
Abstract
Background:
Studies show that workspace for the anesthesia providers is prone to interruptions and distractions. Anesthesia providers experience difficulties while performing critical medication tasks such as medication preparation and administration due to poor ergonomics and configurations of workspace, equipment clutter, and limited space which ultimately may impact patient safety, length of surgery, and cost of care delivery. Therefore, improving design of anesthesia workspace for supporting safe and efficient medication practices is paramount.
Objectives:
The objective of this study was to develop a set of evidence-based design guidelines focusing on design of anesthesia workspace to support safer anesthesia medication tasks in operating rooms (ORs).
Methods:
Data collection was based on literature review, observation, and coding of more than 30 prerecorded videos of outpatient surgical procedures to identify challenges experienced by anesthesia providers while performing medication tasks. Guidelines were then reviewed and validated using short survey.
Results:
Findings are summarized into seven evidence-based design guidelines, including (1) locate critical tasks within a primary field of vision, (2) eliminate travel into and through the anesthesia zone (for other staff), (3) identify and demarcate a distinct anesthesia zone with adequate space for the anesthesia provider, (4) optimize the ability to reposition/reconfigure the anesthesia workspace, (5) minimize clutter from equipment, (6) provide adequate and appropriately positioned surfaces for medication preparation and administration, and (7) optimize task and surface lighting.
Conclusion:
This study finds many areas for improving design of ORs. Improvements of anesthesia work area will call for contribution and cooperation of entire surgical team.
Keywords
Background
Published studies (Held & Krueger, 2000; Joseph et al., 2018; Joseph et al., 2019; Joseph et al., 2021; Jurewicz et al., 2020; Palmer et al., 2013; Pape & Dingman, 2011) have highlighted the high rates of perioperative medication errors and adverse drug events in the operating room with one study finding that as many as one in 20 medication administrations included an error or adverse drug event (Nanji et al., 2016). There are many factors that contribute to this problem (Nanji, 2020) including time pressure, high-acuity nature of patient care in the Operating room (OR), medication label design, design of technology, and equipment and the design and layout of anesthesia workspaces. The anesthesia provider’s workspace is prone to interruptions, distractions, and interference which have been linked to errors in many different healthcare settings.
In operating rooms, the anesthesia workspace is often located near the head of the patient and anaesthesiologists perform a range of medication related tasks that include gathering information for medication preparation from visual displays and electronic medical records (EMRs), preparing medication supplies from a Pyxis machine/storage cabinet, administering anesthesia to patients, and recording and documenting medication. Anesthesia providers often perform multiple tasks simultaneously and switch between tasks frequently (Jurewicz et al., 2020). Monitoring a patient’s status while performing other tasks can be challenging, involving numerous movements and unsuitable rotations to different locations (Jurewicz et al., 2020; Seagull et al., 2004). This workspace is often limited and cluttered with movable and/or fixed equipment and is usually shared with other members of the surgical team (Jurewicz et al., 2020). For example, the clutter from cables in this crowded workspace can obstruct access to equipment and result in poor sightlines to the patient or to patient monitors. Inadequate lighting for anesthesia tasks can also contribute to medication errors (Fraind et al., 2002; Joseph et al., 2018; Martin et al., 2017; Orser et al., 2001; Rostenberg & Barach, 2012; Youn et al., 2015). Joseph and colleagues (2019) found that 30% of flow disruptions during surgery occurred in the anesthesia workspace and more than half were due to the layout. These disruptions may lead to errors, particularly in the performance of medication-related tasks that include medication preparation, administration, and documentation (Savoldelli et al., 2010). There is a need to design the anesthesia workspace to support medication-related tasks of the anesthesia providers.
Disruptions related to the physical environment range from those attributed to poor equipment adjacencies and ergonomics to loud noises and inadequate working areas for anesthesia providers (Bayramzadeh et al., 2018; Joseph et al., 2018). These physical environment factors can create latent conditions for medical errors, especially during critical medication-related tasks. The Anesthesia Patient Safety Foundation recommends implementing protocols, policies, and interventions to address potential distractions during anesthesia medication tasks and their impacts on patient safety in ORs (van Pelt & Weinger, 2017). These recommendations include developing policies, understanding the environment and the interpersonal dynamics of the OR, and recognizing the clinician’s need for user interfaces during care delivery. However, there is a lack of clear evidence-based guidance for designing anesthesia workspaces in operating rooms. Evidence-based design guidelines are needed to support the design of anesthesia workspaces in the OR to support the work of anesthesia providers.
While the existing literature (Joseph et al., 2021; Jurewicz et al., 2020) has addressed some key characteristics of the operating room, such as flexibility, adaptability, movement, and flow, the impact of surgical table configurations, and the integration of technologies on flow disruption and movement patterns, the present study recognizes the need to develop design guidelines to specifically support the design of the anesthesia workspace. Research shows that different equipment arrays in the anesthesia workspace can impact the provider’s focus on patients, visual displays, and tasks. Therefore, guidelines focusing on task demands and ergonomic issues can help improve workflow efficiencies and patient outcomes.
Objectives
The objective of the present study is to develop evidence-based design guidelines for the anesthesia workspace to support safe anesthesia medication tasks in the OR and to reduce disruptions and failures during the preparation, administration, and recording of anesthesia medication. The research team developed a set of guidelines/recommendations to address multiple evidence-based design goals. These guidelines incorporate key considerations related to the anesthesia providers’ tasks, processes, and interaction with equipment or people in their workspace. The purpose of these guidelines is to encourage the design and management of anesthesia workspace to support safe anesthesia medication selection and delivery during surgical procedures. The present study serves as a means for informing the overall design process as well as future design evaluations.
Method
The evidence-based anesthesia workspace guidelines were developed based on a review of the literature supported by the observation of anesthesia medication tasks during surgical procedures. The guidelines were then reviewed and vetted by anesthesia providers and human factors experts with expertise in anesthesia work.
Literature Review Process
To examine how the design of the anesthesia workspace and equipment layout impacted anesthesia work—specifically, medication tasks—the team conducted a narrative literature review. Key words used to identify articles include anesthesia (anesthetic and anesthesiology), ergonomics (cognitive ergonomics, information load, situational awareness visibility, response time, visual and auditory alarms, and noise), physical ergonomics (subcategories of interface, awkwardness, positioning, placement, human factors, occupational risk/health, displays, lighting), equipment ergonomic design, workspace (workspace ergonomics, layout, and design), workflow, medication tasks (induction, administration, preparation, and task analysis), monitoring, workload, documentation, operating room, surgical team members, operating room layout, operating room equipment, equipment (anesthesia equipment and supplies, anesthesia machine, anesthesia novel equipment, anesthesia monitoring equipment, Pyxis and medication drawers, anesthesia medication cart, anesthesia documentation, and surgical table), and patient safety (disruption, interruption, distraction, fatigue/burnout, infection control, and adverse events). The search was conducted primarily using Google Scholar through the University Library. Secondary databases included PubMed, Science Direct, and the Center for Health Design Knowledge Repository.
Abstracts of identified articles were first reviewed and categorized (based on their relevance) into equipment (anesthesia machine, monitoring, novel equipment, recording station, and surgical tables), layout and design (anesthesia zone dimensions and configuration), ergonomics, workflow, errors, and flow disruptions. The literature review focused on understanding how the design of the physical environment and equipment configuration in the anesthesia workspace impacted the work of anesthesia providers. A total of 239 articles were identified for review; after eliminating duplicates and screening the article abstracts, 31 relevant studies were identified for full-text review.
Narrative summaries of the articles were drafted into a table, which included their abstracts, research questions or hypotheses, the country where the study occurred, sample (size and subject role), surgery types (if mentioned), research designs (experimental, correlational, survey, case study, and observational), data collection methods (interview, surveys, etc.), environmental variables (the aspect[s] of the built environment as measured/described), environmental attributes (i.e., height, width, type, visual control related to the environmental variables), environmental metrics, other variables (nonenvironmental) and their relevant metrics, outcome variables (e.g., error, disruption, discomfort), outcome metrics (e.g., number of bumps), reliability, valuable points, and further resources.
Observation Process
To gain understanding of the anesthesia providers workflow and challenges, a facility tour visit was conducted to observe and interview anesthesiologists. An observation instrument was developed after screening the existing tools (Antoniadis at al., 2014; Arfanis & Smith, 2012; Broom et al., 2011; Campbell et al., 2012; Jothiraj et al., 2013; Seelandt et al., 2014; Weinger et al., 1994) to understand anesthesia workflow. The observation tool allowed the team to understand patterns of medication tasks and equipment usage in the anesthesia workspace. The research team observed 10 videos of different surgical procedures, focusing on the activities of the anesthesia providers. The videos came from the Medical University of South Carolina and were captured in the OR by four cameras, one in each corner of the operating room so that no part of the OR was hidden. The video data collection was approved by the MUSC IRB (IRB # Pro00082024). The recordings began when the patient entered the OR and stopped when the patient was removed to recovery. These data have been previously used to address research questions related to OR design and the likelihood of surgical safety events (Joseph et al., 2019; Joseph et al., 2021; Jurewicz et al., 2020; Neyens et al., 2019).
This study focused on the intra-operative and postoperative phases of the procedures. Specifically, researchers observed four main categories of medication tasks performed by anesthesia providers—medication preparation, medication administration, recording/documenting, and seeking/gathering information. Additionally, researchers identified the equipment with which anesthesia providers interacted. Researchers took descriptive notes and screenshots of specific challenges experienced by anesthesia providers while performing medication tasks. The research team created sketches and diagrams based on notes and screenshots to document the observed challenges.
Guideline Development and Validation
Once a preliminary list of physical environment challenges and design recommendations was developed from an examination of the relevant literature and observations, the key findings were synthesized into a set of design guidelines. Each guideline included a rationale that explained why it was important and how to achieve it through design.
The design guidelines were then vetted by content experts (anesthesia providers and researchers with human factor expertise) to obtain feedback on the relevance and content of the guidelines. An online survey was administered to five anesthesiologists and human factor experts. The aim was to identify if each specific guideline addressed a key issue/problem for anesthesia providers. The content experts were also asked to provide specific changes to the wording of the guideline and related content and if there were additional issues related to the anesthesia workspace design not addressed by the guidelines.
After reviewing the comments from the content experts, the team implemented general and targeted revisions and developed a final set of seven guidelines for anesthesia workspace design.
Results
Current standard anesthesia workspace layouts result in anesthesia providers performing their tasks in dispersed locations, which can lead to increased head and body rotation and movements. These movements can cause disruptions, fatigue, and musculoskeletal and safety issues (Guy et al., 2011). Because anesthesia work surfaces are often cluttered, which may lead to contamination and errors, it is necessary to ensure that they have an organized area in which to perform their tasks. Moreover, due to suboptimal positioning and equipment accessibility, many anesthesia providers are also challenged by personnel moving into and through their workspace, causing distractions and contamination.
The observations and literature findings were supported by vetting process and channeled into seven evidence-based design guidelines, which categorize the problems and direct the development of potential design solutions while considering tradeoffs between different recommendations.
Locate Critical Tasks Within a Primary Field of Vision
The anesthesia workspace should facilitate the need to cover a wide angle of viewing, working at multiple locations and task-switching, enabling anesthesia providers to optimize task performance and overall situational awareness during all phases of surgical procedures (Grissinger, 2012).
Why it is important
Anesthesia providers need to monitor the patient’s status while performing other tasks such as medication preparation, medication administration, and documentation. The literature identifies visual attention and limited distractions as priorities for anesthesiologists (Seagull et al., 2004), who often perform simultaneous tasks with conflicting task demands, that is, monitoring patients while watching displays and managing anesthesia machines. The extent to which anesthesiologists deviate from monitoring patients may be correlated with the dispersion of attention (Seagull et al., 2004). Their workspace can lead to unsuitable postures for reaching and monitoring and to the dispersion of attention during airway management tasks, such as adjusting ventilators, checking ventilator settings, and patients’ vital signs (Seagull et al., 2004). Surgical teams prefer lower height displays for better line of sight and reduced head and neck movements, preventing significant body repositioning and allowing for easy information retrieval during the phases of surgery (Bayramzadeh et al., 2018).
Anesthesia providers’ many tasks and dispersed locations call for a significant degree of body and head rotation (sometimes 270° horizontal and 120° vertical; Figure 1) and frequent movements that can result in distractions, fatigue, and loss of field of view (Jurewicz et al., 2020; Seagull et al., 2004). Anesthesia equipment is bulkier than before, often with longer breathing circuit tubing and located farther from the patient, leading to an increased degree of rotation and movement while working. This can distract the anesthesia provider from monitoring patients and impair their overall situational awareness (Grissinger, 2012; Guy et al., 2011).
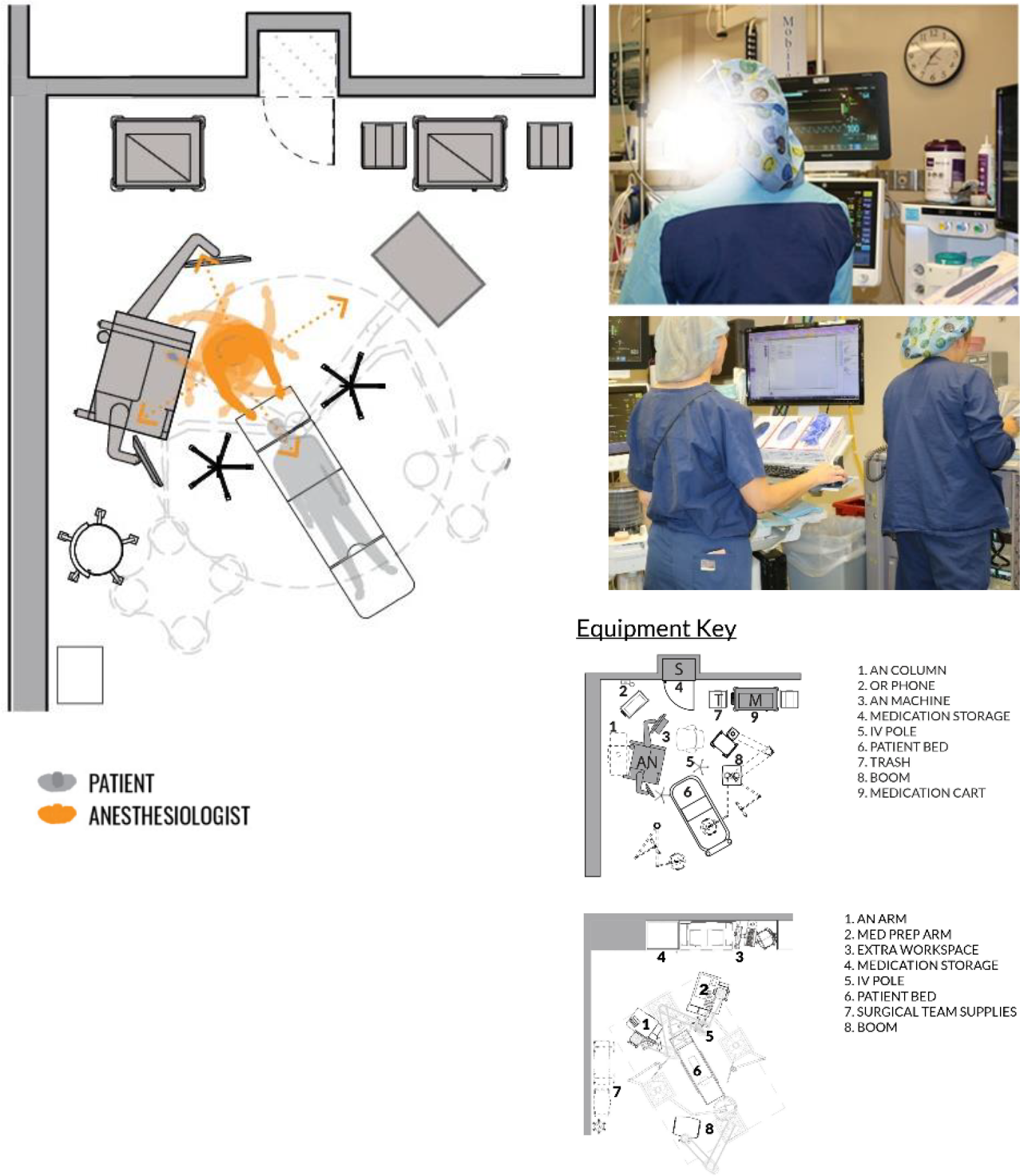
Observed head and body rotations of anesthesia providers.
How to achieve it
There are several design features, each identified in the literature, that may help to locate the anesthetists’ critical tasks within their primary field of vision. Among them are that the anesthesia equipment should integrate all visual displays, work surfaces, and data entry surfaces to provide clear views of the patient and surgical procedures from a single work position. Additionally, the height of work counters and supply areas should be set to maximize task efficiencies and product visibility (Grissinger, 2012). Anesthesia machines should also have adequate and functional work surfaces positioned close to the patient to minimize time away from medication preparation. What is more, the use of integrated surgical tables will reduce the rotational arc by incorporating anesthesia equipment under the table, over the ceiling, or beneath the floor (Ofek et al., 2006). Finally, OR designers should continue to explore improvements in design and technology to increase the focus and efficiency of operational tasks while maintaining a clear line of sight to all monitors (Sanderson et al., 2005).
Eliminate Travel Into and Through the Anesthesia Zone (for Other Staff)
The design of the anesthesia workstation should eliminate unnecessary staff travel into and through the anesthesia zone to eliminate safety risks, disruptions, accidental disconnections, and improve circulation and flow in the operating room (Figure 2).
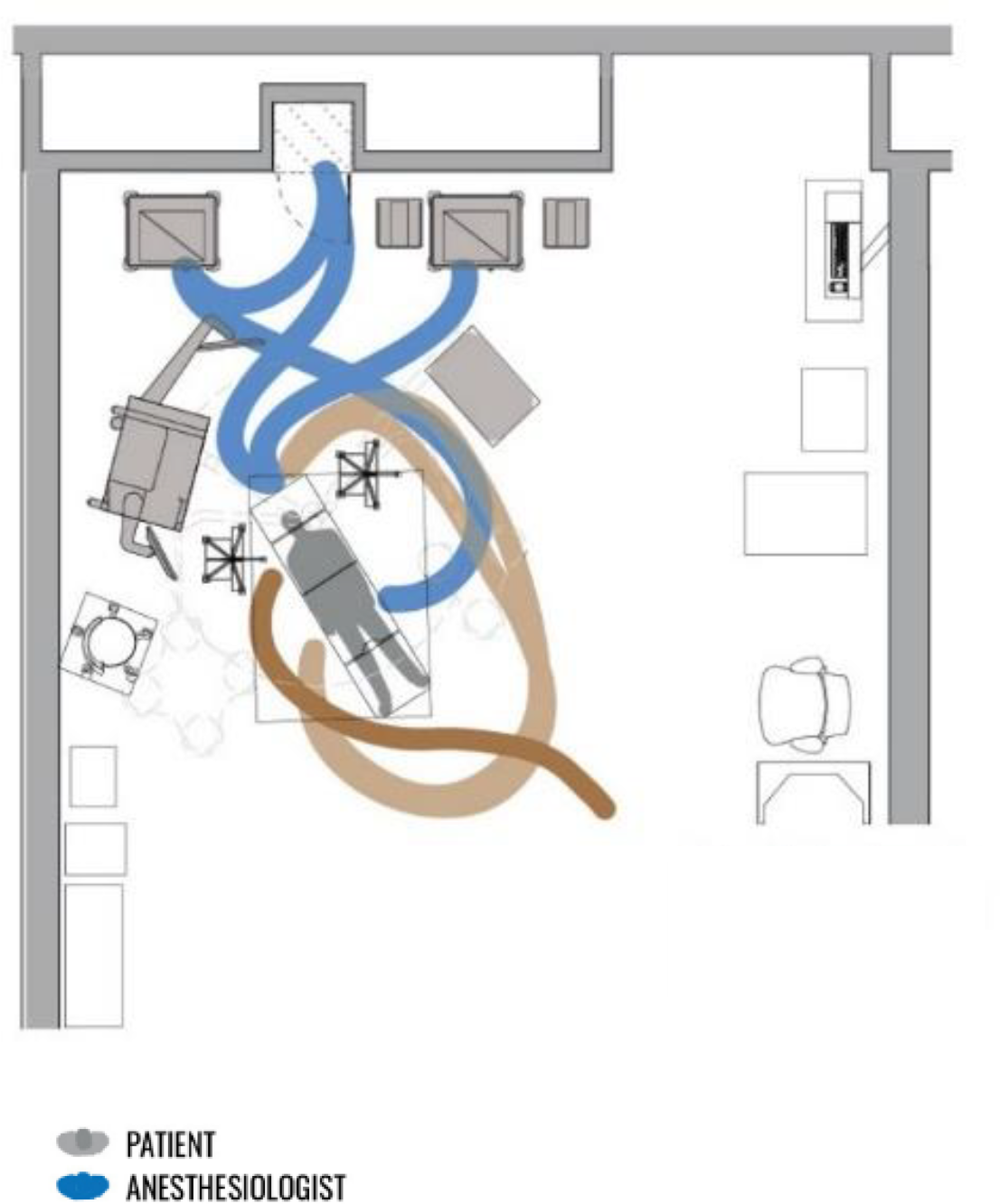
Incursions in the anesthesia workspace by other team members (brown).
Why it is important
The operating room’s configuration and obstructions in the OR can create situations where surgical team members must pass through the anesthesia zone to access supplies/medication, locate equipment, contact the anesthesia providers, or perform other tasks (Barach & Rostenberg, 2015; Bayramzadeh et al., 2018). High traffic and physical movement in the OR are positively correlated with the microbial load in different areas within the operating room, and the proximity of the zones to the door may influence the traffic level and bacterial count (Andersson et al., 2012; Taaffe et al., 2018). Still another study that investigated the link between OR traffic flow and air contamination in the vicinity of surgical wounds found a positive correlation between air quality and total traffic flow per operation (Andersson et al., 2012). Distractions in the OR can result from too many personnel in the anesthesia workspace, excessive movement during the surgical procedure, and conversations unrelated to the task at hand, all of which can raise the risk of accident or infection (Broom et al., 2011).
Placing nonanesthesia-related items in the anesthesia work zone and anesthesia-related items outside the anesthesia work zone increases the chance of distraction and task disruption due to moving into and through the anesthesia zone (Campbell et al., 2012; Koneczny, 2009).
Loud noises from dropping equipment, alarms, loud conversation, slamming bins or doors, and music (Broom et al., 2011) might decrease mental efficiency and short-term memory (Murthy et al., 1995).
How to achieve it
To reduce or eliminate travel by nonanesthesia staff into and through the anesthesia work zone, the design of the OR should include positioning the anesthesia work zone on the far side of the operating room, away from the patient, staff, and material points of entry. The OR should also be organized so that high-traffic areas lie outside and away from the surgical field and anesthesia zone. Minimizing movements within the operating room should reduce the risk of contamination. This can be achieved by incorporating built-in recessed storage and movable workstations, moving traffic attractors away from the surgical field (Taaffe et al., 2018), improving visibility for team members by strategically placing cameras and projection systems, and positioning doors to keep traffic away from sterile areas and anesthesia work zones.
Identify and Demarcate a Distinct Anesthesia Zone With Adequate Space for the Anesthesia Provider
The anesthesia workspace should be located in a demarcated and distinct anesthesia zone with adequate space and the required equipment and storage to perform tasks effectively without requiring unnecessary movement in the OR.
Why it is important
The literature reveals the need for an optimal distance between the anesthesia area and the OR doors to decrease or prevent task disruptions by other surgical personnel who walk in and out of the OR (Figure 3; Bayramzadeh et al., 2018). Also, the anesthesia zone should be clearly defined to discourage its use for circulation by other team members (Barach & Rostenberg, 2015). Adequate square footage is necessary to support current and future equipment, the anesthesia team, and sufficient space for easy movement. The configuration of the equipment and location of the anesthesia zone should ensure that staff move within their functional work areas without accessing other parts of the OR (such as the anesthesia zone).
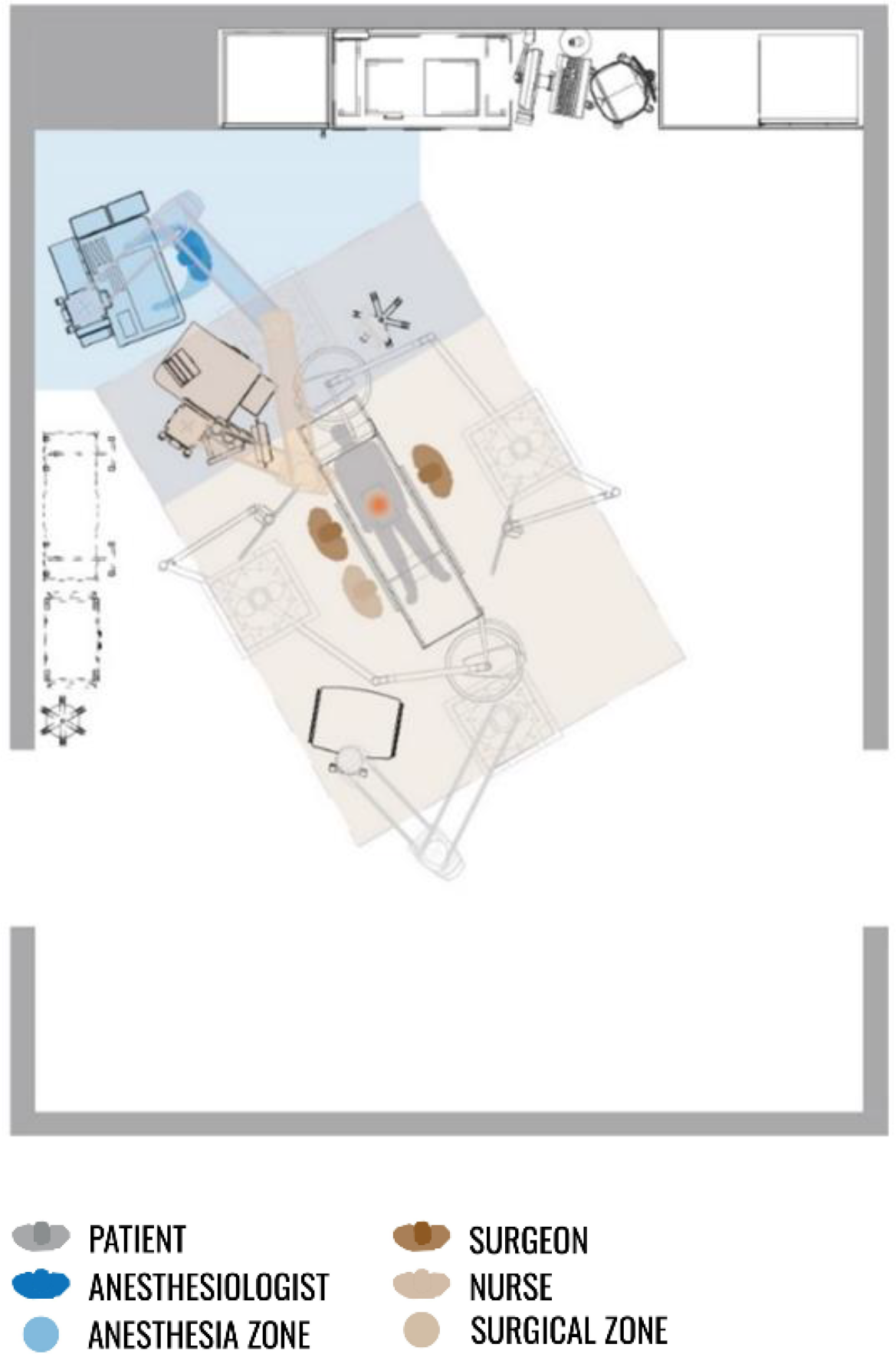
The anesthesia zone in the corner of the operating room, away from all door openings.
How to achieve it
The following design features can help identify and demarcate a clear anesthesia zone with adequate space for the anesthesia provider. Among these are placing the anesthesia zone in the corner of the operating room, away from doors (Bayramzadeh et al., 2018; Figure 4), providing adequate space for storage cabinets, anesthesia cart, and printer for specimen labeling (Bayramzadeh et al., 2018), using boom-mounted equipment to free up floor space and increase flexibility, and having adequate square footage to support an optimal workflow for anesthesia providers. There should also be sufficient flexibility in the OR design to accommodate new equipment and additional staff while minimizing movement conflicts between anesthesia providers and team members.
Optimize the Ability to Reposition/Reconfigure the Anesthesia Workspace
The design of the anesthesia workspace should facilitate the optimal repositioning/reconfiguring of the anesthesia workspace to facilitate workflow, improve ergonomics, and accommodate the changing needs in the OR over time and to reduce the risk of environmental hazards (Figure 4).
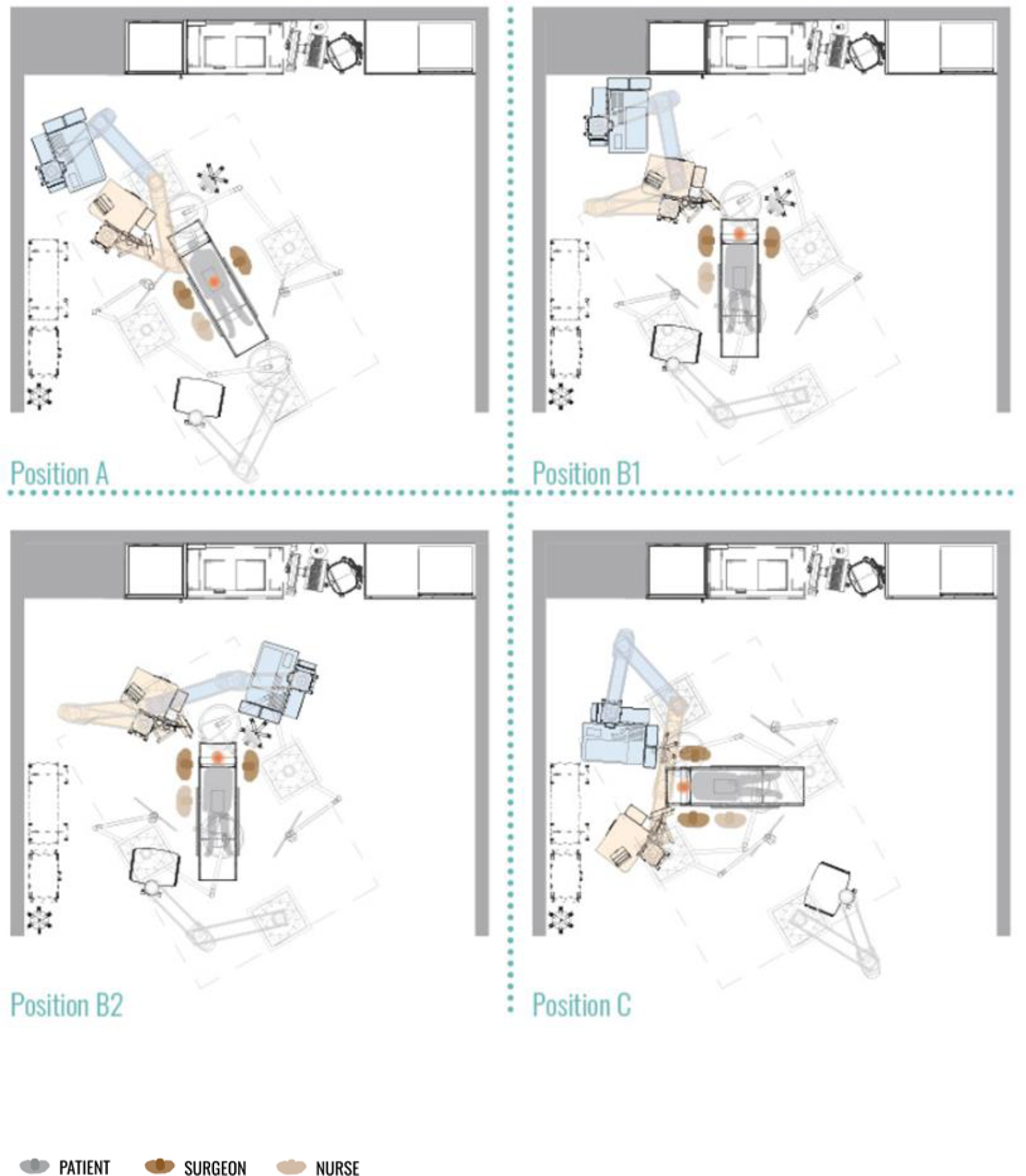
Repositioning of the anesthesia equipment with the patient and surgical table to facilitate workflow.
Why it is important
Continuous reconfiguring/repositioning of the anesthesia workspace can lead to providers temporarily disengaging from their primary medical tasks, which increases the risk of missing potentially vital cues of the patient’s status (Boquet et al., 2017). Frequent repositioning of equipment during surgery can lead to stretching and disconnecting tubes (Boquet et al., 2017).
Other challenges include difficulty in reaching for equipment or lacking a clear view due to equipment misplacements, frequent cable and line handling (Held & Krueger, 2000), and frequent cable connecting or reconnecting (Held et al., 1996). To improve ease of use and efficiency (Grissinger, 2012), recommendations include flexible equipment positioning (Held & Krueger, 2000) and using adjustable fixtures (e.g., screens, counters, and task lights).
The anesthesia workspace needs to support multiple anesthesia providers. Different ergonomic requirements mean that equipment can be adjusted according to the height and preferred working positions of the anesthetists. Sometimes, due to the height of the poles, shorter anesthesia providers were observed standing on wheeled chairs to hang intravenous fluids (Fraind et al., 2002). Undesirable positioning and configuration of the anesthesia workspace can force anesthesiologists to use other sides of the surgical table to conduct anesthesia activities instead of the head of the surgical table.
How to achieve it
To optimize the anesthesia workspace, bulky equipment should use ceiling-mounted or wheeled anesthesia machines in large ORs and/or for complicated procedures. Available space should facilitate the repositioning/reconfiguring of the OR setup to permit the rotation/movement of the anesthesia equipment with the patient and surgical table (Matern & Koneczny, 2007). Plug-and-play design concepts for various equipment will reduce the number of discrete equipment items, connecting cords, tubes, and cables. The operating table should be adjustable for the user’s optimal positioning and convenience (Wauben et al., 2006) and, where possible, equipment should be integrated for easy adjustment and access (Matern & Koneczny, 2007).
Minimize Clutter From Equipment
The anesthesia workstation should have minimal clutter from equipment to reduce environmental hazards and disruptions and minimize contamination in the anesthesia workplace (Figure 5).
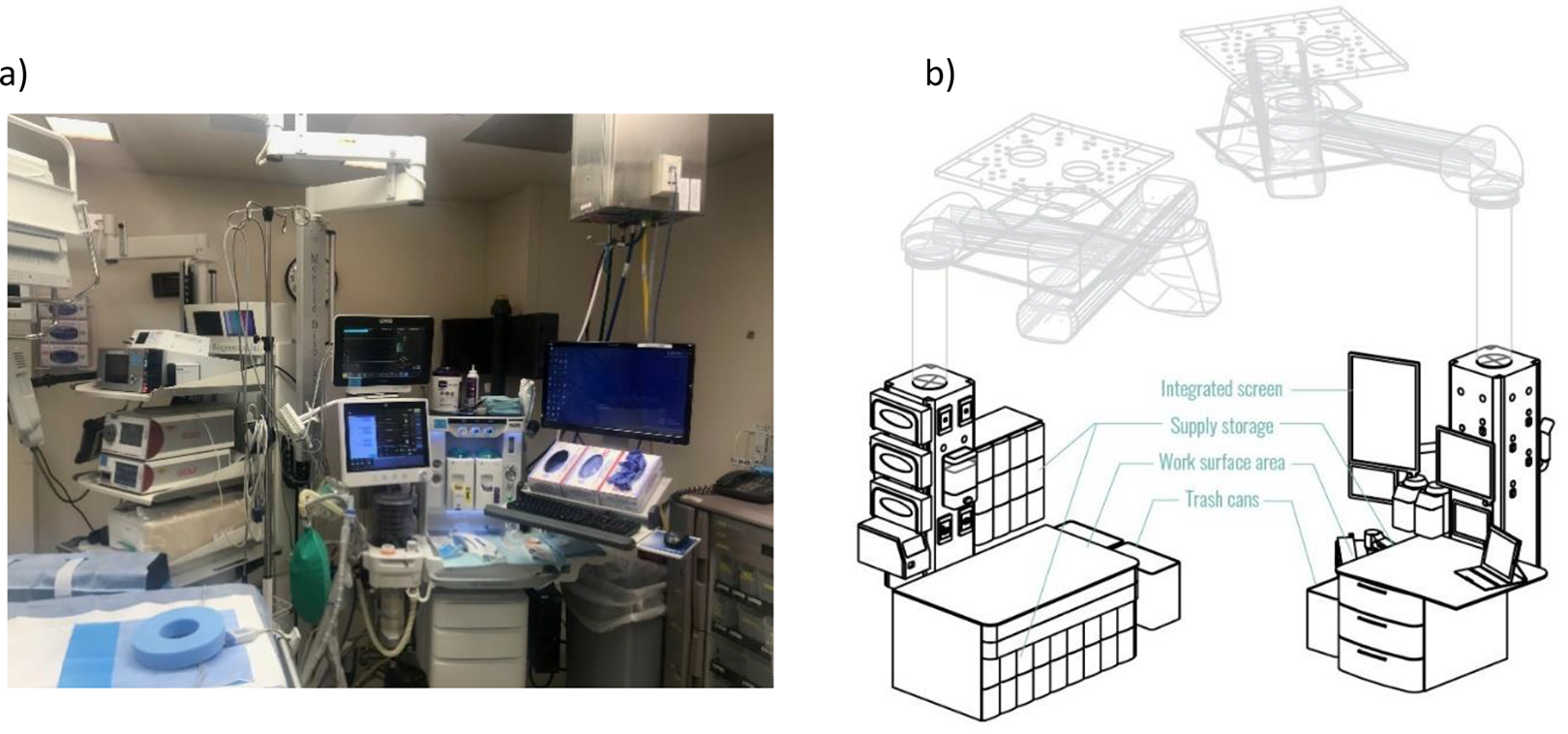
(a) Observed anesthesia work zone with cluttered equipment and supplies and (b) medication preparation and administration boom arms with integrated equipment and supplies.
Why it is important
The anesthesia zone is a small space prone to clutter due to the presence of equipment and multiple anesthesia providers at the head of the surgical table (Fraind et al., 2002). This clutter, which includes cables and tubing attached to the equipment or patient, can present physical barriers that lead to patient safety issues such as accidental disconnections, disruptions, and trip hazards, especially in emergencies (Boquet et al., 2017; Brogmus et al., 2007; Fraind et al., 2002; Held & Krueger, 2000; Held et al., 1996; Matern & Koneczny, 2007; Ofek et al., 2006). A study by Fraind et al. (2002) reported several challenges with intravenous tubing during cardiac cases where the anesthesiologist either slipped or had to lift the tubes over the head to traverse them. The anesthesiologists or other clinicians were observed hitting the intravenous poles or passing the tubes over their heads when they needed to move. When transporting a patient in and out of the OR, anesthesia providers were observed on some occasions bumping the intravenous pole, the overhead lights, or the door. Additionally, not separating used or contaminated and unused drug-filled syringes were also reported as well as unnecessary items were put on anesthesia work surfaces during the surgery’s administration phase (Fraind et al., 2002).
How to achieve it
To create a safe, well-organized and clutter-free workspace for anesthesia-related tasks, all non-essential or non-anesthesia-related equipment/supplies in and around the anesthesia workspace should be eliminated. Where possible, wireless equipment and sensors should be used to reduce the number of cabled connections (Koeny et al., 2012). If a ceiling column or movable boom-mounted anesthesia machine is used to supply the anesthesia gas, the column can also hide electrical and data utilities to eliminate cables and tubes running to the floor and wall outlets. A built-in, recessed, well-organized anesthesia storage and/or mobile storage/carts with easy access will eliminate nonessential fixed horizontal surfaces. Also recommended is the use of integrated display technology for a single workstation (Jurewicz et al., 2021).
Provide Adequate and Appropriately Positioned Surfaces for Medication Preparation and Administration
Provide adequate space for critical tasks such as medication preparation and administration. These tasks can be performed safely without disruption or contamination, while at the same time allowing the anesthesia provider to maintain a visual connection to the patient.
Why it is important
Horizontal anesthesia work surfaces (usually on the anesthesia machine and medication cart) are often cluttered with extra supply packages, which may block the visibility of critical items such as syringes and airway supplies. This contributes to delays in medication administration tasks and poses potential risks to the patient (Fraind et al., 2002). Additionally, anesthesia medication preparation and administration surfaces are prone to contamination (Martin et al., 2017). Cleaning and disinfecting a cluttered anesthesia zone can be challenging, leading to contaminated work surfaces. Also, the presence of bulky equipment around the surgical table limits the usable horizontal workspace and the placing of displays and monitors in undesired locations, such as behind the anesthesia providers (Held et al., 1996).
Bayramzadeh et al. (2018) reported concerns by anesthetists about a lack of adequate and easily accessible storage, as well as items cluttering the workspace. Additionally, the inappropriate location of storage can cause difficulties with opening cabinet doors in confined spaces. The same study suggests that placing the storage in front of the monitors is less intrusive and provides better access for anesthesiologists and other OR team members such as circulating nurses (CNs) who may need access to it (Bayramzadeh et al., 2018). The authors do not recommend placing the storage either adjacent to or behind the monitors.
Nonstandardized anesthesia workspace and medication storage equipment can contribute to confusion and potential errors in the OR (Shultz et al., 2010). Storing medication on cluttered surfaces can lead to difficulties in differentiating and lead to dispensing errors. U.S. Pharmacopeia recommends uncluttered medication storage with at least 1 inch of space between each medication. Additionally, optimal counter height to ensure the visibility of items/supplies is advised (Grissinger, 2012).
How to achieve it
To provide adequate and appropriately positioned surfaces for medication preparation and administration, the design of the OR should integrate a dedicated horizontal anesthesia workspace integrated with critical equipment while giving the anesthesia provider clear sightlines to patient monitoring devices. The workflow of medication preparation tasks should avoid contact between medication syringes and “unclean” anesthesia workspace surfaces. To control infection, the number of intravenous access points and separate “clean” and “dirty” anesthesia workspaces (medication preparation and administration spaces) should be minimized (Martin et al., 2017): The use of a “one-way” workflow—moving syringes in one direction from the medication drawer to a specially designed bracket and then to the “active” workspace—will help to achieve this goal. Moreover, the syringe bracket, together with the “one-way” medication preparation workflow, can reduce cognitive load, reduce the risk of syringe swaps, improve medication availability, and safeguard against syringe contamination from other anesthesia workspace items and surfaces (Long et al., 2019).
Optimize Task and Surface Lighting
The medication preparation areas, whether on the top of the anesthesia workstation or the medication drawer, should have sufficient task and surface lighting to improve the visibility necessary for medication-related activities.
Why it is important
To provide a better view of the procedure on screen, operating rooms are often dimly lit (e.g., laparoscopic surgeries). Low lighting levels, however, can be problematic for anesthesia providers during medication-related tasks, leading to medication errors, slips, trips, and falls (STFs; Youn et al., 2015). Surface lighting for medication preparation should not create distractions for other surgical team members (Martin et al., 2017; Orser et al., 2001).
Poor lighting can lead to poor attachment of tubing. The operating room, therefore, needs specialized lighting for the surgical site and ambient lighting for the surrounding space (Joseph et al., 2018; Rostenberg & Barach, 2012).
How to achieve it
To optimize task and surface lighting in the OR, dark areas should have supplemental lighting to ensure that the anesthesia provider has adequate illumination for medication preparation, administration tasks, and safe movement (Grissinger, 2012). Supplementary lighting is recommended for darker areas where anesthesiologists work (Youn, 2015). Lights should be optimally positioned to prevent glare on computer monitors (Grissinger, 2012). To prevent visual fatigue, brighter lighting is recommended (Grissinger, 2012).
Offset ceiling supports in complex operating rooms, such as cardiovascular hybrid rooms, should be used to prevent shadowing from bulky equipment. The ceiling surface should be used for ambient illumination (Rostenberg & Barach, 2012). Adjustable fixtures for tasks, counters, and screens to promote safety and visibility should be used (Grissinger, 2012). The OR design should also provide an unobstructed view of the floor and adequate lighting for walking paths during the various stages of surgery to minimize the risk of STFs (Brogmus et al., 2007).
Discussion
In this study, we collected data through literature review and observations and developed seven design guidelines using expert review. These design guidelines may help reduce or prevent failures while performing anesthesia medication tasks and also help lessen the physical and cognitive demands on anesthesia providers in the operating room. The design of the anesthesia workspace in the OR represents a unique challenge due to limited space, complex and bulky equipment, and the size of the surgical and anesthesia teams. These design guidelines are not prescriptive but provide guidance for developing creative design solutions that directly address the task demands and ergonomic challenges of anesthesia providers within a complex work system. The present study recognizes that workflow challenges in the OR are complex, sometimes overlap, and may not fit perfectly into one design guideline. Therefore, guideline boundaries sometimes blur.
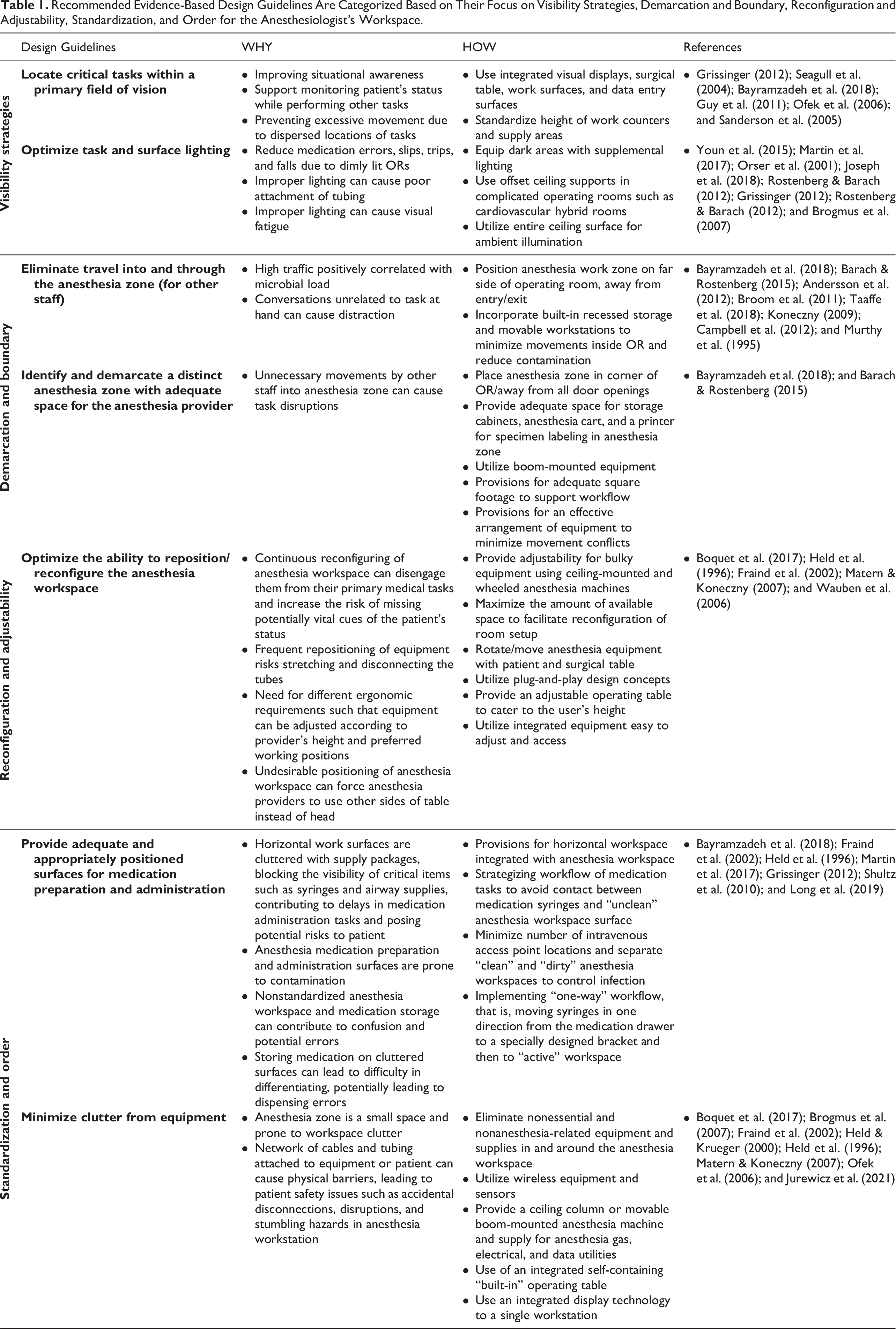
An alternative way to categorize these recommendations would be to say whether they focus on visibility, demarcation and boundary, reconfiguration and flexibility, standardization, orderliness, and adequacy of space for the anesthesiologist’s workspace (Table 1). While the design guidelines are based on the literature, Table 1 simplifies them into an evidence-based, user-friendly environmental design tool that focuses on Why and How for practitioners.
Recommended Evidence-Based Design Guidelines Are Categorized Based on Their Focus on Visibility Strategies, Demarcation and Boundary, Reconfiguration and Adjustability, Standardization, and Order for the Anesthesiologist’s Workspace.
Visibility Strategies
In this study, we developed strategies to maximize visibility for performing different tasks by locating equipment strategically and redesigning the anesthesia equipment to provide clear views of the patient and surgical procedure. Locating critical tasks within the anesthesiologist’s field of view will improve situational awareness, which is vital for anesthesia providers. Placing critical tasks within their line of sight should reduce excessive movements and unnecessary rotations (Bayramzadeh et al., 2018; Grissinger, 2012; Guy et al., 2011; Ofek et al., 2006; Sanderson et al., 2005; Seagull et al., 2004).
On the other hand, the anesthesia workspace should optimize task performance by enabling task switching between multiple locations while allowing for a wide angle of viewing (Grissinger, 2012).
Demarcation and Boundary
Demarcating a distinct anesthesia zone may help to eliminate the excessive travels for other staff or visiting observers that can cause distraction and task disruption for anesthesia providers. Therefore, arranging the OR so that the anesthesia work zone is away from entry/exit points can reduce or eliminate movement conflicts (Barach & Rostenberg, 2015; Bayramzadeh et al., 2018). However, a well-placed camera was noted to elevate such issues. On the other hand, a high traffic can be positively correlated with microbial load (Andersson et al., 2012; Taaffe et al., 2018); hence, the optimal placement of equipment, including movable workstations, should support the OR’s general workflow, reduce movements, and minimize the risk of contamination.
Reconfiguration and Adjustability
This study recommends optimizing the ability to reposition/reconfigure the anesthesia workspace. Continuous reconfiguring of anesthesia workspace can disengage them from their primary medical tasks (Boquet et al., 2017), therefore adjustable operating equipment is suggested, so that reconfiguring or repositioning of the equipment can be unnecessary.
For all equipment, adjustable or fixed, it may be necessary to take into account the specific ergonomic requirements and anthropometric measurements unique to a particular OR.
Standardization and Order
While adjustability of operating equipment is recommended, standardizing anesthesia workspace may provide the anesthesiologist with clear sightlines to all monitoring devices.
Additionally, adequate and appropriately positioned surfaces for medication storage can reduce workspace clutter in small anesthesia spaces.
Implementing a “clean” and “dirty” anesthesia workspace strategy may reduce the risk of infection (Martin et al., 2017).
Limitations
The findings of this study are limited by the research design, as well as the existing research into the design and equipment layout of the anesthesia workspace. Although the findings of this study may be applicable to a variety of operating rooms, future studies may improve some of the current limitations. The observations were limited to a single OR and it seems likely that other OR’s might afford opportunities to observe additional problems. The methodology limitations include lack of critical appraisal of the literature, sampling strategy, and analysis approach for observations. This study didn’t use a critical review tool to appraise the strength of the included research. Although, the sampling and analysis strategy for observations were limited. Therefore, we recognize the need for using methodologically rigorous literature review and observational methods that were validated in previous research. Finally, the vetting process suffered from limited numbers of the participants who may not fully represent their colleagues’ view on the challenges and the developed guidelines. Nevertheless, our results highlight the key findings and challenges concerning the anesthesia workspace design. These findings should help to improve the safety and efficiency of the anesthesia work area in the operating room.
Conclusion
This study investigated how the design of the anesthesia workspace can enhance task efficiency, ergonomics, patient safety, and the workflow for the surgical team. The study finds many areas for improving the design of ORs and recommends seven evidence-based design guidelines to assist the creation of new or remodeled ORs to support anesthesia delivery. Improvements to the anesthesia work area will call for the contribution and cooperation of the entire surgical team.
Implications for Practice
Design practitioners and researchers can use the guidelines to integrate ergonomics into the OR design, maximize visibility for performing different tasks, introduce adjustable operating equipment to accommodate the operator’s height, and integrate equipment for ease of use.
The anesthesia workspace is a complex area, the design of which requires a comprehensive understanding of the tasks performed by anesthesia providers and their equipment.
A multidisciplinary team of designers, human factor specialists, and anesthesia providers can effectively identify key work system challenges and develop solutions to address task demands and ergonomic challenges.
The seven evidence-based operating room design guidelines will support an evidence-based design process focused on improving the efficiency, ergonomics, and safety of the surgical team and patients.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231190646 - Anesthesia Workspaces for Safe Medication Practices: Design Guidelines
Supplemental Material, sj-pdf-1-her-10.1177_19375867231190646 for Anesthesia Workspaces for Safe Medication Practices: Design Guidelines by Soheyla MohammadiGorji, Anjali Joseph, Sahar Mihandoust, Seyedmohammad Ahmadshahi, David Allison, Ken Catchpole, David Neyens and James H. Abernathy in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-2-her-10.1177_19375867231190646 - Anesthesia Workspaces for Safe Medication Practices: Design Guidelines
Supplemental Material, sj-pdf-2-her-10.1177_19375867231190646 for Anesthesia Workspaces for Safe Medication Practices: Design Guidelines by Soheyla MohammadiGorji, Anjali Joseph, Sahar Mihandoust, Seyedmohammad Ahmadshahi, David Allison, Ken Catchpole, David Neyens and James H. Abernathy in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Agency for Healthcare Research and Quality.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.