
Abstract
Objectives, Purposes, and Aims:
Principles of behavioral economics are now being used across fields in changing human behavior toward perceived benefit. We studied the effectiveness of simple, cost-effective design cues based on these principles, in encouraging use of a neglected outdoor space in a hospital.
Background:
Benefits of access to nature and green spaces are established in healthcare; however, we found utilization of an outdoor space to be suboptimal. Presenting choices in different ways is known to influence user choice.
Methods:
We designed four design interventions based to nudge relative-caregivers waiting outside the operation theater toward utilizing an adjoining outdoor balcony. These included making the terrace prominent, reducing indoor sensory stimulation, adding stereotypical elements, and improving usability. We measured usage via video camera data and satisfaction using questionnaires.
Results:
The number of users and average time per person spent on the balcony increased over the consecutive intervention periods as compared to baseline (trend p < .01 for both), mainly driven by the addition of stereotypical elements. There were no adverse events in the balcony. There was no difference in the satisfaction related outcomes on questionnaire; a larger percentage of positive comments tended to be related to the balcony in the final intervention.
Conclusions:
Cost-effective design cues nudged patient-caregivers toward spending more time with nature, thus changing behavior toward that with perceived benefits.
Introduction
Recent behavioral insights, chiefly from the field of economics, show a gap between how people behave spontaneously in stressful settings versus when they deliberate. These deviations from expected behaviors are not random and are in fact systematic (Rice, 2013). Data from the field show that it is incorrect to assume that all decisions, including in the healthcare setting, are always optimal (Muhlbacher & Johnson, 2016). The principles of behavioral economics provide a framework to change human behavior for their benefit. Thaler and Sunstein popularized the use of interventions that harnessed cognitive biases to steer people’s decisions, called “nudges.” Nudges were defined as “interventions in the choice architecture that alter behavior in a predictable way without forbidding options or significantly changing economic incentives” (Thaler & Sunstein, 2008). Subsequent work has shown simple steps can “nudge” people in making the optimal or healthy choice and have since been widely used by policymakers for both economic and healthcare decisions.
Framing is a concept that helps understand how people choose and act in these environments and could be used to predict user behavior (Kahneman, 2011). A common example of framing is to suppose a patient is considering an optional surgical procedure and asks their doctor for some information about it. The doctor may say either of the following: (1) 90% of patient surgeries are easy, and (2) 10% of patient surgeries have a complication. In the first response, patients will want to go ahead with the surgery but will hesitate or opt out altogether in the second response. This is despite the two statements meaning the same risk, where the difference lies in the first communicating “easy” and the second communicating “complication”—two ways of saying the same thing. In the broader context, we took framing to mean the manner of presentation of a choice to an agent. Presenting information in different ways can influence user choice for and against an action (Kahneman, 2011). We interpreted framing in a more broadly encompassing manner to suggest a method of presenting a choice.
These concepts also lend themselves to the field of design and architecture, termed “choice-based design” or “choice architecture” (Parikh & Parikh, 2017). Framing is experienced by a user as a trigger, and insightful design cues can prompt people into action. Since the behavior is spontaneous it means a person must experience the design as a positive effect (or a negative one) which is why they choose to act. The design cues should be easy, attractive, effective, and rewarding to motivate people’s interest, yet not obvious.
Healthcare institutions in India, like most public bodies, administer numerous rules, safety restrictions, and government regulations. The long history and tradition of these rules impact hospital environments in their usage, social norms, and influence people’s behaviors into status-quo thinking. With this study, we endeavored to examine the use of nudges to promote the well-being of patients’ family members waiting for patients in surgery outside the operation theater (OT). Patients’ friends and family act as informal caregivers and typically contribute to holistic care of patients (Shaji & Reddy, 2012). In India, family structures mandate the patient being accompanied by many people and taking part in the caregiving process along with doctors, nurses, and other healthcare professionals. We refer to these family members as family-caregiver. Family caregivers in hospitals spend long hours in crowded and institutionalized waiting rooms, increasing mental stress (Hogan et al., 2022). Family caregivers are stakeholders in treatment decisions including financial and the choice of healthcare facilities; thus, their opinion of the hospital experience matters in overall satisfaction, independent of the medical outcomes in the patient (Miller et al., 2016).
Many studies have demonstrated the benefits of easy access to nature in healthcare settings (Weerasuriya et al., 2019). Indoor greenery and easy access to outdoor spaces improve a variety of health outcomes in users—inpatients, outpatients, and healthcare workers—as compared to spaces where no green is utilized (Ulrich et al., 2008; Whitburn et al., 2019). This evidence has led to many ways of thinking about using greenery in hospitals and healthcare settings. Despite the robust evidence, we noticed that a green space in our hospital was not utilized. Could we nudge potential users toward using this space using behavioral principles?
The scope of the project included adding cost-effective interventions to a balcony that adjoins the OT waiting room. We sought to test the hypothesis that different strategies of presenting the decision would encourage waiting family caregivers to access the outdoor space, ultimately bolstering caregiver participation in maintaining an overall therapeutic environment. We studied the effect of different interventions carried out in a sequential manner in nudging family-caregivers toward using the balcony, in turn lowering stress and improving satisfaction in their waiting experience in the hospital setting.
Method
Setting
The King Edward Memorial Hospital, Pune, India, was established in 1912 and is now a large, tertiary care hospital with more than 600 inpatient beds. Run by a registered charitable trust, the hospital predominantly caters to the lower-middle socioeconomic strata from Pune and the surrounding rural areas. Over the last century, the hospital structure has grown organically with a series of buildings built at various time points.
The area of the hospital selected in this experiment is housed in the Terres des Hommes building, built in 1979, which houses intensive care units (ICUs), OTs, and radiological diagnostic services. The area is a rectangular indoor waiting area outside the doors of the main OT, 35 by 19.5 feet. The area also receives two elevators for patients and other users, one staircase landing, and a small kiosk manned by one server for light snacks and beverages (Figure 1).
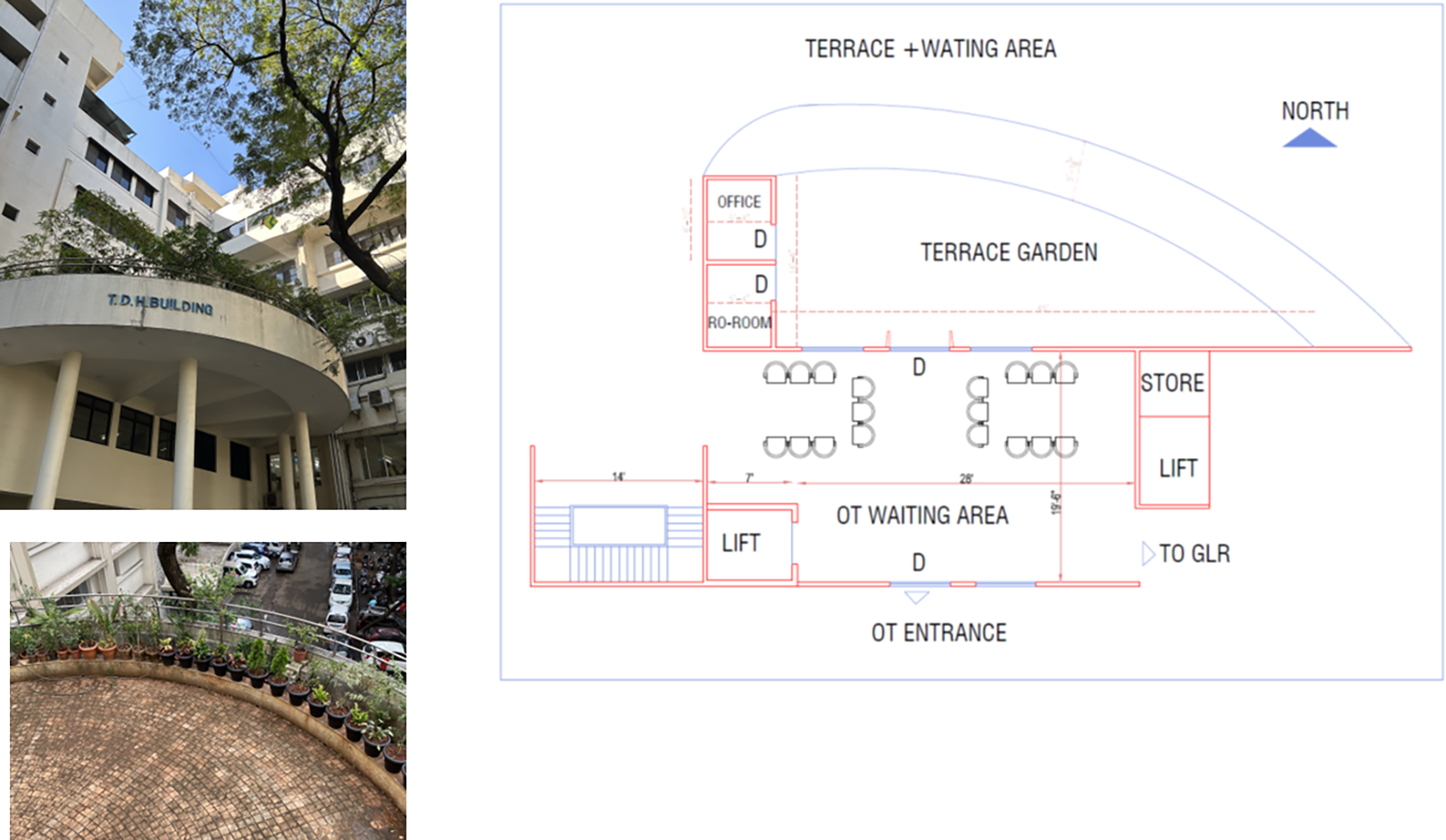
Photographs of study setting. (A) View of the semicircular balcony from below and an aerial view prior to the start of the interventions. (B) Plan of the waiting area outside the operation theater complex and the balcony.
The indoor waiting area is abutted on the north by a semicircular balcony, open to the sky but covered by a canopy of large trees three floors above it. One single glass door and three windows open out connecting the indoor waiting space from the balcony.
Study Design
The study evaluated the effects of four sequential low-cost interventions in a behavioral framework on the amount of time spent by users on the balcony. Variables of interest were calculated from video camera data. The interventions were each performed in a 2-week period from February to May 2022 and are described as follows: Week 1–2: No intervention
No specific intervention was performed in the initial 2 weeks to establish a baseline. Nothing was done to actively open the door or windows to the balcony and practices continued as before; the waiting chairs faced the OT. Usage and questionnaire data were gathered. Week 3–4: Make the balcony prominent
Seating was oriented to be perpendicular to the windows, with a clearly demarcated area in between, so that users would either face each other and would have access to open windows on one side that looked out onto the balcony. The space immediately inside the balcony door was kept free of obstacles, and the door was deliberately kept open.
Behavioral principle: A simple reorientation of the indoor waiting room to the outside aimed to evoke an outdoor significance and bring the balcony in a clear field of vision. The reorientation of caregivers also meant the OT and clinical spaces were not in direct sight during waiting. Week 5–6: Reduce indoor sensory stimulation
The floor was marked with green colored cues to clearly demarcate the pathway leading to the outdoor space. Indoor plants were kept around the indoor waiting area. Picture frames with botanical prints or green landscapes were installed on the walls.
Behavioral principle: Directional floor patterns, indoor plants, green colored art, and nature prints in the indoor space aimed at framing the indoor space as an intuitive extension of the outdoor balcony, aimed to subconsciously make the transition to connect with nature and greenery easier. In addition, indoor greenery and art would reduce the generally unpleasant “clinical” sensory stimulation in the hospital environment to those waiting. Week 7–8: Stereotypical elements in the outdoor balcony
Larger plants were added on the balcony, framing an attractive garden effect. Chairs were placed in the area in groups as to aid conversation while facing the greenery. Large umbrellas were kept to provide shade and protection from sunlight and rain. All previous changes made in the indoor environment were left unchanged.
Behavioral principle: Stereotypical elements generate memories in people. We hoped that large plants and umbrellas in the balcony would make people reminisce about pleasant experiences in home gardens and parks, providing mental respite in the immediate hospital environment. This was the first time an intervention was carried out in the actual area of study. These elements would invite users to recall moments of natural life and sounds in a home garden or park, reducing stress by the brief distancing from illness. The plants were arranged in an informal, grouped way rather than with geometric, formal landscaping to evoke memories of home gardens or backyards in this geographic area. To the same end, local plants were used, and not exotic varieties. Week 9–10: Improve usability
An awning was installed in the balcony which was partly fixed and partly retractable. Along with chairs, hand sanitizer stands, waste disposal bins, and pedestal fans were added to the space.
Behavioral principle: In addition to the stereotypical elements, these interventions aimed at demonstrating usability of the outdoor space. The awning would add a sense of permanency and show the space could be used across seasons; the other elements would invite users to linger, encourage germ control use and keeping cleanliness, add ventilation and comfort, and the bins would allow for use of the space to consume snacks.
Outcomes
These design interventions were used to study (a) if usage of the balcony increases with a design option and (b) if caregivers who stayed or interacted longer with nature, greenery and sounds in the balcony felt they had an improved waiting experience.
Primary outcomes: Usage of space
Usage of space was measured using video security camera footage. The video cameras were attached in both the OT indoor waiting space as well as the OT balcony area with a resolution adequate to record movement of people without being able to identify the face. A single human observer entered the time of entry and exit for each individual. The difference between these was counted as time spent on the balcony. If one participant entered the balcony multiple times, times spent were summated. Variables of interest included the following: (1) the number of people using the outdoor area per day; (2) cumulative time spent in the outdoor area per day, in minutes, calculated as an addition of time spent for all individuals; (3) average time spent per person per day in minutes; and (4) maximum time spent by one person in a day in minutes. In addition, adverse outcomes were also recorded via camera footage, which were defined as activities deemed unsafe, such as climbing balcony railings, falls, or accidents.
Secondary outcomes
We distributed feedback questionnaires to relatives and attendants of patients undergoing surgery in the major OT complex, assuming these to have been users of the balcony space. These questionnaires were distributed and collected on the first postoperative day and not while they waited in the area, therefore avoiding possible confounding by attention drawn by the questionnaire itself. For participants who were unable to understand the questions or the language, the person administering it offered to translate, explain, or write answers. Anonymity was explained and participants’ names were not recorded on the answers. The questionnaire was self-authored and has not been psychometrically tested. It contained directed questions about users’ experience while waiting outside the OT on a Likert-type scale (1–4), with a higher score denoting a more positive experience. We preferred a 4-point Likert-type scale to avoid safe answering with the middle value. Out of the eight questions (shown in Table 2), six pertained to the experience pertaining to the space (Q3: outdoor view; Q4: direction of seating; Q5: appearance and cleanliness of waiting area; Q6: floor patterns for wayfinding; Q7: plants providing relief; 8: welcoming nature of the waiting room). Two questions were added as “control” questions (Q1: duration of waiting time; Q2: communication about the waiting process). In addition, the questionnaire provided free space for participants to answer what they felt was positive about their waiting experience. These answers were later classified into themes (balcony/outdoor space, refreshments, staff, medical care, cleanliness).
Analysis
We calculated sample size considering a 25% rise in use of the outdoor area to be significant as compared to the baseline period of observation. Using the Lehr equation (n = 16/Δ2), a sample size of 55 in each period would achieve 80% power and 95% confidence intervals (Lehr, 1992). The KEM OT complex typically conducted 15–20 surgeries per day on each working day, and therefore we expected at least 40 users of the outdoor space per day. To be able to find additional smaller differences between two intervention groups, we considered a pragmatic time duration of 2 weeks.
The primary video outcome variables were calculated daily for each 2-week period. The four outcomes were compared with that in the first 2 weeks (no intervention period, statistical significance denoted as p1 in Table 1) as well as the period directly preceding it (statistical significance denoted as p2 in Table 1), using independent sample t tests. In addition, an analysis of variance was performed for significance of overall trend over the five consecutive interventions (denoted as p3).
Video Camera–Based Usage of the Balcony Outside the Operation Theater.
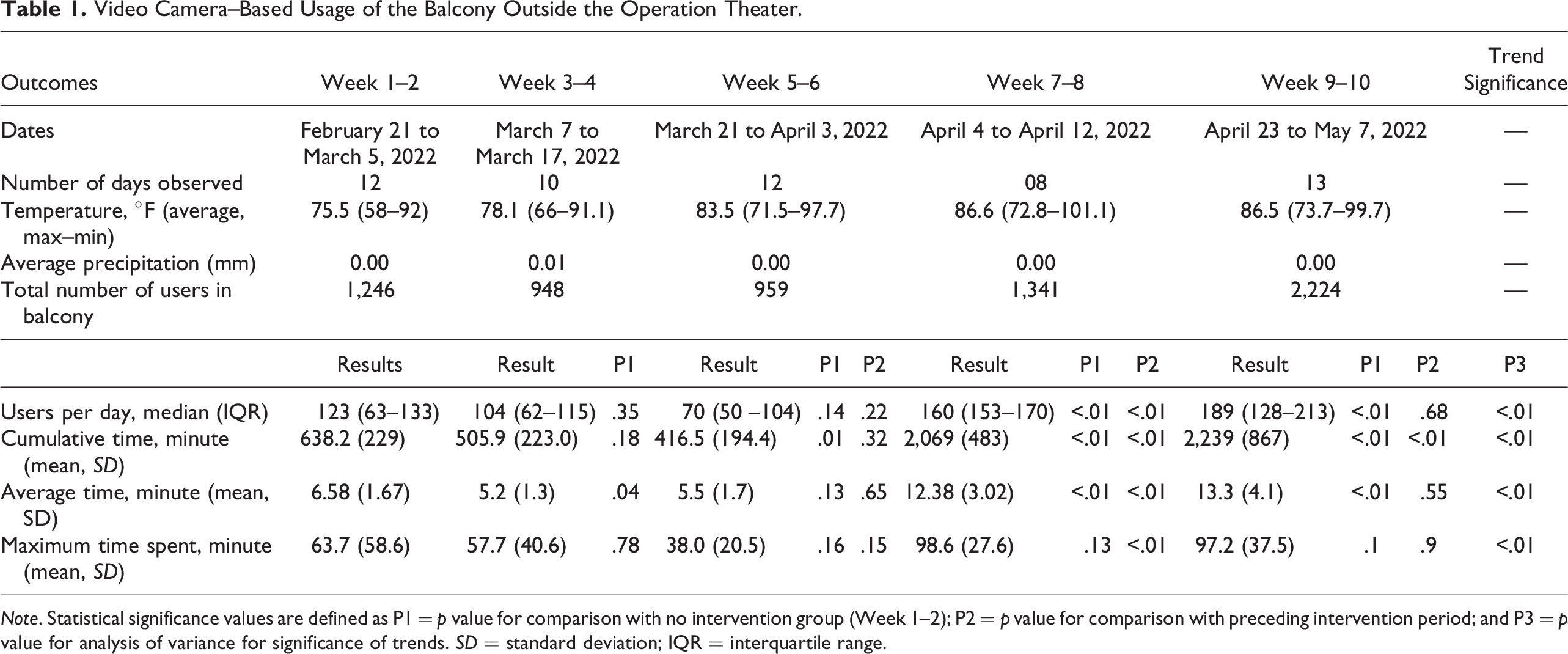
Note. Statistical significance values are defined as P1 = p value for comparison with no intervention group (Week 1–2); P2 = p value for comparison with preceding intervention period; and P3 = p value for analysis of variance for significance of trends. SD = standard deviation; IQR = interquartile range.
For questionnaire-based outcomes, median answers on the Likert-type scale (1–4) were compared for each question between all four intervention periods and Week 1–2 (no intervention, denoted as p1) and with the preceding intervention period (denoted as p2, Table 2) using the Wilcoxon signed–rank test. In addition, differences were also calculated for the proportion of responses being the highest (4) and the proportion of positive comments pertaining to the balcony in each intervention period compared to Week 1–2, using the χ2 test. Statistical analysis was performed using GraphPad Prism (Version 9.3.1 for Windows; GraphPad Software, San Diego, CA).
Ethics and protection of human subjects
This study received prior ethics committee clearance from the KEM Hospital Research Centre Ethics Committee (KEMHRCEC, 2136). Confidentiality was maintained by ensuring the video camera footage stored was of a resolution that could not identify individuals by face. The data were entered by a single person (S.S.) who was not connected to the treating teams nor the hospital administration. Preexisting video cameras were used, and the balcony had signs warning that people were under video camera surveillance. The committee waived the need for individual informed consent, especially since it was believed that behavior may change. Participants answered the questionnaires anonymously; names or other identifying details were not recorded. Both video camera and questionnaire data are securely stored at the KEM Hospital Research Centre.
Results
The study was conducted from the months of February to May 2022 (Table 1). The initial period of observation without intervention started on February 21. This comprised the beginning of the summer season in Pune, and average temperatures were in the late seventies (degrees Fahrenheit), gradually increasing toward the end of the study; there was minimal precipitation throughout the period of observation. The number of surgeries per day remained constant throughout the intervention periods.
Primary Outcomes: Balcony Usage–Based on Video Cameras
We found that the number of users per day of the balcony increased significantly over the consecutive intervention periods, from about 120 per day to 190 per day in the final 2 weeks (p for trend < .01) (Table 1, Figure 2). While it remained similar in the first two intervention periods, there was a significant increase in the third (p < .01 compared to earlier intervention and baseline). Apart from the number, the time spent in the balcony by each user nearly doubled, from an average of 7 min in Week 1–2 to 13 min in Week 9–10 (p for trend <.01). Like with the number of users, this increase was driven by the intervention in the third period (Week 7–8, adding stereotypical elements) (Figure 3). There was no difference in the median number of surgeries per day nor the average day time temperatures in these periods.
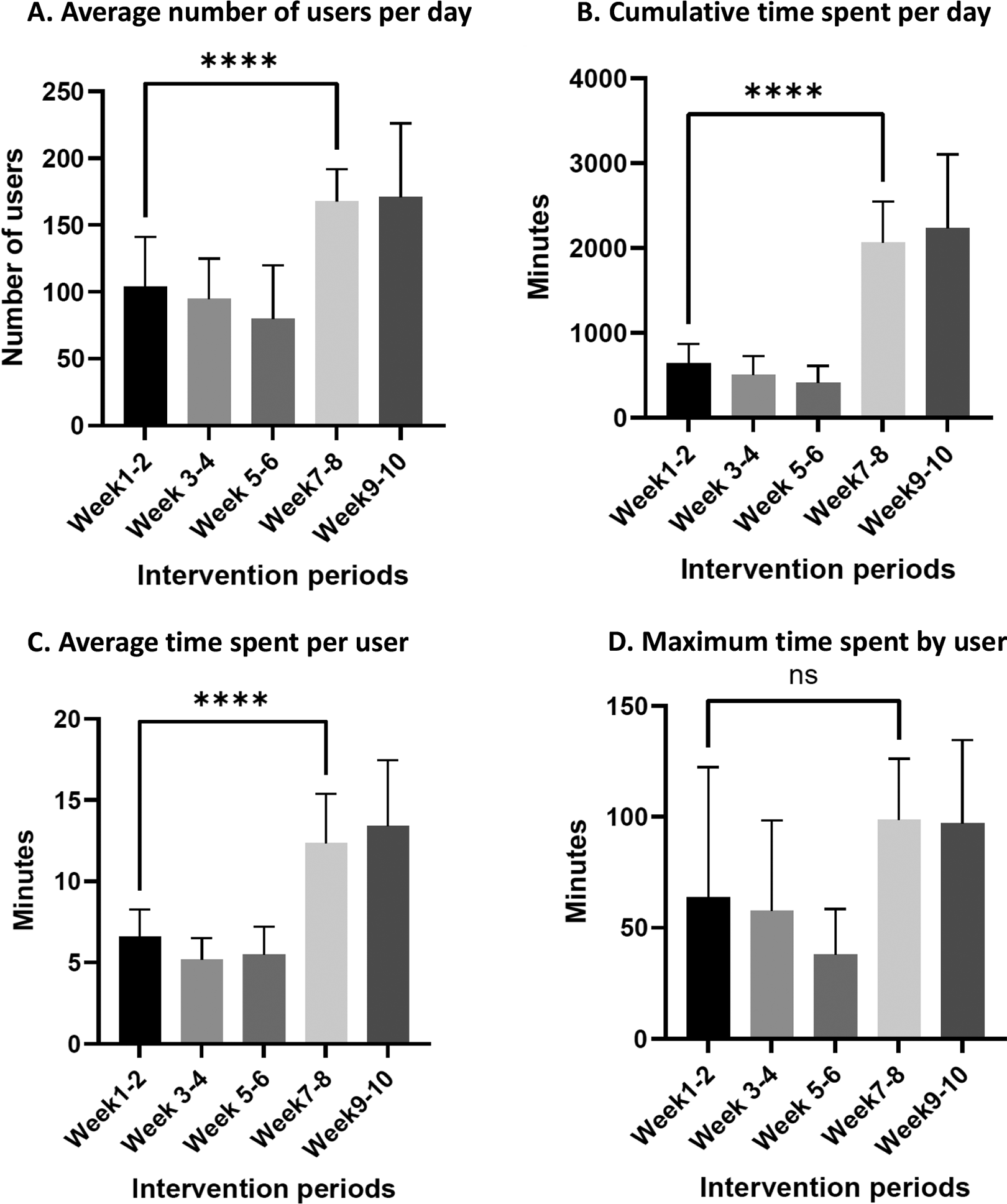
Bar diagrams showing increase in usage in balcony on video camera–based outcomes over subsequent observation periods.
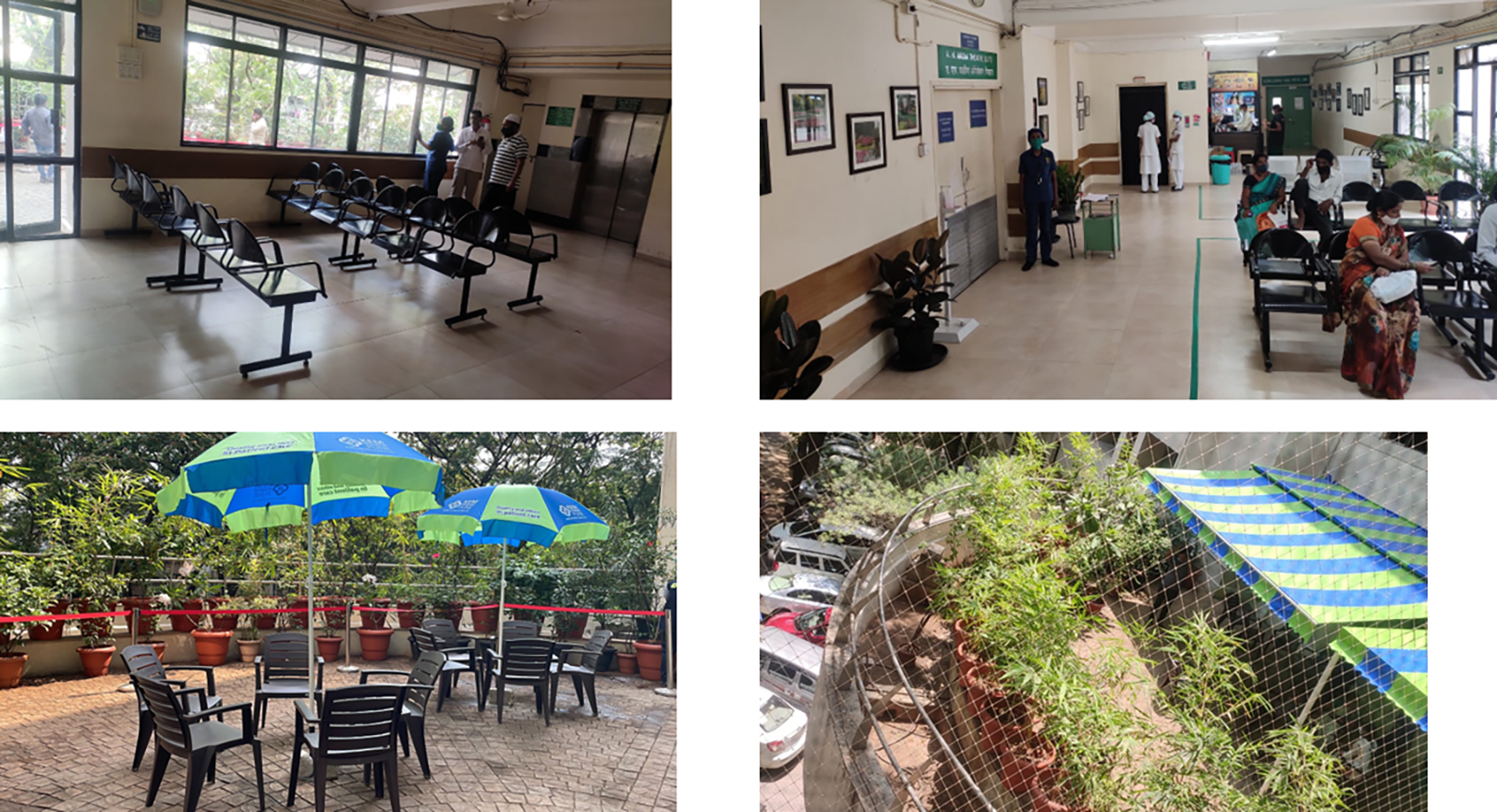
Photographs of each design intervention. (A) Reoriented seating to make the balcony more prominent (Week 3–4); (B) directional floor patterns, indoor plants, and nature inspired art to reduce indoor sensory stimulation (Week 5–6); (C) introduction of larger plants, umbrellas, and chairs as stereotypical elements (Week 7–8); and (D) addition of an awning and waste disposal bins to improve usability (Week 9–10).
Secondary Outcomes: User Satisfaction–Based on Questionnaire Responses
Between 80 and 100, family caregivers answered the questionnaire in each 2-week observation period, administered on the day following the surgery (Table 2). Regardless of questions asked, we found a tendency for users to answer with high scores: The median score for Likert-scale answers to all questions, in nearly all observation periods, was four. This was seen in questions related to the physical surroundings (Questions 3–8) as well as in those which were not related. Consequently, there was no change in median scores, nor the proportion of participants answering with high scores, over the intervention periods. On analyzing the free form answers to what participants deemed a positive experience in the waiting duration, we found that there was a significant increase in the proportion whose answer pertained to the outdoor space or greenery in Week 11–12 as compared to baseline.
Satisfaction Questionnaire Outcomes Regarding Waiting Experience.
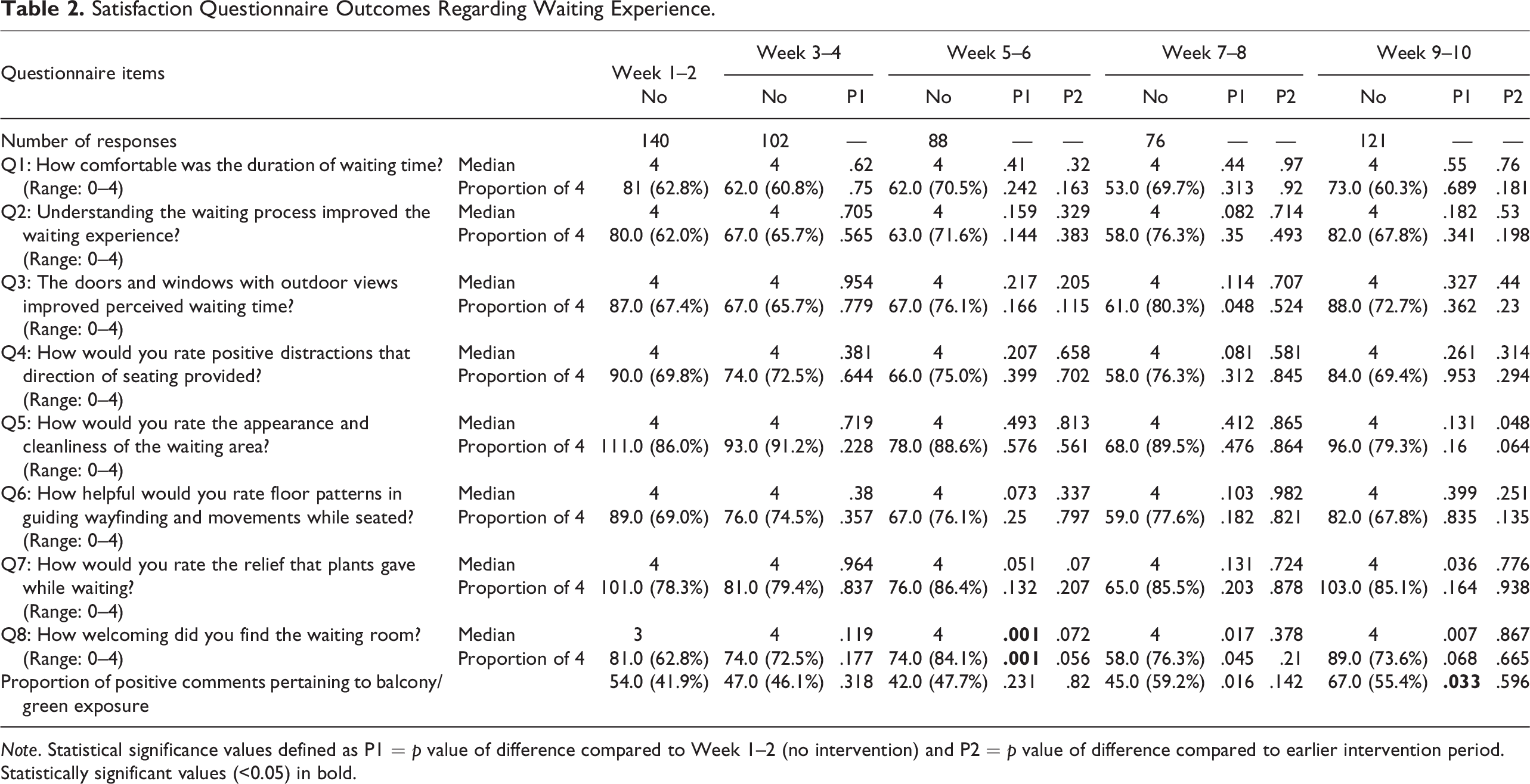
Note. Statistical significance values defined as P1 = p value of difference compared to Week 1–2 (no intervention) and P2 = p value of difference compared to earlier intervention period. Statistically significant values (<0.05) in bold.
Adverse events and safety
From video camera data, we found no potentially dangerous activities in any observation period.
Discussion
In this novel proof-of-concept study, we tested the effectiveness of low-cost design interventions based on the principles of behavioral economics on influencing human behavior toward a perceived benefit in a hospital setting. Sequential changes based on choice design showed a significant increase in the usage of an outdoor, green space by family caregivers waiting outside an OT. The maximum increase in usage occurred by adding stereotypical elements within the outdoor space and improving its usability. Despite the robust differences seen in these direct outcomes of usage, the questionnaires failed to demonstrate any change in participant satisfaction parameters over the intervention periods.
There is established evidence that exposure to nature, including simulated views, helps reduce stress levels (Gu et al., 2022). Viewing nature was shown to reduce anxiety and anger, while improving calmness (Staats et al., 2016). This salutary effect is likely to be causal—with robust evidence available from randomized controlled trials (Ulrich et al., 2008). Gardens in hospitals were beneficial for not only the patients but also for their families as well as healthcare workers (Dushkova & Ignatieva, 2020; Scartazza et al., 2020).
Evidence-based design (EBD) has traditionally had a goal of improving health outcomes through data-based choices in design, and designing healthcare spaces was centered on the patient. However, many spaces in healthcare facilities are used by attendants and family caregivers. In India, structures of families mean most patients are accompanied by multiple members of their families to fulfill the roles of companions, planners, financial representatives, and so on (Shaji & Reddy, 2012). Relieving caregiver stress improves patient outcomes as well the overall hospital experience; consequently, a growing body of evidence—chiefly from the ICU domain—seeks to identify needs of family caregivers (Scott et al., 2019). The beneficial effects of garden spaces in hospitals have been shown to aid emotional well-being of the family members as well in addition to patients (Martin et al., 2021; Reeve et al., 2017; Whitehouse et al., 2001). We chose to conduct this pilot study in caregivers since they are assumed to be healthy and thus probably not affected by multiple possible disease-related confounders such as pain, cognitive impairment, and medications that would influence the experience of the patients themselves.
Despite the availability of an outdoor green space, as well as the robust evidence of its benefits, we noticed that the balcony was being suboptimally utilized. The reason for this counterintuitive observation could possibly also lie with another principle from behavioral economics, namely the status-quo effect (Rice, 2013). The effect shows that people overwhelmingly prefer the current state of affairs and will resist making a change even if the alternative is potentially more beneficial. Measures to circumvent this cognitive bias, such as opt-out systems, have been successful in promoting uptake of various schemes such as insurance policies (Thaler & Sunstein, 2008). The status-quo bias in waiting caregivers could possibly mean an inertia to change from the current state of waiting in the indoor sitting area. With this hypothesis, we attempted using principles of behavioral economics in trying to “nudge” users toward the use of open spaces and access to greenery. We showed that simple, cost-effective measures designed to subliminally bring attention to an already present outdoor space, increased its usage substantially. There was a significant increase in balcony usage over the four intervention periods. The major shift in use was seen in the third intervention, namely the use of stereotypical elements (Week 7–8). The third and fourth interventions differed from the first two in having improvements in the actual outdoor space. The addition of plants, chairs, and shade improved the usability of the balcony translating into more frequent and longer interactions with the greenery. In addition, the use of stereotypical elements is likely to subliminally influence persistence in the space by invoking memories of familiar garden spaces. Since the interventions were sequential, it is difficult to separate the effect of one particular as most useful. However, the users were independent on each day, and thus it is difficult to believe that the earlier interventions “primed” balcony usage in the subsequent weeks.
In the absence of randomization, it is difficult to attribute causality of the observed change in usage to the intervention itself; important confounders are likely to exist. The aim of the first intervention, by realigning indoor seating, was to improve the views of the outdoor balcony. However, this changed seating plan improved the ability of caregiver families to sit in a group and have a conversation in the indoor area. This could explain the reduced usage of the balcony during the first 2 weeks. Aiding conversation may also have worked in the last intervention in the outdoor area, thus contributing to balcony usage. We acknowledge that our study design does not allow us to test the actual mechanisms that were at play and should influence future design in thinking about various effect modifiers.
Despite the substantive change in usage of green space, it was intriguing that the questionnaires failed to demonstrate any measurable change in user-reported satisfaction with each intervention. This discrepancy between observed behavior changes and satisfaction unveils questions about methodology and possible biases in the participant group. We found an overwhelming inclination for participants to answer with high scores, regardless of question or intervention period. We suspect these inaccurate satisfaction data stemmed from an inability of participants to truly understand questions, the presence of leading questions, or a reluctance to voice out negative opinions against a treating facility (Story & Tait, 2019). Knowing the educational status and economic background of the participants could have helped. Another possibility is a representation bias, with only families of patients who had successful surgeries choosing to answer the questionnaires. Additionally, it is possible that time spent on the balcony was a small portion of the overall hospital experience and thus did not help sway their opinion.
Our results highlight the possible pitfalls of using satisfaction questionnaires as primary outcomes, especially in the low-middle income countries with suboptimal levels of literacy (Kelley et al., 2003). In contrast, the increase in usage based on videos provided robust, objective evidence which was not hampered by the participants’ levels of understanding and literacy. The discrepancy also underlines the subliminal nature of the benefits of these interventions, which did not translate into articulation by the users. Our findings have a bearing in designing questionnaires in future studies in this population. Possible improvements are psychometric testing and validation, increasing the number of possible responses to seven, and ensuring participant understanding of the questions.
Strengths and Limitations
To our knowledge, this is the first formal effort in using choice design to influence caretaker behavior and nudging them toward the use of a green outdoor space with multiple perceived benefits. Strengths include the use of objective, painstakingly recorded usage outcomes from a video camera as primary outcomes, and moderately long observation periods in a single season to avoid biases such as holidays or major temperature changes. This allowed us to observe robust numbers of users as well as obtain satisfaction data from nearly 500 participants. We also believe conducting the study on caretakers vis-à-vis patients themselves allows a cleaner attribution of the behavioral changes observed to the interventions. Limitations include the observational design; however, it would have been methodologically difficult to conduct a controlled trial in a singular space, especially since some interventions were permanent. The questionnaires were not psychometrically tested. Knowing the demographics and diversity in the participant pool would have strengthened the applicability. However, these were not recorded to protect confidentiality. As mentioned above, there was a possible bias in those willing to answer questionnaires, leading to uniformly high satisfaction ratings. Finally, we chose to conduct the study in one season to avoid confounding by temperature and weather conditions. Further observations in other seasons, including monsoons and winters, as well as in other countries with varying climate conditions, would add confidence in the generalizability of these techniques.
Conclusion
We found that cost-effective interventions based on choice design were effective in bringing about a change in the behavior of family caregivers in a tertiary care hospital in India. These users were nudged toward an increased usage of an outdoor, green balcony space with resultant perceived benefits, as observed by video cameras in the intervention space. Future work will seek to apply these principles to change design in order to help patients as well as the hospital staff.
Implications for Practice
Principles of behavioral economics can be effectively employed in design to influence behavior toward beneficial or healthy practices. Adding stereotypical elements, generating memories in people, was most effective in nudging patient–caregivers toward using an outdoor balcony space. Video camera-based usage outcomes show a robust increase in space usage, which was not reflected in questionnaire-based outcomes. These might be more useful in low-middle-income countries.
Footnotes
Acknowledgment
The authors would like to thank Ananya Biswas, Chetan Mal, and Veena Rane for their help in logistics.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received intramural funding from the KEM Hospital Research Centre, awarded to Shirin Wadia (principal investigator).