
Abstract
This research explored the relationship between visibility and the level of security risks as perceived by nurses and physicians in emergency departments (EDs). Security in EDs has been reported as a major global concern, and visibility has been identified as a design factor impacting behavior. However, few previous studies have rigorously investigated the role of visibility in reduction of ED security risks with evidence-based design approach. There is a lot of significant questions about how visibility impacts the reduction of security issues in EDs.
Methods:
How visibility may influence ED security was explored via qualitative methods in five EDs using semi-structured one-on-one interviews with 17 clinical staff and 48 hr of field observations. The coding process for both interviews and observational notes followed the principles of naturalistic inquiry.
Results:
The findings suggest security risks can be decreased by improving visibility. Medical staff (registered nurses and physicians) felt more secure in the EDs with higher visibility.
Discussion:
This study provides a framework to identify preferable levels of visibility in EDs and proposes design strategies to minimize security issues. Registered nurses and physicians can improve their team’s sense of security by considering visibility throughout their daily practices.
Introduction
Healthcare facilities, especially emergency departments (EDs), are considered high-risk workplaces where staff are exposed to verbal and physical violence (Amaniyan et al., 2020; Anderson et al., 2010; Carayon et al., 2014; Pich et al., 2010; Pinar & Ucmak, 2011; Weyand et al., 2017). Some security risks can be minimized by the presence of security personnel, implementation of safety equipment, assigning safety policies/norms, training, and applying environmental design considerations (Forjuoh, 2014; Guinther et al., 2014; Levin et al., 1998). Patients’ fear of an unfamiliar situation/environment, being in pain, and waiting for a long time are contributing factors to aggression in healthcare delivery (Knowles et al., 2013; Lee & Cho, 2012).
A growing body of literature addresses security in EDs as a global issue (e.g. Anderson et al., 2010; Pinar & Ucmak, 2011; Levin et al., 1998; Gillespie et al., 2010; Razzak et al., 2019). Safety, security, and efficiency interact with each other in meaningful ways and are dependent on each other (Pati et al., 2016; Pati et al., 2014). Aggressive incidents can result in immediate disruption to the department, impact staff and patient safety, and distract staff members from their clinical duties (Carayon et al., 2014; Connellan et al., 2013; Guinther et al., 2014; Knowles et al., 2013; Koppenjan, 2001).
Many environmental factors, including access control, surveillance (natural and mechanical), visitor reception design, and levels of observation, can influence the measure of security in healthcare facilities (Carmel-Gilfilen, 2011; Feldbauer et al., 2008; Halpern et al., 2012; Gharaveis et al., 2018; McPhaul et al., 2008; MohammadiGorji Bosch et al., 2021). Physical design is considered one of the factors in managing ED security issues (Angland et al., 2014; Connellan et al., 2013; Gharaveis et al., 2018; Pati et al., 2014; Pati et al., 2016; McPhaul et al., 2008). This study defines security as the protection of people and property, as a subset of safety in healthcare delivery.
One operational factor that can directly and considerably impacted by physical design is “visibility” (Ahmadpour et al., 2021; Calleja & Forrest, 2011; Gharaveis et al., 2018; Gharaveis et al., 2020a; Gharaveis, Shepley, et al., 2019; Harvey & Pati, 2012; Lim et al., 2020; Lim & Zimring, 2020; Lu & Zimring, 2012; Pati et al., 2014). Visibility, as a design factor, is a combination of various components, such as proximity and the location of walls and partitions, which can be affected by wall arrangements (Gharaveis et al., 2019a; Harvey & Pati, 2012; Johanes & Atmodiwirjo, 2015).
Visibility, a characteristic of a layout, is defined by Trzpuc and Martin (2010), who studied medical–surgical units, as the provision of visual connectivity among different spaces. Johanes and Atmodiwirjo (2015) listed components of visibility on general inpatient units as visibility of the entrance area, visibility to and from nurse stations, and visibility of staff while they are walking on the unit. Prior studies identified visibility as a factor to ensure monitoring patient and staff conditions (Doede et al., 2018; Joseph & Rashid, 2007; Patterson et al., 2017; Zamani, 2019). Visibility in EDs also impacts many operational factors where critical resources need to be delivered quickly to stabilize patients (Calleja & Forrest, 2011; Gulrajani, 1995; Gordon et al., 2010; Gharaveis et al., 2018; Gharaveis et al., 2020b; Gharaveis, Shepley, et al., 2019; Pati et al., 2014; Pati et al., 2016; Zamani, 2019). This study defines general visibility as the level of visual connectivity among different points within a defined and closed environment. Targeted visibility, as a subset of visibility, is defined as visibility between two specific destinations.
Objective
This study is intended to investigate the nature of the relationship between reduction of security risks and configurations/layout of different EDs through the lens of qualitative research. Although research has been conducted separately exploring security and visibility, nothing similar to the current study (which extensively concentrated on security issues in multiple EDs within the same healthcare system) was available in the published literature. Also, there is a lot of unanswered questions about the nature of visibility in ED and how it impacts the reduction of security issues. For example, an exploratory study by Gharaveis et al. (2018) raises the question of the preferred security office locations in EDs. In another study, Zamani (2019) sets up the next step to investigate how visibility can potentially contribute to reduce the security risks that are associated with behavioral health patients. Additionally, this study applies the Naturalistic Inquiry method in which the physical environmental where we work, live, and play have different critical effects on many aspects of human life including spatial behavior and social organization formation. This new approach, in which a well-established qualitative method (the Naturalistic Inquiry), has been applied for a research question in healthcare settings and allows the experts to study the issue from human experience perspective in which the numbers cannot be easily assigned to. Furthermore, many aspects of this research topic cannot be explored outside of the real setting.
Method
This study used an exploratory approach to investigate the role of visibility in enhancing security from nurses’ and physicians’ perspectives, using semi-structured interviews and field observations at five subject sites. Having two independent methods to explore the research question helped the researchers to triangulate the findings. The intention to conduct field observations was to observe the events that participants were unable/unwilling to disclose. Also, the observations made the authors familiar with the environmental design attributes (visibility as a design factor) and security concerns (as a behavioral issue) in the ED. A pilot study was first conducted at Site 1, a community hospital within a healthcare system in the United States. Data collection and analysis were then improved and used in four additional EDs in hospitals from another healthcare system (Sites 2–5). All the subject sites were located in Southwest part of the United States, and Sites 2–5 were located in the same metropolitan area. The observation method was revised, and a few items were added to the interview questions. Data collection occurred in Fall 2016, and the study protocol was reviewed and approved by the corresponding author’s university-based Institutional Review Board.
Subjects
The inclusion criteria included 3 years of ED experience and 1 year at the current facility. Purposive sampling strategy was applied, and the researchers accepted highest qualified nurses and physicians in each site based on the inclusion criteria and number of different units they had been exposed to. At Site 1, three RNs and two ED physicians were selected per homogenous purposive sampling strategy. The same number of volunteers were selected from Sites 2–5, and initially 25 participants were informed. However, after achieving the saturation level, which is defined as the point where enough data have been collected and repeated ideas were addressed to draw conclusions (Lincoln & Guba, 1985), the lead author did not follow the same protocol and canceled the rest of the one-on-one interviews in Sites 2–5. Accordingly, 17 medical staff members in five facilities including two experienced RNs and one physician from Sites 2–5 were interviewed.
Sites
Site 1, with a race-track design and a central team station in the middle, was divided into two different connected wings with low visibility to each other. Sites 2–5 were comparable in terms of patient beds, annual visits, number of staff, and management systems but had very different floor plans (see Table 1).
The Ranks of Different Sites.
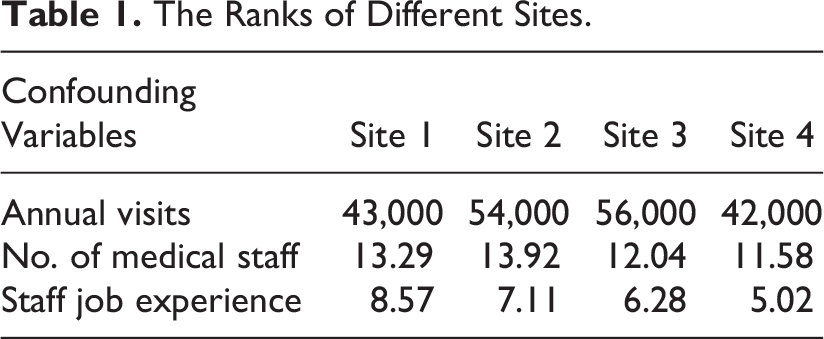
The layout of Site 2 was linear, and staff worked at three major workstations. Site 3 had a distributed plan and different pods accommodated medical and nonmedical staff. Site 4 had two pods, with one pod having a higher patient load than the other. Site 5 had one main area, with a nurse station at each end, while the trauma and fast-track areas were segregated from the main area (see Figure 1 for floor plans).
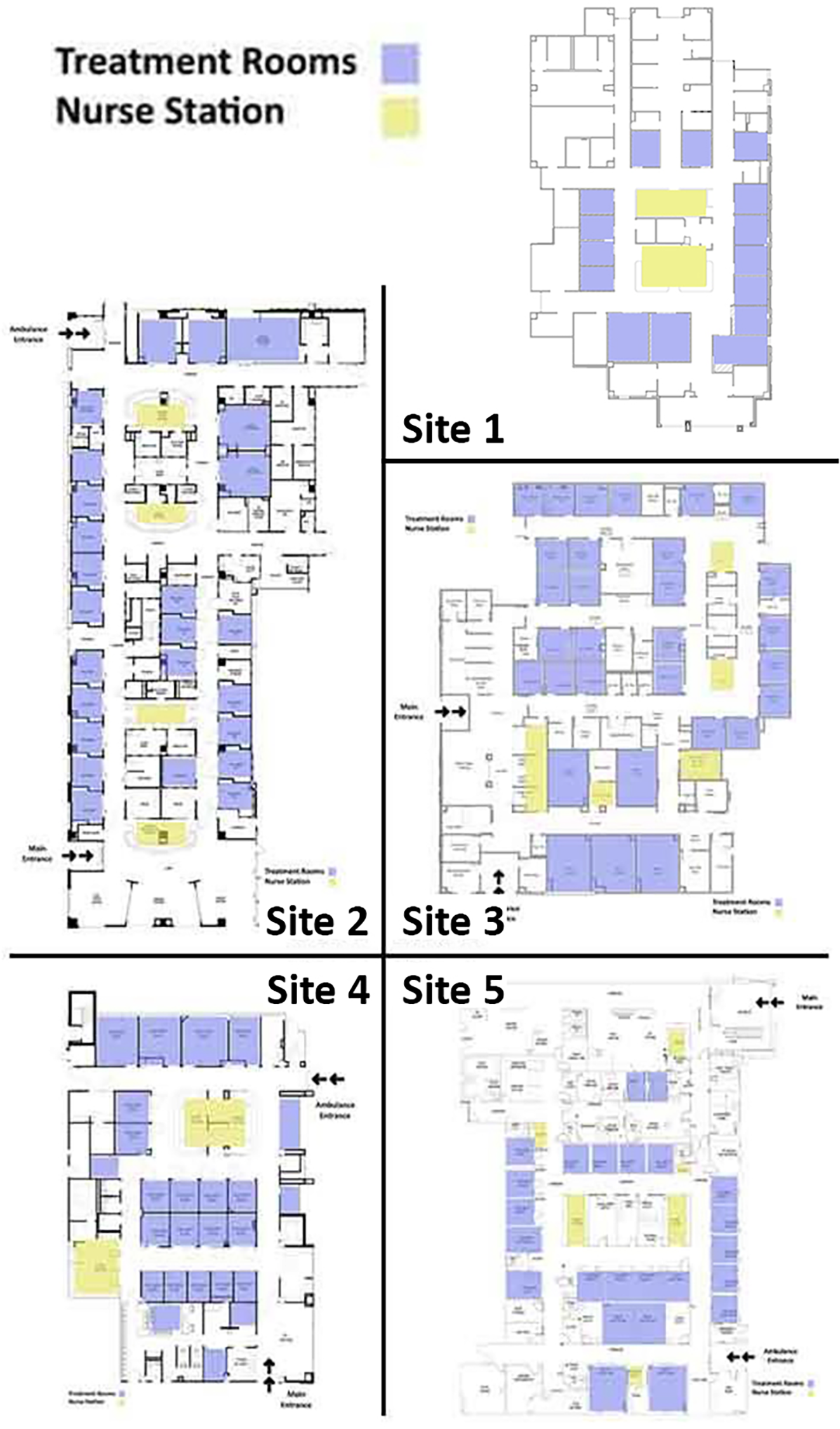
Five subject sites plans.
Data Collection
The interviews were conducted privately in staff (RN) break areas and physicians’ rooms. Each interview took approximately 20–30 min and was digitally recorded using the instrument: Olympus WS-803/802/801. The recordings were transcribed by a professional transcriber, then checked for accuracy by the lead author who also took notes about physical design and security issues during the interviews. The notes were typed for further analysis.
The ethnographic field observations were conducted by the lead author, and the follow-up questions were asked from the frontline staff to clarify the reasons of the events that were not clear to the observer. To assess field observation methods at Site 1, observations were conducted in two sessions (2 hr in the morning and 2 hr in the evening), with the observer stationed all around the unit. At Sites 2–5, 48 hr of observations (12 hr per site) took place in locations that afforded the greatest visibility of staff workstations, patient flow, and work traffic routes during the sites’ busiest hours based on each site’s historical database. The lead author moved to a new location for observation as soon as there was not any significant event based on the established observation framework from the lead author’s perspective. The busiest hours were targeted to allow the observer to witness more events. Notes from these discussions in observation hours were included in narratives. The observation process included making notes to document staff visibility, locations, interactions, and security events using methods framed by Spradley (1980) but did not include audio or video recordings. The notes were typed and checked twice for accuracy before the analysis, once by the lead author and once by one of the authors who was working at the facility.
Data Analysis
A similar approach was used to analyze the transcripts from Site 1 and Sites 2–5. The transcribed information was separated into data units, which is defined as a piece of information from an interview that can stand alone and make sense (Gharaveis et al., 2018). The data units were reviewed twice before coding. Related unit ideas were clustered together to identify themes, categories, and research memos that were entered into Microsoft Excel 2016. Different themes and subthemes were titled, and some influential ideas were reported as quotes which summarized multiple similar responses. Ideas that were not repeated (called nonsaturated data) were deleted (Emerson et al., 1995).
For the field observation, all notes were checked for accuracy before being coded. The process for both interviews and coding observational notes followed comparable principles of naturalistic inquiry, where similar ideas were summarized in brief terms or phrases and grouped together to develop the emerging codes (Lincoln & Guba, 1985). Two rounds of coding, starting with the domains of code identification, were pursued to report the subject locations, settings, acts, activities, actors in the setting, the situation of the actors in the setting, objects, time, goals of behaviors, and emotions/feelings as the framework for analysis and comparison (Lincoln & Guba, 1985).
After completing the domain analysis, which included reviewing the notes and observation records, a focused analysis was started. In this step, the details regarding security which had emerged in the initial step of domain analysis were further expanded. Next, a taxonomic analysis investigated the relationships between visibility and security risks. Finally, a componential analysis was conducted, in which different ideas and terms in the selected domains were differentiated and subdomains were identified.
Results
Observation
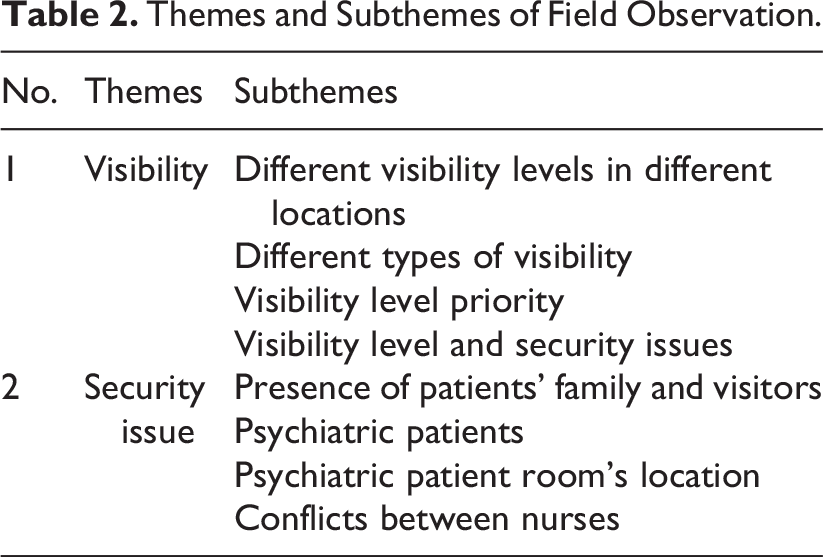
The observation results from Site 1 were compared with Sites 2–5 but were not included in the thematic analysis because of the limited number of observations at this pilot site. The observational results from Sites 2–5 were categorized into two major themes and seven overlapping subthemes relevant to the impact of visibility on security issues (see Table 2).
Themes and Subthemes of Field Observation.
Theme 1: Visibility
The positive impact of visibility on the security and safety of EDs is supported by the observation sessions. In departments with high levels of visibility, staff members quickly became aware of risky events and efficiently respond to them. In contrast, when sightlines were limited, problematic events might occur and further escalate. This main theme includes four subthemes that explore more detailed aspects of visibility in ED.
Subtheme 1: Different visibility levels in different locations
Visibility and accessibility were not distributed evenly across different sites. In Sites 3–5, the RNs and staff in fast-track areas were segregated with limited visual connectivity to others, which hampered notifying others in risky situations.
Subtheme 2: Different types of visibility
In EDs where staff spent time in all parts of the unit, general visibility had higher priority, since staff could notice risks and act upon them quickly. Targeted visibility was considered important in emergencies, when staff in the work stations needed to see their colleagues and security officers.
Subtheme 3: Visibility level priority
Sites differed on the levels of priority for room supervision. In the trauma and psychiatric rooms where supervision was considered important, providing visibility appeared to be a priority for RNs. Segregated fast-track areas, where staff usually had limited visibility to the rest of the ED, appeared to be a big concern. Placing security personnel in highly visible locations was reported as enhancing the perception of security.
Subtheme 4: Visibility level and security issues
One of the ED design considerations for security purposes was placing security officers at high-risk locations. When staff could visibly see an officer, it was thought to enhance nurse confidence when handling insecure events. Additionally, having visibility to the whole department when charting was considered very important.
Theme 2: Security issues
The observation sessions confirmed the vulnerability of RNs to security threats since they interfaced with patients and visitors more than physicians. Not surprisingly, the physicians who were interviewed and observed in this study had less patient exposure and fewer concerns regarding risky events. In Sites 2–5, the observations were able to identify five subthemes regarding latent security concerns.
Subtheme 1: The presence of a security officer
During the observation sessions, the presence of security staff was crucial in controlling and supervising the ED. Visibility, accessibility, and appropriate placement of security officers were considered by ED healthcare staff as paramount factors for quick response. In some distributed layouts, the security officers did rounds as dynamic observation, which was a useful strategy in alleviating aggression.
Subtheme 2: Psychiatric patients
Psychiatric patients, especially young adults, were perceived as a source of risk in most of the sites in addition to potentially interrupting department functions. In this study, it was observed that psychiatric patients were assigned one-on-one supervision by ED-based paramedics or technicians to increase security. In a few observed cases, a security officer became involved to control agitated patients.
Subtheme 3: Psychiatric patient room location
In most of the observed departments, the psychiatric patients’ rooms were located close to the main workstations, to facilitate supervision by nurses and other medical staff. This placement was preferred by staff, as it enabled them to respond to problems more quickly. However, in the case of two behavioral health patients’ aggression, the noise caused disruption to the function of the department.
Subtheme 4: Conflicts between nurses
The researcher observed one conflict between two nurses, since they could not find each other, and this required an intervention by the charge nurse to resolve the problem. The nurses’ conflict might have been minimized by enhanced visibility among nurses and others due to the nature of the conflict
Interviews
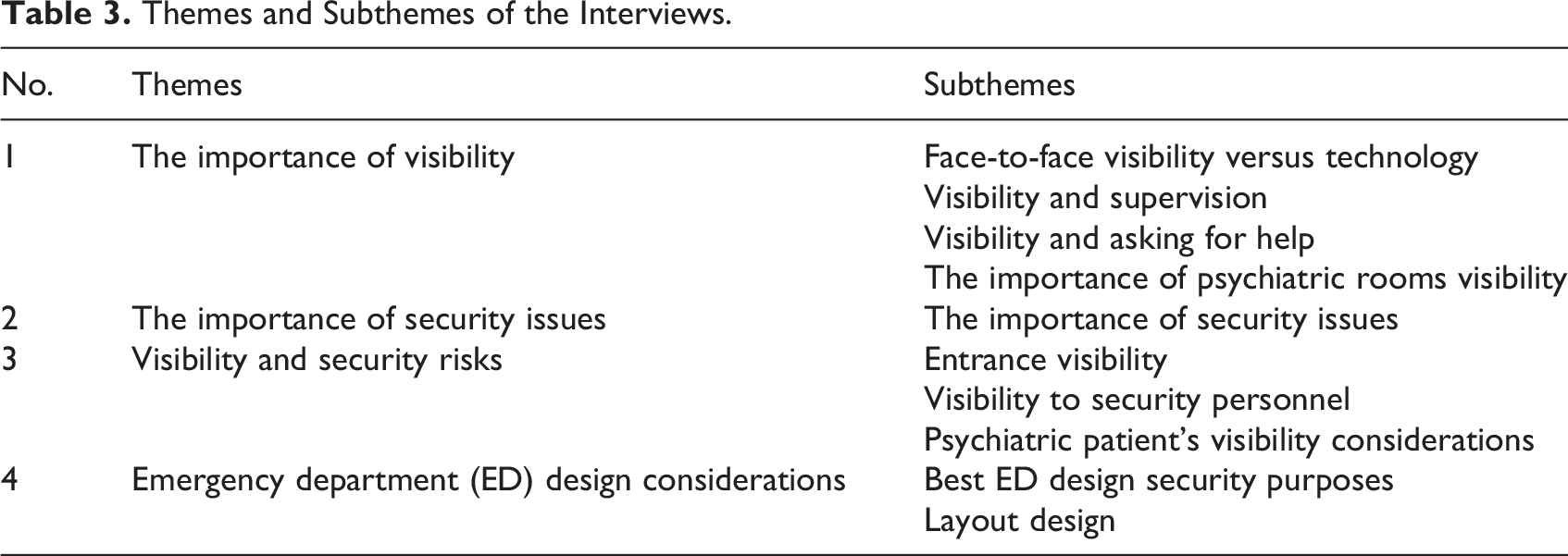
The importance of visibility in EDs and the effects of visibility on security were explored in 17 one-on-one interviews. After the analysis of qualitative data, four major themes and 11 subthemes emerged. The major themes were (a) the importance of visibility, (b) the importance of security considerations, (c) the impact of visibility on security issues, and (d) ED design considerations (see Table 3).
Themes and Subthemes of the Interviews.
Theme 1: The importance of visibility
Most research participants agreed on the importance of visibility in reducing ED risks. Some of the respondents referred to the influential role of visibility in supervision, asking for help, and minimizing distractions. This theme is divided into four subthemes relevant to the significance of the research question.
Subtheme 1: Face-to-face visibility versus technology
The interviewees considered face-to-face communication to be the most efficient and effective means of exchanging information in risky situations and for managing activity in the department. The nurses mentioned that the advancement of technology resolved some problems, but there were various complications associated with using different devices.
– “…If you know you need help quickly, you can actually see them instead of trying to dig out your phone and call for help” (RN10).
– “The phones I mean, they are pretty good, they are kinda pain to carry around…. But (laughing)…. I think they are less effective than talking face-to-face” (P4).
Subtheme 2: Visibility and supervision
The nurses discussed the priority of continuous supervision of the department by enhanced visibility in EDs. They emphasized visibility’s impact on the management of potentially risky conditions.
– “In the ED specifically, visibility is so important, since the patients are unstable and it makes the situation hard” (RN2).
Subtheme 3: Visibility and asking for help
Nurses and doctors referred to urgent needs for help, which can be facilitated by having high visual connectivity to other colleagues to handle the problems as a team.
– “Visibility, if I cannot see my co-workers, it is very hard to know if they need help, if they are feeling rushed or stressed out” (RN6).
– “If you can see, you can identify the needs but if you can’t see, you are depending on people to ask you, or tell you, or alert you which is not always possible…” (RN3).
Subtheme 4: The importance of psychiatric patients’ rooms visibility
The physicians and nurses shared their preferences about the high visibility of psychiatric patient rooms as a top priority. Some of the nurses mentioned they were more concerned with managing psychiatric patients than trauma patients.
– “Even though the trauma is important, unfortunately psych is the first one and trauma is the second…” (RN7).
Theme 2: The importance of security issues
In the interviews, ideas regarding security issues emerged, which they regarded as threats to ED care delivery. The nurses, as the most vulnerable staff members, highlighted the influential role of environmental design in controlling risks during day and night shifts. The medical staff shared a diverse range of security risks in EDs from psychiatric patient assaults to the serious risk of being harmed by patients or families.
– “People are getting more and more turned on to narcotics and alcohol, drugs and everything and things that make them mentally not right so the risk and danger in the ER is very high all the time” (RN4).
Theme 3: Visibility and security risks
Visibility was identified as an important design factor in promoting security, since visibility would increase staff awareness of problems, allow them to react quickly, and feel protected. Nurses noted visibility had a critical role in reducing aggression and controlling escalating situations. The nurses reported if aggressive people perceived that many staff members could observe them, in general, they might behave more logically.
– “It [visibility] makes it safer because everyone can see everything and if you are in trouble or it’s a risk, then everybody can help identify the risk” (RN6).
“If you could see what’s going on, with the open line of sight of all rooms, then nobody gets to the corner, and if somebody needs help, other can rush in, I mean there is less need for…. Yeah, increase visibility greatly helps the place be more secure” (RN7).
Subtheme 1: Entrance visibility
The control of ED entrances was discussed by participants as a factor in minimizing different security risks. In addition to unauthorized attempts to enter the department, psychiatric patients may try to escape and cause problems outside the ED. Thus, high visibility to/from different locations including security officers, nurse stations, and reception areas was an important issue.
– “…it [entrance] is [an] uncontrolled entrance, multiple entrances that people can come from without anyone standing by to keep an eye on them. They are locked but that changes as soon as someone goes out the door—someone can come in….” (P1).
Subtheme 2: Visibility to security personnel
The presence of security personnel inside the main ED and their visibility from outside were mentioned as factors that could minimize aggression. In particular, their supervision of the entrance and waiting area may mitigate aggressive behavior.
– “The optimum situation is that […] the security personnel have…good visibility—both…being seen and seeing” (P3).
Subtheme 3: Psychiatric patients’ visibility considerations
The supervision of psychiatric patients in order to stop them from harming others and themselves was addressed in the interviews. In many cases, one-on-one supervision was considered an important strategy to minimize the risk. Also, the placement of psychiatric patients to achieve higher visibility was emphasized by the nurses.
– “You know for the psych patients running around and trying to hurt somebody. You know we have kind of a locked down unit, but they can jump over the counters, even the front is not locked….” (RN7).
Theme 4: ED design considerations
This theme represents all of the specific design considerations that emerged during the interviews regarding security issues in EDs.
Subtheme 1: Best ED design for security purposes
Visible workstations and the visibility from work stations to the whole department were noted in interviews. Medical staff referred to a big rectangle, race track, or linear layout that allows the whole department to be visible and accessible.
– “It [department’s layout] was a large rectangle and a huge nurse station, spread around, seeing a lot of rooms and staff…plenty rooms for computers and whatever your room assignment was blocked together, and you could see your rooms” (RN10).
Subtheme 2: Layout design
Preference for a compact layout in which all the functions can be done in singular location emerged in the interviews. The nurses and physicians complained about the distributed layouts in which they have to serve many pods at the same time.
– “Not so spread out. We don’t need five hallways and then one bay area. Somehow it needs to be where the nurses and doctors can see each other…” (RN6).
Discussion
Overall, the data suggested that in EDs with high visual connectivity to all locations, security issues could be prevented, controlled, or minimized more easily. The departments with centralized layouts had higher visibility, as staff tended to be located in the main work stations during less busy times. Conversely, distributed layouts with separated pods had lower visibility, resulting in lower levels of staff helpfulness during risky events.
Furthermore, the informants found the ED entrance, waiting area, and triage to be critical locations needing the highest visibility to and from other locations. Concerns regarding psychiatric patient visibility frequently emerged in the interviews, and nurses preferred to have their work stations and charting areas close to the psychiatric patients.
Security in ED settings has been found to be disruptive to the vital treatment of patients. Aggressive behaviors of psychiatric patients and family members were the most frequently reported concerns of ED medical staff. The field observation data supported the value of one-on-one supervision of psychiatric patients by staff, while in some cases a team of technicians, security personnel, nurses, and a physician were involved in stabilizing the psychiatric patients. This led to disruption in ED service consistent with findings from a previous study by Knowles et al, (2013). One-on-one observation of psychiatric patients was a strategy found in the literature and observed at the sites in this study (Neckar, 2015). The findings of the interviews as well as observation sessions are in agreement that visibility is important to improve security and this is consistent with the existing literature (e.g. Gharaveis et al., 2018; Gharaveis, Hamilton, et al., 2019; Gharaveis, Shepley, et al., 2019; Pati et al., 2014; Pati et al., 2016; MohammadiGorji et al., 2021). The RNs and physicians noted that with high visibility, potentially risky events can be seen quickly, allowing staff and security personnel to intervene appropriately. Additionally, the presence of security officers was perceived as an intrinsic factor in hampering aggressive behavior. A similar result was found during the observation sessions, where security staff were involved in handling aggressive behavior in psychiatric patients.
The overall findings of this study are consistent with most of the previously reviewed studies (see Table 4). The collected data supported the findings of Anderson et al. (2010) regarding the vulnerability of nurses in EDs. Additionally, this study contributes to the body of existing literature regarding environmental design strategies to reduce aggression in hospitals (e.g., Angland et al., 2014; McPhaul et al., 2008; Pati et al., 2014; Pati et al., 2016; Poyner & Fawcett, 1995).
Comparing Security Findings Between This and Previous Studies.
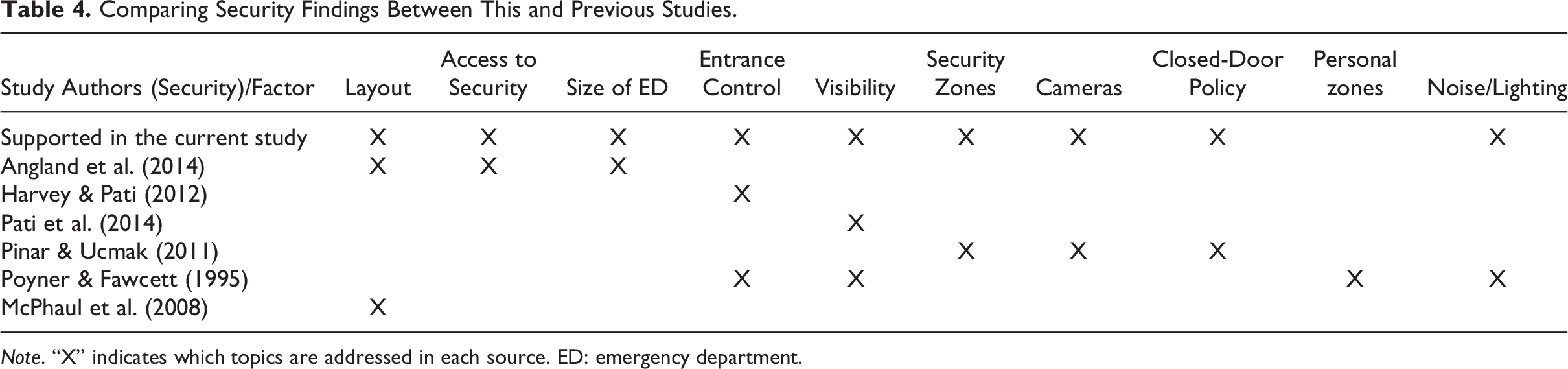
Note. “X” indicates which topics are addressed in each source. ED: emergency department.
Limitations of the Study
This study benefits from qualitative data that were based on real-life experience and perceptions. The subject sites were conservative in disclosing the exiting security-related data within the scope of this study. However, more objective perspectives regarding the same research question can be applied to triangulate the results. The current study was conducted in 2016 in five community hospital EDs that varied from 20 to 36 exam rooms and the results are generalizable to community hospitals. However, the collected data can still be considered relevant because of multiple reasons. First, there are still similar challenges in EDs that can be minimized by rigorous investigations. Second, all the operations and protocols in subject sites regarding ED healthcare delivery have not been changed since data collection. From the qualitative research perspective, the dynamics in all the subject sites have not gone through major operation and cultural changes. Finally, there has not been a similar study published in the peer-reviewed journals at the time of writing this publication. Future studies might include a wider variety and larger number of ED settings and more updated design layouts might be included. The study participants were a convenience sample with potential biases, and their opinions may not be representative of others in similar settings; future studies could use randomly selected research participants. Additionally, this study was limited to medical staff; future studies might encompass a wider range of professions including administrators, unit clerks, technicians, security personnels, and other nonmedical staff. Finally, because of the changes in the dynamics of the behavioral health issues after the emergence of COVID-19, future studies should focus on this issue extensively.
Conclusion
This study supports the idea that enhanced visibility can improve actual and perceived security in EDs. The findings of this study can help designers to increase the acceptance of design solutions by stakeholders. Also, the data offer some baseline theories for future researchers to develop other conceptual plans with more details. From another perspective, this study is intended to be useful to design practitioners, healthcare administrators, nurses, and experts from healthcare industries, including medical professionals and nonmedical staff who are impacted by the ED environment. The results of this investigation can be used by community hospital administrators and healthcare designers to improve nurses’ and physicians’ levels of performance through architectural design by reducing security risks. Additionally, the security-related improvements will help nurses, physicians, and nonmedical staff to work in safer environments, potentially leading to increased job satisfaction. Furthermore, the findings can contribute to the body of knowledge with respect to the effect of environmental design on behavior in healthcare facilities.
Implications for Practice
This qualitative study investigated the impact of visibility on security in EDs.
The main implications for practice are as follows: Environmental design is one of the critical factors for security enhancement in EDs. Nurses prefer to have visual connectivity to their colleagues to feel more secure and facilitate the healthcare delivery. Nurses and physicians in the study indicated that security can be highly improved by high visibility. This study founds some values of visibility can be highly important for future investments.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231188985 - How Visibility May Reduce Security Issues in Community Hospitals’ Emergency Departments
Supplemental Material, sj-pdf-1-her-10.1177_19375867231188985 for How Visibility May Reduce Security Issues in Community Hospitals’ Emergency Departments by Arsalan Gharaveis, D. Kirk Hamilton, Debajyoti Pati, Mardelle McCuskey Shepley, Susan Rodiek and Denise McCall in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Institute of Architects (AIA-AAH Practice Advancement Initiative).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.