
Abstract
Objective:
Translational research to advance design criteria and apply the Childbirth Supporter Study (CSS) findings to practice.
Background:
The physical design of birth environments has not undergone substantial improvements in layout or ambiance since the initial move to hospitals. Cooperative, continuously present childbirth supporters are beneficial and are an expectation for most modern birth practices, yet the built environment does not offer support for the supporter.
Methods:
To advance design criteria, we use a comparative case study approach to create translational findings. Specifically, CSS findings were used as indicators to advance the Birth Unit Design Spatial Evaluation Tool (BUDSET) design characteristics in pursuit of better support for childbirth supporters in the built hospital birth environment.
Results:
This comparative case study provides eight new BUDSET design domain suggestions to benefit the supporter-woman dyad, and subsequently the baby and care providers.
Conclusions:
Research-informed design imperatives are needed to guide the inclusion of childbirth supporters as both a supporter and as an individual in the birth space. Increased understanding of relationships between specific design features and childbirth supporters’ experiences and reactions are provided. Suggestions to enhance the applicability of the BUDSET for birth unit design facility development are made, specifically ones that will better accommodate childbirth supporters.
Keywords
Introduction
There are well-recognized benefits for both mother and baby when the woman receives support from a chosen birth companion as reflected in Cochrane reviews (Bohren et al., 2017; Hodnett et al., 2013) and by the World Health Organization (WHO, 2020), yet we claim a dichotomy in current birth environment design exists which does not reflect this knowledge. While in most resource-rich nations, a continuous supporter is expected to accompany the woman throughout her labor and birth experience, the supporter is usually not well accommodated in the birth space (Johansson et al., 2015, Minnie et al., 2018) and subsequently may be unable to function effectively in their support role.
In their role, supporters often feel overwhelmed, anxious, or uncertain (Gawlik et al., 2015). Although recent design guidelines show an awareness of supporters’ importance, it appears supporters have been overlooked when it comes to birth environment design (Harte et al., 2016).
Hospital culture, sociocultural and material/technological context are interwoven influences (Maffi, 2016) affecting this claim. Healthcare settings are inherently complex spaces that provide endless challenges for designers to accommodate all necessary delivery of care components (van Hoof et al., 2015). Within architectural and design practice, the demand for efficient execution of each commission allows few opportunities for user-based research (Andrade et al., 2012); therefore, it is important that rigorous research findings are regularly incorporated into design practice.
Design assessment tools, akin to guidelines, are both embraced and resisted by practitioners who dislike the prescriptive “checklist” approach while also needing to incorporate the latest best-practice evidence-based design knowledge into their project within the budgeted time frame (Brambilla et al., 2019; Moore et al., 2015). This tension of bringing evidence into practice is an ongoing effort and opportunity for improvement on the part of environment design behavior researchers, as well as for many other design and architectural fields (Forsythe, 2018). We join others to claim evidence-based design is a key design process for childbirth environment design, especially for patient comfort and reducing stress (Brambilla et al., 2019; O’Callaghan et al., 2019).
Aim
The aim of this comparative case study is two-fold: (1) to present research-informed design principles developed from the video-ethnographic Childbirth Supporter Study (CSS; Harte et al., 2016) and based on the comparison of these results (2) to discuss and suggest refinements to the Birth Unit Design Spatial Evaluation Tool (BUDSET version October 2, 2010), the leading assessment tool for physical birth environments to better reflect the needs of childbirth supporters in hospital contexts.
The Study Case Setting and Context
The research presented here is a comparative case study, which will be explained further in the Method section. The two cases compared are the CSS (Harte et al., 2016) and the BUDSET (version October 2, 2010; Foureur, Leap, et al., 2010; Foureur et al., 2011). The CSS is an empirical study conducted as part of a doctoral dissertation (Harte, 2015), while the BUDSET is both a conceptual and empirical pilot research study (Foureur, Leap, et al., 2010; Foureur et al., 2011). Both CSS and BUDSET occurred in Australia between 2011 and 2016, while the comparative case study research presented here, which is both empirical and theoretical, occurred between 2015 and 2022.
We draw on research into the experiences of childbirth supporters from the CSS (Harte et al., 2016) to initiate discussion around the inclusion of supporter needs in birth environment design. We use the BUDSET as a second case to compare the CSS results to, as a technique for improving the BUDSET, with the goal of facilitating improved experiences for childbirth supporters. We refer to Version 2.0 developed in 2010 throughout this article. For an abbreviated BUDSET, see Table S1 in the Online Supplements.
To lay the groundwork for the comparative case study, we first provide a brief background of childbirth supporters in the designed birth space, the theoretical framework and the methods used for the CSS, and an overview of the BUDSET before turning our attention to the comparative case study.
Supporters in the Designed Birth Environment
Supporters, for this research, are defined as untrained companions from the woman’s personal network (Harte, 2015). Professional supporters may also benefit from the results presented here, however; they are not the focus. Birth supporter’s roles include many activities, including physical comfort and touch (for instance, massage, wiping the woman’s forehead, holding her hand, providing ice chips/water; Johansson et al., 2012). Psychological and affective support (both overt and covert) are equally important, including verbal encouragement, eye contact, and active listening and positive response to expressions of pain or fear the woman may convey (Johansson et al., 2012).
The softer aspects of care can be facilitated with reimagined birth spaces harmoniously rich with sensory, color, and light/dark patterns that foster a supportive atmosphere (Balabanoff, 2017). A range of accommodation types enable the supporter to regulate their participation type and level, with confidence in assisting at the birth, as shown in the scoping review of eight crucial building spaces in maternity care (Setola et al., 2019).
Theoretical Frameworks
As this comparative case study is centered on the CSS as a central axis, or case, the following briefly describes the CSS theoretical framework and analysis technique. The theoretical underpinnings, methods and research design for CSS are described in detail in related publications (Harte et al., 2017; Harte et al., 2014). The CSS comprises ethnography (as both a research collection technique and as a theory), “birth territory” theory (Fahy et al., 2008; Fahy & Parratt, 2006), and the “safe, satisfying birth” hypothesis (Foureur, Davis, et al., 2010) to support the data collection method, while symbolic interactionism (Blumer, 1986; Prus, 1996) and a thematic coding approach informed by both Saldaña (2013) and the activities, environment, interactions, objects and users (AEIOU) framework originally developed by Wasson (2000) guided the data interpretation.
The above-described theoretical framework grounds the CSS and supports the process for the comparative case study, while the comparative case study adopts the additional theoretical framework of critical theory. Broadening the view of each case to include the phenomena in question—how better to support childbirth supporters in the design environment—the comparative case study attends to power and inequality, informed by Marxist, feminist, and critical race theory (Bartlett & Vavrus, 2017). Questioning the evidence with a “meaning-making,” theoretical stance is a hallmark for the comparative case study approach, as it facilitates both an unbounded frame and active iteration to progress the complex field of birth environment design.
Case 1: The Childbirth Supporter Study
This and the following section describe the cases compared. The first case is the CSS and the second case is the BUDSET. The CSS is a video-ethnographic case study of one family’s experience. This included eight participants (one woman, her partner and three family supporters, plus three midwives), 1-hr of video footage from 15 hr of labor, observational field notes, and five postnatal video-cued interviews. CSS is a substudy of the larger birth unit design (BUD) study conducted in hospital birth units in Australia between 2011 and 2015. Both studies received ethical approval (HREC/10/HAWKE/135 and SSA/10/SG/190).
The CSS study was a focused, short-term ethnographic study that used thick description to provide sufficient evidence and context for the “reader to evaluate the extent and truth of the phenomenon under investigation and how it may resonate with other environments, circumstances, and people (Lincoln & Guba, 1985)” (Harte et al., 2016).
Video-ethnography is an ethnographic technique that uses video of the participants engaged in the experience in question to observe complex lived experiences (“the data”), which then enables deeper reflection on the part of the participants and the researchers. In the CSS study, the video-reflexive ethnographic data collection consisted of unobtrusive labor recording, followed by postpartum interviews conducted while viewing the footage, to explore the participants’ experiences and the meanings they attribute to their experiences in the designed space. The participants were invited to view the video, being aware of the researcher’s intention to activate a reflexive process.
In the CSS study, reflexivity was practiced in two shared but different ways by the researcher and by the participants. Reflexivity is a process of stepping back from the data to view it with a personal recognition as to one’s place in the experience to enable the data to be interpreted in a systematic and layered way (Darawsheh, 2014; Palaganas et al., 2017). The researcher practiced a reflexive stance with an aim to gain honest and open assessment of multiple aspects, for instance, their personal station and values, while the participants were also invited to practice a reflexive stance in the act of watching the video—to interpret their actions based on multiple aspects, for instance, their memories and feelings as well as novel observations.
All CSS study participant names are pseudonyms. Felicity, the woman in labor, aimed for a natural, unmedicated labor. Felicity’s mother, Frances, acted as her main supporter for most of the labor. Although Frances acted as Felicity’s main supporter, Felicity’s partner, Martin, was available as needed to provide support. Felicity’s two sisters also occupied the birth environment and provided support in varying (lesser) degrees. Three midwives present at various points of the labor provided contextual evidence to facilitate ethnographic understanding.
Three themes were identified in the CSS analysis: an “unbelonging paradox,” “role navigation,” and “supporting the supporter” (Harte et al., 2016). Eight subthemes characterize these three themes as seen in Harte et al. (2016). Design characteristics to facilitate optimal BUD have previously been proposed in the BUDSET (Foureur, Leap, et al., 2010; Foureur et al., 2011; Sheehy et al., 2011). We will now provide further contextual background for BUDSET.
Case 2: BUDSET
An important research component that supported the development of the CSS was the presence of a physical birth spatial design audit tool, the BUDSET. The original BUDSET tool serves as the second case for this comparative case study report. Upon completion by birth unit caregivers, staff, designers, or related people, the BUDSET enables a valid and reliable audit of physical childbirth environments in terms of the quality of the built spaces, including the objects within them, specifically from the perspective of a target group of women’s experiences.
It may clarify the relationship between BUDSET and the CSS findings to picture the entire birthing journey as both a series of physical movements through physical space, as well as a psychological journey outside of space (and time) for the woman and her supporter(s). Optimally, the woman and her chosen supporter synergize as a cooperative dyad.
The BUDSET has four domains, which serve to assess design factors contributing to the “fear cascade” cycle (Stenglin & Foureur, 2013), including the attributes of “facility,” “aesthetics” of the space, and “support” for family and friends (Foureur, Leap, et al., 2010). These domains are comprised of 18 characteristics—the design principles.
Results of a pilot test indicate that the BUDSET is a viable tool for “assess[ing] the optimality of birth units…[and to] determine which domain areas may need improvement” (Foureur et al., 2011, p. 36). Other studies confirm content validity for the original target group of women, while proposing the opportunity for refinements to better reflect the experiences of diverse groups, midwives, and supporters (Menke et al., 2018; Sheehy et al., 2011).
Comparative Case Study Methods
The research presented here uses the comparative case study approach (Bartlett & Vavrus, 2017), an empirical approach to making extended meaning of two or more cases. We present, framed with theory, the relationship of the CSS findings as compared with the BUDSET design recommendations. Similarly, the BUDSET is compared to the CSS to demonstrate the relevance, applicability, and validity of the CSS study.
The strength of the comparative case study method is the ability for the researcher to attend to simultaneous and overlapping axes, as described by Bartlett and Vavrus (2017). Specifically, the “horizontal, which compares how similar…phenomena unfold in locations that are connected and socially produced; vertical, which traces phenomena across scales; and transversal, which traces phenomena and cases across time” (p. 15). It is important to understand the need for context to not be solely defined “as place or location, but…should rather be conceptualized as something spatial and relational” (p. 15).
Additionally, the comparative case study method “eschew(s) a static, bounded notion of culture in favor of a view of culture as an on-going, contested production” (Bartlett and Vavrus, 2017, p. 15). This method supports the extension of an existing spatial evaluation tool via comparative superimposition of ethnographic results. The comparative case study method as promoted by Bartlett and Vavrus works in an iterative way to trace relevant and contingent actors, both human and nonhuman, to achieve “a sense of shared place, purpose, or identity with regard to the central phenomenon” (p. 10), which in our case is the support of childbirth supporters in the designed environment.
Analysis Process
As there are important design practice suggestions (also called design imperatives) revealed by the CSS, so too design imperatives are also included as the spine of the BUDSET. The comparative case study approach was conducted using a line-by-line comparison of all CSS findings, as reported in Harte et al. (2016), overlayed directly to each BUDSET characteristics. The aim was to authenticate fit, utility, validity, reliability, rigor, and trustworthiness for both cases (Miles et al., 2018), as meaningful to design scholars, childbirth design evidence-creation, and design practitioners.
Because BUDSET was developed prior to the CSS study, there is a gap we argue should be addressed, to strengthen BUDSET by more completely including the needs of childbirth supporter(s). The BUDSET characteristics are evident in the CSS findings, as the CSS findings also demonstrate the relevance of the BUDSET characteristics. Each component of each data set (BUDSET and CSS) was taken in turn and compared to each of the other set of components by the first author and later verified as accurate by the coauthors. Narrative examples of this process follow in the Findings section.
The complete comparative case study is presented in Table S2 as a online supplementary file, as a technique to demonstrate the iterative suggestions to better include supporters within the existing BUDSET, Version 2.0. All 18 BUDSET domains are stated, followed by CSS findings to highlight supporters’ needs within the design as related to the BUDSET characteristic. The degree to which the BUDSET characteristics are reflected within the CSS study are indicated as either strong, mixed, or limited to the degree in which the listed items were relevant and matched to the CSS participants’ experience, either as example or as counter example. For instance, if the ability to adjust lights is a BUDSET characteristic, and this ability was absent but desired by the CSS participants, it is listed as mixed.
The analysis highlights BUDSET aspects that account for supporters, and areas where the CSS suggests a need for development of supporters’ design-related needs. First, we provide contextual information about BUDSET, followed by two examples of how design elements participated in the childbirth supporters’ experiences.
BUDSET Domains Related to Supporters
One further proviso, before describing examples, is that a person’s perception of their experiences is true for them, while—in the case of supporter’s—this self-perception may not transfer into the most optimal behavior to facilitate labor. This article aims to provide context for suggested future and more nuanced research. A further research question that could be posed is, do design features play a mediating role, or do they have a moderating role in clarifying supporters’ self-perceptions of their activities—while also improving the actual supporter role?
As reported in the CSS (Harte et al., 2016), supporters have two parallel sets of needs: (1) to provide support for the woman and (2) (to have assistance in) managing the physical and emotional demands of their role. Implicated within these two roles, which we call “engaged” and “waiting,” although neither term is exclusive, are both sets of supporter’s needs: to support the woman and to be supported in attending to their own well-being.
With a finer grained comparative case lens, we now examine BUDSET as reflected in the CSS findings while the CSS findings are simultaneously assessed as reflected in the BUDSET characteristics. A few examples are identified to demonstrate this relationship, with design imperatives identified.
Extended Findings as Narrative Discussion
We now offer some descriptive examples to support a revised BUDSET version to better highlight design elements supporting supporters. For succinctness, only a few of the design interventions arising from this study are reported in narrative form. For the complete list of design imperatives, please see Table S2 in the Online Supplements and Table 2.
The first example arises from the CSS, specifically related to the second characteristic of the BUDSET domain “fear cascade,” which is “space: outside.” This characteristic was not mentioned during the CSS interviews perhaps because most of labor took place at night (in the birth room) or within the en suite bathroom. Felicity seemed surprised to “actually ha[ve] a window,” implying that she desired a window and assumed there wouldn’t be one (see Figure 1).

“Space: Outside”—view from window.
The CSS birthing suite didn’t have access to an outdoor area suitable for night use. Visual access to outdoors, via a window view of nature, physical access (such as a healing garden) and/or positive distractors are desirable features of birth units and healthcare settings in general (Andrade & Devlin, 2015; Wang et al., 2019). One midwife reported that other women walk to a nearby green space. Although the midwife speaks about the birthing woman, this sentiment would appeal equally to supporters: The [cricket] oval is where we often send women…there is nice sun…and grass. They…quite enjoy walking out there…But obviously being…night [for Felicity’s labor] it was not an appropriate option…I think [going outside] helps because…maybe [the birthing woman] feels more comfortable in herself and obviously an increase in oxytocin and maybe a decrease in adrenaline.—Veronica—student midwife
The next characteristic in the BUDSET, in terms of the birthing journey, also relates to space, specifically the reception area. The CSS provided few details on the experience of reception spaces by Felicity and her supporters. Optimally, reception is inviting, invokes feeling welcome and facilitates transition. For this birthing journey, after entering the room, Felicity left only once during the 15 hr of filmed labor to briefly walk the halls. Likewise, her mother, Frances, rarely left the birth room. However, Martin, the husband, whose support was passive until the final labor stage, spent considerable time in the waiting area; therefore, he had sufficient experience to report. Although these areas were not included in the video recording, the interview and field notes reveal Martin’s disappointment towards the design of these spaces.
Martin frequently sought confirmation from the midwives at reception that Felicity was “doing okay,” yet it is likely that the midwives couldn’t determine Felicity’s status from their location either; indeed, Martin could have been encroaching on their workspace. Aside from places for supporters to sit, none of the “reception” elements were noted in the CSS analysis, most notably a lack of plants, flowers, or living things. These design features may have been appreciated if they were present, yet it is believed that these elements often remain unnoticed except on a subconscious level (Grinde & Husselman 2022). This may be due to the amount or concentration of plants in a space.
Another aspect of the “reception” characteristic includes spaces for supporters to sit, wait, and eat. Martin felt dissatisfied with the seating, as he was unable to lie down or rest. He felt physically uncomfortable as well as disconnected from Felicity and he had no positive distraction. This area was some distance away (about a 2-min walk), so there was little opportunity for him to be close yet unobtrusive, as he may have preferred.
Martin also noted privacy issues, reporting hearing another family arrive, and soon after, their baby’s cries. He spoke with anxiety about his perception that Felicity’s labor was “taking so long.” His direct role in supporting Felicity, which he had yet to initiate, was limited by the design, as he was not able to rest in preparation for his later active role.
This example reveals design attributes that relate to “engaged supporter by the woman’s side” and more directly to “waiting while caring for self.” It has been demonstrated as important for laboring women to have a sense of privacy (Rados et al., 2015). Ideally, supporters have similar opportunities to choose self-care in a private setting, away from the sights and sounds of others’ birth experiences and also a means to maintain communication and sense of connection.
Martin also outlined the inadequate beverage and snack provisions: they were not familiar or home-like, such as coffee in Styrofoam cups and ill-suited plastic knives to butter toast. This provides strong validation of these BUDSET characteristics (as seen in Table S2 in the Online Supplements), indicating that provision of seating and snacks are the minimum design parameter, with leeway for increased comfort considerations for those waiting a long time. What can be considered reasonable expectations for providing snack and beverage provisions in the design of the space? This is an area that would benefit from more research to further our understanding on how best to design birth spaces regarding supporters’ food and beverage needs.
Limitations
A research limitation was that filming occurred only within the birth room, the en suite bathroom, and the hallway just outside the birth room. Other areas were not filmed, such as the entrance, reception desk, and waiting room. In these locations, observations, field notes, and interviews were used to reveal the experiences of the supporters.
Although the CSS and BUDSET studies both occurred in Australia and may resonate with many readers who are occupied with childbirth environment design, readers should exhibit caution when generalizing these findings to their specific cultural, contextual, and population characteristics.
Additional BUDSET Design Characteristics
Based on the provided design examples, as well as the other design imperatives outlined in Table 1, eight suggestions for additional BUDSET design characteristics are proposed. Within the Fear Cascade Domain, “Space: Birth Rooms,” we suggest adding: Family alcove or window bench seating to provide a space for both togetherness and privacy. Also, for the Fear Cascade domain, either “Space: Birthing Rooms” or “Sense of Domesticity” characteristic should now include “Place for personalization to increase sense of control and familiarization.” For domain “privacy,” another characteristic of the Fear Cascade domain, we suggest including visual and spatial transition area between the public space and the room to psychologically remind people they are entering a new and different space. This could be accomplished with different floor colors and ceiling heights at the entrance.
Design Recommendations From CSS.
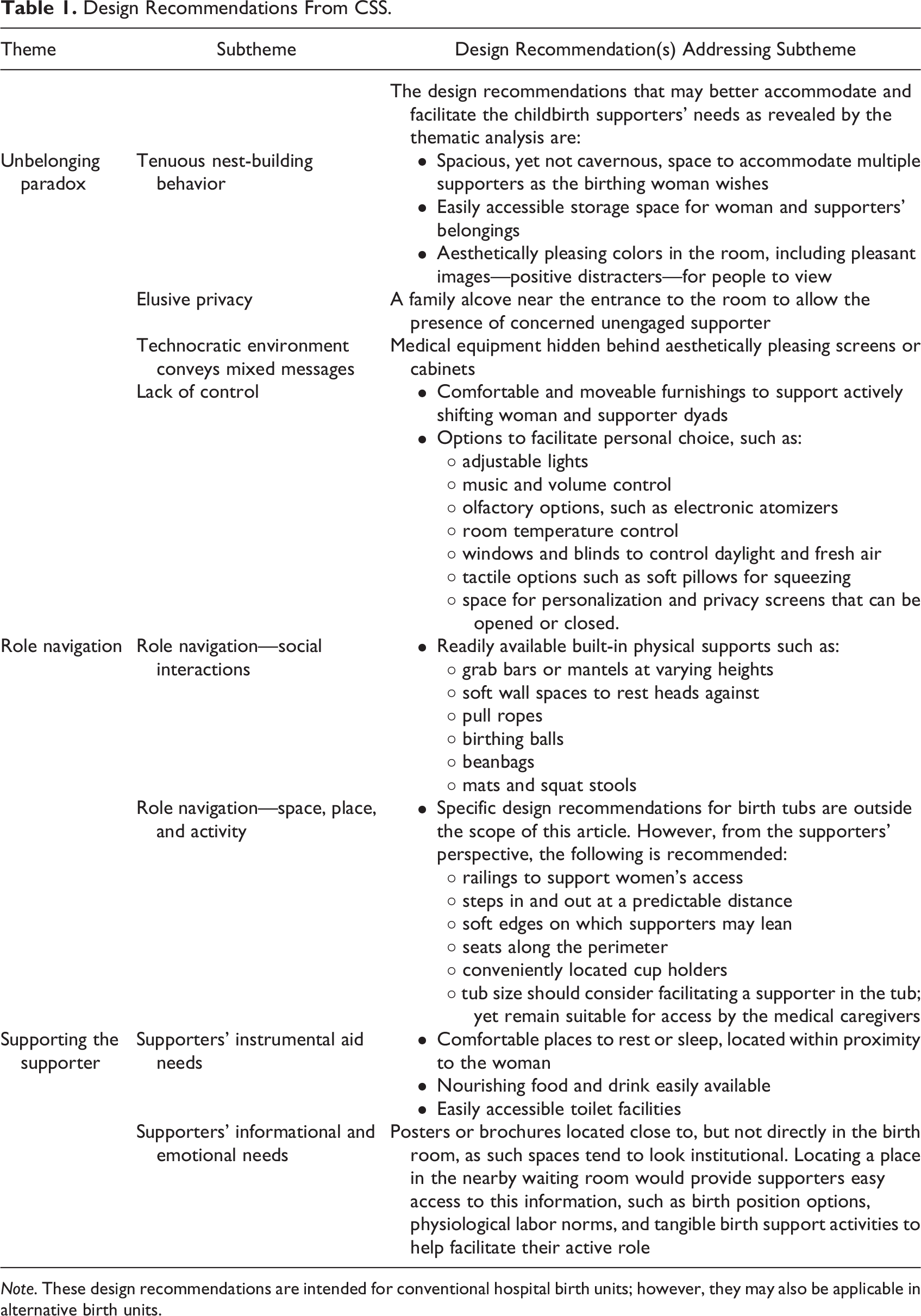
Note. These design recommendations are intended for conventional hospital birth units; however, they may also be applicable in alternative birth units.
Suggested Birth Unit Design Spatial Evaluation Tool Amendments to Facilitate Supporters’ Role.
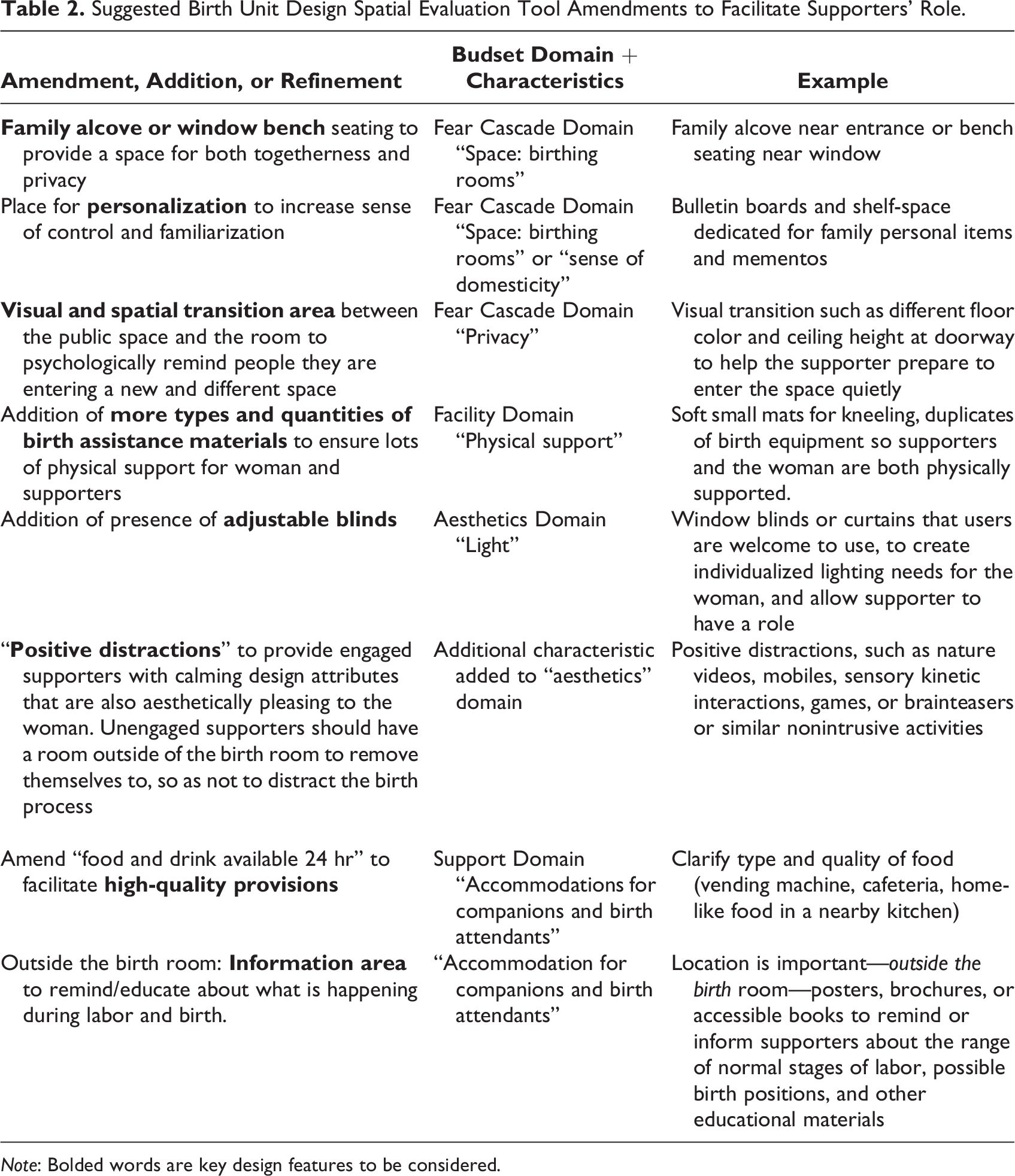
Note: Bolded words are key design features to be considered.
Within the BUDSET Facility Domain, the “Physical Support” characteristic, we recommend the addition of more types and quantities of birth assistance materials to ensure lots of physical support for women and supporters. For the aesthetics domain, “light” characteristic, we recommend the addition of adjustable blinds (operable by the user). We recommend adding to the aesthetics domain a new “positive distraction” characteristic to provide supporters who are not engaged in an active role with design features that reduce supporters’ stress by creating positive interest within the room. This must also be done in a way that is beneficial for the woman. Relatedly, we also recommend creating an alluring nearby waiting room to provide unengaged supporters a means to leave the birth room if they are not actively supporting the woman. For support domain, “support” characteristics, we have two recommendations, the first is to amend “food and drink available 24 hr” to facilitate high-quality provisions. The second is to add an informational area, such as a bulletin board, to remind/educate about what is happening during labor and birth—but only outside of the birth room as educational information areas are considered aesthetically institutional. The suggested amendments to better facilitate supporters roles within BUDSET are shown in Table 1.
Conclusion
With these examples from the comparative case study analysis coupled with the complete results in Table S2, we identify an overarching message symbolically communicated by the designed environment. Specifically, we sense a cultural belief expressing that the supporter, like the woman, is perceived to be a patient in the hospital in terms of how the designed environment supports the supporter. There is a commonly held belief among design/midwifery researchers, that birth is a normal physiologic activity, one that is a normal human activity and not an illness or injury. However, despite only the woman in labor having been admitted to the hospital for childbirth, the entire dyad or group are symbolically grouped into “patient” status. This often equates to feeling disempowered and under supported by the space.
Currently, the BUDSET instrument frames supporters as mostly passive participants in childbirth. Within BUDSET the supporters’ section is a standalone “characteristic” located in the final section and with a single appearance in the “Facilities Domain: Physical Support” and “Fear Cascade domain: Space: Reception” sections. The supporters’ sparse appearance in this version conveys the message that supporters are “add-ons” to the birth experience. We take a different position: supporters are integral to the woman and the birthing journey and should be supported in this role from the beginning and throughout labor especially within the physical space. Throughout the BUDSET tool, the supporter role should be integrated, to complement the appropriate focus on the woman.

Room showing monotone colors, institutional aesthetics, medical equipment, and lack of textural variety.

Room showing monotone colors, institutional aesthetics, medical equipment, and lack of textural variety.

Room showing monotone colors, institutional aesthetics, medical equipment, and lack of textural variety. However, note the pillows that were brought from home provides some familiarity.
Moving Forward: Amplify Childbirth Supporters in BUDSET
The BUDSET has been validated for the birthing woman as the assessment focus but has not been examined for supporters nor—it is important to note—was it originally developed with them in mind. The focus of this article is to elucidate BUDSET’s efficacy and provide suggestions for improvement in terms of supporters’ experiences and to translate CSS results into design practice. Based on this discussion, most BUDSET characteristics, although designed to measure the birth space with the woman as the focal point, are also relevant to supporters’ experiences. We propose that the description of supporters’ needs primarily limited to one domain (“Support” domain) is insufficient to address supporters’ needs. The research findings presented here reconfirm that BUDSET is an appropriate means to determine birth environment optimality for the woman as the focus. However, it is recommended that measurement refinements for the BUDSET are made to facilitate supporters’ needs in filling their roles.
The CSS findings are shown to be valid when compared to BUDSET as all thematic results were identified as exhibiting BUDSET components. When reflected upon BUDSET, the CSS findings highlighted that more than half of the BUDSET domains were congruent to meet supporters’ needs within the physical birth environment.
The comparative case study revealed domains that did not address supporters’ needs, and therefore two new domain sets are recommended. Supporters have overlapping needs: (1) “as supporter” and (2) “as an individual.” The BUDSET domains address the supporters’ needs as an individual but lack support for them as active supporters. With the addition of these two proposed domain sets, BUDSET could better integrate supporters’ needs in its entirety, without any reduction to the level of support the birthing woman would receive by the built space. Table 1 shows recommendations for a suggested updated BUDSET.
The BUDSET includes features to support childbirth supporters that were also revealed in the CSS findings, for instance: access to food and drink, access to toilet facilities, aesthetic features, and noise control and privacy. However, there are identified needs of the supporters that were absent in BUDSET as indicated throughout this article and in Table S2. We identify BUDSET amendments and design recommendations via both the original CSS analysis (Harte et al, 2016) and in this study as located in Table 1.
To establish BUDSET’s validity for assessing supporters’ needs in the built birth space, this article identifies eight suggestions related to five of the BUDSET characteristics. These design recommendation refinements, when implemented in practice, may improve the ability for the BUDSET tool to assess the physical birth environment’s influence on the childbirth supporter(s), while also improving the assessment from the perspective of the birthing woman.
Implications for Practice
Research-informed design imperatives to guide the inclusion of childbirth supporters as both a supporter and as an individual.
Foster understanding of possible relationships between specific design features and childbirth supporters’ experiences and reactions. Enhance the applicability of the BUDSET for BUD facility development, specifically when also accommodating childbirth supporters.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231177304 - Application of the Childbirth Supporter Study to Advance the Birth Unit Design Spatial Evaluation Tool
Supplemental Material, sj-pdf-1-her-10.1177_19375867231177304 for Application of the Childbirth Supporter Study to Advance the Birth Unit Design Spatial Evaluation Tool by J. Davis Harte, Athena Sheehan, Susan Stewart and Maralyn Foureur in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-2-her-10.1177_19375867231177304 - Application of the Childbirth Supporter Study to Advance the Birth Unit Design Spatial Evaluation Tool
Supplemental Material, sj-pdf-2-her-10.1177_19375867231177304 for Application of the Childbirth Supporter Study to Advance the Birth Unit Design Spatial Evaluation Tool by J. Davis Harte, Athena Sheehan, Susan Stewart and Maralyn Foureur in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-3-her-10.1177_19375867231177304 - Application of the Childbirth Supporter Study to Advance the Birth Unit Design Spatial Evaluation Tool
Supplemental Material, sj-pdf-3-her-10.1177_19375867231177304 for Application of the Childbirth Supporter Study to Advance the Birth Unit Design Spatial Evaluation Tool by J. Davis Harte, Athena Sheehan, Susan Stewart and Maralyn Foureur in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.