
Abstract
Background:
Physical surroundings of healthcare facilities are suggested to influence young patients’ well-being and hospitalization experiences.
Purpose:
The current research seeks to understand young patients’ views and perspectives of the hospital lobby and inpatient rooms. Thus, a qualitative study was carried out in a social pediatric clinic for young patients with disabilities, developmental delays, behavioral problems, and chronic health conditions, that is undergoing reconstruction.
Method:
Operating from a critical realist position, the study employed arts-based methods in conjunction with semi-structured interviews. The data were explored by employing thematic analysis.
Results:
37 young people between the age of four and 30 years participated in the study. The analysis illustrates that the built environment should contain comforting and joyful elements, while enabling patients’ autonomy. The ideal lobby was depicted as open and accessible and an ideal patient room as practical and adapted to personal needs.
Conclusion:
It is suggested that disabling and medicalized spatial arrangements and features may restrict young people’s sense of control and autonomy, while possibly posing a barrier to a health-promoting environment. Large and open spaces with comforting and distracting features are cherished by patients and may be embedded in a comprehensive, yet simple overall design and structural concept.
Keywords
Most people in Western society visit healthcare facilities at some point in their lives. Our societies are constantly adapting to the complex requirements of modern public health. For instance, changing healthcare demands from acute to chronic illnesses in younger populations has led to rethinking practical standards in health-related fields (Perrin et al., 2014). In addition, theoretical advancements in health sciences shifted the focus from physical to mental and more complex conditions. This progress prompted the development of holistic care models. Concurrently, hospital designs have become relevant in maintaining patients’ well-being (Gaminiesfahani et al., 2020).
Supportive Design and Psychosocial Effects of Hospitalization
Patients tend to characterize their associations with clinics negatively, reporting hospital fears (Andrade & Devlin, 2015). Specifically, children’s and adolescents’ hospitalization experiences can be demanding due to concerns related to pain and loss of autonomy (Bsiri-Moghaddam et al., 2011). Patients’ health is considered to be affected by design elements and spatial structures. For example, a lack of exposure to natural light or loud noises may increase stress and anxiety, cause headaches, and contribute to poor sleep quality (Schweitzer et al., 2004). Ulrich (1991) suggested that a supportive design helps patients handle the stress of hospitalization. A supportive design includes a sense of control, social support, and positive distractions (Andrade & Devlin, 2015). Enabling choices in the surrounding elements, such as lighting and entertainment systems, can provide a sense of control (Peditto et al., 2020). Positive distractions, including access to nature, may reduce stress and provide comfort (Ulrich, 1991). Several studies indicated that nature-related design elements (e.g., pictures of oceans, animal themes) and access to nature (e.g., gardens) are beneficial for patients’ healing processes (Gaminiesfahani et al., 2020). Options to connect with others, including a place for visitors and family members to sleep, promote perceived social support (Peditto et al., 2020).
Hospitalization Experiences of Patients With Long-Term Conditions
Young people with chronic conditions are often subject to hospital visits and stays. They have different hospitalization experiences compared to patients who are only admitted once that could harm their well-being (Pao et al., 2007). Children and adolescents usually share these experiences with family members (Watts et al., 2014). Their contentment can affect the parents’ emotional well-being (e.g., feelings of insecurity) and vice versa (Mayan et al., 2021). Consequently, this influences the treatment success of the therapy (Robinson, 1984).
The framing of a hospitalized young patient as “sick child” opposes normative cultural conceptualizations of childhood (James & Curtis, 2012), which is considered “a time of innocence, play and protection from the negative concerns of the adult world” (Crafter, 2018, p. 65). Thus, there are attempts to “normalize” children’s and young people with disabilities’ hospitalization experiences using different strategies (Anderson, 1981). Efforts of normalization could be palpable in the material surroundings of hospitals, where leisure activities are enabled in different spaces. Playrooms, for instance, evoke a sense of familiarity in the foreign environment (Crafter, 2018; James & Curtis, 2012; McLaughlan et al., 2019; Robinson, 1984).
Environmental Preferences in Different Developmental Stages
Previous research examined the effects of physical surroundings on diverse age groups and patients with various conditions (Eisen et al., 2008). As individuals in different developmental stages have specific needs and abilities, their preferences regarding designs and material environments vary. Children with physical disabilities need accessible playgrounds, while people with visual impairments need landmarks for orientation (Courtney & Keith, 2017). Following Piaget’s theory of cognitive development (Piaget, 1964), researchers highlighted differences in design preferences between infants, toddlers, and early and later adolescents (Cartland et al., 2018; Eisen et al., 2008). Younger children, for example, need space for play, while adolescents rather have space for socializing with others (Cho et al., 2019; Peditto et al., 2020). Indeed, hospitalized teenagers, who are in a transitional period to adulthood, expressed a dislike for childlike environments (McLaughlan & Willis, 2021; Ullán et al., 2012). Whether this holds up for children, adolescents, and adults with multiple disabilities is yet to be determined. In light of developmental differences of patients, designers and researchers need to carefully consider stakeholders’ perspectives when reconstructing healthcare facilities.
Significance
To our knowledge, no study dealing with the clinical environment of people with disabilities in different age groups was conducted in Germany. Earlier research explored the topic predominantly in Commonwealth countries and the United States of America. Based on a universal multipayer healthcare system (including public and private health insurance) offering free healthcare for all, German hospitals are largely publicly funded. Both public and private hospitals are accessible to anyone, allowing for the inclusion of people with a variety of backgrounds.
Following the United Nations Convention on the Rights of Children (1989, Articles 3 and 18) and the United Nations Convention on the Rights of Persons with Disabilities (2008, Articles 4 and 31), it is considered paramount to include the voices of vulnerable groups in research and decision-making processes. Accordingly, study designs and research methods need to consider patients’ abilities and needs. Depending on how developed participants’ communication skills are, for instance, data collection methods need to be adjusted. Younger children may want to draw ideas, because they are unable to express their feelings verbally. Teenagers are cognitively further developed and can discuss more abstract concepts. Therefore, they may be more inclined to speak to interviewers. Thus, different creative methods, such as arts-based research, were put into practice (Angell et al., 2015). Arts-based methods can simplify the dialogue with children or people with disabilities, who are underrepresented in research (Boydell et al., 2012), despite often constituting the target group (e.g., in a children’s clinic). Such methods can empower participants to voice their perspectives, while using familiar and comfortable communication practices (Boydell et al., 2012).
Context and Aim
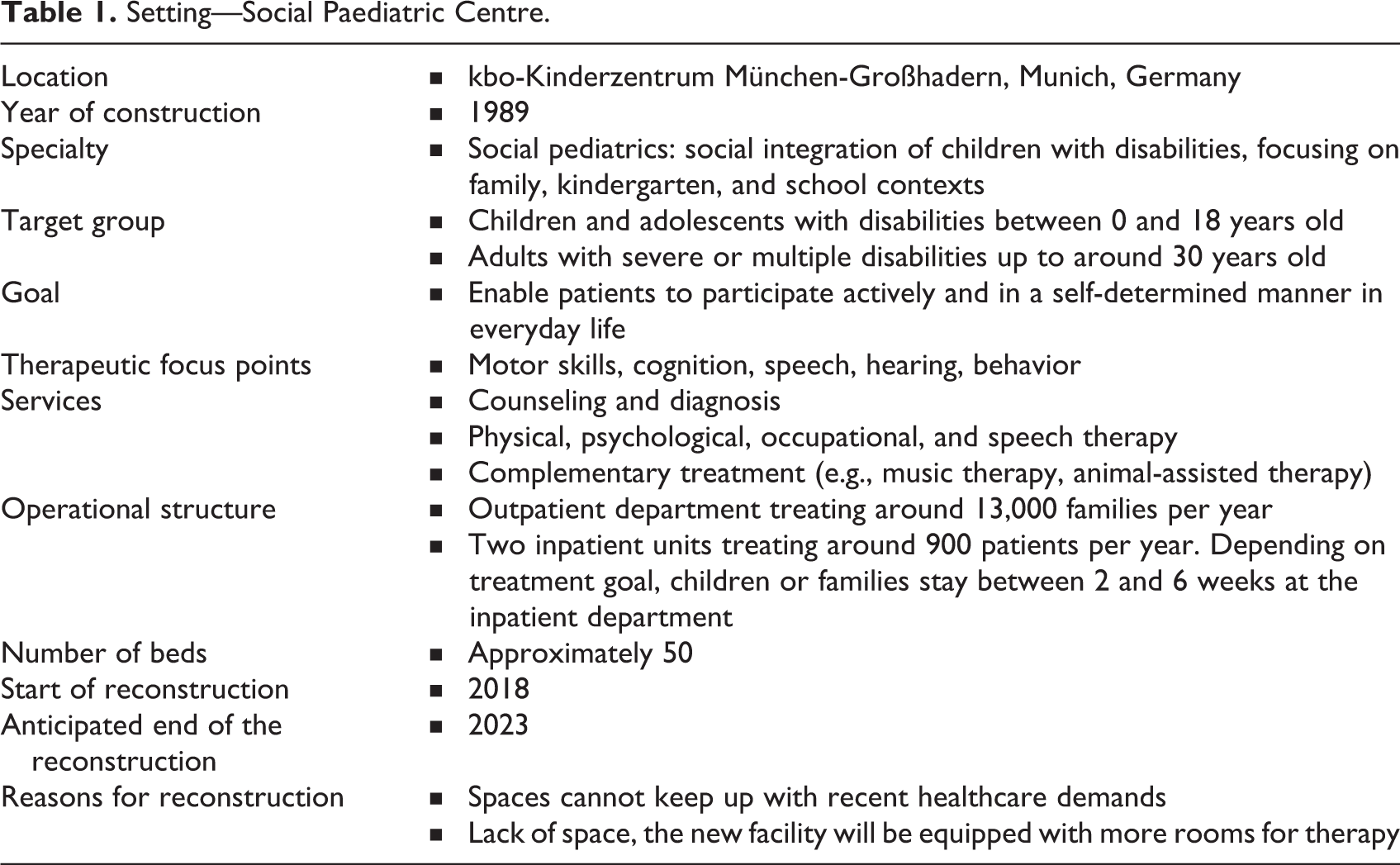
In view of this, a qualitative study was conducted in a social pediatric clinic for young patients with disabilities, developmental delays, behavioral problems, and chronic health conditions in Germany, which is undergoing reconstruction. Details on the clinic are summarized in Table 1.
Setting—Social Paediatric Centre.
This investigation aims to understand the patients’ views on their material surroundings to implement them into the new clinic design. The following questions are sought to be answered: How do young patients describe and talk about the clinic lobby and the hospital bedroom? What are the implications of their descriptions?
Method
Ethical Considerations
Ethical approval was granted by the ethics commission of the TUM School of Medicine in September 2019 (394/19 S-SR), and investigators signed nondisclosure agreements. Parents of minors and patients of legal age (above 18 years) received participant information sheets, as well as consent forms after being verbally informed, and only if their child expressed an interest to learn more about the investigation. Moreover, participants were handed age-appropriate assent/consent forms. Children under 13 years received participant information sheets with simplified explanations of the study on which they could declare their consent. Children 13 years and older received similar sheets with more detailed information. Every participant received a pseudonym to avoid a direct connection between the data and the individual.
Research Team and Reflexivity
Two women and three men were part of the team. All but the third author have experience working with children in clinical, therapeutic, and educational settings. The primary author is a practicing child psychologist and researcher, who has previously worked on studies related to hospital designs. The second and the third author have close relatives with a disability, thus providing them with more of an insider’s view. The last two authors are researchers at the children’s center.
Data Collection
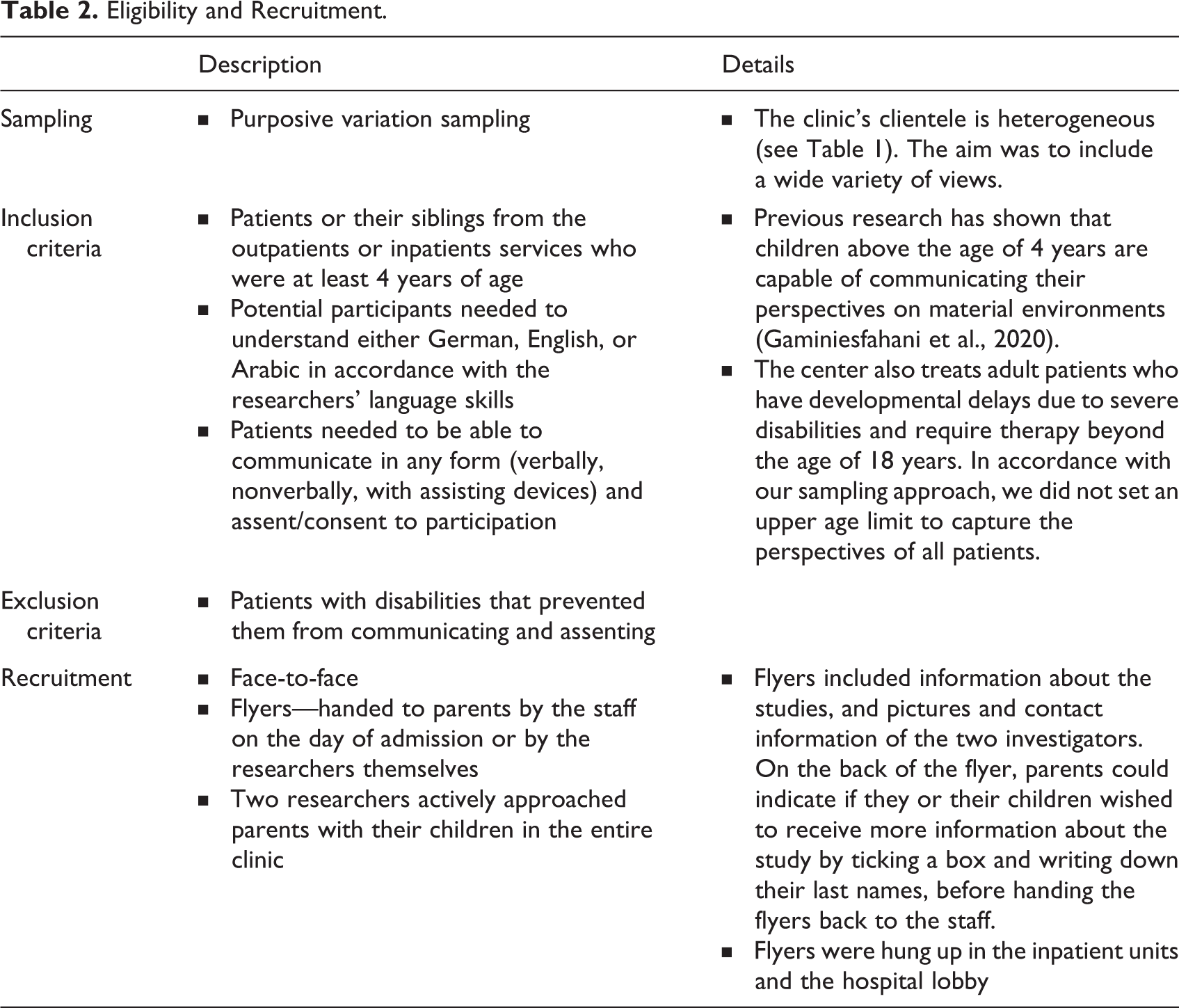
Data were collected from individuals based on certain criteria that are detailed in Table 2.
Eligibility and Recruitment.
A man (second author) and a woman (third author) collected data using arts-based research techniques. The current investigation utilized the “draw, write and tell” method (Angell et al., 2015), where participants could choose between drawing a picture or writing a letter about the lobby or the model room. If the patients decided to do so, they received a booklet, in which they could write down their artist names (pseudonyms) and their age on one page, and express their artistry on the other. Afterward, patients took part in a semi-structured interview, using the letter or drawing as the center of the conversation. During the interview, patients were asked questions about experiences and perspectives on the lobby or patients’ rooms. Every interview was recorded, and we asked every participant for permission to take a photo of their art pieces, so that they could keep the original. The outcomes of the data collection process are summarized in Table 3.
Data Collection Process.
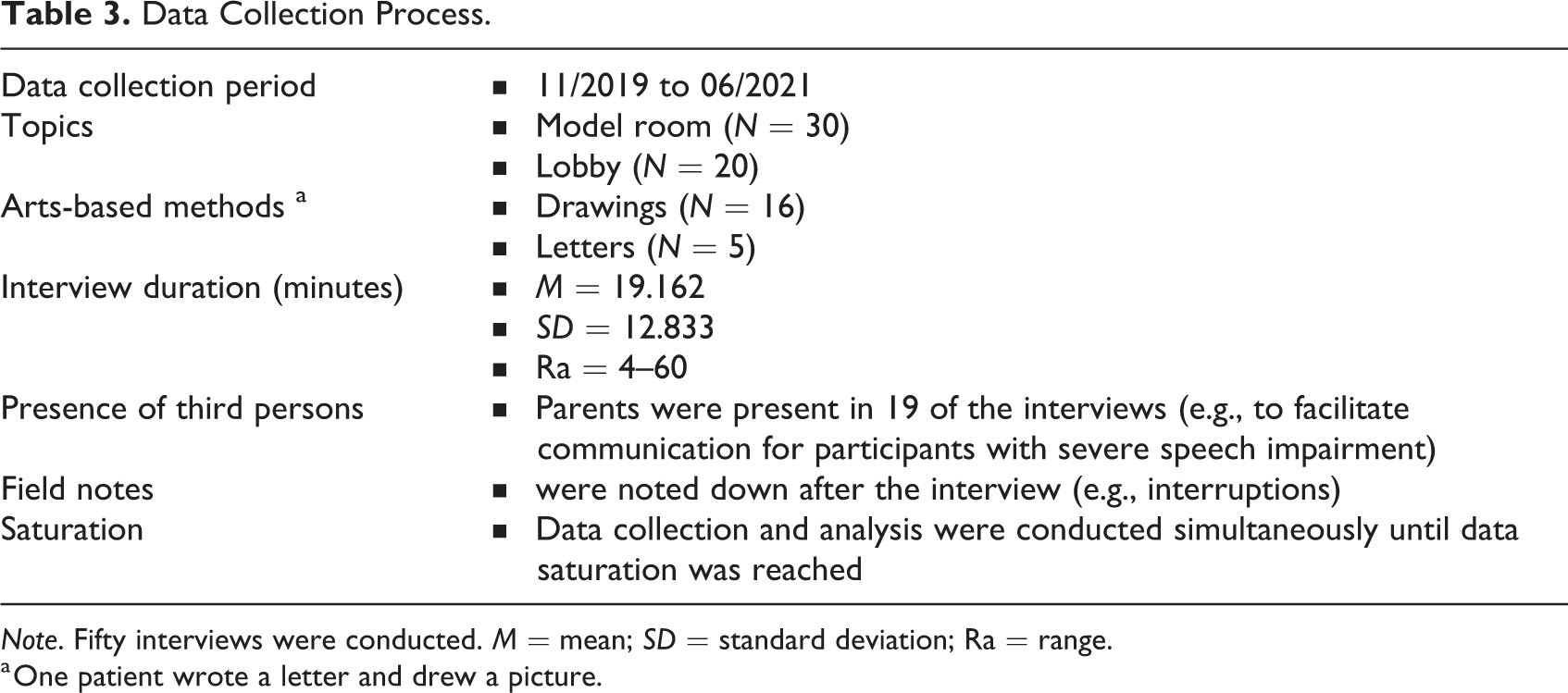
Note. Fifty interviews were conducted. M = mean; SD = standard deviation; Ra = range.
a One patient wrote a letter and drew a picture.
More than half of the patients did not want to write or draw and preferred just being interviewed, giving two primary reasons. Firstly, they (especially patients aged above 12 years) wanted to be seen as independent grown-ups, as opposed to vulnerable children. Secondly, the physical disabilities along with limitations in motor skills prevented them from writing or drawing. Patients could choose the place for the conversations to enable their sense of autonomy. Therefore, interviews concerning the entrance hall were conducted, for example, in the lobby or the cafeteria. Interviews about the patients’ rooms were mostly conducted in a model room. This room was provided by the construction managers and served as an example of what a finished patient bedroom in the future clinic might look like (see Figure 1). Participants were given the option to ask for study results.
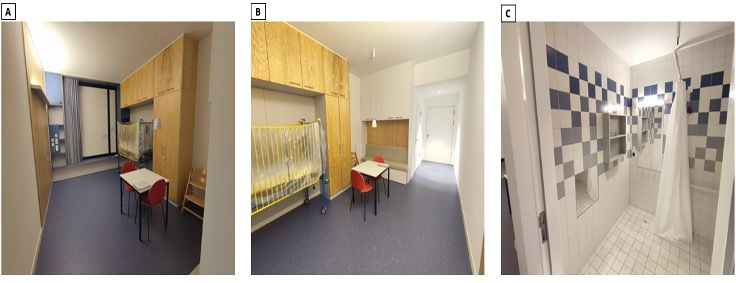
The model room.
Participants
Overall, 37 patients took part in the study (see Table 4), whereby 13 of them talked to us about both topics, the lobby, and the patients’ room.
Participants’ Characteristics.
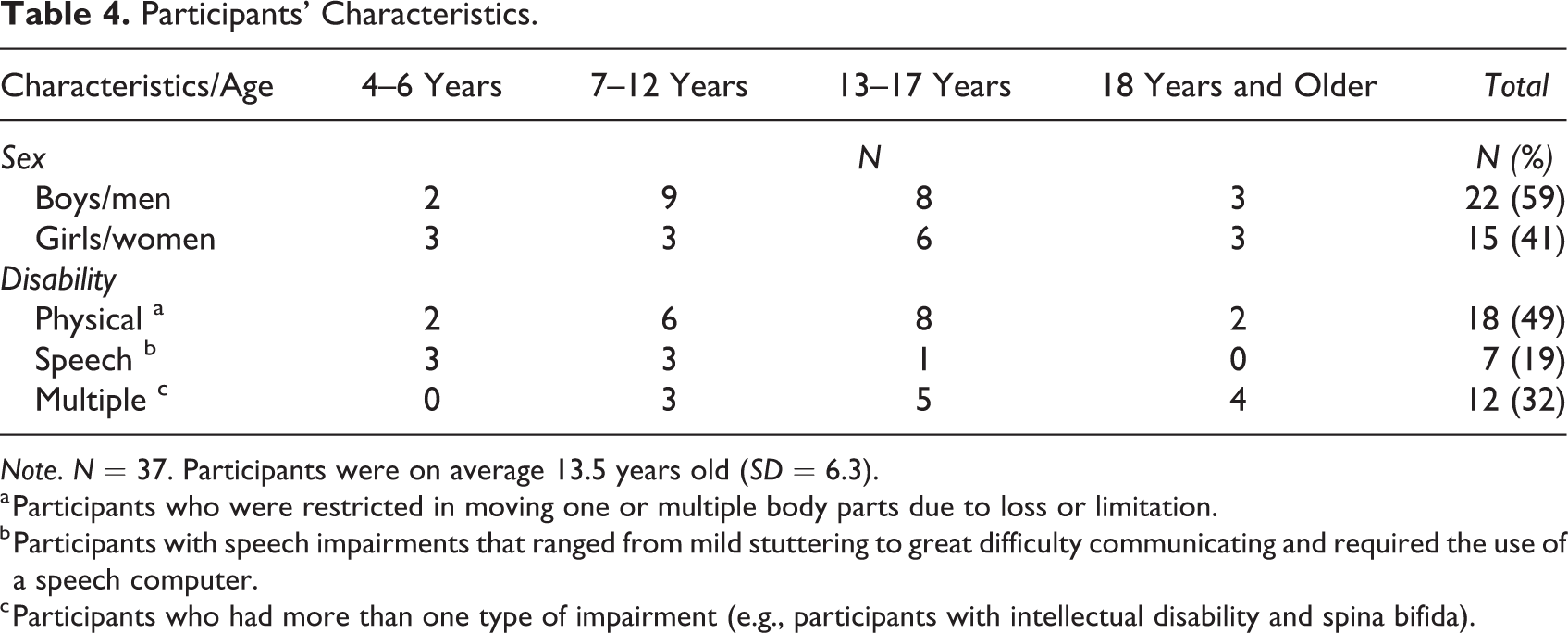
Note. N = 37. Participants were on average 13.5 years old (SD = 6.3).
a Participants who were restricted in moving one or multiple body parts due to loss or limitation.
b Participants with speech impairments that ranged from mild stuttering to great difficulty communicating and required the use of a speech computer.
c Participants who had more than one type of impairment (e.g., participants with intellectual disability and spina bifida).
Data Analysis
The data were analyzed within a critical realist framework, employing a reflexive thematic analysis (Braun & Clarke, 2019). Critical realism assumes an independent reality outside of human perception and construction (Pilgrim, 2019). However, critical realists believe that there are different domains of reality and that any form of experienced truth is associated with theory. This assumption makes human knowledge potentially “always fallible” and its relevance dependent upon the circumstances (Danermark et al., 2002). Subsequently, the current study focuses on explanation rather than description of expressions (see Maxwell, 2012). The material hospital environment is the subject of inquiry. In accordance with Campbell et al.’s (2021) approach to applied health research, attention was given to semantic and latent meanings. An inductive approach was used to determine mainly participant-driven themes and to avoid potential constraints of previous theories. The analysis of drawings, letters, and transcripts followed Braun and Clarke’s (2019) six steps presented in Table 5.
Data Analysis—Thematic Analysis following Braun and Clarke (2019).
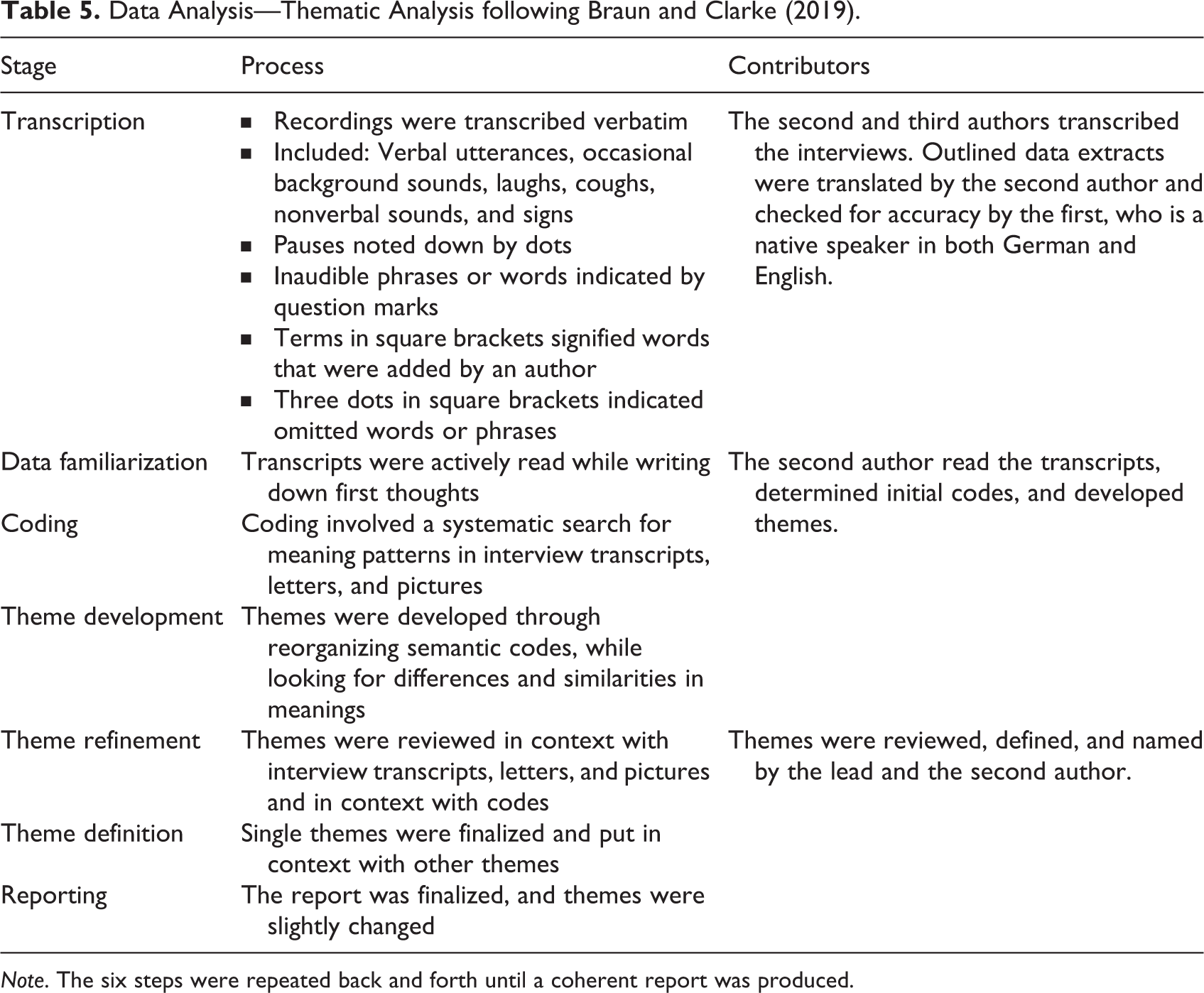
Note. The six steps were repeated back and forth until a coherent report was produced.
Findings
In general, patients described an optimal hospital environment as joyful, helpful, and as an open space, containing clear and simple structures. Taking on agentic and parental roles, patients were oriented toward practical aspects while presenting intricate solutions for the overall design concept and particular spatial elements. Three themes were determined and are presented in the following subsections.
Not a (Typical) Hospital Environment
Familiar, distracting, and entertaining surrounding elements were considered important for the entire children’s center. Older participants (of legal age) with delays in cognitive development wished for play spaces, similar to children and early adolescents in the sample. Indeed, participants in all age groups positively acknowledged distracting design features in the current lobby and expressed further wishes. One participant drew a picture about his wishes (see Figure 2).
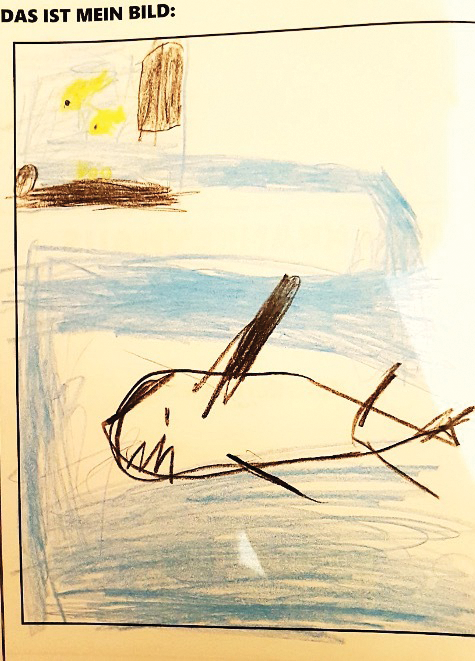
Drawing by Bragi (Boy, 10 years).
The top left of his picture shows the current aquarium and a shark surrounded by water is present in the center. Bragi explained that the floor of the lobby needs to be like an aquarium itself, with sharks in it, and suggested other animals in the lobby. These are reminders of nature that contrast a sterile clinic, highlighting the broader idea of a space that does not look like a “typical” hospital lobby. Indeed, the space should feature living elements, which potentially promote wellness (Ulrich, 1991). However, though the aquarium was viewed positively, it must be incorporated in a way that enables free movement and lessens barriers. All age groups, particularly wheelchair users, shared this sentiment. Moreover, the lobby environment should distance itself from the traditional symbols of medical institutions. Instead, it may resemble a natural setting with healthy living beings associated with leisure activities. This is further highlighted by Nanna, as she talks about the bedroom: Nanna: Then, I don’t know, an elf room, a pirate room (Int: Mh-mh, right) I think in the Europa-Park [theme park in Germany], there’s a room like that—one more pirate-like (Int: Mh-mh) You can find that in Legoland, these amusement parks, there’s always something like that in hotels (Int: Mh-mh) So if it’s like this, somehow like this…the sickbed also more like this- with wood somehow (Int: Aha, okay) Like a pirate bed or a princess bed…and this window sill that is just a bit…wider, so that you can sit on it better (Int: Mh-mh) And also with cushions and somehow a nice…colorful curtain, matching the theme of the room. (Int: Mh-mh) And somehow also on the wall graffiti or something beautifully painted…uh…elf forest, unicorn…exactly, somehow like that. (Int: Mh-mh). (Girl, 16 years; Translation) Sophia: [Picture] of…maybe a landscape or something (Int: Mh-mh) Then it would look—(Int: And- hm?) Ah. Then it would look more like a hotel room. (Int: Ah) And not as it would be a hospital. Otherwise, you’d feel sick (laughing). (Girl, 16 years; Translation)
The sterile clinic character was not viewed in a neutral fashion, but rather as a pathologizing environment that adversely impacts the mental state. Therefore, spatial modifications to counteract the typical hospital associations do not only serve the purpose of increasing patients’ well-being, but also prevent further negative health consequences. While a medicalized space might pathologize patients and threaten their independence (Kanyeredzi et al., 2019), recreational spaces, enabling children to have fun, support a sense of control (e.g., Adams et al., 2010; Lambert et al., 2014b). Material surroundings are viewed as part of cultural or organizational contexts. When considering hospitals as physical, social, and symbolic spaces (e.g., Koller & McLaren, 2014), a medicalized space may inherently position the patient in a constricting inferior role. Consequently, a patient may surrender autonomy and independence to medical authority (Kanyeredzi et al., 2019; McGrath & Reavey, 2018). A sense of control could be further threatened by complex and confusing spatial arrangements, which were often discussed in the context of the lobby as shown in the next theme.
An Overwhelming and Confined Space
The lobby was depicted as an unclear, overwhelming, and confusing space. All patients above the age of 6 years raised wayfinding issues, while portraying it as a crowded place and pointing out restricted pathways. Issues of navigation were presented: Fulla: So, I find it [the lobby] a bit unclear […] so one does not know where something is if you have not been here often […] there are a lot of corners and doors an—(Int: Mhm.) you—you do not directly see where to go […]. (Girl, 16 years; Translation) Dear Prof. Mall, an entrance area with a clear map on each floor. The information is right at the entrance. I like that. The doors are electric. I think it’s good that you can see which doctor is on duty today. I would like to have a place where you can leave your luggage in the meantime and parking spaces that are relatively close to the entrance and where you can quickly bring your luggage into the building. I would like there to be Wi-Fi and internet, I would like to feel at home in the children’s center, the play area should be accessible for wheelchairs and there should be games for different age groups. I would like the entrance area to have no steps, not be small and have a wider foyer. I want toilets that are accessible for wheelchairs with changing table. Kind regards from Erdbeere. (Boy, 10 years; Letter translation) Eira: [The most important thing about the lobby is] […] that it is clear […] that I know as quickly as possible where I have to go […] that it is bright…. and that it is simply appealing, and I don’t have a feeling like “Oh great…. uh…Farewell, beautiful world,” like that […] Yes. That it’s really an open, pleasant room. You feel already miserable when you’re a patient…. Also, not too low, not too dark, because that’s always constricting (Girl, legal age; Translation).
Nonetheless, especially patients over 12 years mentioned that a larger space might relieve the pressure of being in a hospital (Bsiri-Moghaddam et al., 2011). This allows for more breathing room, which might support a sense of freedom and control (Lambert et al., 2014a). Correspondingly, having control over spatial elements was also considered important for the bedrooms as outlined next.
A Practical Room to Fit Everyone’s Needs
More than half of the participants across all age groups described the importance of usefulness, simple handling of furniture, aspects of accessibility, and options for personalization in the model room. Patients expressed that a hospital bedroom needs to be functional and suitable to individual needs by proposing changes to material elements: Eira: Further the sink is quite low, that’s clear. That was thought for children, that it is a bit lower. But maybe it would not be bad if one could somehow have the possibility to do something with the height, because if then again now an adolescent came, the sink would be at his knee height. That’s a bit impractical. […] It would not be bad. If then just different age groups would be in these rooms. (Girl, legal age; Translation) Wali: I don’t think that’s right. (Int: OK, how-wa-) Because opening the bed every time is a pain in the back for the parents. […] The better solution is to have a bed with a remote control (Int: Mhm.) so that the parents also have a remote control. (Int: OK.) And that you—that you make sure that it runs automatically like the other things, like the doors (Int: OK.) that you also have automatic buttons (Int: Mhm.) and that the bed opens directly with a button (Int: Mhm.) […]. (Boy, legal age; Translation) Freya: I think I would [at the empty white wall] just um…so, a cabinet, I wouldn’t put a cabinet there. I’d rather put a thin shelf that maybe runs along the…at belly or chest level, um, and either…. I think it would be- I’d put it along the whole…. I think it would be- I would do it along the whole corridor until you get to the room and then it stops when the room actually starts, so that you also have a separation between the corridor and the room (Int: Ah) Um, and then I would just put personal things there, either pictures or cards or…. Posters theoretically […]. (Girl, legal age; Translation)
Implications for Research
Patients with multiple and severe disabilities in different age groups are competent and helpful research participants who can detail their wishes regarding built environments. Indeed, they consider complex and multiple perspectives, such as economic, emotional, and social aspects. Challenges in data collection with participatory arts-based methods, specifically for young people with physical impairments may be overcome by allowing the participants to choose communication options they feel most comfortable with. In this regard, future investigations could, for instance, inspect or provide different creative methods that enable the artistic expression of people with motor impairments.
Our findings indicate that age differences in environmental preferences are not as clear-cut as previously presented (Peditto et al., 2020; Ullán et al., 2012), especially when adding the disability dimension to the analysis. We have shown that in a sample that is heterogeneous in age and ability, there is a great deal of consistency within the views on positive distraction and control. Even though different age groups emphasize different material aspects, there is a consensus around personal suitability, accessibility, and functionality. Nonetheless, further research is needed on differences in spatial preferences across different types of disabilities and different age groups.
Implications for Practice
Large and open spaces with comforting and distracting features are cherished by patients and may be embedded in a comprehensive but simple overall concept. Every aspect of the environment needs to be tailored to a wide range of abilities (Freund, 2001), ages, and service users. Providing young patients with such an environment can facilitate their growth in different developmental stages. We recommend practical surroundings that facilitate the use for families, and enable patients’ freedom of movement and choice, while providing appropriate options to pass time. Thematically coherent environments resembling homes, hotels, or places of familiarity and fun are regarded as comforting and welcoming. Conversely, physically limited spaces and a sterile clinical atmosphere potentially challenge patients’ autonomy, while possibly hindering health promotion by increasing distress (McGrath & Reavey, 2018). A health-promoting environment may not only be tailored to young patients, but also to parents, as the children and young adults seem to be mindful of their parents’ experiences and emotions during their hospital visit.
Limitations
The results are limited in generalizability, as they represent the perspectives of 37 young people, who were patients at a children’s social pediatric clinic in southern Germany. Nonetheless, the study extends previous findings through views from a hard-to-reach German population. Furthermore, since almost no personal information was collected to protect participants’ anonymity, conclusions cannot be drawn about potential differences in opinion based on, for example, socioeconomic status or cultural background. Lastly, a health-promoting environment consists of a larger concept including hallways, therapy rooms and other clinical areas. However, despite patients’ occasional mentioning of other spaces and rooms in the children’s center, the findings are specific to descriptions of the lobby and clinic bedrooms.
Implications for Practice
Hospital spaces for children/young people with disabilities should be large and open and contain comforting and distracting features resembling homes, hotels, and places of fun.
The environment should accommodate a wide range of abilities and ages, such as wheelchair users, adults with intellectual disabilities and children with vision impairment.
Surroundings need to be practical and include remote solutions for furniture and doors to facilitate the use for families, enabling freedom of movement.
Health facilities should provide a choice of entertainment options and decorative elements for patients of all age groups.
A health-promoting environment should be tailored to young patients, as well as parents.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231165763 - Designing Well-Being: A Qualitative Investigation of Young Patients’ Perspectives on the Material Hospital Environment
Supplemental Material, sj-pdf-1-her-10.1177_19375867231165763 for Designing Well-Being: A Qualitative Investigation of Young Patients’ Perspectives on the Material Hospital Environment by Shahin Payam, Jihad Hossaini, Katharina Zaschka, Anna Friedmann and Volker Mall in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
We would like to thank the participants and parents for taking the time to share their valuable views with us. We also like to extend our gratitude to the staff of the kbo-Kinderzentrum for their hospitality and their help in recruiting the participants. Further recognition goes to Prof. Dr. Elisabeth Wacker for providing a platform that facilitated the connection of the researchers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.