
Abstract
Objective:
This exploratory study examines a rural critical access hospital (CAH) staff’s perception of current obstacles and needs concerning the physical environment.
Background:
CAH intends to improve access to healthcare, coordinate with experts and providers, and serve as the rural population’s healthcare hub. It is imperative to understand environmental qualities that impact the quality of care to develop effective policies and design guidelines for rural healthcare. Nevertheless, a limited number of studies have focused on user or organizational outcomes related to the physical environment of rural healthcare settings.
Methods:
This cross-sectional exploratory qualitative case study was conducted as part of the facility planning process for a CAH in rural North Carolina. Hospital staff participated in a survey exploring their satisfaction with the overall physical environment privacy, space allocation, and department adjacency. An open-ended question asked staff to elaborate on needed improvements and changes in their department.
Results:
Findings show low satisfaction levels for space allocations for emergency department, lab, surgery, and wound care. Safety and quality were the two emerging outcomes of the physical environment’s shortcomings. Two clusters emerged from the content analysis, representing facility needs (rightly sized spaces, functional needs, COVID-19 needs, and improved access) and ambient conditions (clutter, visibility, flooring quality, noise, privacy, cleanliness, aesthetics, and temperature).
Conclusion:
The findings from this study suggest that the interior and exterior facility and ambient conditions of the CAH play a key role in quality and safety outcomes.
Keywords
Introduction
Critical access hospitals (CAH) aim to improve healthcare access for a rural population with healthcare access inequities. Living in rural areas of the United States associates with inferior health outcomes, with a 40% higher preventable hospitalization rate and a 23% higher mortality rate than urban residents (Johnston et al., 2019). Established disparities, such as longer driving distance to a hospital (Billi et al., 2007; Cai et al., 2019) or lack of access to healthcare specialists, have resulted in different health outcomes between rural and urban areas (Brundisini et al., 2013; Johnston et al., 2019). To bridge this gap, CAH intend to improve access to healthcare, coordinate with experts and providers, and serve as the hubs of healthcare for the rural population (The Rural Health Information Hub, 2022).
It is essential to improve the understanding of environmental qualities that impact the quality of care for developing effective policies and design guidelines for rural healthcare. Current evidence suggests physical environment is one of the factors affecting rural healthcare patient experience, staff recruitment, patient participation, patient satisfaction, processes, and staff satisfaction (Cai et al., 2017, 2019; Haddox, 2018; Pati, Gaines, & Valipoor, 2016). Nevertheless, a limited number of studies have focused on user or organizational outcomes related to the physical environment of rural healthcare settings (Cai et al., 2017, 2019; Haddox, 2018; Pati, Gaines, & Valipoor, 2016). These studies recommend investigating rural care teams’ perceptions of the potential relationships between environmental variables.
Cai et al. (2017) study showed that existing facilities need to be improved in providing high-quality patient care satisfaction and staff work experience. In another study, Cai et al. (2019) survey of rural residents suggested the topmost important environmental quality as privacy, adequate chairs in exam rooms for families, and practical tools for information sharing and communication between patients, families, and clinicians. The research also found a correlation between design features for an open counter to communicate with the receptionists and simultaneously supporting patient privacy. The authors also emphasize the need for patient privacy support in exam rooms to discuss insurance information and financial implications, as such topics are a paramount concern for rural residents.
Haddox et al. (2018) performed a pilot qualitative study on the elderly population of a rural outpatient clinic. The study found that lack of privacy or confidentiality at check-in, clutter, seating proximity to contagious patients in waiting rooms, and inadequate natural lighting in the reception and exam rooms were some of the perceived barriers to patient participation that may cause missing appointments. Pati et al. (2016a) conducted an explorative qualitative study of administrators of four rural hospitals. The findings indicated that older facilities were inadequate or unattractive workspaces, negatively affecting efficiency, safety, clinician specialist recruitment, staff morale, and patient perception of their local hospital patient experience. Small operating rooms (OR) needed more flexible teamwork space and imposed equipment installation issues that impacted surgeon recruitment. Laboratory, pharmacy, imaging, or radiology departments also reported challenges such as the inadequate size of space, configurations with improper adjacencies, or in demand for additional storage size. These conditions negatively impacted operational efficiency and safe delivery of care.
The focus of this exploratory study was to address the following research questions: What is the staff’s perception of the current obstacles and needs relevant to the CAH’s infrastructure, physical environment attributes, or ambient conditions? Furthermore, why is improving and overcoming these obstacles and needs essential? The underlying framework in this study is that the facility design and qualities of CAHs impact participant or organizational outcomes. Additionally, the study adds to the limited body of knowledge on the impact of a pandemic on rural healthcare facility design. Finally, this study aims to contribute to the evidence-based design literature and inform decision makers of future CAH design policy, practice, and research.
Method
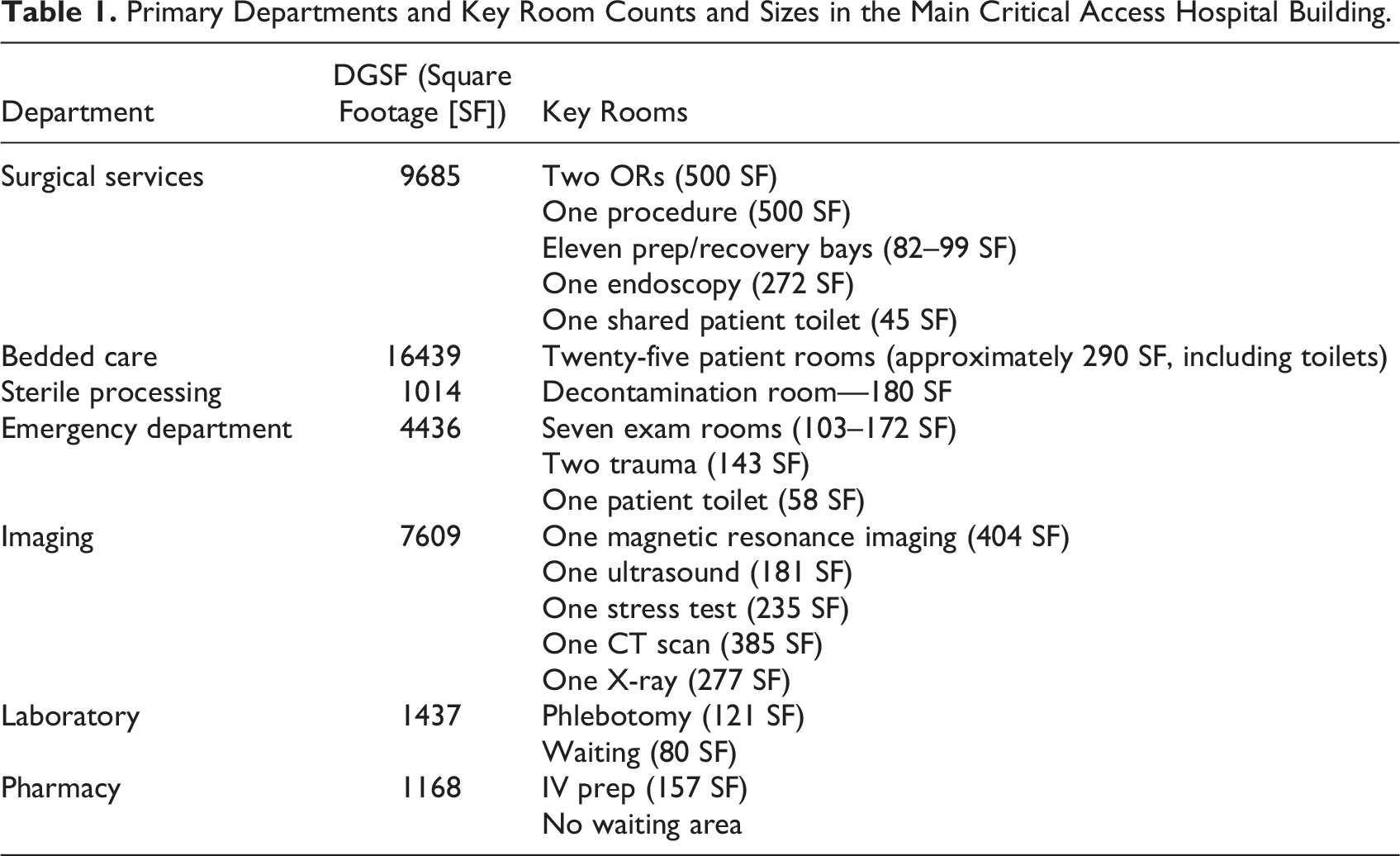
This cross-sectional exploratory qualitative case study was conducted as part of the facility planning process for a CAH in rural North Carolina. The hospital was open to the rural county in 1930 and included specialties such as cardiology, family practice, urgent care, wound care, orthopedic surgery, women’s health, and emergency department (ED). Table 1 and Figures 1 and 2 explain critical department: Departmental Gross Square Foot (DGSF) and room Square Footages (SFs). The main hospital had two levels for a total of 85,000 SF. Outpatient clinic buildings comprise seven detached buildings scaled between 1754 and 4201 (SF). An additional nursing center department, with approximately 22788 (SF), was currently vacant and used for storage.
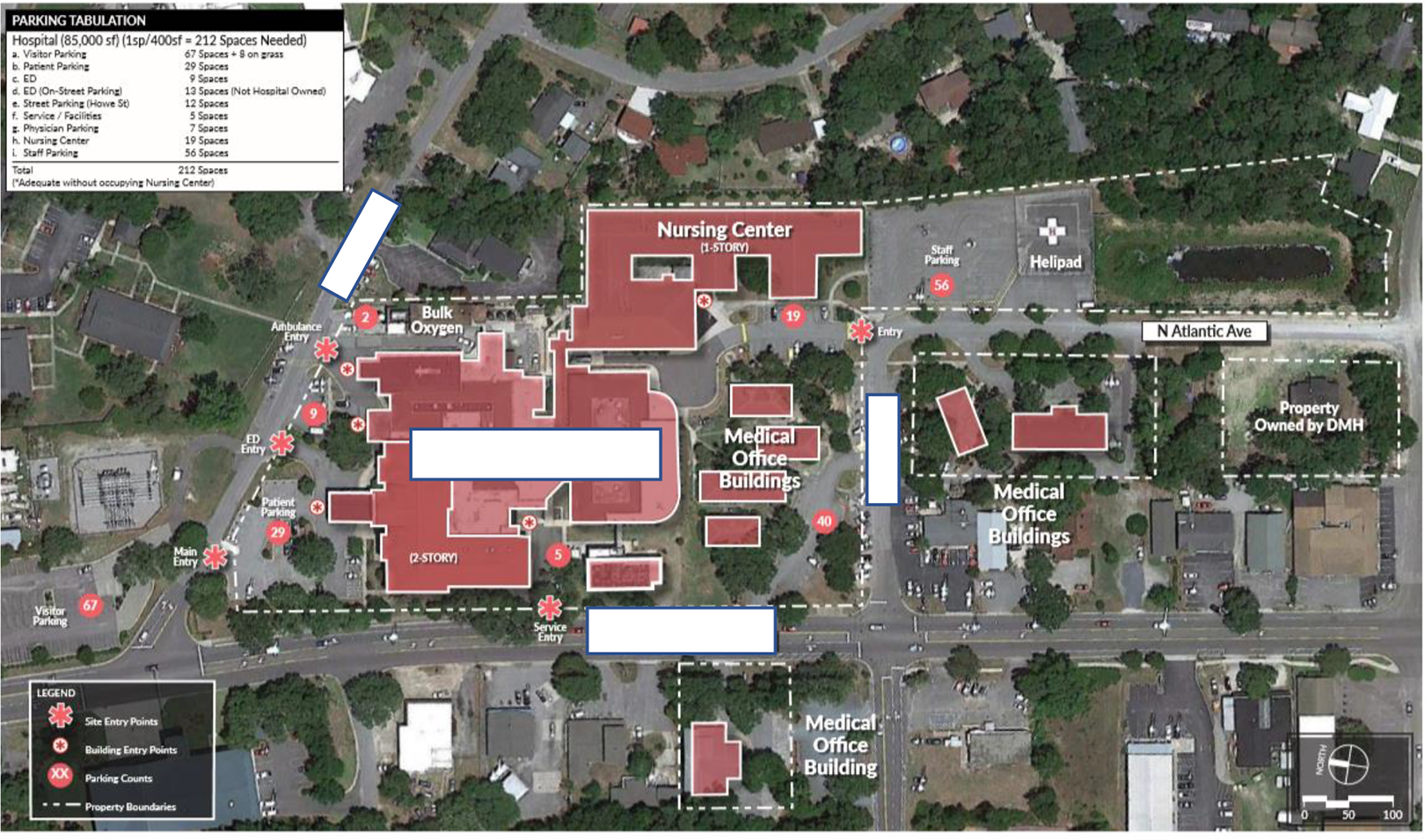
The main hospital site plan comprises various buildings, including the emergency department, surgical department, medical office buildings, and a vacant nursing center. Source: Image Copyright: Author.
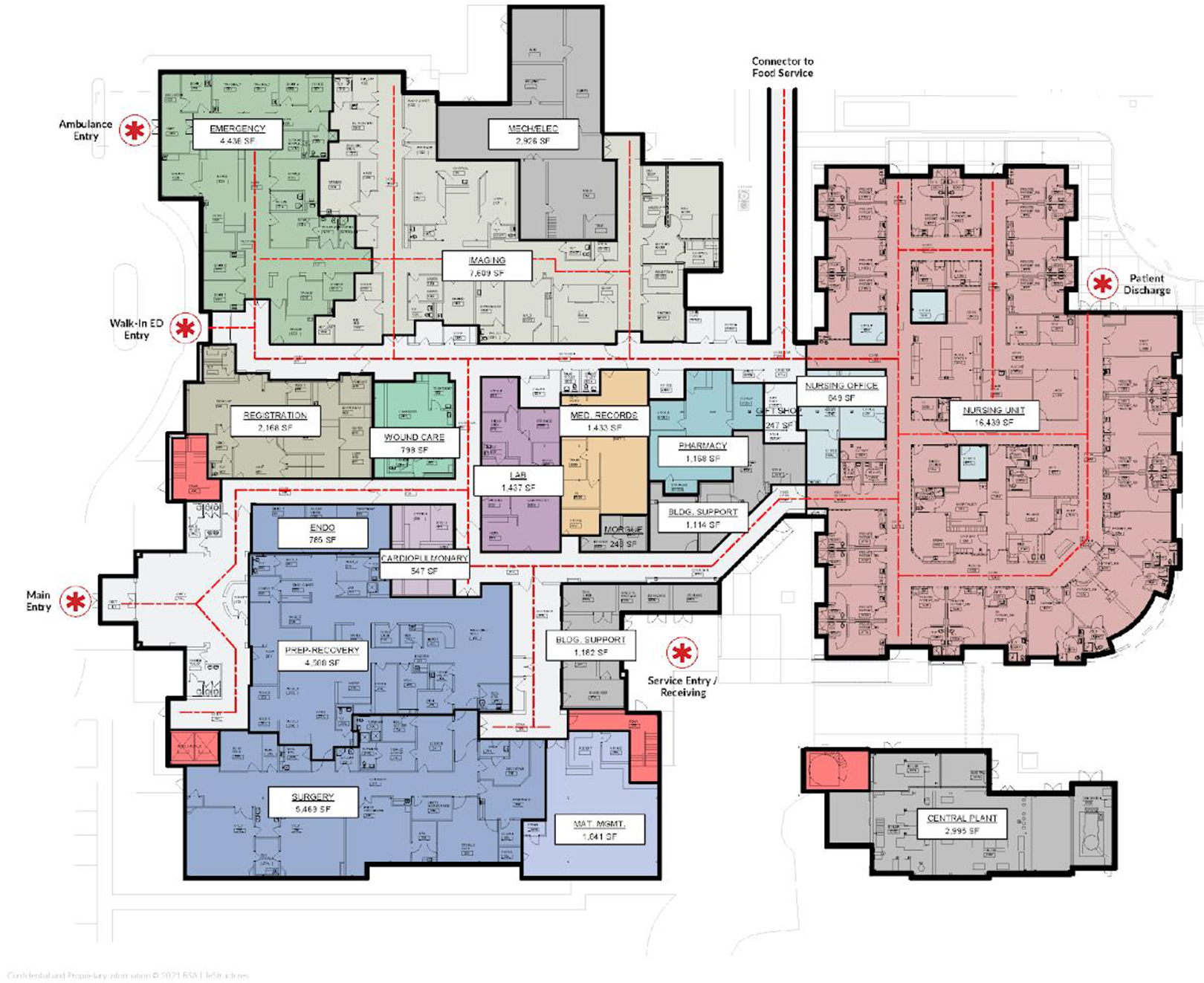
This image displays the department adjacencies and circulation flow of the main critical access hospital. Source: Image Copyright: Author.
Primary Departments and Key Room Counts and Sizes in the Main Critical Access Hospital Building.
Procedures
The planning, architecture, and operational assessment team combined semi-structured interviews, surveys, and observation assessment methods to understand needs, goals, and environmental challenges across diverse departments. The CAH’s Ethics Committee reviewed and approved the study protocol. For this article, we will primarily focus on the survey responses. We collected data during November and October 2021 over 4 weeks. Initially, the survey was printed in paper format and distributed by the CAH coordinator. Later, the CAH used departmental email distribution lists to distribute the online survey link created in Google Forms. It was noted in the email and surveyed introductory paragraph that participation is voluntary. The study avoided coercion to participate by not offering payment incentives and no threat of harm if they declined participation. We collected no identifying information from participants.
Instrument
An expert panel of planners, architects, and researchers collaborated to create a short survey to understand staff’s satisfaction with 13 items, including overall physical environment, space allocation, team communication, patient flow, medication flow, privacy, provider flow, family–visitor flow, or departmental adjacency. We could not perform a reliability test due to limited access to participants. Respondents were asked to rate the various items based on their perceived satisfaction level using a 5-point Likert-type scale ranging from 1 = extremely dissatisfied to 5 = extremely satisfied. Demographic questions included department type and role. The open-ended question asked to the participants is: “What is working well in your current department? What would you change to make your department work better?”
In addition to the surveys, 21 staff participated in 10 focus group sessions. The hospital coordinator recruited staff through emails, encompassing nurses, physicians, administrative, and leadership roles. The team explored clinical and administrative staff experiences regarding physical environment needs impacting processes and performances. Questions focused on department goals, challenges, and success factors. Similar to the open-ended questions in the survey, we also asked the staff about the physical environment changes needed to improve their care delivery. Handwritten notes were taken during the focus group interviews, capturing essential insights. This article focuses primarily on reporting the responses relevant to the physical environment concerns.
Participants
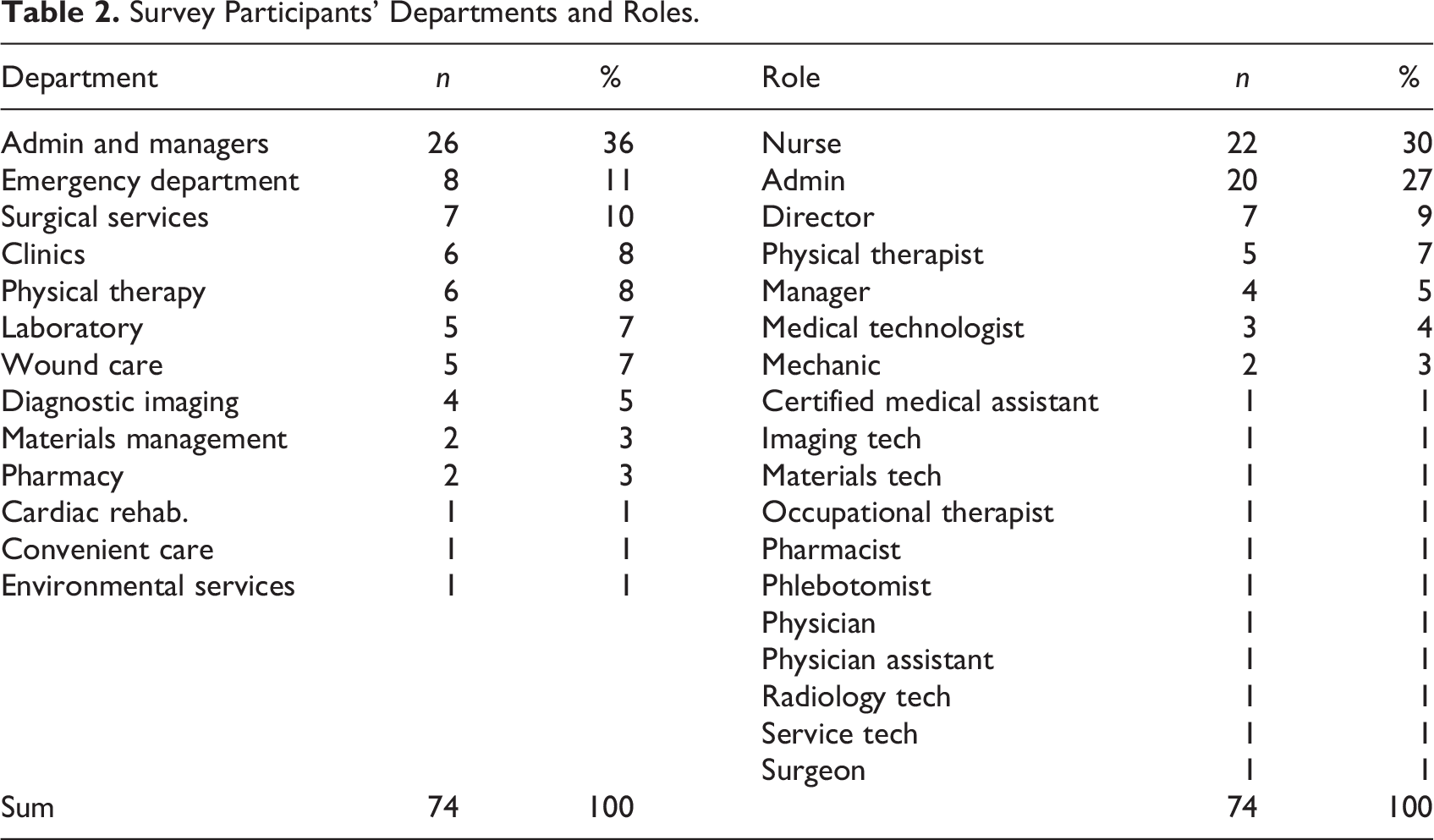
The CAH site was undergoing a 3-year master facility planning; thus, the study was based on a convenience sample. The entire CAH staff was the population of interest, including managers, clinicians, and nonclinicians (n = 207). There were no exclusion or inclusion criteria. Seventy-four individuals completed the online or paper survey with an overall 36% response rate. Tables 2 and 3 display participants’ departments and roles. Due to limited direct access to participants, we conducted no further analysis to determine the characteristics of staff who did not respond.
Survey Participants’ Departments and Roles.
Data Preparation and Analysis
Qualitative data preparation and analysis of open-ended responses were performed in MS Excel. The Google Form and paper-based responses were organized and merged into an MS Excel document. Descriptive statistics were analyzed using the JASP Version 0.16.4.0 software for the Likert-type scale-based questions. The internal expertise team reviewed all codes to ensure data validity and interpretation. The goal was to understand the staff’s level of satisfaction with the overall physical environment, space allocation, department adjacency, and privacy. The second phase included looking at departments with lower satisfaction ratings for these physical environment ratings. Initially, all transcripts were coded based on their contents with particular attention to subthemes suggested by Pati et al. (2016a): (a) any direct reference to the facility needs or physical environment qualities of the CAH, including the buildings, departments, and workspaces, and (b) any outcomes associated with the physical design such as staff or patient experiences, care quality, operations, or safety. Next, we clustered the subthemes into key themes aligning with the content analysis performed by Cai et al. (2019) and Pati et al. (2016a).
Results
Satisfaction Ratings
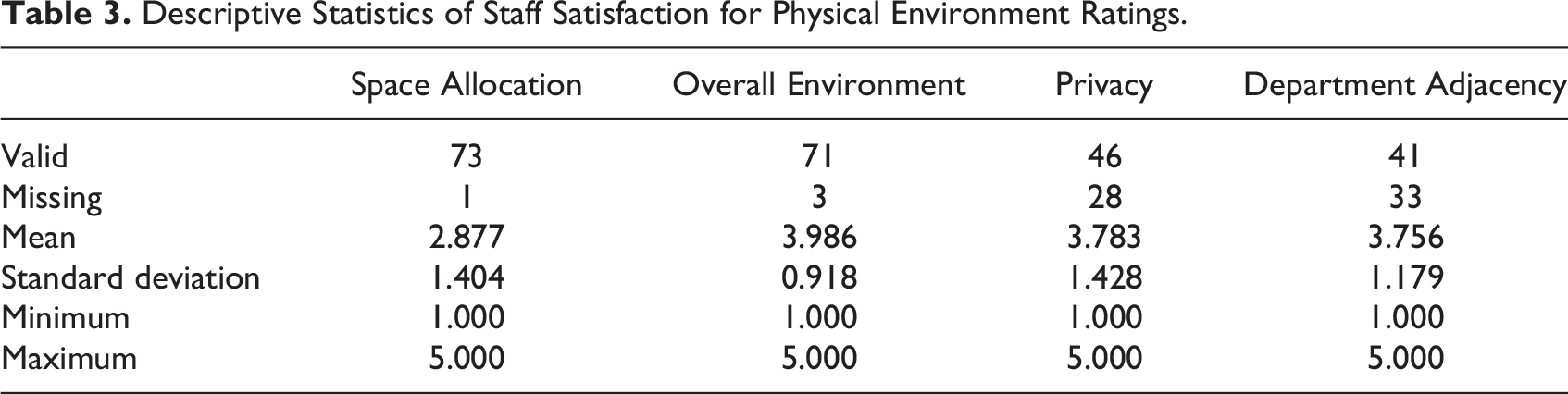
Table 3 displays the descriptive statistics for the overall CAH and staff’s average satisfaction per department (Table 4). The findings suggest low satisfaction levels for ED, lab, surgery, and wound-care space allocations. Wound-care staff was also comparatively dissatisfied with department adjacency and the overall environment compared to other departments. The surgical staff was the least satisfied with the privacy attributes of their department. Due to low participation from some departments, the survey results are qualitative and not generalizable.
Descriptive Statistics of Staff Satisfaction for Physical Environment Ratings.
Descriptive Statistics for Physical Environment Satisfaction Ratings per Department.
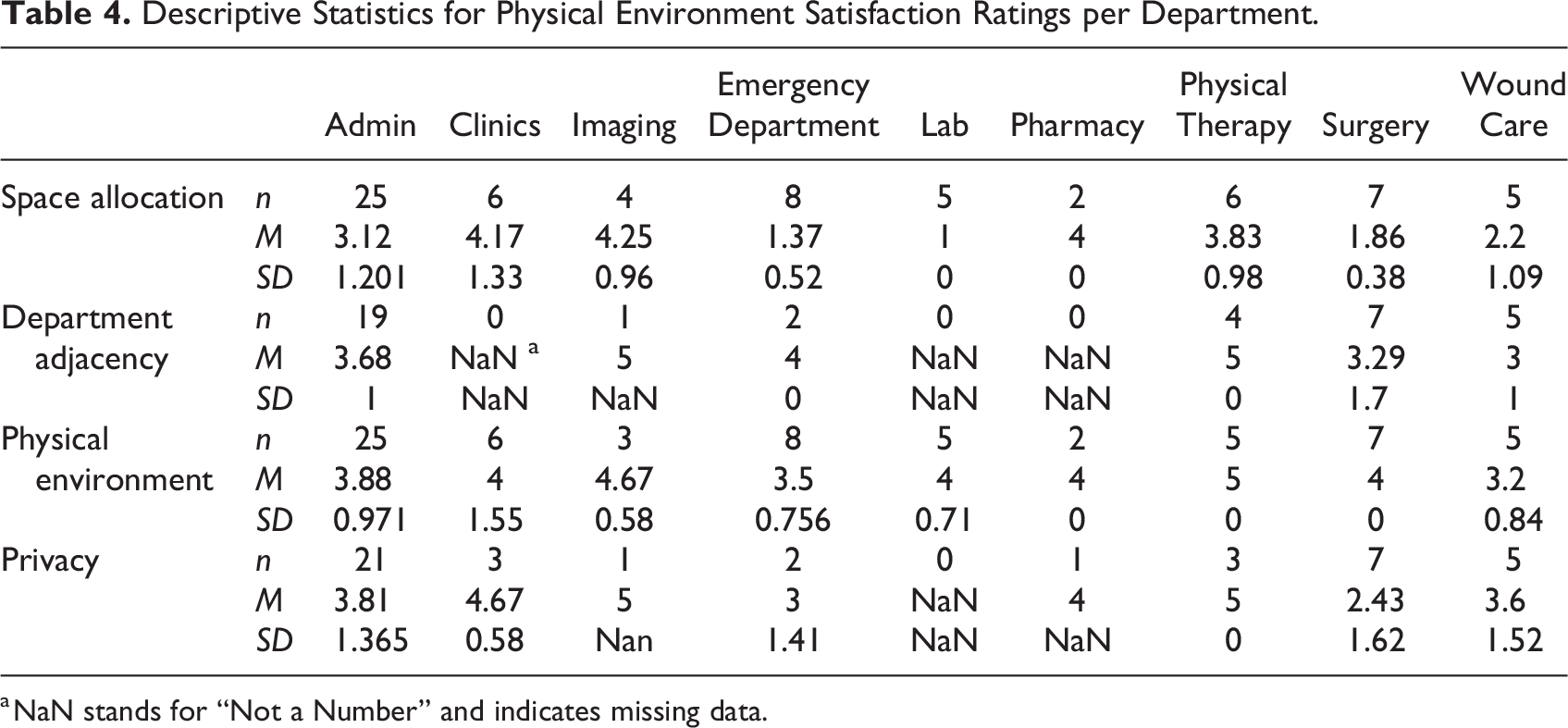
a NaN stands for “Not a Number” and indicates missing data.
Open-Ended Findings
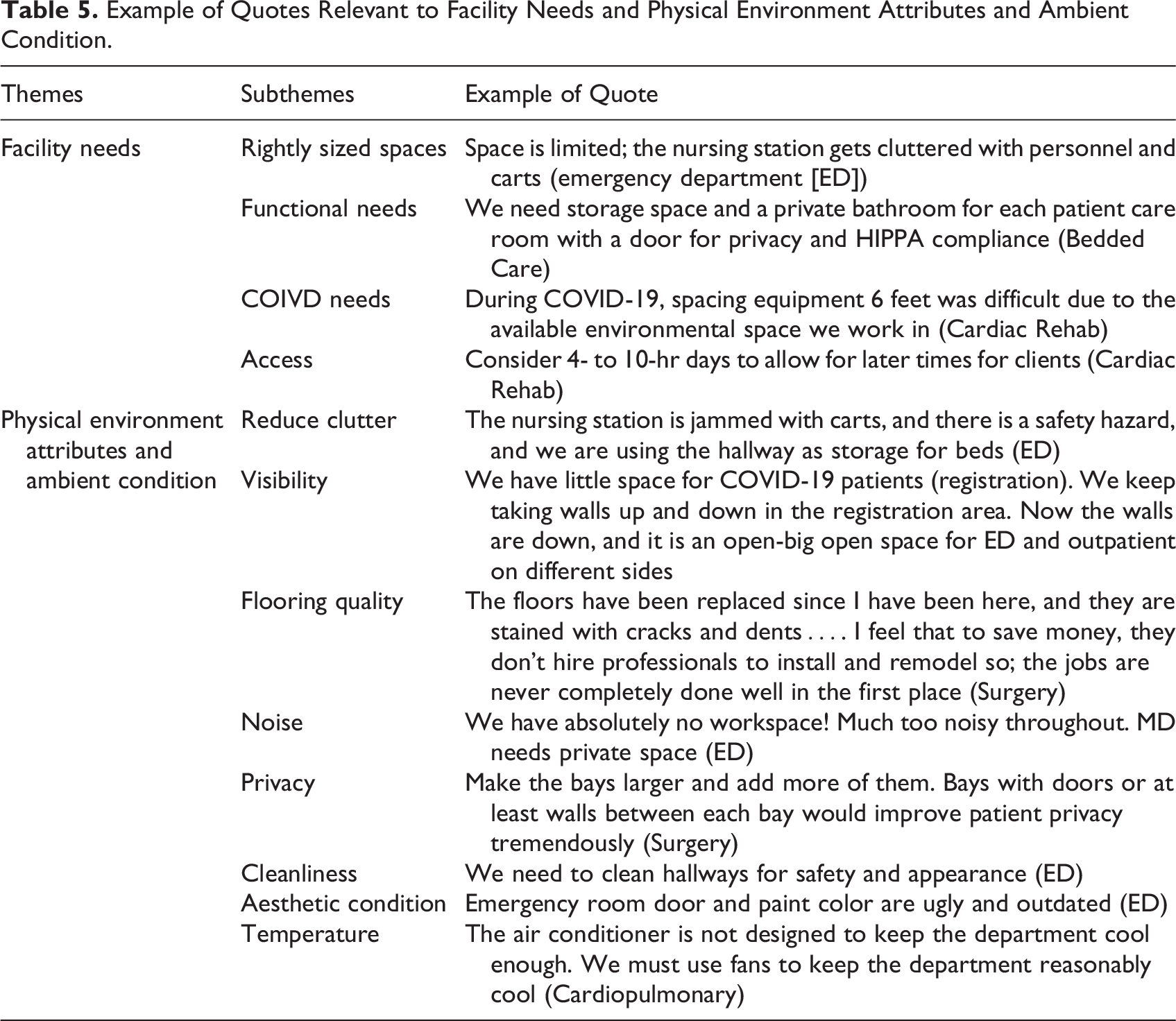
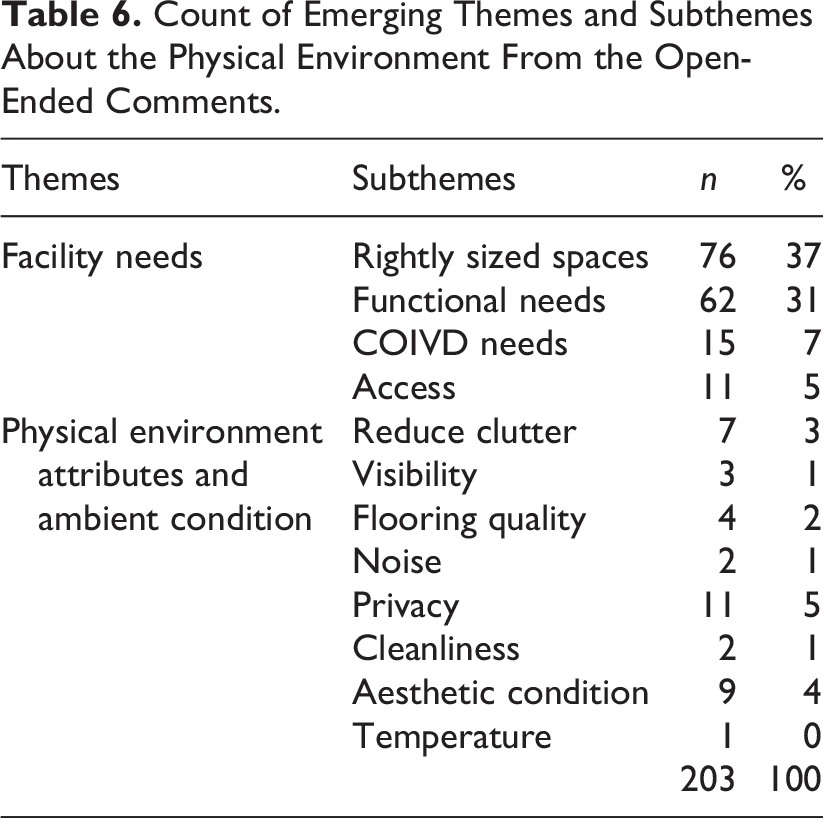
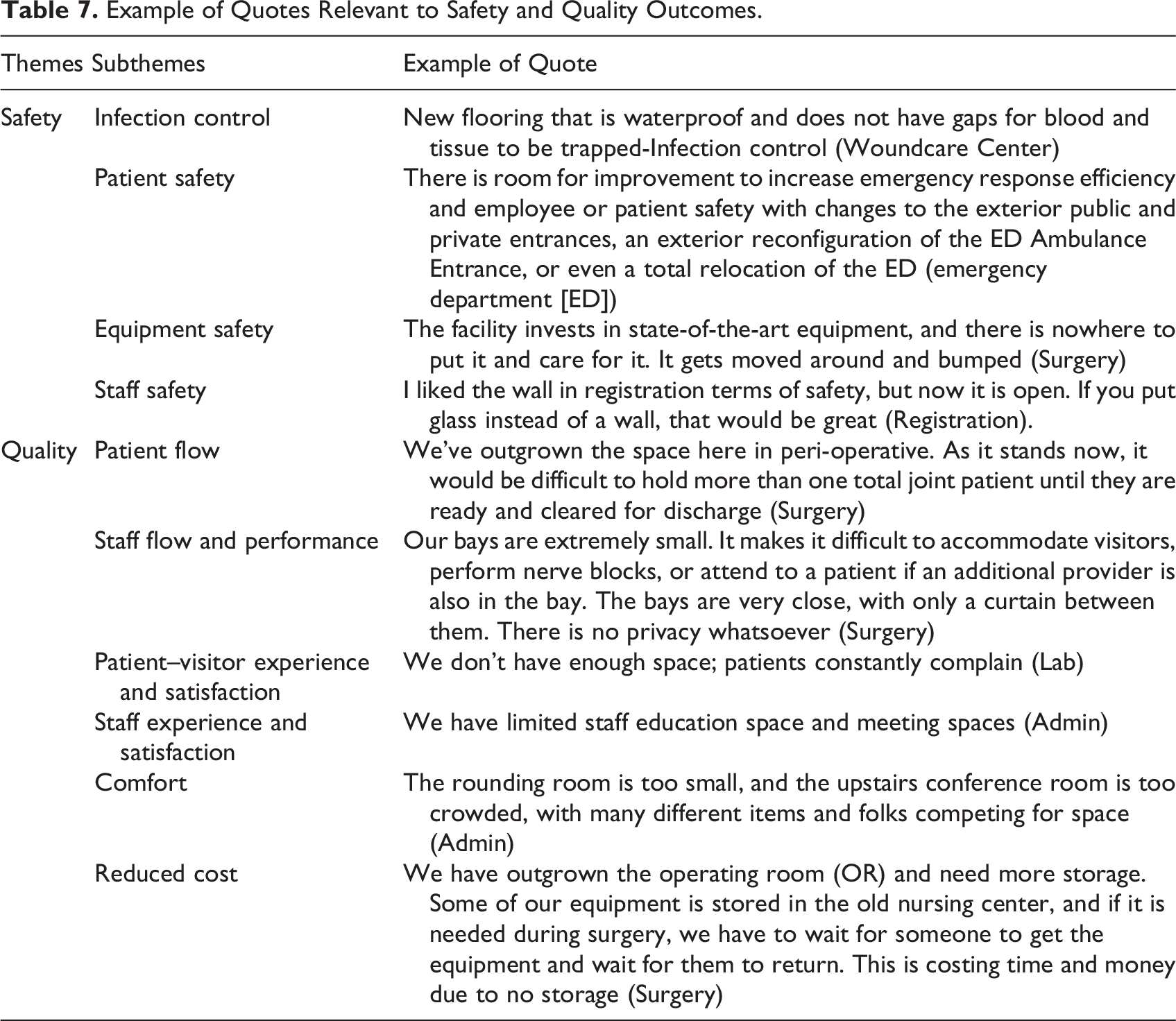
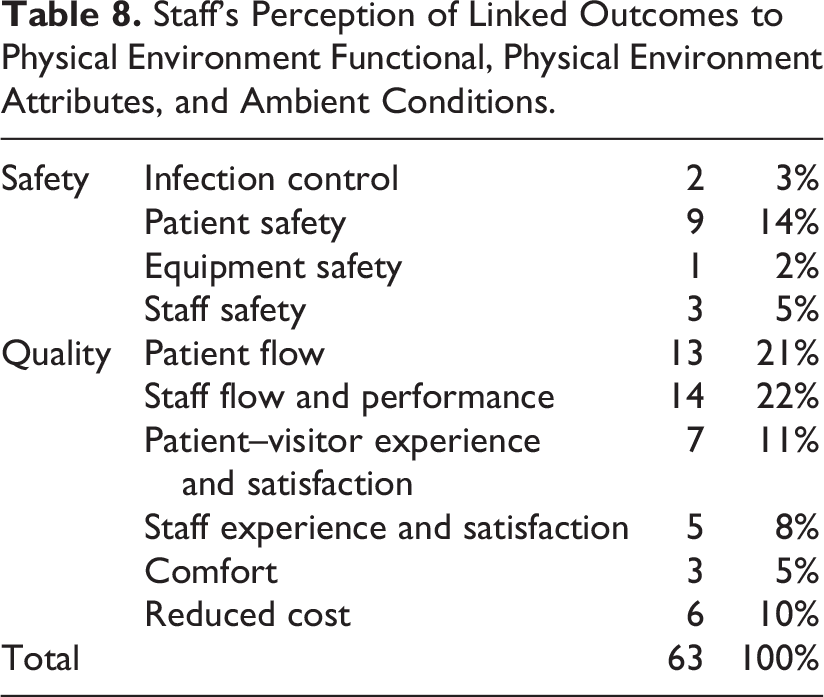
Two clusters emerged from the content analysis, representing facility needs (rightly sized spaces, functional needs, COVID-19 needs, and improved access) and physical environment conditions (clutter, visibility, flooring quality, noise, privacy, cleanliness, aesthetic conditions, and temperature; Table 5 and 6). Safety and quality were the two emerging outcomes of the physical environment’s shortcomings: safety concerns to infection control compliance and patient, equipment, and staff safety; quality pertained to patient flow, staff flow, staff performance, patient–visitor satisfaction, staff experience and satisfaction, comfort, and cost outcomes (Table 7 and 8).
Example of Quotes Relevant to Facility Needs and Physical Environment Attributes and Ambient Condition.
Count of Emerging Themes and Subthemes About the Physical Environment From the Open-Ended Comments.
Example of Quotes Relevant to Safety and Quality Outcomes.
Staff’s Perception of Linked Outcomes to Physical Environment Functional, Physical Environment Attributes, and Ambient Conditions.
Facility needs
Facility needs were the most mentioned themes in the open-ended responses. Emerging subthemes included the need for adequately sized spaces, functional needs, COVID-19 needs, and access improvements that will be reviewed in the subsequent paragraphs.
Rightly sized spaces
The first subtheme focuses on the inadequate space sizes in outdated buildings. These included desiring larger departments, workstations, exam rooms, bathrooms, offices, meeting spaces, waiting rooms, equipment rooms, break rooms, or training rooms. Administrative staff reflected the need for larger meeting spaces for staff, office spaces, and rounding rooms. Lab department staff requested more extensive patient waiting, storage, drawing area, testing space, equipment room, or intravenous (IV) rooms to improve patient experience and flow. The ED staff mentioned needing larger patient rooms to accommodate computers, equipment rooms, storage space, and adequately sized nurse stations to improve patient flow. Universal and flexible rooms that were identical to monitoring capabilities were desired. The surgical team perceived the space needed to be more responsive to departmental growth. They emphasized the need for larger storage spaces, nurse stations, ORs, patient bays, and central sterile spaces corresponding to the patient volume. The insufficient equipment storage space affected equipment safety outcomes, as one of the staff explained: We are outgrowing our space in the OR. We need more room to store our equipment. The facility invests in state-of-the-art equipment, and there is nowhere to put it and care for it. It gets moved around and bumped.
Staff emphasized the need for a more extensive Sterile Processing Department (SPD) to accommodate more washers, storage, and desk space to support the number of sterilized trays and OR procedures. The inadequate space resulted in stacking trays on each other, which resulted in the risk of case delays, contamination, and subsequent patient infection. Further, the poorly stacked trays created safety concerns for staff as they needed to bed down to pick heavy trays from shelves (Figure 3).

The Sterile Processing Department was considered small to accommodate the surgical department patient volume. Source: Image Copyright: Author.
Functional needs
Functional needs were captured by mentioning additional spaces or revised adjacencies varying by the department. Administrative staff reflected the need for more meeting or conference spaces, additional classrooms, workspace, or rounding rooms with integrated technology for virtual meetings. Another administrative staff mentioned the need for private office rooms to “be more cohesive to accomplish more work.”
The clinical staff communicated the concern about the lack of storage in the ED, resulting in cluttered hallways and a “jammed” nurse station that imposed a safety hazard. ED staff requested additional bathrooms, equipment rooms, safe rooms, and exterior decontamination storage. One of the ED staff elaborated on the possible reuse of the nursing home currently used as storage for the ED spatial needs (Figure 4). One of the staff elaborated: [the closed nursing home facility] area would give the Emergency Room (ER) the Space it needs, storage, extra bathrooms, and privacy adjacent to our helicopter flight area. Saving the patient at least 10 minutes of critical time.

The Nursing Center department was vacant and functioned as a storage space for other departments. Source: Image Copyright: Author.
Staff from the imaging department thought the adjacency to ED was optimal. They reflected the need for an additional shower and changing rooms for the entire facility. Laboratory staff reflected the need for staff break rooms and lockers, American Disability Act (ADA)–compliant toilets, and storage. One staff noted that departmental adjacencies were substantial for efficient flow, cost, and patient satisfaction: “We need more space. And not chopped-up space; you must walk across the hall to use additional space. We need space that is all together.”
The pharmacy department requested additional patient toilet rooms and a satellite pharmacy. Outpatient clinic staff thought the separate clinic buildings with three to four exams per building were not optimal, as one described: “It would be best to consolidate to a multi-specialty model to reduce cost and overhead terms of staffing.”
The wound-care center reflected on how the separated buildings from the hyperbaric affected inefficient operations or increased staffing requirements. With this inefficient adjacency, there was a need for reserved parking and a risk of patient falls. This situation also impacted patient safety and satisfaction outcomes as patients needed to gown and drive to the chamber.
Surgical staff explained the need for additional equipment storage, workspaces, bathrooms, and walled patient bays. An inadequate number of post anesthesia care unit (PACU) bays resulted in an urge to discharge patients to maintain flow from the OR to patient bays, which affected the patient experience of feeling “rushed to be discharged.” Staff perceived the need for bays with doors to protect patient privacy and satisfy storage needs in bays. Surgical staff described that inappropriately located equipment storage affects efficiency and cost outcomes.
COVID-19 needs
Smaller departments, such as lab, cardiac rehab, or ED, were more concerned about spatial limitations that restricted the COVID-19 social distancing guidelines. The ED registration staff complained about the waiting area congestion and its impact on visibility and safety during the pandemic. The staff noted that moving sick patients to another section with removable dividable walls during the pandemic was safer. However, these walls impeded visibility for the ER registration staff. Therefore, the ED registration staff recommended including glass walls to support visibility and patient separation (Figure 5). With the ease of pandemic limitations, the CAH removed the walls with only one glass wall remaining, resulting in the current open waiting room that decreased the perception of safety for staff.

Emergency department waiting room had a partial glass-wall division to accommodate the pandemic guidelines for infectious patient divisions. Other wall divisions that impeded visibility had been removed. Source: Image Copyright: Author.
The pandemic highlighted the need for revisiting the ambulance entrance to the ED as it presented spatial challenges to accommodate officials for mass casualty and contaminated patient incidents. Further, staff elaborated on the need for climate-controlled storage for decontamination equipment adjacent to the ED. Decontamination equipment stored in a distant location from the ED entrance and exterior space could have been more efficient spatial adjacency.
Most outpatient clinic patients had complex chronic conditions; some traveled up to 20 miles to access primary care services. Clinicians recommended expanding telehealth services for wellness visits due to Medicare reimbursement. The current use of telehealth for provider visits was 10%. In the current state, preregistration occurs through text messages, patients wait in the car and alert their arrivals, and nurses screen patients in the cars and direct them from back doors if suspected to be infectious by COVID-19. However, older patients struggled with telehealth and preferred meeting the provider in person or over the phone.
Improve access
The old infrastructure and inadequate spaces resulted in many noncompliant ADA toilet rooms. To improve patient access, staff recommend extending the operating hours for some departments, including physical therapy. Staff also mentioned necessary exterior upgrades to improve patient accessibility, especially for older patients: “For patients with walkers, walking across sand or accessibility with a ramp is difficult; we need to improve the patient experience.”
Smaller scale clinics were a positive attribute for patient experience outcomes as they reduced walking distances for older patients. Adjacency and access to or within departments were also crucial for staff. For example, lab staff explained the need for a more cohesive department to reduce walking distances and improve staff performance. Adding automatic doors for ED was also a recommendation to improve visitor access and staff efficiency to eliminate the need for staff to open doors.
Physical environment attributes and ambient condition
Staff elaborated on improving physical environment attributes and ambient conditions by reducing clutter, improving visibility, flooring material quality, cleanliness, aesthetic condition, temperature comfort, and privacy attributes discussed in the upcoming paragraphs.
Reduce clutter
Restricted space in specific departments such as ED or surgery resulted in a need for more storage spaces for equipment, carts, or beds cluttered ambiance (Figure 6). Staff believed that reducing the clutter improves efficiency, safety, and costs. Staff commented on the need for additional equipment storage to improve flow and reduce hallway clutter for operational efficiency outcomes. One of the ED nurses described how the nursing station gets cluttered with personnel and carts. This condition reduced the clinician’s satisfaction, as one described: “We feel like we are sardines in our nurse’s station.” State-of-the-art equipment stored in the hallways surgical department was bumped and moved around, which harmed equipment quality. The surgical services staff emphasized the importance of reducing OR clutter to improve operations and movements.
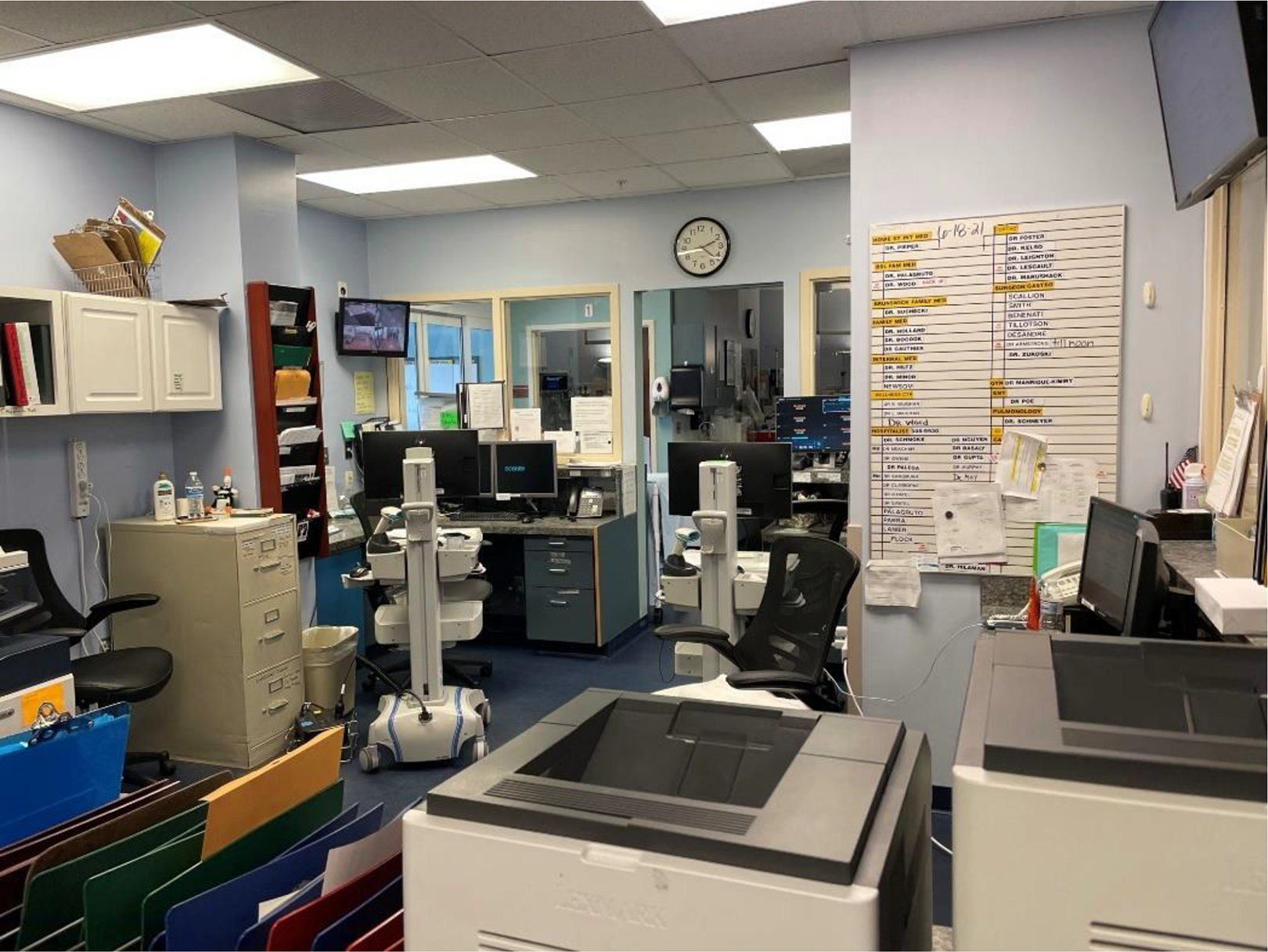
This image shows the cluttered emergency department nurse station. Clinical staff complained about the lack of privacy and impeded visibility in the department. Source: Image Copyright: Author.
Visibility
Visibility was an important attribute, especially for the ED department. Staff noted that the nurse station size and form affected visibility toward psychiatric patients. The registration staff noted that the wide registration area with inadequate security staff in the evenings is a security concern. The lab department staff considered the open workstation design a positive attribute, improving visibility and communication among staff and managers.
Flooring quality
The bedded care staff noted the need to replace the corridor carpet in a few years, when obsolete, with a hard surface—luxury vinyl tile to improve infection control outcomes (Figure 7). Staff recommended flooring quality improvements that included removing stains and cracks, improving exterior flooring quality, and installing waterproof material without gaps. Such improvements needed the dismissal of short-term costs to satisfy infection control guidelines and patient safety.

Carpets were recommended to be replaced due to infection control concerns. Source: Image Copyright: Author.
Improve cleanliness, aesthetic conditions, and temperature
The hospital needed updating, cleaning, and modernization to improve staff recruitment, visitor perception, safety, and conformance to the current healthcare architectural style. Staff found that departments were “antiquated” and reflected the need to remodel and replace dark floorings and walls (Figure 8). For example, a staff described: “the hospital should not look old. We need to improve the flooring and waiting rooms and facelift things. Landscaping needs attention: the parking lot needs to be kept up, and visual needs to improve.” The hospital’s physical environment attributes and ambient conditions influenced staff recruitment and retention. One of the outpatient clinic staff mentioned: For recruitment, the Hospital should not look old, including flooring, waiting rooms, face-lift things. Landscaping needs attention, the parking lot needs to be kept up, and visual needs to improve.

Staff recommended replacing and enhancing the ambient condition of the emergency department by replacing the dark floors and colors. Source: Image Copyright: Author.
Reduce noise and improve privacy
Smaller departments and insufficient workspaces resulted in a perception of a noisy environment impeding performance, especially for ED and surgical staff. Privacy concerns for patients and staff were vital for physician dictation rooms, phone call rooms, triage rooms, check-in areas, registration, and patient bays. Several clinicians mentioned adding doors to the bays or private patient rooms in the ED to improve patient privacy (Figure 9). The ED and surgical staff reflected that the curtain between beds was insufficient for patient privacy. Patient privacy was also essential for registration-check-in staff, as one staff noted: “we need something better for patient privacy instead shouting information out to everyone.”

The small preoperative bays impeded patient privacy. Source: Image Copyright: Author.
Discussion
Previous studies have shown the close relationship between rural hospital physical environment and perceptions of cleanliness, quality, and safety of care, staff retention, access to care, confidentiality, or operational efficiency (Cai et al., 2017, 2019; Haddox, 2018; Pati, Gaines, & Valipoor, 2016). The primary reason driving this study was to evaluate staff’s perception of current obstacles and needs of the infrastructure, physical environment attributes, and ambient condition of a CAH and how they are connected to potential outcomes.
In alignment with previous studies (Cai et al., 2017; Haddox, 2018; Pati, Gaines, & Valipoor, 2016; Pick et al., 2021), participants mentioned the need for rightly sized spaces, functional needs, pandemic needs, and improved access. Inadequately sized departments and spaces influenced technology integration, patient satisfaction, visitor experience, care delivery, patient flow, cost, and safety outcomes. Staff described the importance of rightly sized ORs and SPD to accommodate efficient flow, tray stacking, and technology integration that has been previously noted (Pati, Gaines, & Valipoor, 2016). This finding applies to designers and planners. We recommend that future studies explore short-term and long-term flexibility approaches to solve variable healthcare demands in rural regions.
Team rooms and adequately sized workstations were critical elements for staff satisfaction outcomes. The inadequately sized patient bays or rooms affected staff movement, performance, or teamwork. In line with prior literature (Naccarella et al., 2019; Zamani, 2019), clinical staff requested adequately sized nurse stations that support patient visibility, team communication, and privacy for clinicians. The need for private and enclosed rooms for dictation and private team discussions is a noteworthy recommendation pertaining to designers and planners.
Findings highlight the need for leveraging unused CAH spaces for departments in need of more space. This result again suggests that designers and planners design modular spaces functioning during unused hours or conditions for high or unpredictable volume departments. Staff explained the importance of providing adequate spaces and department adjacencies aligning to the patient, visitor, and staff needs to improve efficiency, access, patient experience, patient privacy, or operations that have been documented in previous studies (Cai et al., 2017; Pati, Gaines, & Valipoor, 2016). Participants also suggested that consolidating multiple outpatient clinics would reduce operational costs and improve communication. However, the consolidation of outpatient clinics raises the question of adequately distanced and accessible healthcare facilities for rural communities that need further evaluation by policy makers and hospital administration.
Staff reflected on the ADA accessibility issues hindering wheelchair access for bathrooms in various departments reported in prior studies (Pati et al., 2016). Noteworthy for CAH administrators and facility managers, the findings reflect the need for improved floor quality, floor type, exterior ground elevation, slopes, and adjacency between departments to improve visitor access and staff efficiency. The inadequate size of departments and rooms resulted in cluttered hallways, nurse stations, or ORs found in prior studies (Pati, Gaines, & Valipoor, 2016). Clinical staff pointed out the need for relocating old technology before adding newer ones to reduce clutter in hallways, equipment damage, or flow disruptions. Future studies are recommended to explore the adequate size and number of storage spaces for different departments in CAHs.
Concurrent with previous studies (Naccarella et al., 2019; Pati et al., 2016b; Zamani, 2019), staff expressed safety and security associated with multiple entrances, inadequate security stations and staffing, and visibility concerns. Further, the results suggest that the ED waiting room be open for visibility and with divisional transparent walls to reduce infection transmission. There is a need for further exploration to address security and safety implications for CAH that may be associated with different entrances or visibility concerns arising for older infrastructures with limited structural spans. The results are pertinent for future planning and design considerations.
Flooring quality and type were perceived as integral components for reduced infections, noise, or improved patient accessibility, which aligns with previous studies (Dixit et al., 2019). These findings highlight the need for life-cycle analysis protocols for CAH’s administrators in selecting flooring types for justifying higher initial cost installation for better quality floorings. In agreement with prior studies (Cai et al., 2019; Pati, Gaines, & Valipoor, 2016), staff emphasized the importance of exterior and interior aesthetic conditions, positive distractions for staff recruitment, and patients’ experience outcomes. This is an imperative recommendation for interior designers and hospital leaders in the process of future renovation or construction of CAHs.
Staff expressed improving patient privacy in registration, waiting, and patient bays as crucial concerns expressed by staff. Several studies (Haddox, 2018; Pullmann et al., 2010) point out a correlation between patients’ need for privacy in rural hospitals and the rural population’s lower income and poor access to insurance. The finding applies to hospital administrators, clinicians, designers, or planners. Staff noted the importance of private and enclosed patient rooms to reduce the risk of airborne infection transmission, as suggested in prior literature (Dancer, 2021; Pati et al., 2016a). Nevertheless, some research proposes the importance of privacy curtains to provide a direct line of sight to patient bays for effective patient monitoring and to prevent adverse events (Nurses Association of periOperative Registered Nurses, 2005). As an alternative, recent design interventions include a remote patient monitoring system to ensure quality patient care, efficient staff allocation, and protect patient acoustical privacy (Axis Communication, 2017). This result raises the need for reevaluation of open curtain bays versus closed patient rooms in the context of CAHs, depending on patient types and the requirement for monitoring.
COVID-19 Pandemic Findings
The study yields new information for policy makers, designers, or hospital administrators on the impact of the COVID-19 pandemic on the CAH design and physical environment needs. The importance of exterior and interior spatial adjacencies was a significant safety concern. Staff emphasized the importance of decontamination equipment spaces, access to main roadways, and controlled entrances for contaminated patients for the ED entrance.
The pandemic affected the concept of waiting rooms across different healthcare facilities. ED waiting rooms in this study were divided into smaller sections or isolated areas to reduce the risk of infections (Hollander & Sharma, 2021; Pick et al., 2021). Accordingly, ED staff in this study reported a higher sense of safety with waiting room divisions corresponding to patient acuity and risk of infection transmittals. However, these partitions impeded visibility. Visibility is crucial for ED waiting room security and safety outcomes (Pati, Pati, & Harvey, 2016; Tresenriter et al., 2021; Zamani, 2019). Therefore, staff suggested dividing waiting rooms with transparent partitions to ensure patient segregation and sustain staff visibility. Future studies are recommended to explore creative strategies for designing waiting rooms segregating infectious patients, supporting wayfinding, and sustaining the security and registration staff visibility.
In addition to waiting room spatial alterations, the COVID-19 pandemic enforced virtual platforms and applications that reduced the need for waiting rooms, which has been reflected in recent publications (Hollander & Sharma, 2021; Pick et al., 2021; Tresenriter et al., 2021). Aligning with previous studies (Butzner & Cuffee, 2021; Goldberg et al., 2021; Pick et al., 2021; Wang et al., 2021), these results suggest the successful application of telehealth services to improve primary care access for the rural community by reducing the direct and indirect costs to patient (travel cost and time).
This finding pertains to CAH policy makers and leadership. Nevertheless, telehealth implications during the pandemic were a challenge for older generations that aligns with recent literature (Goldberg et al., 2021). Administrative staff used phone calls or on-site parking screening to overcome this challenge. Future studies must evaluate how technology integrations may benefit the CAH waiting experience or access to care.
Limitation
It should be emphasized that this study is exploratory, and all interpretations and recommendations are based on the reported experiences of the CAH staff. Therefore, any recognized correlation may not be generalizable due to the small sample size. However, future studies may confirm some of the identified issues for CAHs to develop meaningful implications for policy makers, managers, planners, architects, or interior designers. Future research may identify additional challenges that have yet to be realized in the current article. The need for increased space size may have resulted from a deficient operational model or an outdated inventory management system rather than a space planning issue. This aspect of the evaluation was not explored in the current study. Thus, future studies are recommended to explore the relationship between effective operational models and satisfaction with space size. Further, systematic observations and studies with more representative samples may contribute to corroborating the findings of this study. Further studies are suggested to explore the perspectives of patients and families.
Conclusion
The findings from this exploratory study provide evidence that the facility, physical environment qualities, and ambient conditions of the CAH affected staff perceptions of safety and quality outcomes. Staff expressed that overcoming these shortcomings is imperative for improving infection control compliance, patient safety, equipment safety, staff safety, staff flow, performance, satisfaction, experience, comfort, and reduced costs. Study data inform designers, planners, interior designers, clinicians, CAH administrators, and leadership on critical physical environment qualities that improve quality and safety outcomes. A larger sample involving more CAHs in multiple regions can propose more generalizable findings. Architects and planners are encouraged to design CAHs that are convertible and scalable depending on patient volume and staff needs. Furthermore, the future strength of CAHs depends on the capability to organize and invest in programs and technological platforms that improve access to care, specialists, and wellness visits for rural communities.
Implications for Practice
Flexibility is essential for planning and designing CAHs that expand or alter depending on functional needs and patient volume.
Leveraging technology integration into the CAHs work system improves patient access to care and reduces waiting room crowding.
Consider parking and exterior spatial flexibility, size, and adjacency to interior spaces to improve disaster management and access.
Providing adequate space for teamwork, private documentation, and focus time is essential for staff performance and satisfaction.
Improve acoustical privacy in patient bays, patient rooms, and registration areas to enhance the quality of care, infection control, and patient privacy compliances.
Footnotes
Acknowledgment
The author would like to acknowledge Monte Hover, Kristen Rickord, and Adam Fateley for their contributions to this facility planning project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.