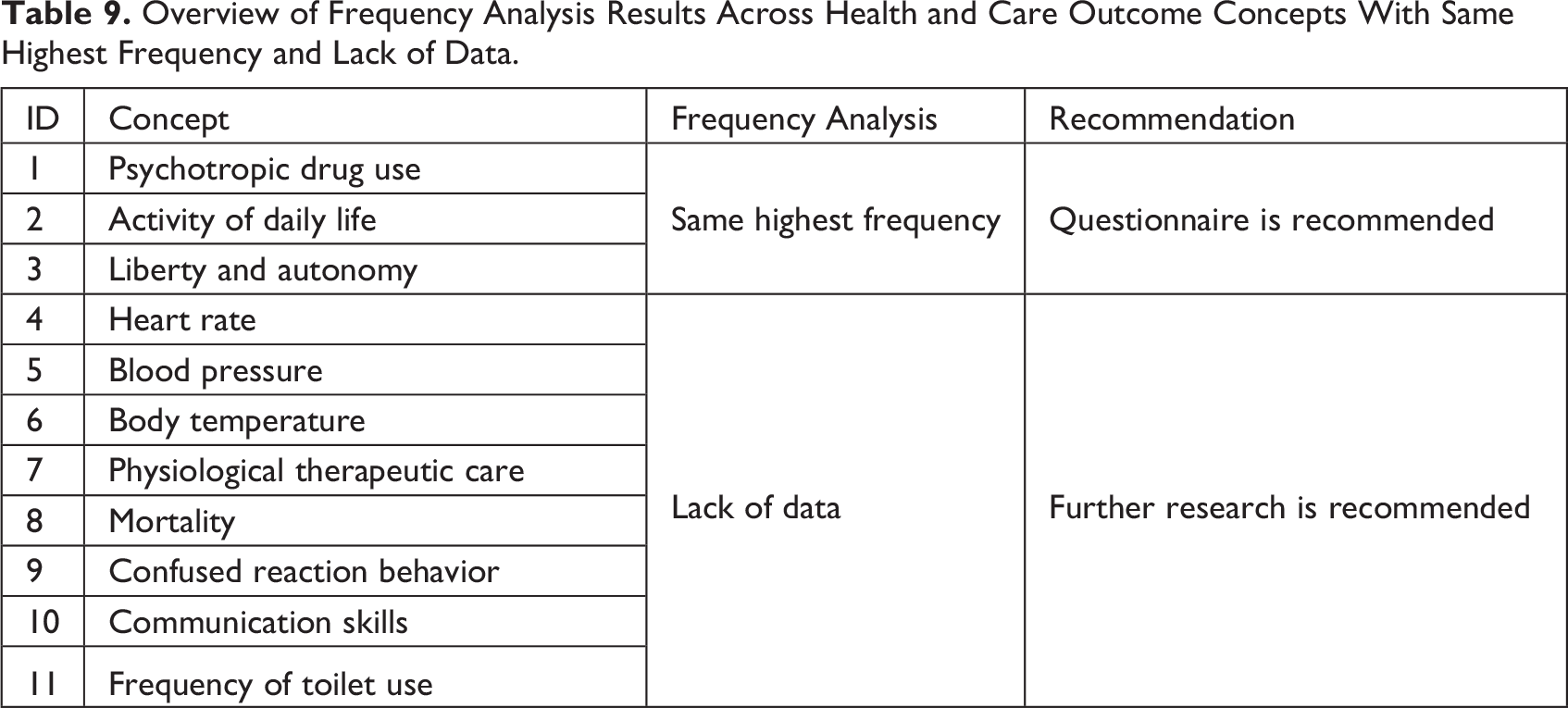
Among the AV and HCO concepts, in addition to the concepts that resulted in the unique highest frequency in which their representative terms are introduced, there were instances where multiple terms had the same highest frequency. In such cases, seeking expert input to determine a representative term is recommended. Additionally, there was insufficient data for certain AV and HCO concepts to conduct a comprehensive frequency analysis. In these instances, some concepts had terms with a frequency of 1 before and after term modification, while others had only one term identified after reviewing the studies. This lack of diversity in terminology poses challenges for conducting reliable frequency analysis and drawing meaningful conclusions. Therefore, further research with a specific and focused approach is necessary. This research should aim to gather additional terms and data, enabling the identification of representative terms and the establishment of standardized terminology.
Overall, the selection of representative terms based on frequency analysis is an essential step in this research that ensures the validity and reliability of the findings. By selecting representative terms, a clear understanding of the language used as AVs and HCOs in the reviewed studies is obtained, and the criteria used for selection provide transparency and reproducibility in future studies.
Strengths and Limitations
This article has identified and addressed several important concepts and their associated terms related to AVs and HCOs. One of the key strengths of this study lies in its utilization of the variable-value distinction approach, which has proven valuable in standardizing terminology and reducing variation in the language used to describe AVs and HCOs across the reviewed studies. This approach has introduced representative terms, laying the groundwork for further analysis and practical application. Furthermore, this study contributes to the development of standardized terminologies by comprehensively analyzing the concepts, their frequency, and the statistical significance of their associated terms. This serves as one of the first steps toward promoting consistency and clarity in the field.
However, it is important to acknowledge the limitations of this study and address potential criticisms. The research paradigm adopted in this article leans toward a positivist perspective, primarily focusing on quantitative analysis of the relationship between the built environment and human outcomes. It is crucial to recognize that the relationship between the built environment and human outcomes can be nuanced and multifaceted, requiring a broader range of research approaches to capture its full complexity. While this study contributes to the advancement and standardization of terminology in the domain of EBD, it is essential to recognize the need for complementary qualitative research and a more comprehensive understanding of the subjective experiences and qualitative aspects related to AVs and HCOs.
Furthermore, this study has inherent limitations that should be considered. The subjective judgments involved in defining and labeling concepts may introduce bias or inconsistency in the analysis. The focus of this study is limited to dementia-friendly design, which may restrict the generalizability of the results to other contexts within the broader field of EBD. However, the framework and methodology presented in this article provide a foundation that can be expanded upon in future research to encompass a more diverse range of studies, allowing for a more comprehensive and inclusive understanding of terminology standardization in the field of EBD.
Conclusion
This article provided a comprehensive analysis of the terms used in the EBD studies to refer to the concepts of AVs and HCOs in the dementia-friendly design field and to generate a list of representative terms for them through content and frequency analysis along with the statistical tests. The results of this study indicate that standardizing terminology related to AVs and HCOs is essential for effective communication and the comparison of findings across different studies. The majority of representative terms were easily identifiable, indicating general agreement among researchers in the field. However, it is important to acknowledge the need for further investigation in cases where the observed frequencies did not result in the introduction of representative terms. In such cases, questionnaires and specific area-focused systematic reviews can provide a more comprehensive understanding of the appropriate representative terms. The findings of this study contribute to the development of EBD research by providing a standardized terminology for the concepts of AVs and HCOs and a foundation for future research exploring the potential benefits of incorporating AVs into healthcare design to improve HCOs for people with dementia.
Implications for Practice
Standardizing terminology in EBD research can improve communication and collaboration among researchers, practitioners, and stakeholders. Using standardized terminology can facilitate the comparison of findings across different studies, enhancing the generalizability of results. The development of EBD guidelines can be supported by the standardization of terminology. Further investigation may be needed in cases where representative terms are not easily identifiable. Incorporating architectural variables into healthcare design can potentially improve health outcomes for people with dementia.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231225395 - Are We Speaking the Same Language? Terminology Consistency in EBD
Supplemental Material, sj-pdf-1-her-10.1177_19375867231225395 for Are We Speaking the Same Language? Terminology Consistency in EBD by Tahere Golgolnia, Maja Kevdzija and Gesine Marquardt in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.