
Abstract
Objectives:
This article examines a novel theoretical framework, which we term Home Triad, for research and practice involving people living with dementia (PLWD).
Background:
Most of the existing home-related research on PLWD focuses on interior modifications, home care interventions and models, place attachment, and/or institutional homelike environments. However, limited studies have examined the meaning of home from PLWD’s perspective, and even fewer have simultaneously considered the individual experience of PLWD, the external power (e.g., the role of design), and their interaction dynamics in the meaning-making process.
Methods:
We developed home triad based on Lefebvre’s spatial triad. Inspired by Chaudhury’s home story structure, we conducted a life story analysis of a person living with dementia, “Kai,” under four contexts—childhood home, neighborhood and city, daily routine, and attachment—within home triad.
Results:
Home triad abstracts “home” with a dialectically interconnected relationship of the conceived, perceived, and lived home. Through PLWD’s everyday life, the essence of home is primarily shaped by the interaction between their lived and perceived homes. However, a person’s experiences of and participation in home living activities are also planned and/or regulated by different groups of people (caregivers, designers, and policymakers), who play important roles in the conceived home. Critically examining how PLWD’s lived and perceived home is constrained or enabled through the conceived home deserves greater future research efforts.
Conclusion:
A systematic examination of the essence of home for PLWD using home triad can facilitate subsequent research and practice that promote PLWD’s health, well-being, and quality of life.
Introduction
I want to go home!
In this article, we present a personal narrative, “Kai’s story,” based on observations and conversations between the first author and the individuals “Kai” and “Yu” (pseudonyms used to maintain confidentiality) to introduce and explore a theoretical framework, Home Triad, which is developed from Lefebvre’s spatial triad. This proposed framework brings together and builds on two closely associated research areas: (1) dementia-friendly environments, especially home/community environments, and (2) the application of Lefebvre’s spatial triad in the field of healthcare, especially dementia care. Furthermore, this framework contributes to research and practice by considering the multiple moments through which homes are produced by, with, and for PLWD.
Research Gap
Home has significant benefits regarding positive feelings and meaningful activities for PLWD (Soilemezi et al., 2019) and the reduction of caregiver burden. According to the Centers for Disease Control and Prevention [CDC] (2019), most PLWD in the United States receive care in their homes. Similarly, 61% of PLWD over 65 in the United Kingdom are living in the community (Prince et al., 2014), and South Koreans have a strong preference for caring for the elderly with dementia at home (Park, 2012). Also, home-based care provided by family members is the main form of support for individuals with dementia in China (Xiao et al., 2014). Research on the topic of PLWD’s home can involve many aspects, such as modification and renovation in the physical home environment (Struckmeyer & Pickens, 2016; van Hoof et al., 2010), supportive interventions and models for homecare (Low & Fletcher, 2015; Zabalegui et al., 2014), place attachment to the home during old ages (Aliakbarzadeh Arani et al., 2022), and even the development of the institutional homelike and therapeutic environment (Day et al., 2000; Verbeek et al., 2009). However, only a relatively limited number of studies have touched on the meaning of home for PLWD comprehensively and systematically.
In Soilemezi et al.’s (2019) systematic literature review of the role of home environments for PLWD, a person’s home experience is negatively influenced by the disruption and tensions between safety and comfort, familiarity and adaptation, and risks and independence. Therefore, modifications are needed when home conditions are no longer suitable for PLWD in terms of safety, accessibility, and comfort (Soilemezi et al., 2019; Struckmeyer & Pickens, 2016). Soilemezi et al. (2019) noted that modifications with full involvement of caregivers, family members, and the person with dementia are best suited to take the PLWD’s physical, cognitive, social, and behavioral needs into consideration. This, in turn, can help PLWD adapt to their own homes with better care, maintain their functions, and improve their quality of life. Of the already few studies on the meaning of home from the perspective of PLWD, even fewer have simultaneously considered the role of design in the meaning-making process.
Theoretical Foundations
Theories Related Meaning of Home
More than 3 decades of research on the meaning of home has shown that it is a significant factor across the life span and especially so for the elderly. Després (1991) thoroughly examined the literature on the meaning of home and outlined ten categories—Security and Control, Reflection of One’s Ideas and Values, Acting Upon and Modifying One’s Dwelling, Permanence and Continuity, Relationships with Family and Friends, Center of Activities, A Refuge from the Outside World, Indicator of Personal Status, Material Structure, and A Place to Own. Additionally, Sommerville (1997) summarized Després’s (1991) review for related theories and settled on two overarching frameworks: (1) Home represented deep-rooted psychological needs for identity, control, privacy, security, intimacy, and social status from psychological and social–psychological perspective, and (2) phenomenological and developmental perspectives focus on permanence and continuity and that the meaning of home changes throughout a person’s lifetime.
As people age, the meaning of home indeed changes. Older people spend more time at their physical home as well as accumulate more home memories. Molony (2010) conducted a qualitative metasynthesis on the meaning of home for the elderly, aiming at informing nursing practice during residential transition of the elderly. She concluded that home is (1) a place-based entity, representing older adults’ empowering, refuge, relationship, being known and knowing others, and self-reconciliation; and (2) a transitional process of integration, involving integration, closing one door and opening another, homelessness, nesting, and the “Meaning of Me” moving forward for the elderly. Oswald and Wahl (2005), on the other hand, drew from extensive studies on environmental psychology and gerontology to develop a tripartite framework for understanding the meaning of home in later life—the social home, the physical home, and the personal home. The personal home further included behavioral aspects (e.g., activities), cognitive aspects (e.g., identity), and emotional aspects (e.g., rootedness).
For PLWD, their meaning of home may further change due to cognitive impairment. As an example, Chaudhury (2008) identified four themes of how homes become a part of memories based on home stories collected from PLWD and a review of related empirical and theoretical studies: (1) Belonging to a place: Home provides a sense of belonging that is created by the person’s experiences with particular others in particular places; (2) Place anchors outside: Home embodies and anchors lived memories whereas other places shape, mediate, and anchor place memories; (3) Place as process: Places become meaningful through the involvement of the person’s aspirations, emotions, and expectations; and (4) Attachment to home: The person builds deep affective bonds with their home through significant life experiences and identity processes. Specifically, place attachment, as the link to the space and home in which the elderly have spent part of their lives and established relationships, is intricately related to the meaning of home for PLWD with both concepts being well studied concurrently (Burholt & Naylor, 2005; Rowls, 1993).
As Sommerville (1997) stated, “…an individual’s meaning of home can be internally explicated as a physical/psychological/social construct…” (p. 226), highlighting how individuals as occupants or users construct their meaning of home. While the insider’s perspective is undeniably significant, the meaning of home is also and often influenced by outsiders (e.g., designers, planners, policymakers) in an invisible form. Research on the meaning of home for the general elderly population has included an exploration of both individual experiences and external influences (e.g., Molony, 2010; Oswald & Wahl, 2005). Notably, Oswald and Wahl (2005) highlighted individual and external interaction dynamics. However, when limited to PLWD—the meaning of home focuses primarily on the perspectives of the home insiders (i.e., PLWD themselves) and overlooks external power and the relationship between them (e.g., Aminzadeh et al., 2010). Therefore, we identified a gap, a lack of attention to the dynamic individual experience of home as well as the role of those outsiders, other than PLWD, who have the power to shape those places. Therefore, we drew on Lefebvre (1991), French Marxist, existentialist, philosopher, and sociologist to develop such a framework. On the production of space, Lefebvre (1991) stated “The space thus produced also serves as a tool of thought and of action; that in addition to being a means of production, it is also a means of control, and hence of domination, of power” (p. 26). He introduced the concept of the spatial triad to integrate external power’s influence on social space. Building upon this framework, we believe that Lefebvre’s spatial triad offers a robust foundation for comprehensively and multidimensionally understanding of the meaning of home for PLWD.
Lefebvre’s Spatial Triad
In The Production of Space, Lefebvre proposed the spatial triad, whereby produced social space can be broken down into three dialectically connected dimensions: (1) spatial practice (the perceived space), (2) representation of space (the conceived space), and (3) representational space (the lived space). Carp (2008) further interpreted the spatial triad in a more structured and concise manner. As a result, we adapted Carp’s (2008) interpretation and developed a graph that helps illustrate the relationships among the three dimensions (see Figure 1).
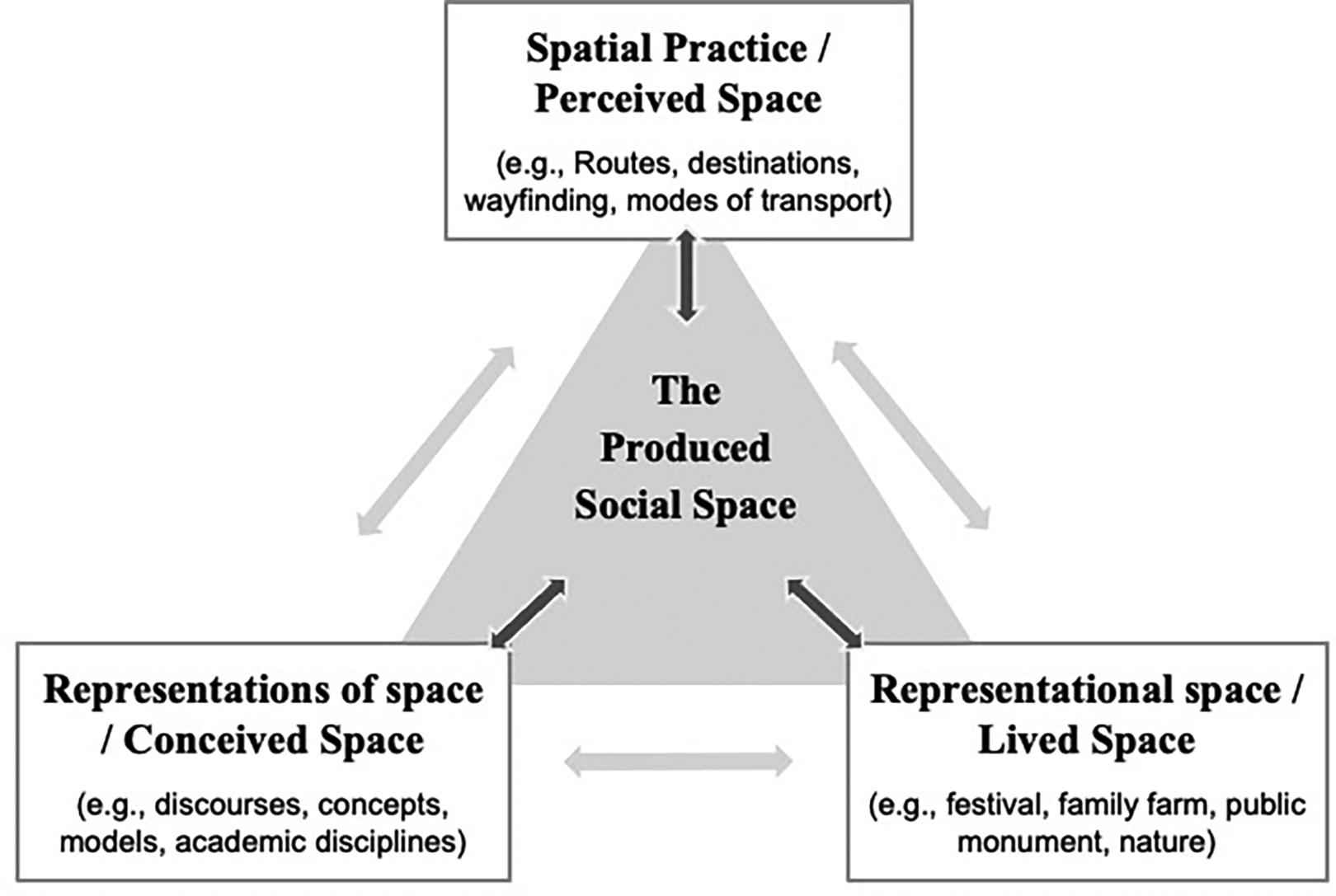
Lefebvre’s spatial triad based on Carp’s works (2008).
In the triad, spatial practice/perceived space refers to the materially produced space, which exists physically and can be observed empirically. Simply stated, it is what we often refer to as physical space. People perceive space through their senses, such as seeing, smelling, and touching. All the acts of sensory perception are traceable and can be captured. Representation of space/conceived space refers to the abstract mental space, which is conceived by discourses of power and knowledge. It is a rationalized and intellectualized space that is presented in the form of a floor plan, models, and so on and is based on the unitary organizing principle, codes, et cetera. People conceive this space through mental activities, including thinking, imagining, and interpreting, a responsibility often controlled by professionals or others with administrative roles. The tangible expression of these conceptions may be on paper or in words as the production of knowledge. Representational space/lived space implies the social space and emphasizes meaning and human experience. People live within this space and recall their unique or shared experiences, including loving, fearing, and remembering. The subjective or intersubjective experiences of lived space are not only rooted in the here and now but also connected to the past, present, and future.
Lefebvre’s spatial triad has been used as an analytical tool to study urban public spaces (e.g., Allen & Pryke, 1994; Soja, 1996; Watkins, 2005). Learmonth and Hardin (2006) introduced Lefebvre’s theory into evidence-based healthcare management. Van der Meide (2017) contributed to and examined humanizing hospital care using Lefebvre’s triad, advocating for healthcare professionals to pay more attention to the dynamic interplay between these three dimensions for improved care practices.
Lefebvre’s triad offers a fresh viewpoint on the perspective of outsiders (e.g., designers, planners, policymakers), revealing how they conceive the space independently of insiders and often through normative design discourses, and subsequently represent it in forms such as drawings, policies, and the like that hold power in their ability to shape space. The “Representation of Space/Conceived Space” pillar is frequently overlooked, yet its role cannot be disregarded. Little attention has been paid to the spatial underpinnings that set the ground for the fluid and contextual home for PLWD, and none from the systematic three-dimensional perspective of conceived, perceived, and lived. Consequently, there is a need for a systematic framework to investigate the home for PLWD that incorporates this essential element. To address this need, we have developed a novel theoretical framework termed Home Triad, based on Lefebvre’s spatial triad. The framework aims to provide a more comprehensive understanding of the various dimensions of PLWD’s home, enabling researchers and practitioners to better cater to their needs through research and practice.
Home Triad
Under home triad (see Figure 2),
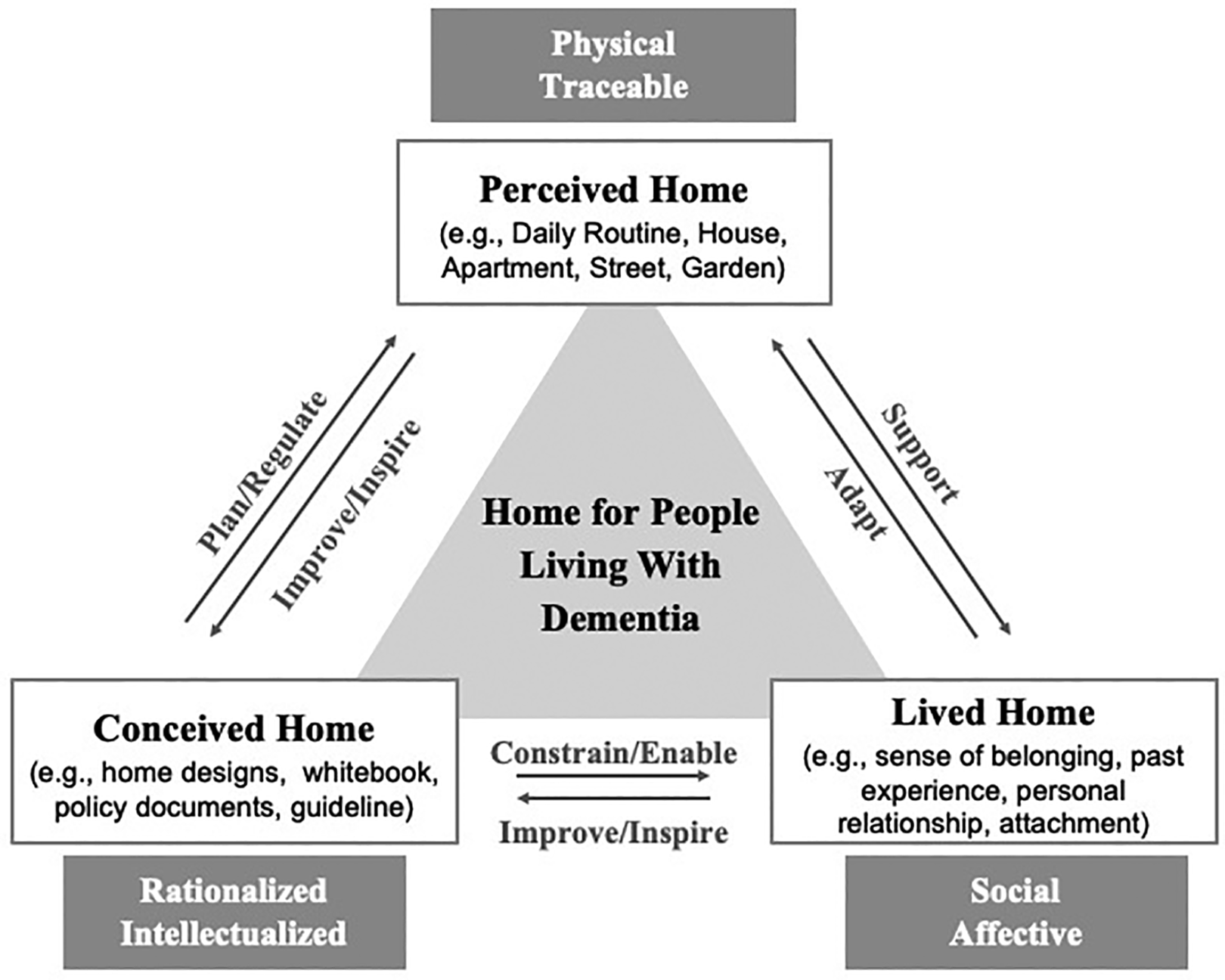
Home triad for people living with dementia based on spatial triad.
The Interconnected Relationship of Conceived, Perceived, and Lived Home
Lefebvre (1991) noted that “…the lived, conceived and perceived worlds should be interconnected” (p. 40). In other words, the combined action of these three pillars, one with the other, leads to the production of space. This is no less true for PLWD as the interconnected aspects of home as conceived (rationalized and intellectualized), perceived (physical and traceable), and lived (social and affective) co-construct PLWD’s homes. PLWD shape and interact with the physical, conceptual, and social home; conversely, the homes PLWD inhabit shape social practice, activities, and inquiries. Figure 2 depicts the interwoven relationship between conceived, perceived, and lived home. A more in-depth explanation will be provided in the following paragraphs.
As suggested by the person–environment fit theories and place attachment theories, there is a strong bond between people’s physical environment and social environment. PLWD’s physical home supports their social home, and in turn, their social home supports PLWD to adapt their physical home to their evolving needs, perceptions, and memories of home. The perceived home reflects the physical environment, not only home as the living environment but also the everyday life that can be visibly captured. The lived home refers to the social environment, including PLWD’s experience, personal relationships, attachment, et cetera.
For PLWD as for all people, how they relate to or feel emotionally about home is of great importance. As people interact with places they develop an, “attachment to place…a set of feelings about a geographic location that emotionally binds a person to that place as a function of its role as a setting for experience” (Rubinstein & Parmelee, 1992, p. 139). Furthermore, as outlined in the person–environment fit theory (Van Vianen, 2018, p. 77), “people have an innate need to fit their environments and to seek out environments that match their own characteristics.” The dynamic interchange between physical home and lived home includes a diversity of settings, such as community gardens for seniors’ gatherings and the home dining room for family reunions (Murroni et al., 2021).
As dementia progresses, the perceived home for PLWD needs to be adapted to fit their new needs, while the lived home can be used as an aid during the adaptation to help PLWD experience the perceived home better by maintaining the emotional attachment with their home environment. For example, caregivers can modify the home with decorations that resonate with memories of home that become more prominent for PLWD. This is particularly important because PLWD experience memory loss including (1) not being able to create new memories, (2) taking longer to retrieve information, and (3) not being able to retrieve information (Alzheimer’s Society, 2021). In light of this, PLWD may recall or speak about their earlier memories in detail while forgetting more recent events. Therefore, the lived home changes to revolve around their older memories, even those going back to their childhood. Staying in touch with former acquaintances or frequently recalling past experiences is of greater significance for their social familiarity (Ward et al., 2018). In various ways, a desire to revisit old places—either physically or mentally—arises. They may recollect old pictures and old things in their living home and hope to go out more often to catch up with friends. In this way, perceived and lived home moments are simultaneously provisional of PLWD physical and social familiarities. When these moments of home triad are attended to, PLWD can be supported to maintain their social and functional abilities and experience cognitive and emotional benefits such as better comfort, reduced effort, and increased processing speed (Son et al., 2004) that may extend beyond the four walls of the home.
Healthcare providers (e.g., formal caregivers, researchers, designers, and policymakers) are a part of home triad position of the conceived home. Though not often acknowledged, this moment of the production of home is influential in that it may be driven more by professional or institutional ideas about home for PLWD, which overshadows the perceived and live homes. The conceived home indicates the rationalized and intellectualized home, including home-related design, organizational policies, and procedures, and so forth. This includes planning and regulating a safe and supportive physical home while simultaneously constraining and enabling certain aspects of the social home that are more abstract and less specific to the PLWD themselves. For instance, some PLWD regard the garden in their community as part of their home. Several empirical studies, research-based design recommendations, and general guidelines provide legislators, architects, urban planners, lending institutions, developers, and landscape architects with evidence that there is a need to construct the conceived garden home for PLWD (Rodiek & Schwarz, 2013). These conceived design guidelines and recommendations influence the actual spatial practice of the therapeutic garden, as well as PLWD’s lived experience within the garden. Specifically, dementia-friendly garden design usually includes a circular path leaving and returning to one access point in order to avoid dead-end paths (Calkins, n.d.). In this way, the perceived physical movement of PLWD and their anxiety and other lived emotions caused by wayfinding and wandering can be significantly impacted by the conceived design. Moreover, staying close to people with whom they have long-term relationships plays an important role in PLWD’s lived home; thus, those people must also be conceived of in dementia-friendly home environments. A number of adaptable sitting options such as chairs and benches in the garden provide PLWD the opportunity to spend time outdoors with their family or friends. However, these sitting areas will be less preferred if they are not designed with appropriate shade or shelter from the elements. Taken together, the conceived home focuses design on what may seem obvious, but there is a need to incorporate how PLWD actually use and experience their homes—in either predictable or unexpected ways—based on their own demands and feelings. This requires healthcare providers and designers to continually reflect on and be inspired by improving, updating, renovating, modifying, and even involving PLWD’s participation in adapting their homes.
Understanding Home Triad: Kai’s Home Story Example
A home story is a place-based, home-related biographical sketch that synthesizes people’s memories of home (Chaudhury, 2008). In his 67 years of life, Kai experienced two significant home moves. Kai and his siblings were raised on his family’s farm in a village (see Figure 3) outside of a small city located in southwest China. Kai later left home and sought work as an accountant in the city, where he and Yu raised two sons and a daughter in a two-bedroom apartment downtown (see Figure 4). After their retirement, Kai and Yu relocated to a three-bedroom apartment in a new neighborhood (see Figure 5) half mile from their previous one, a convenient location that enabled them to visit their extended family and receive care from their children. After his first stroke at the age of 63, Kai’s cognitive functions gradually deteriorated. Three years later, after a second stroke, Kai developed dementia, along with diabetes and poststroke sequelae. As a result, he had to commute frequently between his daughter’s home in a bigger city (for better quality rehabilitation treatments) and his own apartment, which took 6–8 hr by bus each way.
Kai’s childhood home.
Kai’s first apartment.

Kai’s retirement apartment.
Kai and Yu eventually decided to discontinue traveling when Kai’s health conditions improved slightly. They chose to remain in their own apartment in the small town to live a more familiar life and spend time with their acquaintances. However, Kai still suffered from stroke-related health problems, making it difficult for him to function independently. Yu was also concerned about the risk of additional stroke. Furthermore, Kai’s dementia affected his cognitive capabilities. Occasionally, he could not remember where he was or how to get home. Driven by Yu’s worries over Kai’s health and safety, specifically his dementia and past unexpected strokes, it was difficult for her to leave Kai unattended. Consequently, they eventually formed a daily routine (see Figure 6) that made them inseparable from each other. Their day began with worship by chanting and burning incense in a guest bedroom. They would then have breakfast and go to the grocery market located in the adjoining city block. After shopping, they would go to the nearby cultural square to chat or play cards with their acquaintances. Their outing would conclude by walking along the riverfront before returning home for lunch, followed by a nap. In the afternoon, Kai would accompany Yu to the local community senior center to play mahjong (a Chinese game played by four people with 136 or 144 pieces of rectangular tiles) until 5 p.m. Then, they would walk home together to prepare dinner, where they were joined by their children and grandchildren nearly every evening, during which time everyone shared what they experienced throughout the day. In the same manner as their morning, Kai and Yu’s night began with burning incense, chanting, and worship. Later, if the weather was favorable, Yu would ask Kai to go for a walk along the riverfront as an after-dinner activity. After a slow walk home, they would go to bed at approximately 10 p.m.
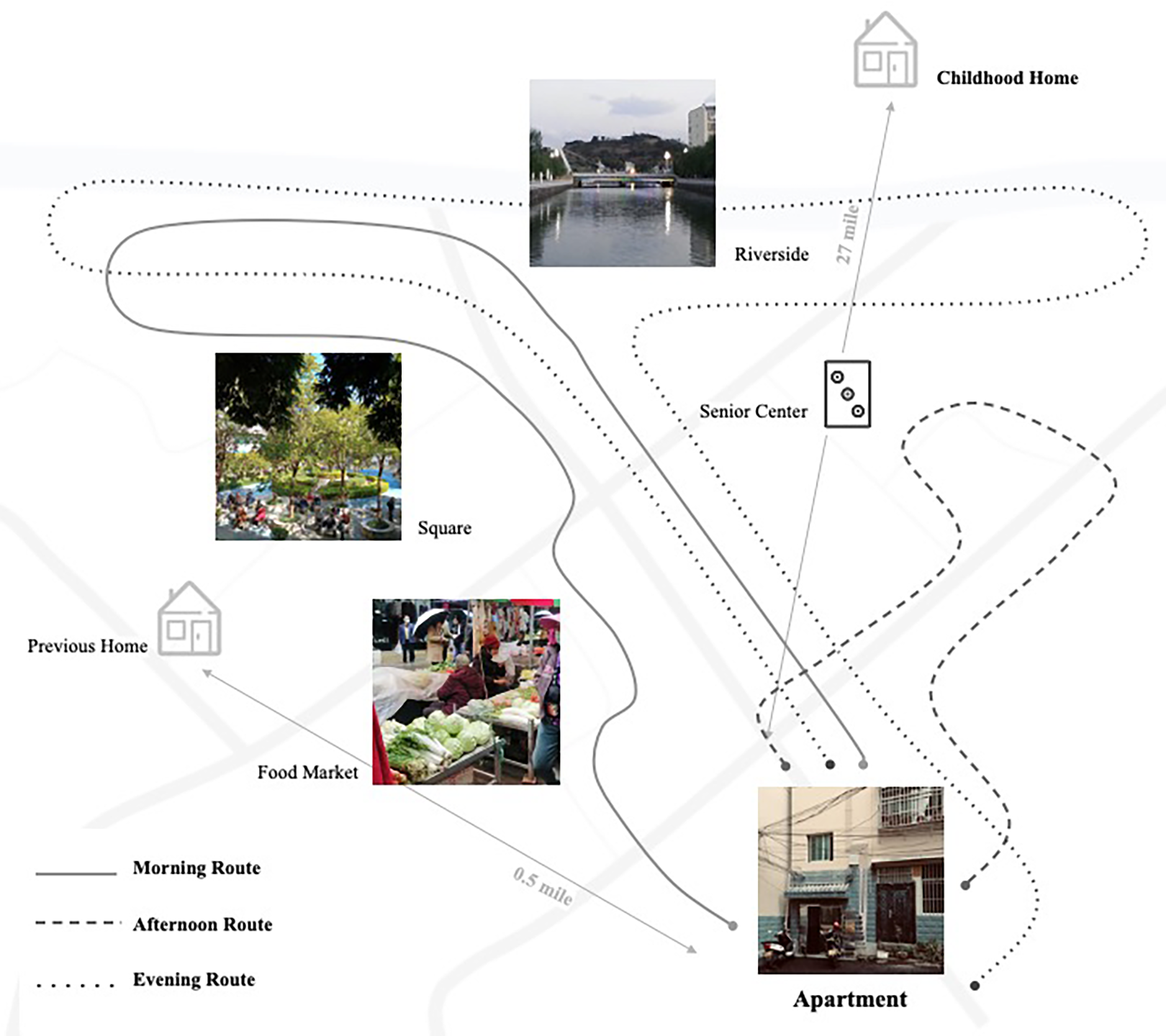
The daily routine of Kai couple.
Although the physical home is present in this narrative, demonstrated by Kai’s daily routine, his home went beyond his residence to include the neighborhood and even the city. As such, we recognize that the meaning of home is multifactorial and multiscalar for most people, especially those living with dementia such as Kai.
Kai’s Home Stories Within Home Triad
To more clearly illustrate home triad and the interconnected relationship of the three pillars, we conducted a home story analysis of Kai’s story within home triad. Kai’s story includes rich home experiences from a rural childhood farmhouse to his downtown apartment where he raised his children, to another apartment where he lived with his wife after retirement. Inspired by Chaudhury’s four-theme structure of home story (i.e., belonging to a place, place anchors outside, place as process, and attachment to home) mentioned earlier (Chaudhury, 2008), we analyzed Kai’s home from different contexts—childhood home, neighborhood and city, daily routine, and attachment—to interpret the key components and their relationships in home triad for PLWD.
Childhood home
The childhood home impacts PLWD’s home meaning-making. As for Kai, his childhood home served as the foundation for his strongest memories and was the place he most desired to return to. The two-story farmhouse where Kai grew up was
Neighborhood and city
For PLWD, the places or landmarks outside their residence may contribute to defining their home. These may include their neighborhood, where they were married, the city they lived in during adulthood, and other places where they spent meaningful time and created precious memories. In Kai’s case, moving downtown from a rural area influenced his perception of home. Kai’s two apartments before and after retirement were located in the same city and in two neighborhoods close to each other. Therefore, during these two periods of his life, there was continuity between the neighborhood places where he spent time. As time went by, the neighborhoods and the city became a part of Kai’s home story. In Kai’s everyday life, his
Daily routine
Home meaning-making is part of a dynamic interchange between person and place, not only an outcome but also a reflexive and circular process as each aspect informs and influences the other. Kai shaped his memories and views of home through his personal experience and everyday life. Kai’s two major home moves were a process from dependence (being supported by his parents during childhood) to independence, then back to dependence (being taken care of by Yu, his wife). To raise a family with his wife, Kai bought his first apartment. The family decorated the home with personal belongings, an example of their
Attachment
A place becoming a home for PLWD involves individual experiences, emotions, self-expression, and so on. Kai’s home reflected his attachment to his experiences, beliefs, and relationships. Kai’s attachment to home influenced how he constructed and
Summary of Kai’s story
Table 1 summarizes the above analysis and offers a more lucid depiction of the core components of home triad as illustrated in Kai’s story. Kai’s complex and multilayered home worked as a narrative tool and example to show how home triad could be applied to a particular case. From the analysis, we see Kai’s perceived home was fully illustrated by his childhood home, two apartments, the neighborhood and the city, and his daily routine. His sense of belonging, past experience, personal relationship, attachment, and religion represented Kai’s lived home. Meanwhile, in addition to illustrating his multidimensional “homes,” the analysis of Kai’s home story using home triad also helps recognize some hidden aspects of the home for PLWD.
Application of Home Triad in Kai’s Story.
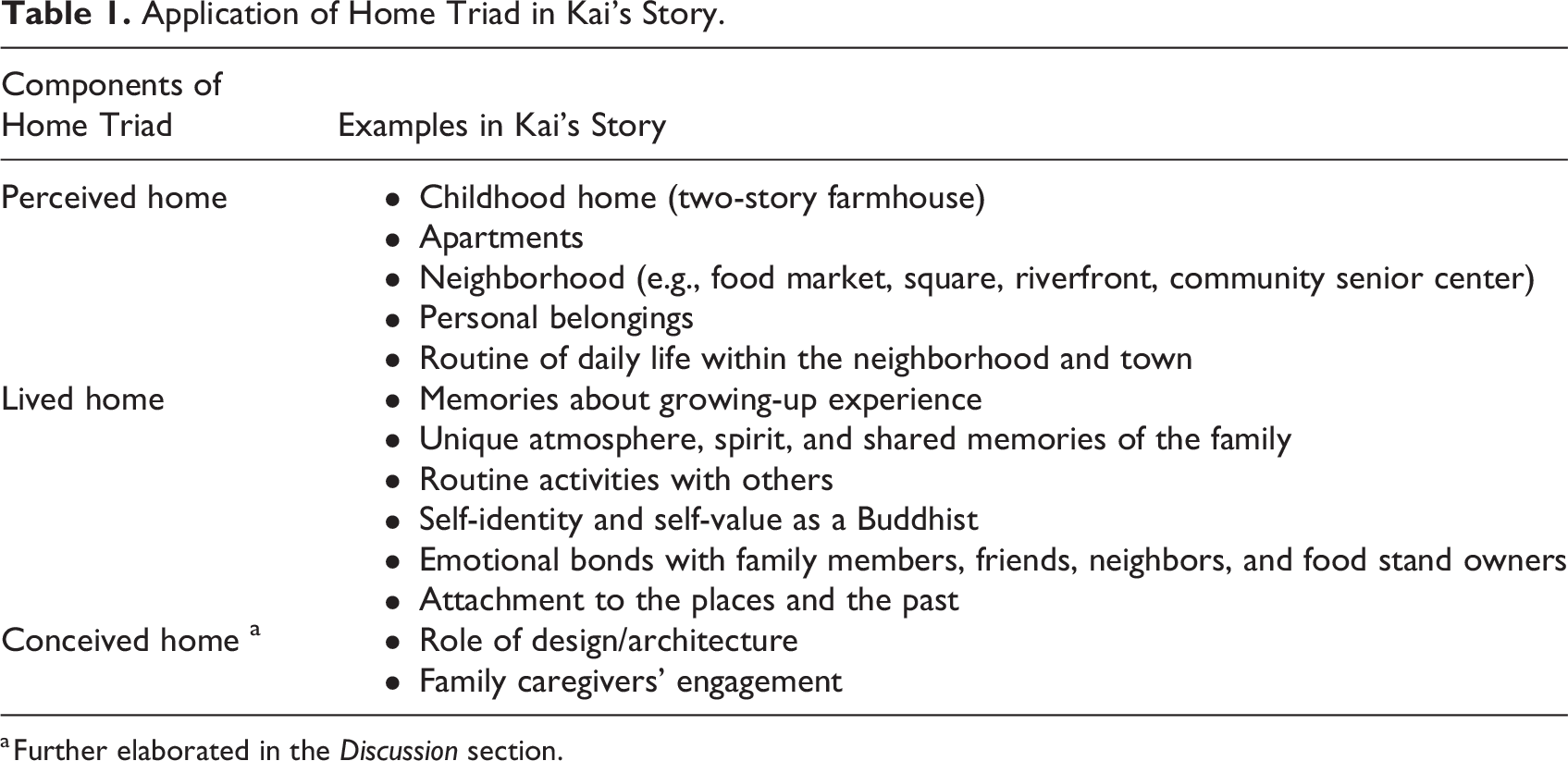
a Further elaborated in the Discussion section.
Discussion
Invisible Conceived Home: The Role of Design
Built upon Lefebvre’s spatial triad, home triad was proposed as a new framework to advance design thinking for PLWD utilizing their home. It is worth noting that the conceived home was left out of the narrative above, where we as designers can play a role in PLWD’s homes. Kai’s residence was modified by Yu to support care activities, whereas his neighborhood and town were built or designed in accordance with regulations and guidelines. As Kai’s physical and cognitive abilities declined, he gradually lost his control of his conceived home. However, Kai’s experience of and participation in the perceived and lived home over time were planned and regulated through the conceived home, where designers, developers, policymakers, and caregivers play an important role.
As outsiders, designers, policymakers, researchers, and caregivers often have the authority to decide on the conceived home for PLWD. As an indispensable pillar in home triad, the conceived home should meet the requirements of dementia-friendly environments, promoting familiarity and legibility and facilitating good wayfinding and meaningful daily activities (The Kings Fund, 2014). These factors are closely connected to the perceived home and the lived home. Critically interrogating PLWD’s lived and perceived homes is constrained or enabled through the conceived home deserves more consideration for the development of dementia-friendly environments. To create a better home environment for PLWD, we argue that it is crucial for designers to adopt a clear understanding of the lived, perceived, and conceived moments where home is produced.
Family Caregivers’ Engagement in the Three “Homes”
PLWD are usually cared for by family members or friends (CDC, 2019). After Kai was diagnosed with dementia, his wife, Yu, served as a caregiver and took on greater responsibility for his care. Yu was critical to Kai’s home-making, not only by curating their perceived apartments in a unique way but also by sharing the same lived experience as Kai. Yu shared much of Kai’s lived home in terms of memories, life experiences, and long-term relationships. Moreover, after Kai’s strokes, he and Yu became almost inseparable, sharing and influencing each other’s perceived physical environments and daily routine. As Kai’s health and cognitive functions gradually declined, Yu often managed his perceived home as the place to receive care and maintain daily activities. She modified their apartment due to Kai’s changing abilities and functions. Yu therefore participated in Kai’s conceived home as a family designer and engaged in all dimensions of Kai’s home-making.
Unlike designers, policymakers, researchers, and professional caregivers, informal family/friend caregivers have unique roles as they are participants in conceived homes. PLWD and family/friend caregivers are generally in a long-term relationship, spending time together throughout their lives and sharing the same life experiences. Therefore, informal caregivers play an integral role in how PLWD live and adapt to their home. Considering the involvement and impacts of informal caregivers in all of the three pillars of home triad deserves further attention. Codesigning with PLWD, for instance, presents benefits such as social interaction, empathic connections, and subjective well-being (G. Wang et al., 2019). However, codesigning also comes with challenges such as difficulties in language and communication due to cognitive impairments (Hendriks et al., 2013), thus rendering the involvement of informal caregivers in the codesign process extremely important. They may contribute incomparably to the conceived home given their understanding of the PLWD’s perceived and lived home.
Home Triad for Home-Related Environment Research and Design
We view the proposed home triad framework as the primary opportunity for improved development of dementia-friendly homes. Under home triad, the three homes are intertwined and together shape the home for PLWD. This three-dimensional perspective provides a new systematic framework for home-related environment research and design as well as place/memory-based therapy.
As stated earlier, there is a paucity of scientific research that explores the essential question of what the home is or what the home means. Qualitative methods such as narrative inquiry can help researchers explore people’s stories and experiences to capture and analyze meaning-making in people’s lives (Connelly & Clandinin, 2006; Riessman, 2008). Home triad could provide a suitable theoretical framework to explore the nature and meaning-making of home for PLWD. Moreover, employing a clear theoretical framework may advance the quality of qualitative research and lead the evaluation ranking from Level 5 to Level 3 in the Levels of Evidence for Healthcare Design, which serves as a tool to aid designers and healthcare leaders in assessing the credibility, reliability, and validity of evidence supporting the impact of particular design features on outcomes (Marquardt & Motzek, 2013; Stichler, 2010).
Home triad also provides a useful and thorough lens for home modifications, aging in place parameters, and homelike environment design. Sense of home really matters. “I want to go home” is a plea often stated by PLWD, not only from those who relocate to care facilities but also those who receive home care and are in fact at home. However, current research and design projects typically consider only physical, domestic characteristics such as personalized rooms (e.g., familiar decorations and furniture), domestic furnishings (e.g., a fireplace and garden), et cetera (Day et al., 2000; Verbeek, 2009). In general, the features of a physical dementia-friendly environment fall into three dimensions (Anderiesen et al., 2014; Harris et al., 2002): (1) ambient environment (the least permanent features), such as calming music (Remington, 2002); (2) interior design (fewer permanent features), such as homelike furnishings (Cutler & Kane, 2009); and (3) architectural design (relatively permanent features), such as building layouts (Marquardt et al., 2014). A holistic exploration of PLWD’s homes based on home triad can lay a good foundation for all-dimensional, dementia-friendly design. For instance, memorabilia and personal items that support a sense of home for PLWD can help them recall positive memories, reduce their psychological symptoms and behavioral abnormalities, and guide their wayfinding by serving as environmental cues (W. Wang & Lu, 2022). Home triad could aid healthcare providers and designers in better capturing the most appropriate photos or objects with positive lived experiences, incorporating these influences into perceived spatial practice, and identifying potential generalized patterns to change corresponding conceived guidelines or recommendations. Additionally, home triad could serve as meaningful guidance for the stimulus selection of memory/place-based nonpharmacological therapies (such as reminiscence therapy) for PLWD (Cammisuli et al., 2016), as well as for better development and continuous improvement of the universal design principles. In sum, the sense of home through design can achieve its greatest holistic benefit for PLWD as their disease progresses and their memories change.
Limitations
Several limitations are important to mention regarding this development of the home triad. First, this article relied on a single home story to illustrate home triad and is not an empirical investigation of the theory. Rather, Kai’s story is a real-world example of tension and opportunity afforded by the practical application of home triad. Future research inspired by our work should consider the specific and full range of experiences and perspectives of PLWD of intersecting genders, cultural backgrounds, occupations, living conditions, and so on. Second, the complex nature of the concept of home has given rise to a diverse array of theories and studies. While our study focused on theoretical frameworks directly related to the meaning of home, we acknowledge that we omitted some environmental gerontology theories, such as Lawton and Nahemow (1973) who focus on the ecology of aging, which may only affect the meaning of home indirectly. We welcome further work on the integration of such fields into home triad. Third, Kai’s home story reveals that cultural, social, and economic factors affect PLWD home experience as considered through home triad. Future research on home triad for PLWD should pay close attention to demographic characteristics and perhaps consider cross-case comparisons. By doing so, researchers can further refine home triad and provide a broader understanding and application of the framework, ultimately benefiting PLWD.
Conclusion
Home triad developed in this article, based on Lefebvre’s spatial triad, provides a novel framework for examining PLWD’s homes from three perspectives—the conceived home (rationalized and intellectualized), the perceived home (physical and traceable), and the lived home (social and affective). This framework highlights our necessity and empowers us to consider the multiple and concurrent ways that home is produced by, with, and for PLWD. In addition to the acknowledged relationship (support/adapt) between perceived and lived home, future development of dementia-friendly homes should give more thought to how PLWD’s lived and perceived homes are constrained or enabled by the conceived home, where designers, caregivers, and policymakers play a significant role. In particular, the role and impacts of informal family/friend caregivers, who are a part of all three dimensions of PLWD’s home, deserve greater attention. Finally, the significance of using home triad to systematically examine PLWD’s homes lies in facilitating subsequent home-related design and research (e.g., homelike environments, place-based therapies).
Implications for Practice
Home triad helps healthcare providers including caregivers, researchers, designers, and policymakers touch on the essence of home—“what the home is” with a comprehensive, multiscalar, and systematic approach.
Home triad provides a new, clear, and systematic theoretical framework for home-related research, which may advance the quality of the qualitative study.
Home triad leads to a better understanding of home as produced through differentiated space relationships of the perceived, lived, and conceived homes. In particular, home triad acknowledges how the conceived design constrained or enabled the perceived and lived homes, which is crucial for designers to create a better home environment for PLWD.
Footnotes
Acknowledgment
The authors want to thank Professor Robert Warden at Texas A&M University for reviewing and providing suggestions to this article. The gratitude is extended to HyeSeung Lee for her thought-provoking insights and the provision of valuable resources as well as to Zijing Hu for his generous support in enhancing the article’s readability and logical structure. We thank four anonymous reviewers for their helpful comments on an earlier version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.