
Abstract
Objective:
This study aims (1) to understand the needs and challenges of the current intensive care unit (ICU) environments in supporting patient well-being from the perspective of healthcare professionals (HCPs) and (2) to explore the new potential of ICU environments enabled by technology.
Background:
Evidence-based design has yielded how the design of environments can advocate for patient well-being, and digital technology offers new possibilities for indoor environments. However, the role of technology in facilitating ICU patient well-being has been unexplored.
Method:
This study was conducted in two phases. First, a mixed-method study was conducted with ICU HCPs from four Dutch hospitals. The study investigated the current environmental support for care activities, as well as the factors that positively and negatively contribute to patient experience. Next, a co-creation session was held involving HCPs and health technology experts to explore opportunities for technology to support ICU patient well-being.
Results:
The mixed-method study revealed nine negative and eight positive patient experience factors. HCPs perceived patient emotional care as most challenging due to the ICU workload and a lack of environmental support in fulfilling patient emotional needs. The co-creation session yielded nine technology-enabled solutions to address identified challenges. Finally, drawing from insights from both studies, four strategies were introduced that guide toward creating technology to provide holistic and personalized care for patients.
Conclusion:
Patient experience factors are intertwined, necessitating a multifactorial approach to support patient well-being. Viewing the ICU environment as a holistic unit, our findings provide guidance on creating healing environments using technology.
Keywords
Introduction
Staying in the intensive care unit (ICU) is known to be highly stressful and traumatic for patients due to their critical condition as well as medical procedures, pain, and a disturbing environment (Egerod et al., 2015). Stressful ICU experiences negatively affect patients’ health outcomes during and after an ICU stay. Patients with stressful ICU experiences are more likely to develop delirium (Zaal et al., 2013), stay longer in the ICU (Gruenberg et al., 2006; May et al., 2021), and suffer from cognitive impairment (Davydow et al., 2013) and postintensive care syndrome (Granja et al., 2005; Parker et al., 2015) significantly reducing quality of life (Maley et al., 2016; Oeyen et al., 2010). Next to that, studies (Goldfarb et al., 2017; Nielsen et al., 2019; Ulrich et al., 2004) have shown that positive ICU experiences result in better health outcomes. These results highlight the need to promote patient experience and, more specifically, patient well-being in the ICU as a means to support healing and recovery.
Well-being in general refers to the state of individuals where they feel happy, healthy, and satisfied with their life (Ryan & Deci, 2001). The concept of well-being, therefore, goes beyond the traditional biomedical view of health which is considered as the absence of disease; it comprises various dimensions of an individual’s life including their physical, mental, social, and environmental status (Kiefer, 2008; Ryan & Deci, 2001). For instance, a person with a leg impairment could still experience well-being as long as personal values, such as a sense of autonomy or flourishing, are fulfilled. Taking this holistic view, well-being is relevant and achievable in the context of critical care, provided that patients are in an environment that supports what is important for their well-being.
The understanding that the environment has an effect on the healing and well-being of patients sparked the design of healing environments. A healing environment refers to the entire context surrounding patients that promotes health and well-being by catering to their physical, mental, social, and spiritual needs (Sakallaris et al., 2015). To effectively design healing environments, evidence-based design (EBD) approaches have been used: empirical evidence on how the design of physical environments can promote better clinical outcomes. EBD has been applied to various environmental factors ranging from space layout to sound and natural light in the space that affect physical (e.g., injuries, effectiveness, infection, sleep) as well as psychological (e.g., stress, privacy, satisfaction) components (Sakallaris et al., 2015).
A relatively new development in this area is the use of digital technology. This has expanded and diversified the role of environments in supporting patient well-being. For instance, an interactive immersive projection technology extends what physical surfaces of the environment can offer beyond color and texture. It creates dynamic visual stimulation that can change over time and, hence, can accommodate changing emotional needs of patients by providing stimuli that evoke high or low arousal (Maltha, 2022). The role of sound in healing environments can go beyond noise reduction by actively comforting patients through positive sound tones conveying messages from loved ones (Özcan et al., 2021). As such, digital technology opened up new avenues for EBD in healing environments. Previous review papers have outlined the implications of technology in supporting patients’ healing and well-being (Cox & Curtis, 2016; Kim et al., 2021; Silvera-Tawil et al., 2020; Smits et al., 2022). However, the new potential of designing healing environments facilitated by technology remains largely unexplored. To optimize the environmental support in the ICU, obtaining a comprehensive view of the fundamental care needs of patients and HCPs in the ICU is important. Several studies looked into ICU patient experiences, of which most studies focus on barriers to patient experiences (Abuatiq, 2015; Krampe et al., 2021; Zengin et al., 2020) and some include also facilitators (Jakimowicz et al., 2017; Samuelson, 2011). In both cases, there was only limited focus on the influence of environmental factors. Furthermore, most of these studies derived insights primarily from ICU patients who reportedly struggle to recall and reflect upon their experiences (Ethier et al., 2011). Therefore, in this study, we focus on the perceived experiences of healthcare professionals (HCPs) who have frequent and collective interactions with patients and explore how technology could support creating a healing environment that provides holistic and optimal care for ICU patients.
Phase I: Understanding ICU Patient Experience From the Perspective of HCPs
Method
Study design, Participants, and Settings
To explore the role of the ICU environment on patient well-being, we designed a mixed-method study consisting of an online survey and an online semi-structured follow-up interview. The online survey aimed to investigate how current ICU environments support care activities and patient experience and identified factors that positively and negatively contribute to these aspects. A follow-up interview was carried out to gain a more in-depth understanding of patient needs and challenges experienced by HCPs in relation to different care activities. All methods described in this section were approved by the Ethics Committee of the University of Twente, the Netherlands (reference number: 2021.110).
HCPs from four Dutch hospitals (two academic and two nonacademic) participated in the study. A total of 27 HCPs completed the online survey: 13 from academic hospitals and 14 from nonacademic hospitals. All HCPs work in adult ICUs including medical and surgical, thorax, and cardiothoracic ICUs. The majority of HCP participants were ICU nurses (n = 22) followed by intensivists (n = 4), and anesthesiologists (n = 1). Most participants had more than 10 years of experience (n = 19, 70%). A total of six of 27 survey participants took part in the follow-up interview. These were five ICU nurses (two from academic and three from nonacademic hospitals) and one intensivist (from a nonacademic hospital), all with at least 5 years of experience.
Procedure
The link to the online survey was shared on the internal newsletter of each hospital ICU department. To lower language barriers, participants could choose either an English or Dutch version. Each participant had to provide their consent on the opening page of the online survey before proceeding with the questionnaire. The online survey included both closed- and open-ended questions covering the following topics: the perceived level of environmental support of the ICU on (1) the patient (affective) experience, (2) different care activities, and (3) factors that either positively or negatively contribute to the patient experience. To assess the affective qualities of the ICU, environmental factors contributing to patient experience were derived from healing environment literature (DuBose et al., 2018; Huisman et al., 2012; Simonsen et al., 2022; Verderber et al., 2021). A total of 13 items were selected and used in the questionnaire list. Using this list, HCP participants assessed the perceived level of environmental support in their ICUs on patient experience on a 7-point Likert-type scale and describe the rationales. To understand the influence of the current ICU environment on care activities, we created an overview of ICU activities using the data from our previous observation study with two hospitals participating in the present study. The list of these activities was used to evaluate environmental support in the ICU for patients and HCPs. To explore patient experience, we used a mood measurement tool as mood state can be an indicator of a person’s overall subjective experience (Desmet, 2015). ICU-relevant positive and negative mood states were selected based on patient experience literature (Halvorsen et al., 2022; Krampe et al., 2021) and an adapted version of the mood measurement tool, Pick-A-Mood (PAM; Desmet et al., 2012), was used. HCPs were asked to describe which mood they most frequently see in their patients and what factors contribute to such moods (see Figure 1 for an example question from the online survey). To expand the knowledge of both positive and negative factors contributing to patient experience, HCPs were also asked to describe when patients are in positive and negative moods and what contributed to these moods to their knowledge. The average time spent on the online survey was 15 min.
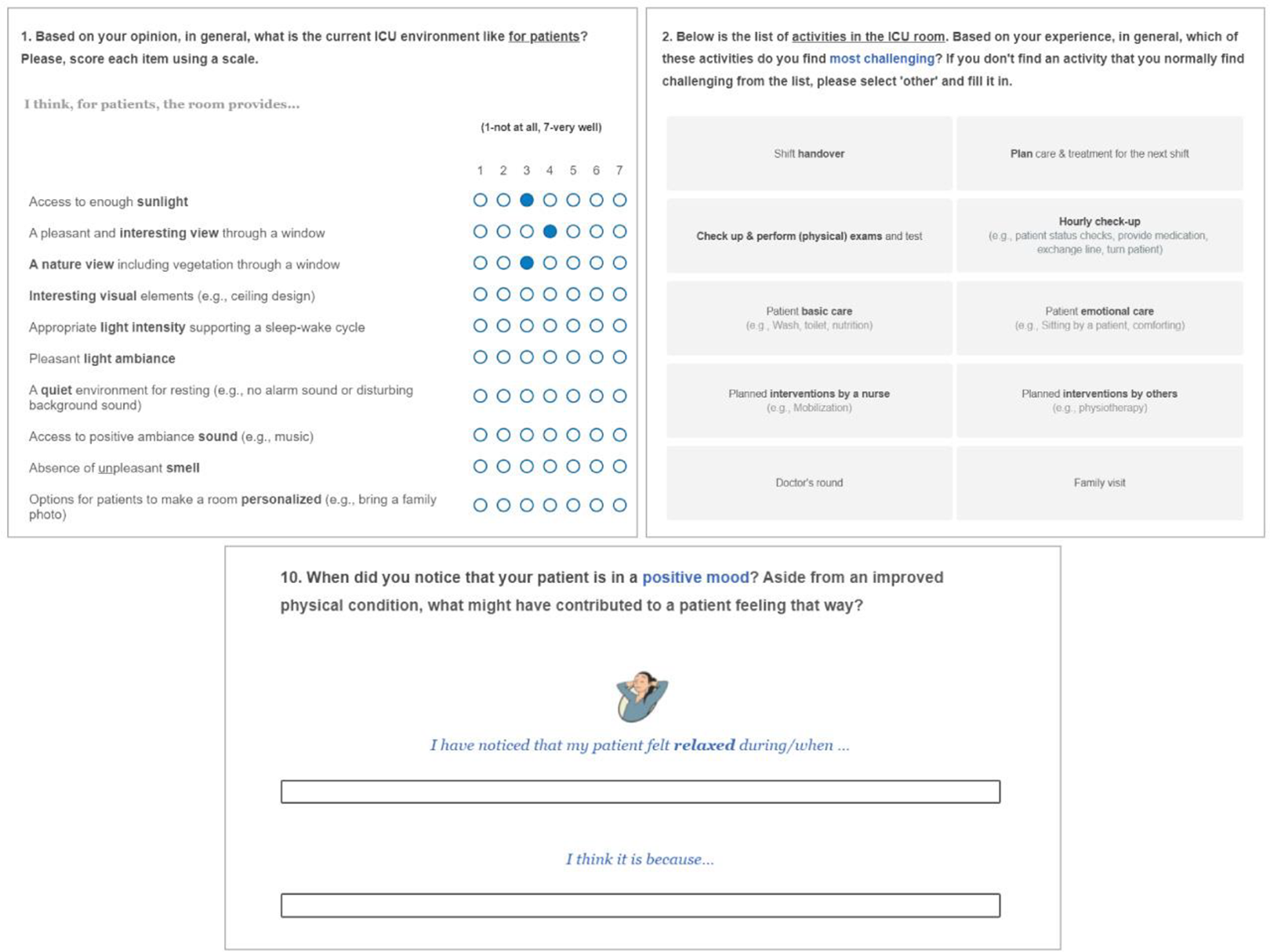
Screenshots of our online survey. Source: Illustration used in the survey from the Pick-A-Mood pictorial tool. Used with permission Desmet et al. (2016). Pick-A-Mood Manual. Delft University of Technology, Delft.
Participants could indicate whether they were interested in taking the online follow-up interview. Interested participants provided a convenient time to schedule the interview. A 30-min follow-up interview consisted of detailed questions about factors that contribute to the patient experience and related needs.
Analysis
Online survey data were collected via Qualtrics (www.qualtricsc.com) and the follow-up interview data were recorded and transcribed using Microsoft Teams (www.Microsoft.com). Responses to open-ended questions of the online survey and interview transcripts were systematically analyzed following the principles of reflective thematic analysis (Braun & Clarke, 2006). The relevant data were organized and analyzed using open, axial, and selective coding techniques. First, codes were made by the first author and reviewed and discussed with the second author. These codes captured information relevant to the factors contributing to the entire positive or negative experiences of patients. An agreement on the code was reached by an iterative analysis process. Finally, codes related to the same concept were grouped into categories and themes were identified.
Results
Environmental Support for Care Activities in the ICU
The majority of the HCPs perceives emotional care (e.g., sitting with patients, comfort talk) as the most challenging care activity (n = 9) followed by dealing with emergency situations (n = 6) and performing planned intervention by a nurse (e.g., mobilization; n = 4; see Table 1).
Most Challenging Intensive Care Unit (ICU) Activities According to Healthcare Professionals (HCPs).
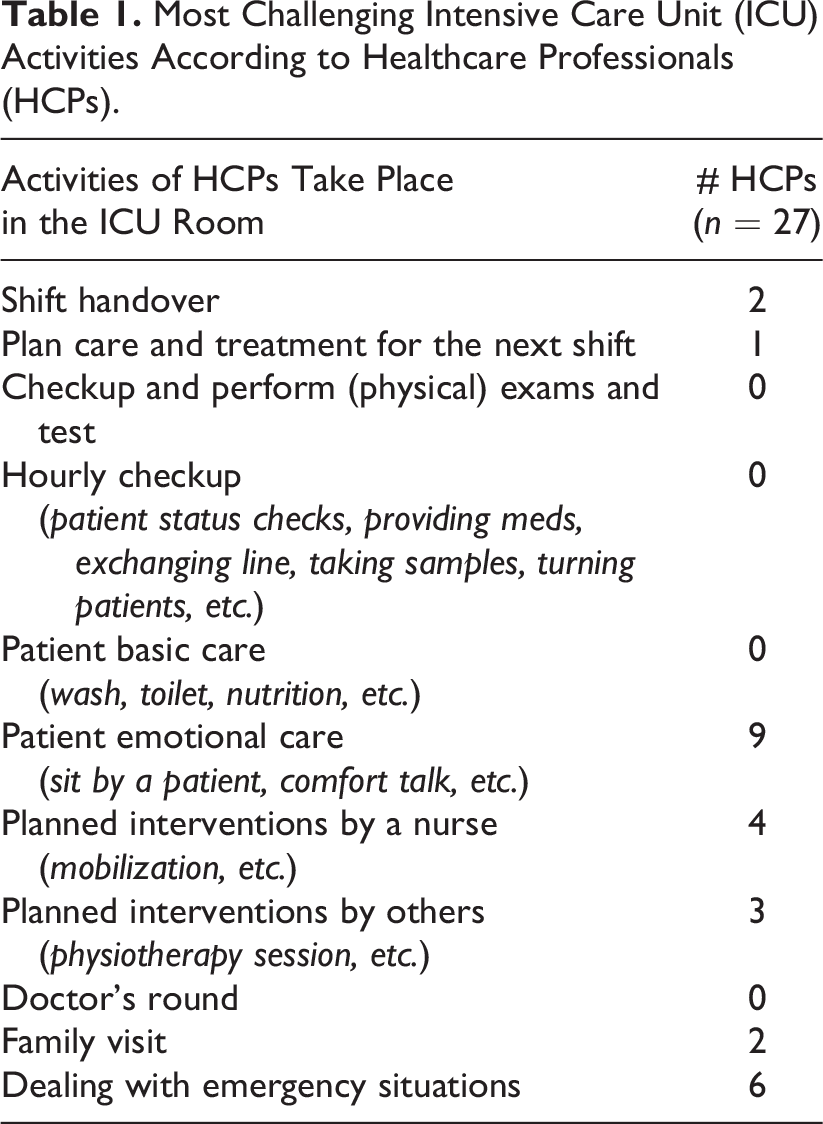
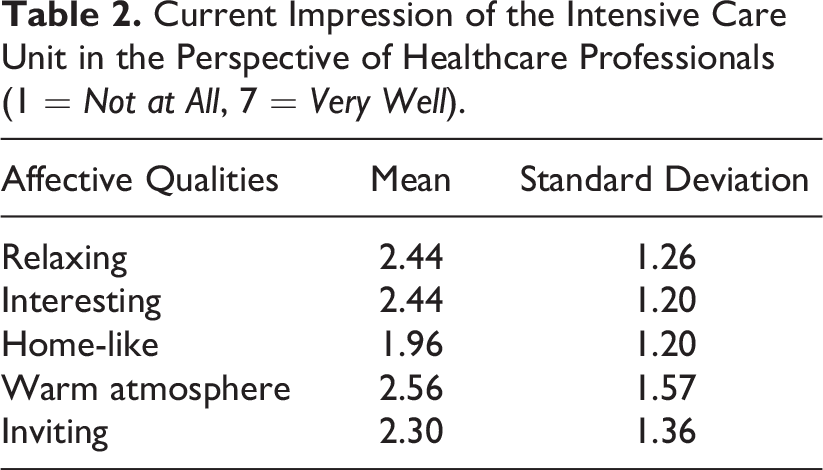
Both ICU nurses and intensivists most frequently mentioned lack of time as a reason for emotional care being challenging: “Because of shortage of staff and time pressure, there is not always time to provide emotional support even though I think it is really important for my patients” (P1, Nurse). “All other activities occur at a specific moment during the shift. For doctors, there is no indicated time for emotional care. It is a challenge to make room for that” (P3, Intensivist). Also, providing patient emotional care was challenging because of the lack of a proper environment such as “Many interruptions and hostile environment” (P6, Nurse). Lack of privacy was another factor: “There is little personal space for the patient and his or her emotions (in a multipatient room). If you want to separate the bed in the room, your only option is to close the curtains” (P5, Nurse). Lastly, difficulties in communication were mentioned: “Because of their inability to speak, it’s not clear whether the patient understands what I am saying” (P1, Nurse). Importantly, although the environment could play an important role in fulfilling the emotional needs of patients, the results showed that the current ICU fails to convey affective qualities as all scores remain below 3 of 7 (e.g., home-like and inviting; see Table 2).
Current Impression of the Intensive Care Unit in the Perspective of Healthcare Professionals (1 = Not at All, 7 = Very Well).
The scores of positive environmental stimuli (Table 3) show how the current ICUs in general lack positive stimuli such as an interesting view, nature view, positive ambiance sound, and interesting (interior) design elements while abounding with elements that can interfere with emotional care for patients: “There is a window in every patient room, but you can only see the wall of the hospital building” (P6, Nurse), “Our ceiling is just white” (P5, Nurse), and “The room is filled with different kinds of clinical equipment. They are so visible and make a lot of noise. It’s far from a homely feeling” (P2, Nurse).
Positive Environmental Factors in the Intensive Care Unit Grouped into Five Themes (1 = Not at All, 7 = Very Well).
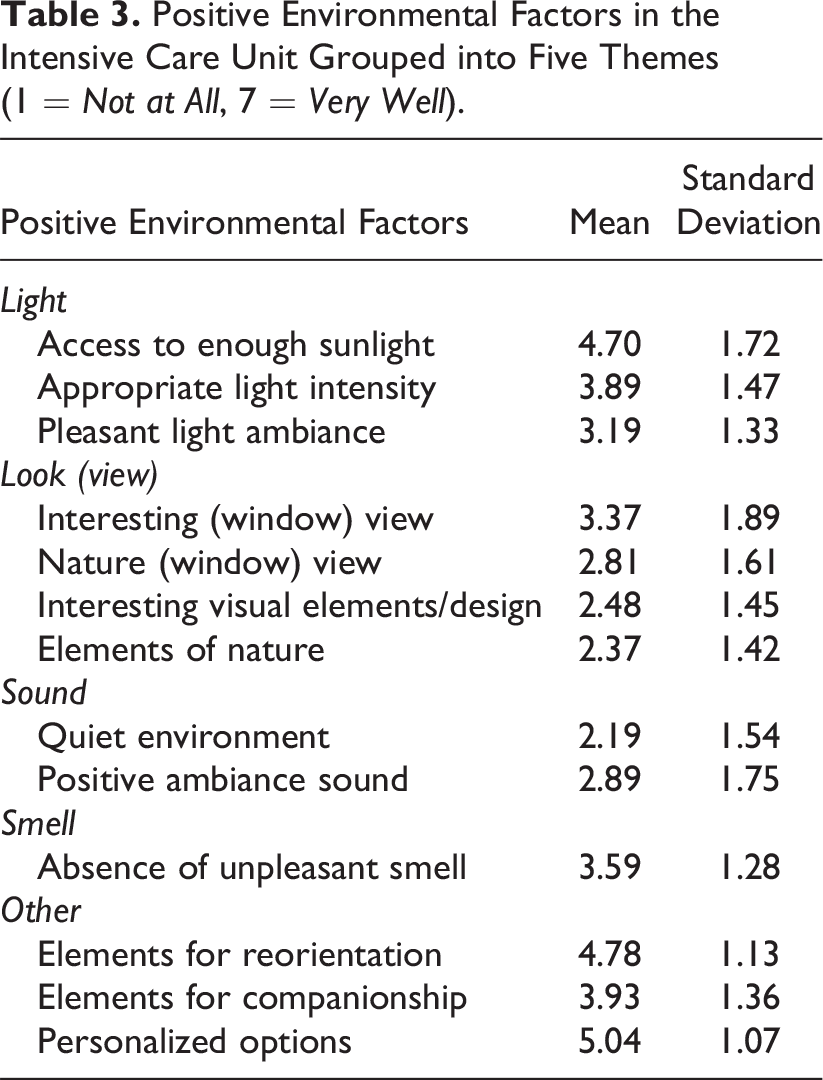
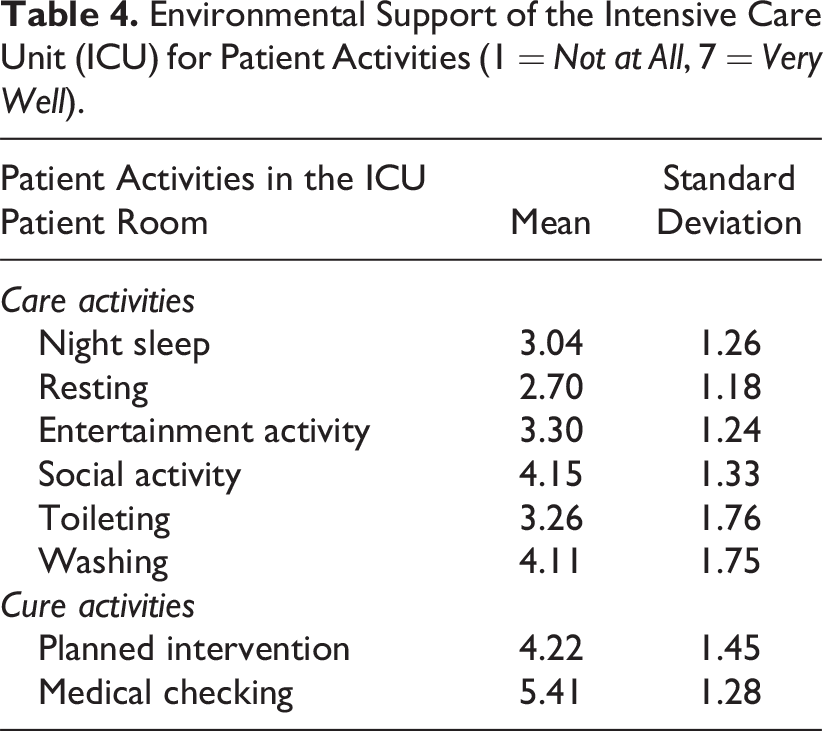
Table 4 describes how HCPs perceived environmental support for diverse patient activities in the ICUs, which we divided into “cure activities” and “care activities.” Cure activities are directed toward treating the patient’s illness or condition, such as planned interventions. The results showed that the current ICU environment effectively supports cure activities, scoring high in both medical checking (mean = 5.41, SD = 1.28) and planned intervention (mean = 4.22, SD = 1.45). On the other hand, the current ICU environment shows inadequate support for care activities, which are aimed at enhancing patients’ overall well-being and comfort, especially activities aimed at restoration including resting (mean = 2.70, SD = 1.18) and night sleep (mean = 3.04, SD = 1.26). “There is always the sound of monitors, ventilators, and talking that are keeping patients awake” (P2, Nurse). “There is too much light (for patients to sleep). Lights are switched on when we enter the room” (P1, Nurse).
Environmental Support of the Intensive Care Unit (ICU) for Patient Activities (1 = Not at All, 7 = Very Well).
ICU Patient Experience and Contributing Factors
According to HCP’s, ICU patients predominantly experience negative mood states: tense (n = 11, 42%), sad (n = 7, 27%), and bored (n = 3, 12%). Nine factors contributing to the patients’ negative mood were identified from the analysis of the open-ended questions in the online survey and interview. These factors were categorized into two groups: psychological and physical factors. Table 5 presents an overview of these factors with the quotes from HCPs and the number of mentions.
Nine Factors Contributing to Negative Intensive Care Unit Patient Experiences and Their Subcategories With Example Quotes From Healthcare Professionals and the Number of Mentions.
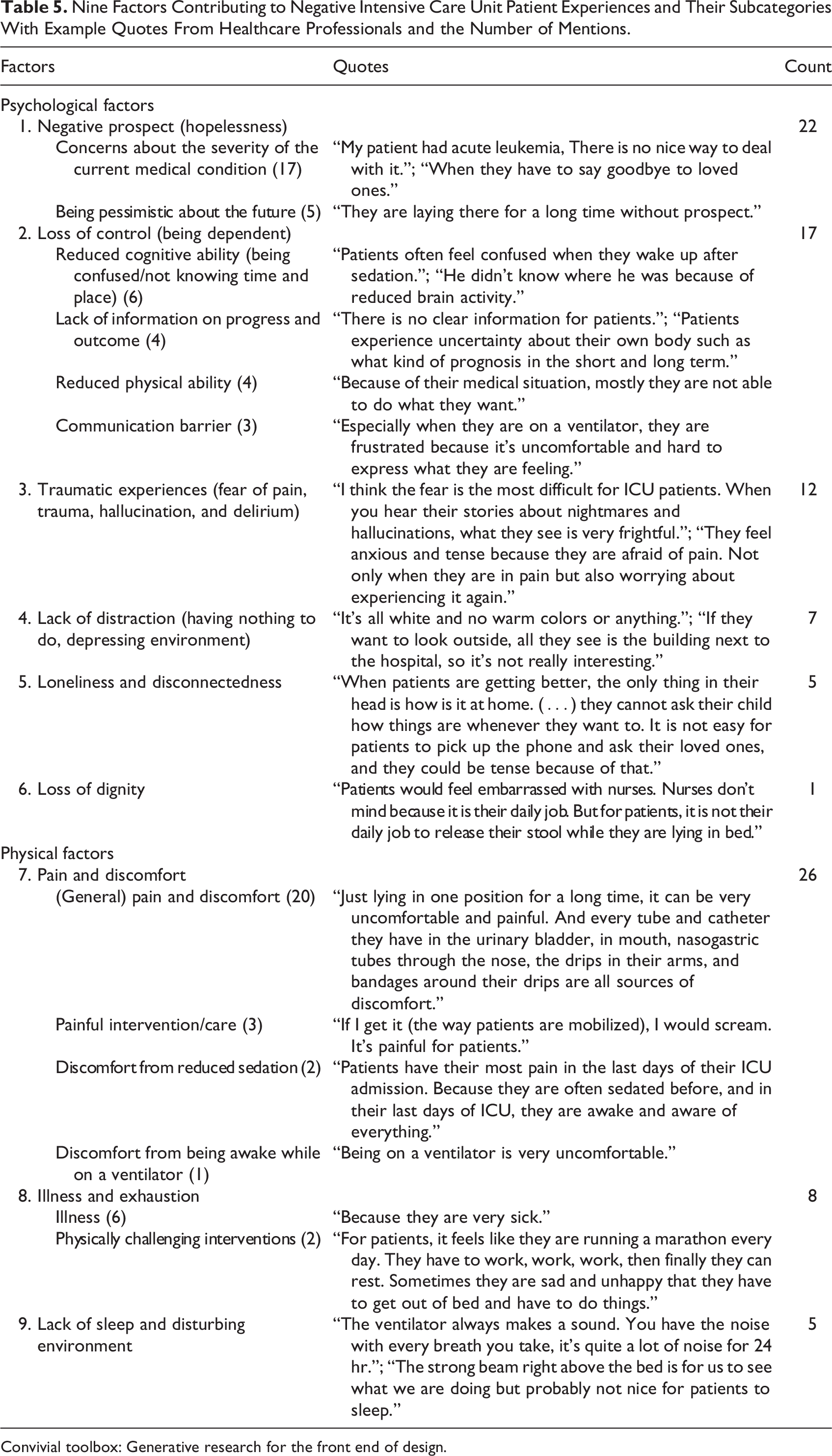
Convivial toolbox: Generative research for the front end of design.
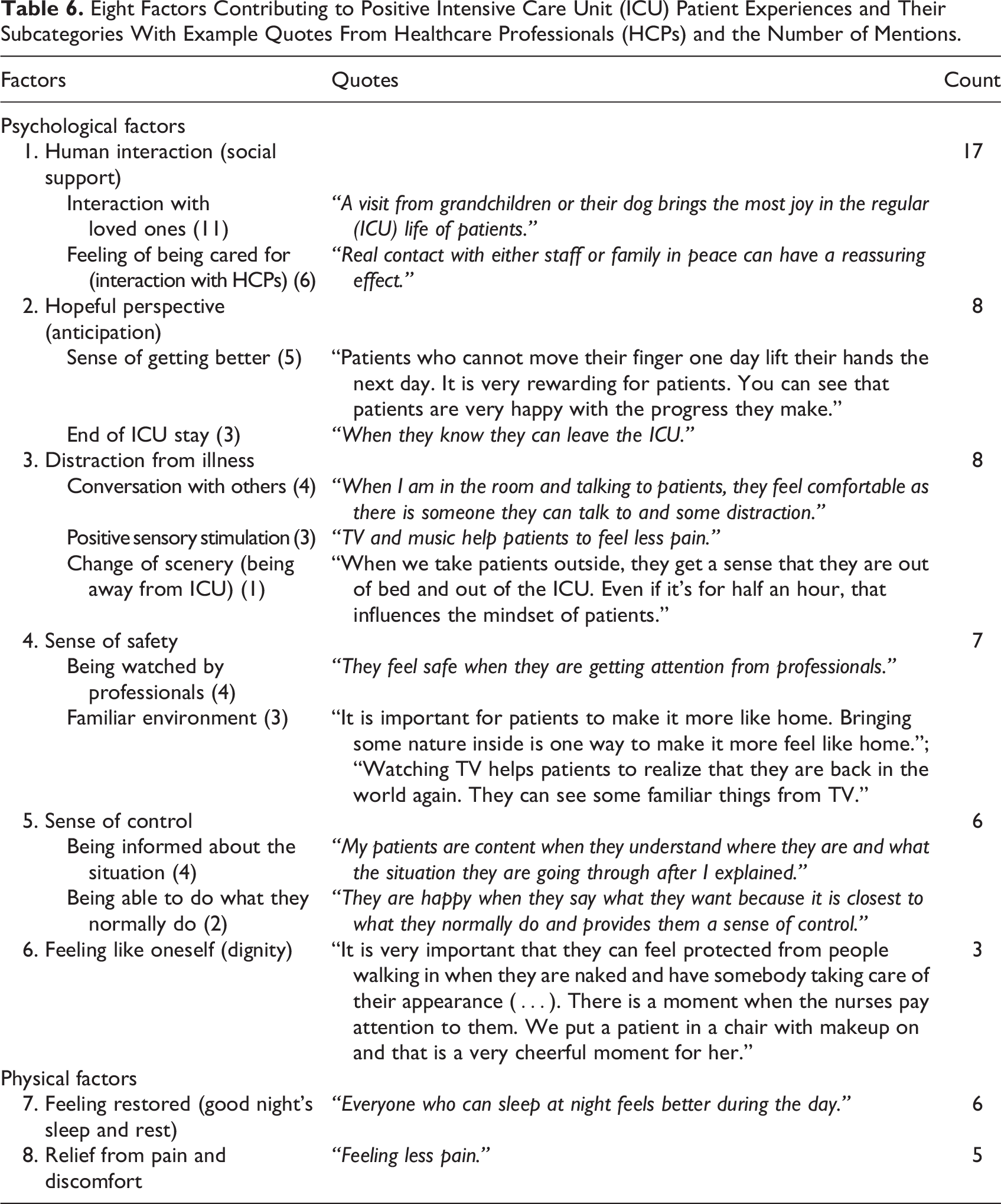
For the positive patient experience, eight themes were identified and divided into psychological and physical factor groups. Table 6 shows the overview of these themes, quotes from HCPs, and the number of times they are mentioned.
Eight Factors Contributing to Positive Intensive Care Unit (ICU) Patient Experiences and Their Subcategories With Example Quotes From Healthcare Professionals (HCPs) and the Number of Mentions.
Phase II: Creating a Healing ICU Environment Supporting Patient Well-Being
Method
Study Design, Participants, and Setting
A multistakeholder workshop was conducted to explore the potential of ICU environments in optimizing support for patient well-being and possible technology-based solutions. The workshop was built upon the results of the mixed-method study and was designed to include multistakeholders, which resulted in a collaborative workshop where different stakeholders came together to share their knowledge, expertise, and perspectives on a particular topic (Sanders & Stappers, 2012). This approach was adopted as the goal of this workshop is to generate innovative and feasible solutions through a structured process that leverages the diverse perspective and knowledge domains of the stakeholders.
A total of 11 participants were recruited to have a diverse group of participants. The group consisted of four ICU nurses from two Dutch hospitals (participating also in the study Phase 1), three academic researchers in healthcare design and psychology, and four industry experts in health technology specialized in the critical care domain.
Procedure
The co-creation workshop was designed following the double diamond model (Design Council, 2015). The workshop consisted of two sessions: consolidation and ideation. The entire workshop lasted 4.5 hr taking 2 hr for the first session and 2.5 hr for the second. Figure 2 illustrates the overall structure of the workshop next to its input and output.
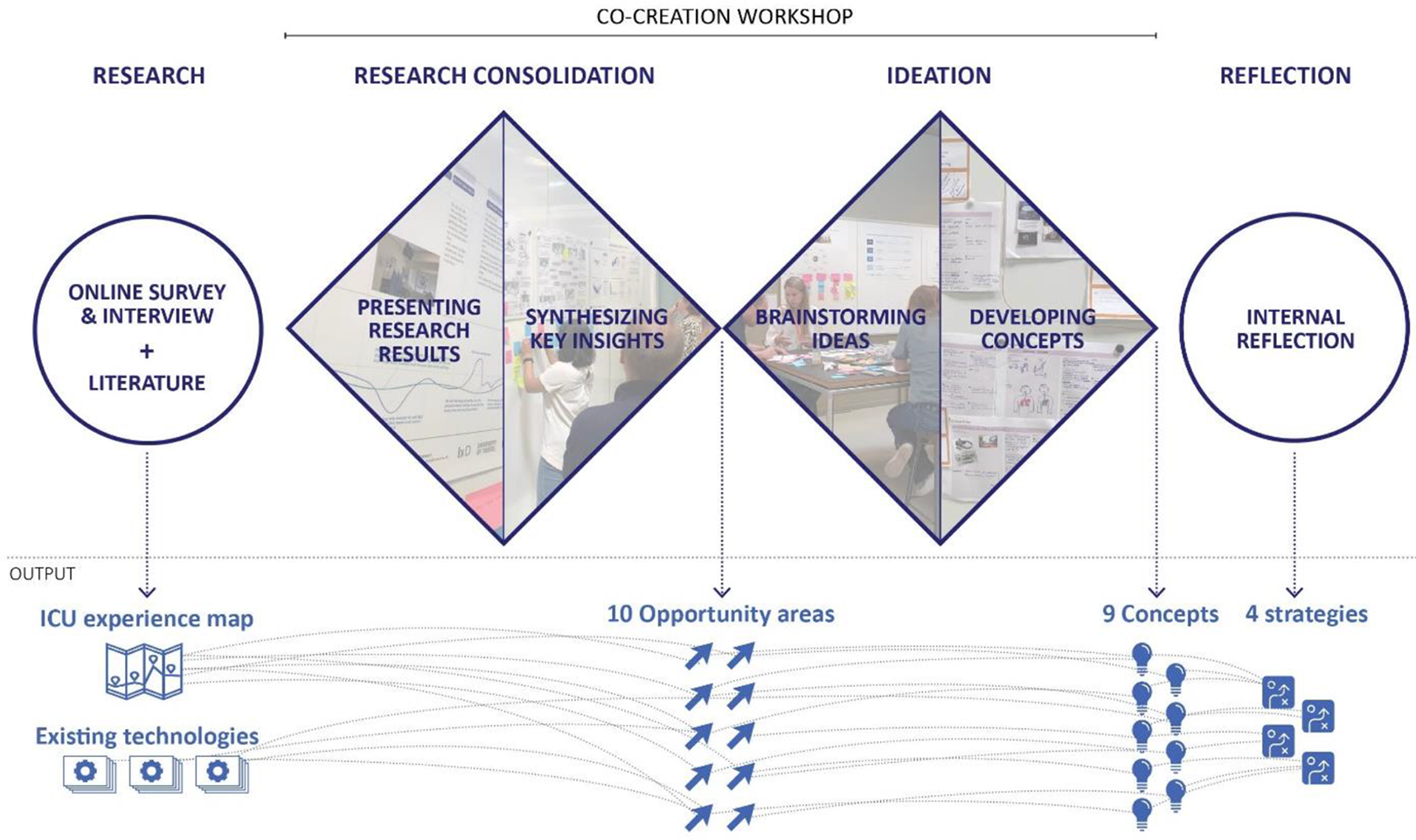
Overview of the workshop.
In the first phase of the workshop, the research consolidation session, a journey map and a visual summary of the online survey results (the content of Tables 5 and 6), and an overview of a literature review on technology-based interventions used in the ICU (Kim et al., 2021) were presented. During the presentation of the data, participants were encouraged to make notes on what they considered as key insights on post-its. Next, these collected key insights were synthesized and summarized as opportunity areas through group discussion. For the second phase of the workshop, the ideation session, participants worked in pairs and developed a vision statement (e.g., “I want the ICU to be….”) based on the opportunity areas and brainstormed about technological solutions. A set of inspirational images and drawing materials were provided with a template containing questions that could support detailing the ideas such as “What problem does it solve?” and “How does it work?” During the last 30 min, each duo presented the vision and ideas they created to the group for feedback.
Analysis
The workshop data, including opportunity areas that were identified and vision statements and initial concepts generated during brainstorming, were analyzed to extract actionable design criteria and opportunities. By integrating them, four strategies were developed by the first author and reviewed with the coauthors. We will further elaborate on these strategies in the Results section.
Results
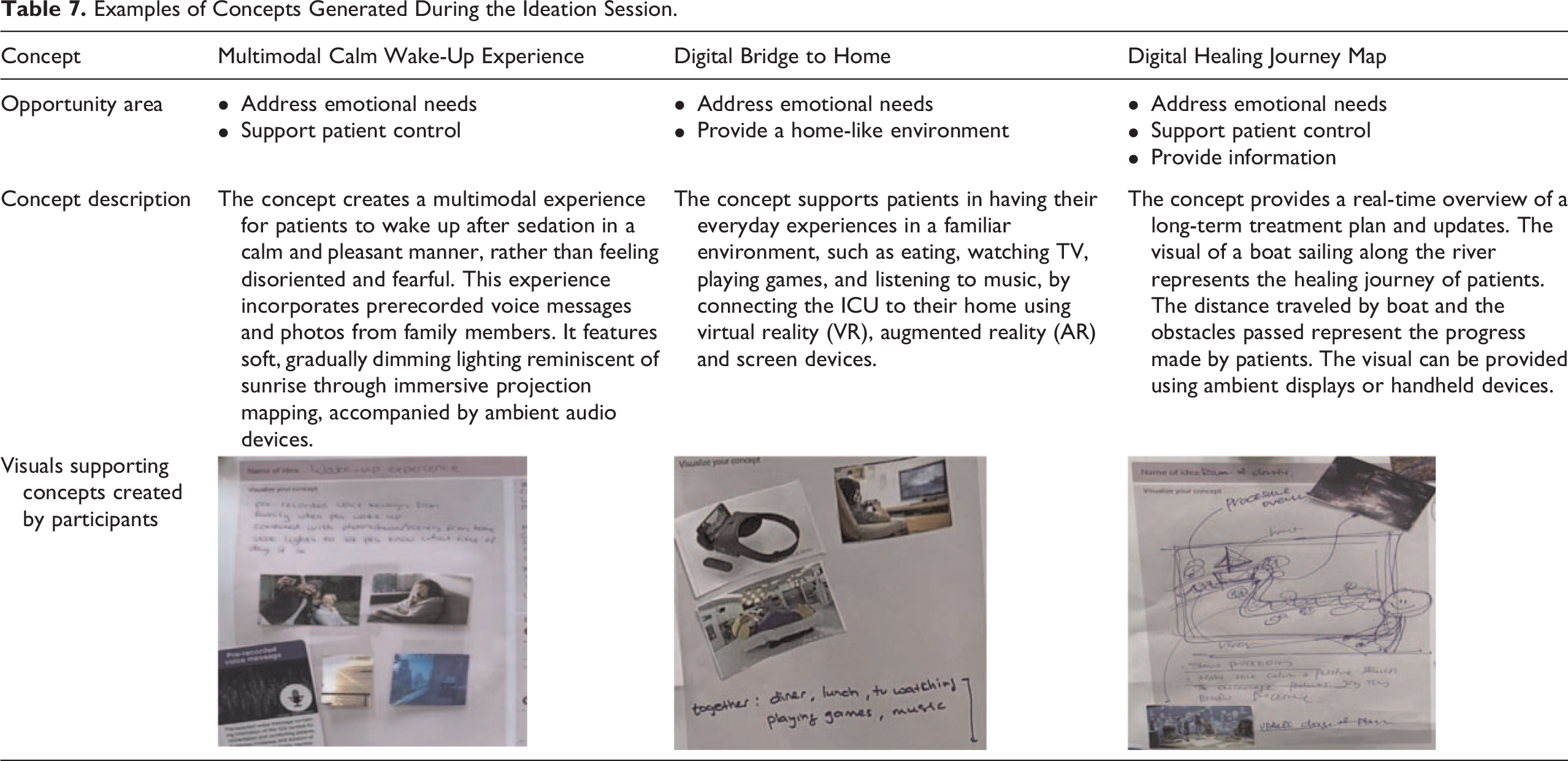
The consolidation session yielded 10 opportunity areas including address the emotional needs of patients, support patient control, and provide a home-like environment (see Table A1 in the appendix for all identified opportunity areas). The ideation session used these opportunity areas and participants generated a total of nine initial concepts which include a multimodal calm wake-up experience, a digital bridge to home, and a digital healing journey map (see Table 7 for a detailed description of these three examples, also see Table A2 in the appendix for all nine concepts). All concepts were presented in the group and their benefits, challenges, and execution plan were discussed. These concepts were presented on a large board which allows an overview and easy comparison between concepts for participants.
Examples of Concepts Generated During the Ideation Session.
Four Strategies to Create Technology-Enabled Healing ICU Environment
The concepts developed by participants provide concrete examples of how technologies could support creating healing ICU environments. Our aim is, for these findings, to enable other designers and HCPs to create solutions that are customized to their unique ICU contexts. To achieve this, we looked into the values underlying each concept and synthesized them into strategies that comprehensively address patient experience factors (see Table 8).
Four Strategies to Create Technology-Enabled Healing Environments With Their Associated Factors and Design Concepts.
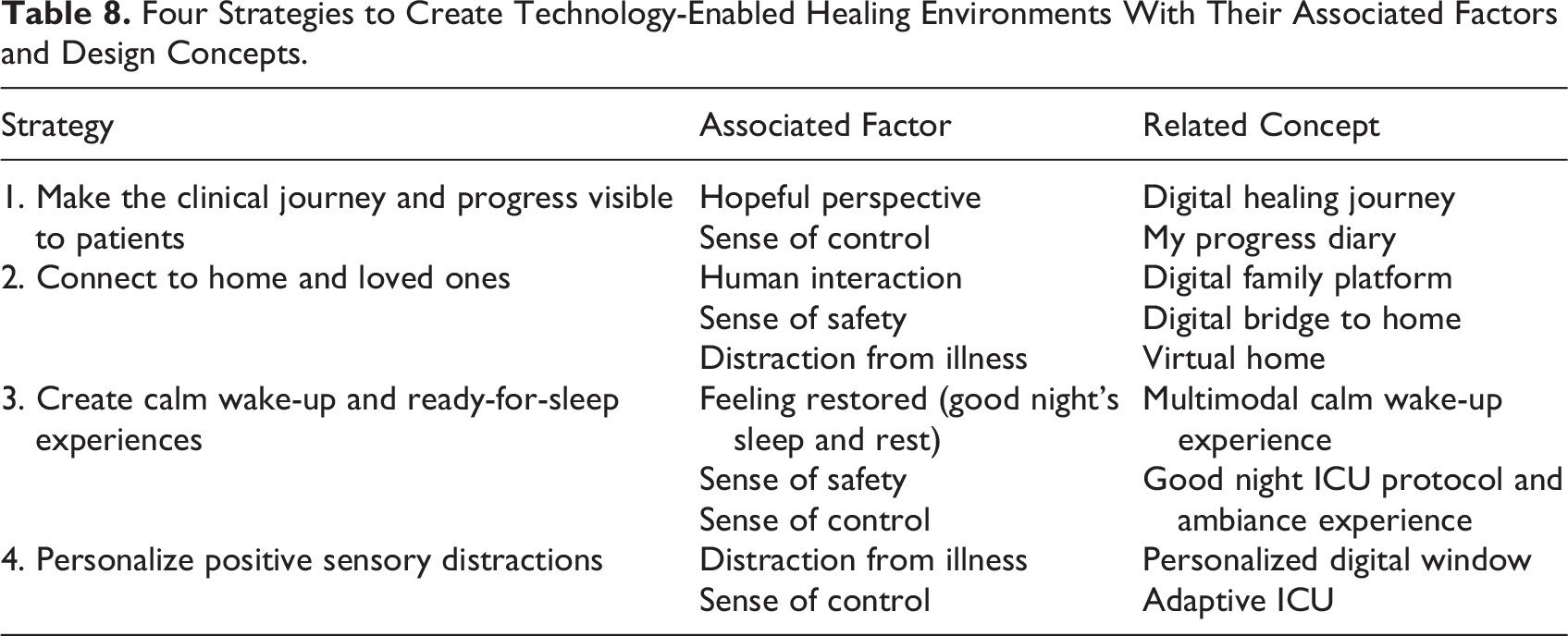
Strategy 1. Make the clinical journey and progress visible to patients: The ICU environment can promote a sense of control and a hopeful perspective among ICU patients by providing an overview of the medical journey which gives patients an idea of what they went through and what to expect for the coming period. To encourage patients, the small progress that patients make should be emphasized in an overview. It could positively influence the mindset of patients and support them in building anticipation toward recovery in the ICU context, where the path to discharge often appears distant and pessimism can easily set in.
Strategy 2. Connect to home and loved ones: Interactions with loved ones promote a sense of safety, human interaction, and distraction from illness for patients. Family visits, for instance, are among the most positive activities in the ICUs that alleviate the loneliness and boredom of patients while providing reassurance. To optimize the benefits of interactions with loved ones, an ICU environment should support pleasant family visits by providing relaxing surroundings and also by supporting pleasant and continuous interactions between patients and loved ones outside of family visit time.
Strategy 3. Create calm wake-up and ready-for-sleep experiences: When waking up from sedation, ICU patients often suffer from feelings of being lost, fear, and anxiety due to an unfamiliar environment. The hostile ICU environment also disturbs patient sleep. The ICU environment can promote the restoration of patients (good night’s sleep and rest) by creating an ambiance that accommodates timely needs and gives patients a sense of familiarity and reassurance.
Strategy 4. Personalize positive sensory distractions: ICU patients need positive sensory stimulations that can distract them from pain and negative thoughts. Using ambient technology including ambient light, display, and sound, the ICU environment can provide a wide range of positive stimulations that cater to the different emotional needs of patients. For instance, to create distractions by positive stimuli, the level of stimuli can be adjusted depending on the perceived pain and discomfort level of patients. To address dynamic negative emotional experiences that ICU patients go through, such as loneliness, sadness, fear, and anxiety, different types of positive stimulation could be provided. For instance, to alleviate fear and anxiety, calming and reassuring stimuli can be utilized, while uplifting stimuli can help alleviate sadness.
Discussion and Conclusion
In this study, we explored the role of the ICU environment in promoting patient well-being from the perspective of HCPs and envisioned how technology could support creating healing ICU environments. The mixed-method study (Phase I) yielded insights into the ICU patient experience including positive and negative contributing factors as well as current limitations and challenges. The co-creation workshop (Phase II) resulted in identifying key areas of improvement and developing concepts that support creating an ideal environment for patients. Drawing from these insights, we formulated four strategies that harness the potential of technology in enhancing ICU patients’ well-being.
An interesting finding from the first phase of the study was that most negative factors stem from being in the ICU environment (e.g., loss of control, lack of distraction, loneliness, and disconnection) than patients’ illness itself (e.g., pain, discomfort, and negative perspective). These negative factors mentioned by HCPs are aligned with the findings from studies conducted with ICU patients (Abuatiq, 2015; Halvorsen et al., 2022; Krampe et al., 2021; Rose et al., 2014) which include loss of control, loneliness, (dull) design of the room, as well as pain and functional distress. We also found that most of these factors are intertwined and can create chain effects; not addressing one negative factor can activate another negative factor. Taking an example, the lack of distraction can increase subjective pain which disturbs sleep and lead to worsening health outcomes and recovery. Therefore, instead of addressing individual factors in isolation, adopting a more holistic approach that encompasses most negative factors would be more effective. Previous studies (Halvorsel et al., 2020; Kim et al., 2021) also support the importance of addressing multidimensional needs in the ICU to promote patient well-being. Our findings on positive factors inform how patient needs are currently met in the ICU environments from the perspective of HCPs. Most of these factors correspond with findings from other studies conducted with ICU patients (Aro et al., 2012; Halvorsen et al., 2022; Van Keer et al., 2017) including social support, sense of safety, sense of control, distraction from illness, as well as relief from pain and discomfort. Importantly, we found that most positive factors are currently reliant on HCPs who cannot act on these needs due to the high workload in the current ICUs. Studies (Carayon & Alvarado, 2007; Hugonnet et al., 2007) pointed out the workload of HCP as a key challenge in the ICU, which leads to “invisible tasks,” such as emotional care, being left unattended (Halvorsen et al., 2022; Kitson, 2018). This problem resonates with our findings: Patient emotional care is currently the most challenging aspect in the ICU for HCPs. We found that despite the effect of positive environmental factors on patient well-being, their implementation is limited or absent. This limitation might be due to physical constraints, such as the location or architectural structure of the hospital building, which do not allow access to nature views or systemic constraints, for instance, not considering positive elements in the hospital interior design process.
The results of the second part of the study provided rich insights into how technology can act upon the current limitations of ICU environments. The four strategies we introduced based on the results from an extensive stakeholder workshop are in line with nonpharmacological interventions that are currently practiced in the ICU. These include, for example, the provision of sufficient information, family involvement, and personalized care from the ICU ABCDEF bundle (Marra et al., 2017) and the hospital elder life program (HELP; Zachary et al., 2020). Along with the strategies, our concepts showed how to extend the implementation of these strategies by adopting technologies. Most technologies are informed by existing technology-based interventions that are also evidence-based. For instance, personalized audio stimuli (Cheong et al., 2016) and the provision of visualized information about medical procedures (Ryu et al., 2019) proved to reduce anxiety among ICU patients.
Our study results contribute to the knowledge of the current positive and negative factors of ICU patient well-being from the perspective of HCPs. We showcased how technology could enable holistic and personalized care in the ICU environment with a variety of concepts and four strategies. We expect our findings to inform designers and developers of healthcare technologies and HCPs in creating customized interventions adapted to their ICU contexts.
Limitations and Future Directions
Our study provided valuable insights from the perspective of HCPs. This study was conducted with ICUs located in the Netherlands. Considering the differences in ICUs with other countries that might affect the perceived experiences of patients, the findings may not be readily transferrable to ICUs in other countries. While most of our insights are supported by other study findings conducted with patients, the development of concepts and strategies for enhancing patient well-being was derived from the ideas of HCPs. Furthermore, the current sample size (n = 27) has offered valuable insights. However, due to our approach (i.e., distributing an online survey using an anonymous link), we cannot rule out a sampling bias in the absence of a precise response rate. That is, participation in our study might reflect interest in the topic of our research. Hence, to validate and extend these findings, follow-up studies with a larger sample size and an appropriate response rate are warranted. To fully explore and validate the identified opportunities for enhancing the ICU environment, further validation with ICU survivors is required. The scope of our study is enhancing ICU patient well-being on an experiential level. Hence, the four strategies we developed do not address problems on an organizational or systemic level. However, considering that the successful implementation of technology-based solutions goes hand in hand with systemic changes, such as changes in procedures and physical aspects of interior design, future studies will need to include multiple perspectives from diverse stakeholders, including ICU patients. We encourage future studies to extend and detail our strategies by involving a wide range of stakeholders.
Implications for Practice
Overall, this study presents how digital technology can extend the potential of the ICU environment in supporting patient well-being from the perspective of HCPs.
The first part of the study outlines both positive and negative factors influencing patient experiences in the ICUs and the challenges experienced by HCPs during care activities, which highlights key areas for digital technology to address in order to enhance ICU patient well-being.
The second part of the study proposes four strategies that provide guidance on how to adopt technology in the ICU environment to offer holistic and optional care: providing clear information for patients and family, establishing connections to home and loved ones, creating an ambiance conducive to effective rest, and offering personalized distractions.
Footnotes
Appendix
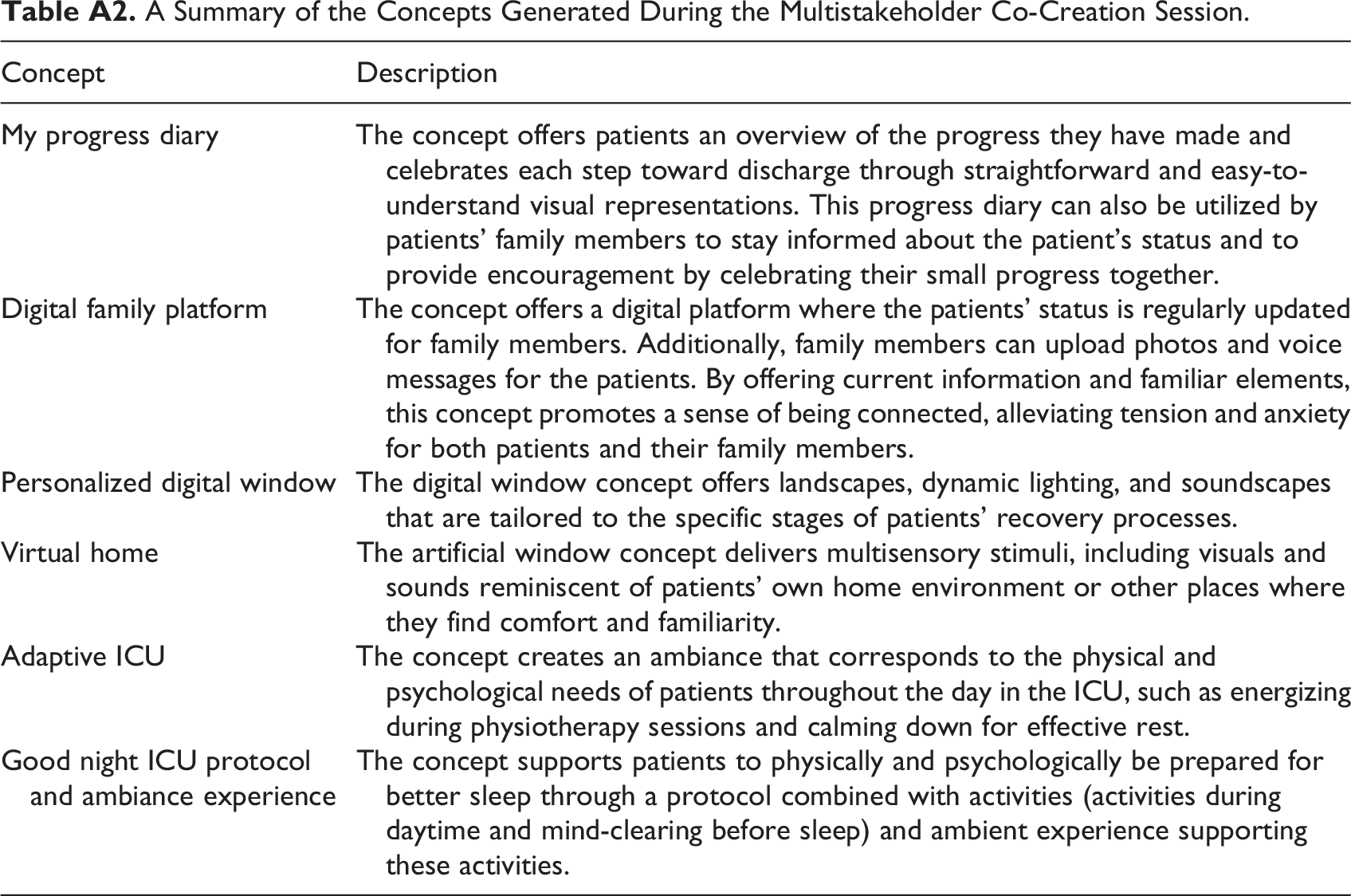
A Summary of the Concepts Generated During the Multistakeholder Co-Creation Session.
| Concept | Description |
|---|---|
| My progress diary | The concept offers patients an overview of the progress they have made and celebrates each step toward discharge through straightforward and easy-to-understand visual representations. This progress diary can also be utilized by patients’ family members to stay informed about the patient’s status and to provide encouragement by celebrating their small progress together. |
| Digital family platform | The concept offers a digital platform where the patients’ status is regularly updated for family members. Additionally, family members can upload photos and voice messages for the patients. By offering current information and familiar elements, this concept promotes a sense of being connected, alleviating tension and anxiety for both patients and their family members. |
| Personalized digital window | The digital window concept offers landscapes, dynamic lighting, and soundscapes that are tailored to the specific stages of patients’ recovery processes. |
| Virtual home | The artificial window concept delivers multisensory stimuli, including visuals and sounds reminiscent of patients’ own home environment or other places where they find comfort and familiarity. |
| Adaptive ICU | The concept creates an ambiance that corresponds to the physical and psychological needs of patients throughout the day in the ICU, such as energizing during physiotherapy sessions and calming down for effective rest. |
| Good night ICU protocol and ambiance experience | The concept supports patients to physically and psychologically be prepared for better sleep through a protocol combined with activities (activities during daytime and mind-clearing before sleep) and ambient experience supporting these activities. |
Acknowledgments
We would like to thank Prof. Dr. Bart Verkerke (University of Twente), Thomas Falck, MSc (Philips Research), for their guidance throughout this study, Dr. Huub van der Oever (Deventer Hospital), Paul van Berkom (St. Elisabeth Hospital), and Gijs Louwers (Delft University of Technology) for their support in the setup and execution of the ICU study. We also thank all participants of our study for their valuable input. Lastly, we thank the anonymous peer reviewers for constructive comments.
Declaration of Conflicting Interests
The author(s) declared the following conflicts of interest with respect to the research, authorship, and/or publication of this article: Chan Mi Kim is employed by the University of Twente through Top Technology Twente Connecting Industry program (TKI Topsector HTSM) fund. Esther van de Heide is employed by Philips. The remaining authors do not have a conflict of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the Digital Nature project that received funding from the Top Technology Twente Connecting Industry program (TKI Topsector HTSM), which is partially funded (paid to institution) by Philips.