
Abstract
Background:
In dementia-specific care, the design of the environment is regarded as an influential element in the support and maintenance of skills and can improve the quality of life of residents. To date, there is no valid instrument in the German-speaking countries with which the quality of the physical environment in residential long-term care facilities can be systematically assessed.
Objective:
To report the translation, linguistic validation, cultural adaptation, and content validity evaluation of the Australian Environmental Audit Tool—High Care in preparation for use in German nursing homes.
Method:
The procedure was guided by an adapted multistep process of the World Health Organization (1998) and included focus groups involving potential users of the new tool such as scientific experts and healthcare professionals (n = 40). Content validity indices were calculated following a two-step expert survey.
Results:
The final draft versions of the German Environmental Audit Tool (G-EAT) included 74 and 77 items, for non-secured units and secure units, respectively, divided into 10 key design principles according to the Australian original. The evaluation of content validity showed that cultural differences existed in several items.
Conclusions:
The G-EAT provides the means for conducting a valid assessment of the environmental quality of people with dementia in German nursing homes. However, its usability in healthcare research must be preceded by testing its interrater reliability.
Keywords
Background
The influence of the physical environment has been identified as a key element in dementia-specific residential long-term care over the previous decade (Chaudhury et al., 2018). Depending on the scientific discipline scholars take, dementia care environments have been described as (1) being therapeutic or rehabilitative, focusing on compensating for existing deficits (mainly geriatrics and health sciences origin) (Chaudhury & Cooke, 2014; Zeisel et al., 1994), (2) needs-based, focusing on how the environment can meet the needs of people with dementia (rooted in nursing science and psychology) (Algase et al., 1996; Morgan & Stewart, 1999), or (3) experience-based, focusing on how people pose meaning to a place through interaction with their environment (i.e., gerontology and social ecology) (Charras et al., 2016; Molony et al., 2011).
From our perspective of nursing and healthcare science—in this context—a well-designed environment may help people with dementia to maintain and enhance their remaining abilities (Fleming & Purandare, 2010), whereas environmental features and layouts that are not adapted to the specific needs of residents with dementia can trigger responsive behavior or lead to disorientation and frustration (Chaudhury et al., 2018; Fleming & Purandare, 2010; Marquardt & Schmieg, 2009; Woodbridge et al., 2018).
As awareness of the influence of the physical environment grew, so did the variety of new care models in residential long-term care worldwide. Many of these new concepts focus on small-scale, homelike environments instead of traditional large-scale living units. This physical environment should help to ensure that residents can use their remaining abilities in daily living in the context of familiar activities (Verbeek et al., 2010): Size and layout of the living unit can facilitate wayfinding. Straight direction from the bedroom to the living-/dining room—as often existing in small-scale environments—may help residents to enter these spaces more independently (Marquardt & Schmieg, 2009). A kitchen in the living unit opens up the possibility to integrate residents into preparing meals and to improve participation in daily activities like cooking. Purposeful use of different stimuli in the outdoor environment—such as a gardening bed or a bird house—may encourage people to spend time outside and thus contribute to achieving a low-threshold approach to dementia-specific symptoms such as an inverted sleep–wake rhythm or the loss of occupational skills (de Boer et al., 2018). As the environment can have these effects on residents with dementia living in nursing homes, it is important to have the means to assess its quality and account for its effect in empirical studies. It is essential that components of the physical environment are evaluated as comprehensively as possible from the perspective of the residents. The quality and extent of a dementia-friendly environment can be determined on the basis of a wide range of factors that can vary among the different living environments in residential long-term care and should reflect the concept of person-centered care. Nevertheless, several authors have commented that the frequent description of the physical environment in terms of the size of the living unit and its housing concept (integrative/segregative) is not sufficient (Palm et al., 2014; Verbeek et al., 2010; Woodbridge et al., 2018). A detailed description of this important context factor is required especially when the built environment is to be investigated in observational and intervention studies.
In English-speaking countries, systematic assessment tools have been used for several decades to assess environment-related factors in nursing homes. Since the late 1990s, quantitative assessment were developed especially in the United States, the United Kingdom, and Australia. Hence, there are reliable and valid instruments available (Elf et al., 2017), but none of them are in the German language. Thus, we aimed to adapt one of these available instruments for our national context. We based our decision for choosing an instrument on several factors: actuality of the instrument, equivalence of the theoretical construct to our nursing understanding, and the establishment of the tool. The Therapeutic Environment Screening Survey for Nursing Homes (TESS-NH) (Sloane et al., 2002), the Professional Environmental Assessment Procedure (PEAP) (Lawton et al., 2000), and the Environmental Assessment Tool—High Care (EAT-HC) (Fleming & Bennett, 2015) were on our shortlist. All three instruments have a well-described theoretical construct based on Lawton’s ecological model (Lawton & Nahemow, 1973) and were comprehensively tested and judged to be valid and reliable (Fleming & Bennett, 2015; Lawton et al., 2000; Sloane et al., 2002). While the TESS-NH and PEAP appeared to be more widely used (Elf et al., 2017), the EAT-HC seemed more appropriate for our national context. On the one hand, the development of the instrument incorporated results from the literature up to the late 2000s. On the other hand—from our point of view—the aspect of safety and autonomy through environmental design is most congruent with our understanding of dementia-specific care, even if it is not completely consistent: Only 30%–50% of the German nursing homes run dementia special care units (Schäufele et al., 2009). These living units are the only ones in which environmental safety features such as fences and exit control through locked doors are permitted. To accommodate residents in a secured living unit requires the approval of a custodianship court according to s.1906 of the German Civil Code 2013 (BGB). In most cases, residents with (advanced) dementia live in integrative nonsecured living units, where access control would mean a restriction of freedom for all other residents, which is not permitted by the German law. While acknowledging this difference in context, we came to the conclusion that, on balance, the EAT-HC provided the best foundation for the development of a German tool as the items on safety can be modified to match the German legal environment.
The EAT-HC
Fleming and Bennett (2015) developed the EAT-HC as the latest version of their first instrument, the EAT (Fleming, 2011; Smith et al., 2012). The tool is based on the theoretical work of Richard Fleming since the late 1980s and Lawton’s ecological model, which implies that congruency between the ability of an aging person and the environment is necessary to maintain the quality of life and independence throughout the aging process (Fleming et al., 2008; Lawton & Nahemow, 1973). Additional items were developed from the longtime expertise of the researchers as an environmental psychologist and as an architect in dementia-specific design, which support and extend the literature-based evidence (Fleming & Bennett, 2015; 2017, Fleming & Purandare, 2010). The EAT-HC is based on 10 “key design principles” including (1) unobtrusive risk reduction, (2) scale of spaces, (3) the possibility to see and be seen, (4 and 5) management of stimulation, (6) support of movement and engagement, (7) familiarity, (8 and 9) spaces to interact with people inside and outside the nursing home, and (10) the concept and aim of the living unit (Fleming & Bennett, 2015). The EAT-HC contains 77 items that are each allocated to one of these design principles (available at https://dta.com.au/resources/environmental-design-resources-introduction/).
Psychometric properties of the instrument were examined in a systematic review (Elf et al., 2017) using the COnsensus-based Standards for the selection of health Measurement INstruments checklist (Terwee et al., 2012). Based on the reported psychometrics (Fleming & Bennett, 2015), internal consistency was described as good (assessed with Cronbach’s α, were satisfactory, ranging from .57 to .88), structural validity as fair, and cross-cultural validity as good. It was noted that the item generation was based on a literature review (Fleming & Purandare, 2010) and experience with an earlier instrument (Fleming, 2011) contributing to the content validity. Concurrent validity was evaluated by calculating a Pearson correlation between the overall score of the EAT-HC, the TESS-NH (.72) and the Special Care Unit Environmental Quality Scale (.34), the correlations of .72 and .34, respectively, were significant beyond p = .01 (Fleming & Bennett, 2015).
Aim
Our aim was to translate the EAT-HC into the German language and to identify possible challenges when applied in a German nursing home context. This article describes the translation process, the first part of the cultural adaptation of the instrument, and the assessment of its content validity.
Method:
The adaptation of the EAT-HC for the German long-term care setting was guided by the manual published by the World Health Organizations (WHO) Division of Mental Health and Prevention of Substance Abuse (1998). The WHO manual describes a multistep translation process that includes the involvement of potential users and experienced researchers and clinicians. Bilingual experts check the translated instrument on two separate occasions. In a monolingual panel, the future users are asked to comment critically on the translated instrument. Because our purpose was to adapt an audit tool to assess environmental factors rather than patient-related measures, we added additional steps to the WHO adaptation method (see Figure 1).
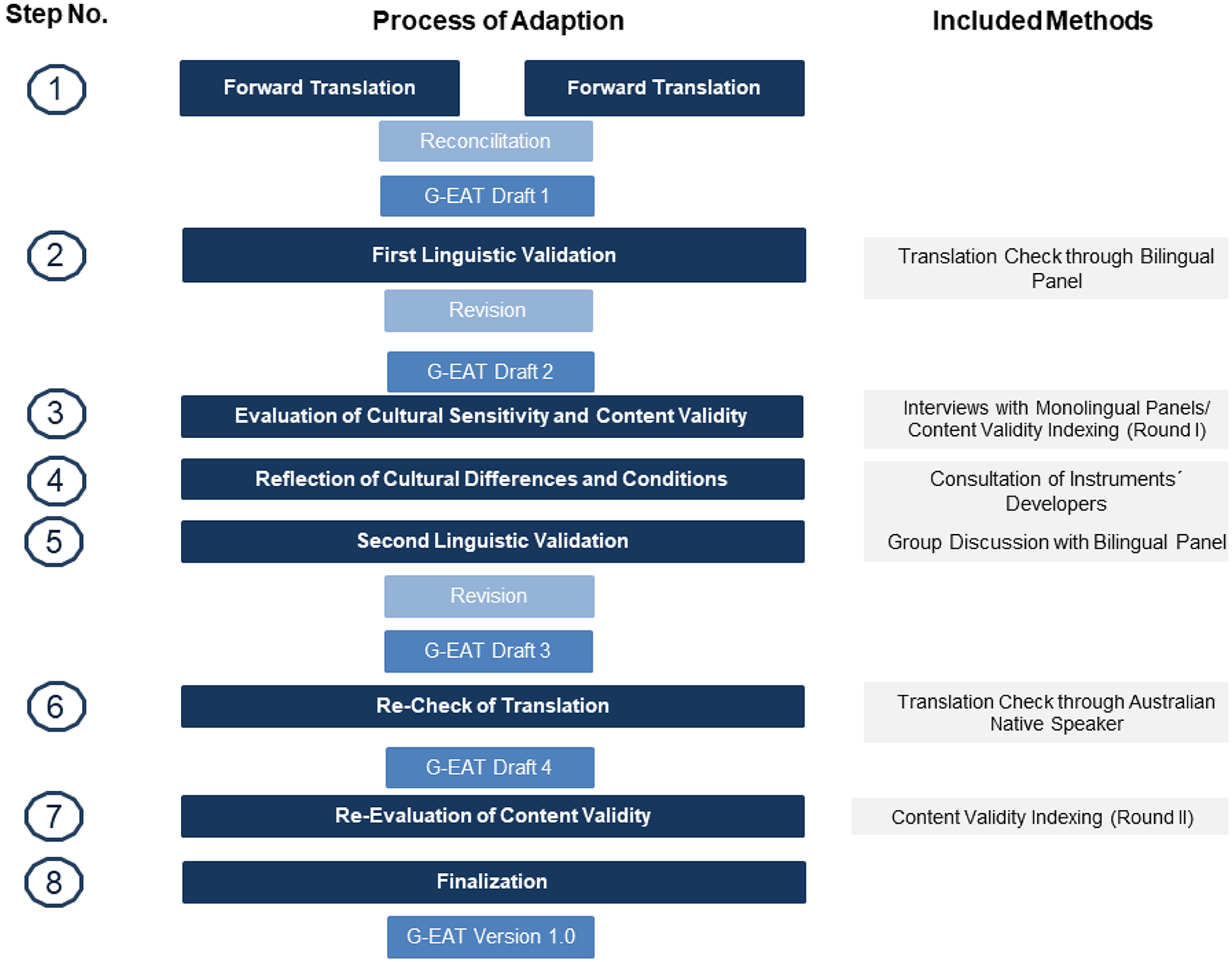
Translation process and content validity evaluation of the German Environmental Audit Tool.
The first step was a forward translation of the EAT-HC by two translators who were familiar with the instrument, its topic, and its field of application. This was followed by the integration of a bilingual panel as part of the first linguistic validation (Step 2). Subsequently, within the focus groups (FGs), the relevance and the comprehensibility of the translated items as part of the cultural sensitivity were discussed. In addition, scientific experts were asked about the same criteria through a quantitative survey (Step 3). The results from this step were discussed with the developers of the EAT-HC (Step 4) and with the bilingual panel a second time (Step 5). The instrument’s translation was re-checked (Step 6) and the content validity was re-evaluated (Step 7). Finalization of the draft to the German version of the EAT-HC (Version 1.0) took place in Step 8. We further refer to the German translation of EAT-HC as German Environmental Audit Tool (G-EAT).
Step 1: Forward Translation
First, the EAT-HC was translated into the German language. The procedure was carried out by two members of the project team who had the required language skills and practical knowledge of the long-term care setting (AF and RP). The team members independently translated the 77 items of the instrument and the 10 key design principles as its underlying construct. The two translations were then synthesized into G-EAT Draft 1 over several sessions and used as the basis for Step 2.
Step 2: First Linguistic Validation
The first linguistic validation aimed to check the previous translation and adjust the linguistics. The panel participants were recruited from the professional network of the project staff. The panel members were experienced in translating research instruments, had excellent English and German language skills, and expertise in the field of long-term care. In a written process, they were asked to give their consent or rejection to the content of the translation and to formulate alternative proposals. The completed tables were summarized, then synthesized by the researches from Step 1 and were documented in an updated instrument draft (G-EAT Draft 2).
Step 3: Evaluation of the Cultural Sensitivity and Content Validity
The content validity of the instrument (G-EAT Draft 2) was evaluated by FGs of experts working in nursing homes and through a quantitative survey of scientific experts. The FGs and the quantitative survey were conducted independently of each other.
The experts for the FGs were recruited from the professional network of the first author and were included because of their practical expertise in long-term care and/or dementia-specific care. In the FGs, the application of the 77 items and the key design principles in the German long-term care setting were discussed in depth. Because the discussion of every single item in-depth was not feasible, the participants were asked to concentrate on those items that they regarded as potentially controversial. The discussion was guided by using different cognitive techniques (probing, paraphrasing, and think aloud technique) (Prüfer & Rexroth, 2005). All interviews were recorded and transcribed verbatim.
The experts included in the quantitative survey were recruited within the field of dementia research following the guidelines of Grant and Davis (1997). The recruitment criteria were having scientific expertise proven by publications and/or several years of practical experience in long-term care or environmental design for people with dementia. All participants received a questionnaire containing two questions for each of the 77 translated items. They were asked to rate each item regarding its relevance for long-term care in Germany and the comprehensiveness of the translation on a 4-point Likert-type scale. Ratings of one or two expressed low relevance or comprehensiveness, and ratings of three or four expressed acceptable (Lynn, 1986). Furthermore, the experts could explain their choices and suggest additional environmental aspects to be included in the German version of the instrument.
Step 4: Reflection of Cultural Differences and Conditions
The first author undertook a 3-month internship with the developers of the EAT-HC to discuss questions that had arisen during the first three stages. Together, recommendations for dealing with cultural differences and conditions in the Australian and German long-term care systems were elaborated, recorded, and supplemented by photos of environments from Australian nursing homes. Additionally, training on assessing the environment using the EAT-HC and an introduction to environmental design was provided.
Step 5: Second Linguistic Validation
The second linguistic validation was based on the results of the preceding steps (Steps 3 and 4). The expert panel discussed the items that were identified as controversial in the FGs and the quantitative survey. The aim was a final linguistic revision and to modify controversial items. Items to discuss were prepared as text and visualized by photos from Step 4. The panel discussion was audio-recorded. The results of the meeting were incorporated into the instrument by the project members from Step 1 and resulted in G-EAT Draft 3.
Step 6: Re-Check of Translation
G-EAT Draft 3 was back-translated by a native Australian-English speaker with excellent German language skills. The Australian and back-translated German instrument versions were compared by one of and the first author. Issues regarding agreement were discussed with the German project team. Minor changes of the wording led to G-EAT Draft 4.
Step 7: Re-Evaluation of Content Validity
Steps 4–6 provided the information required to make essential revisions identified in Step 3. Additionally, the wording of the key design principles was further adjusted to improve the understanding of the instrument for the target group. As recommended (Lynn, 1986), the scientific experts from Step 3 were asked to evaluate the G-EAT Draft 4 again using the same survey procedure.
Step 8: Finalization
Based on the results of the G-EAT Draft 4 evaluation, the project members from Step 1 conducted a final revision.
Ethics Approval
The ethics committee of German society of Nursing Science approved the study (Proposal No. 18-005). All participants were informed about the aims of the study and gave their written consent.
Data Analyses
Several procedures were used during the multistep adaptation process. Reconciliation and synthesis were conducted by two researchers (AF and RP) after Steps 1, 2, 5, and 6. Every synthesis was documented. Transcripts of the FG interviews (Step 3) were analyzed with content analysis according to Mayring (2015) and performed in MAXQDA 2018©. For the expert survey data analysis, the content validity index (CVI) according to Lynn (1986) was calculated on the item (I-CVI) and subscale level (S-CVI). For the I-CVIs, a threshold of .78 indicated items with acceptable relevance/comprehensiveness (Lynn, 1986). On the S-CVI level, .90 was set as the minimum level of agreement, according to the literature (Polit & Beck, 2006; Polit et al., 2007). The CVIs calculated in Step 3 were incorporated into the second panel discussion (Step 5). Items that were commented on in the FGs and had an I-CVI below .78, along with those that only had an I-CVI for comprehensiveness below .78, were discussed in Step 5. The re-evaluation of the CVI in Step 7 validated controversial items and derived meaning for the practical use of the G-EAT.
Results:
Participants
In the different phases of the adaption, we included 40 German experts in the field of long-term care and design as well as dementia-specific care. Four experts participated as bilingual panel in Steps 2 and 5, and 20 participants were included in four FG (FG1: n = 5, FG2: n = 4, FG3: n = 4, and FG4: n = 2). In total, 17 experts took part in the quantitative assessment survey. Some members of the survey sample were replaced by others from Steps 3 to 7 as they declined to reassess the revised instrument due to limited time resources. The majority of participants were female and had works 18 years on average in their profession. Table 1 describes the disciplines represented by the researchers and healthcare professionals.
People involved in the Environmental Assessment Tool—High Care Adaptation Process.
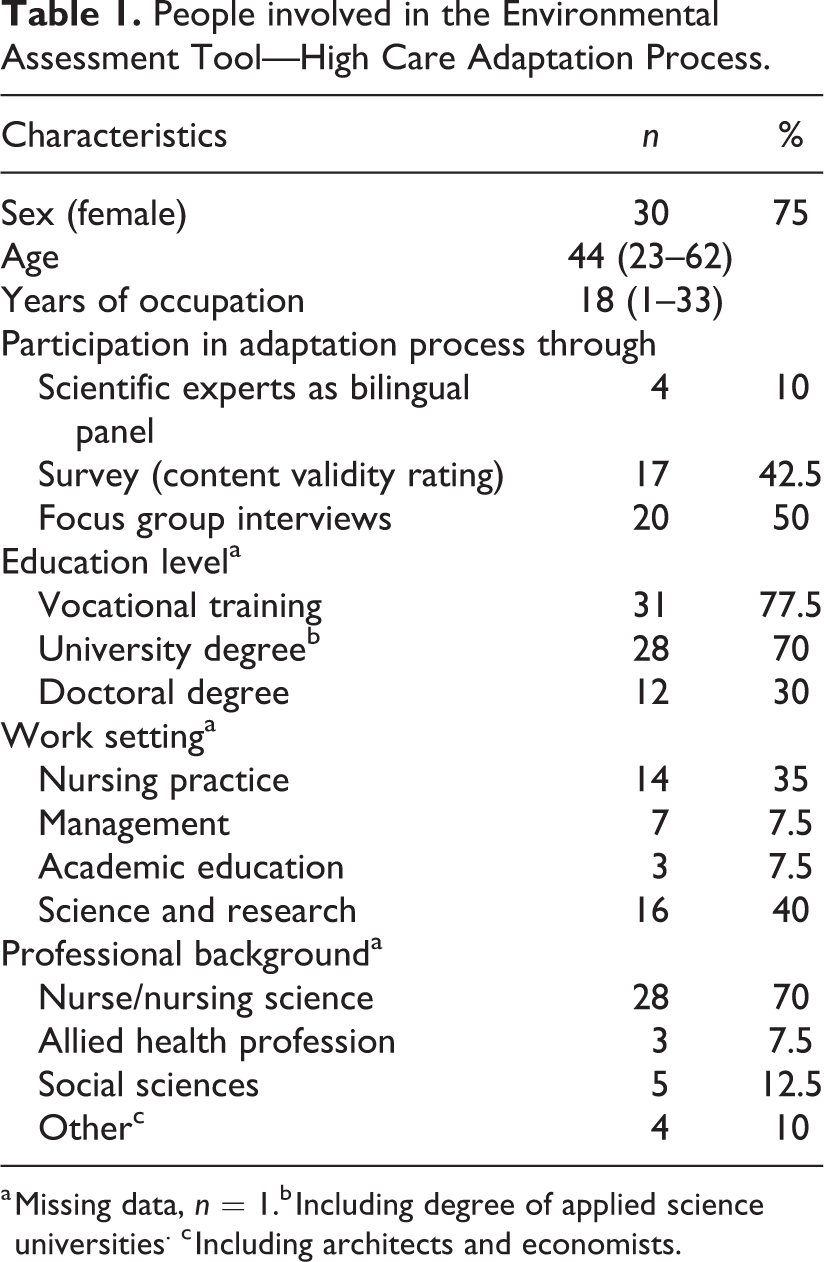
a Missing data, n = 1.b Including degree of applied science universities. c Including architects and economists.
Results of the Translation and Adaptation Process
The results of the individual adaptation steps were systematically documented, so that changes to the items could be made accordingly. Figure 2 shows an example of the information from the individual steps and the adjustments they led to. Due to the relevance of the perspective of future users, the results from Step 3 and the modifications of the EAT-HC to the G-EAT are focused on below.
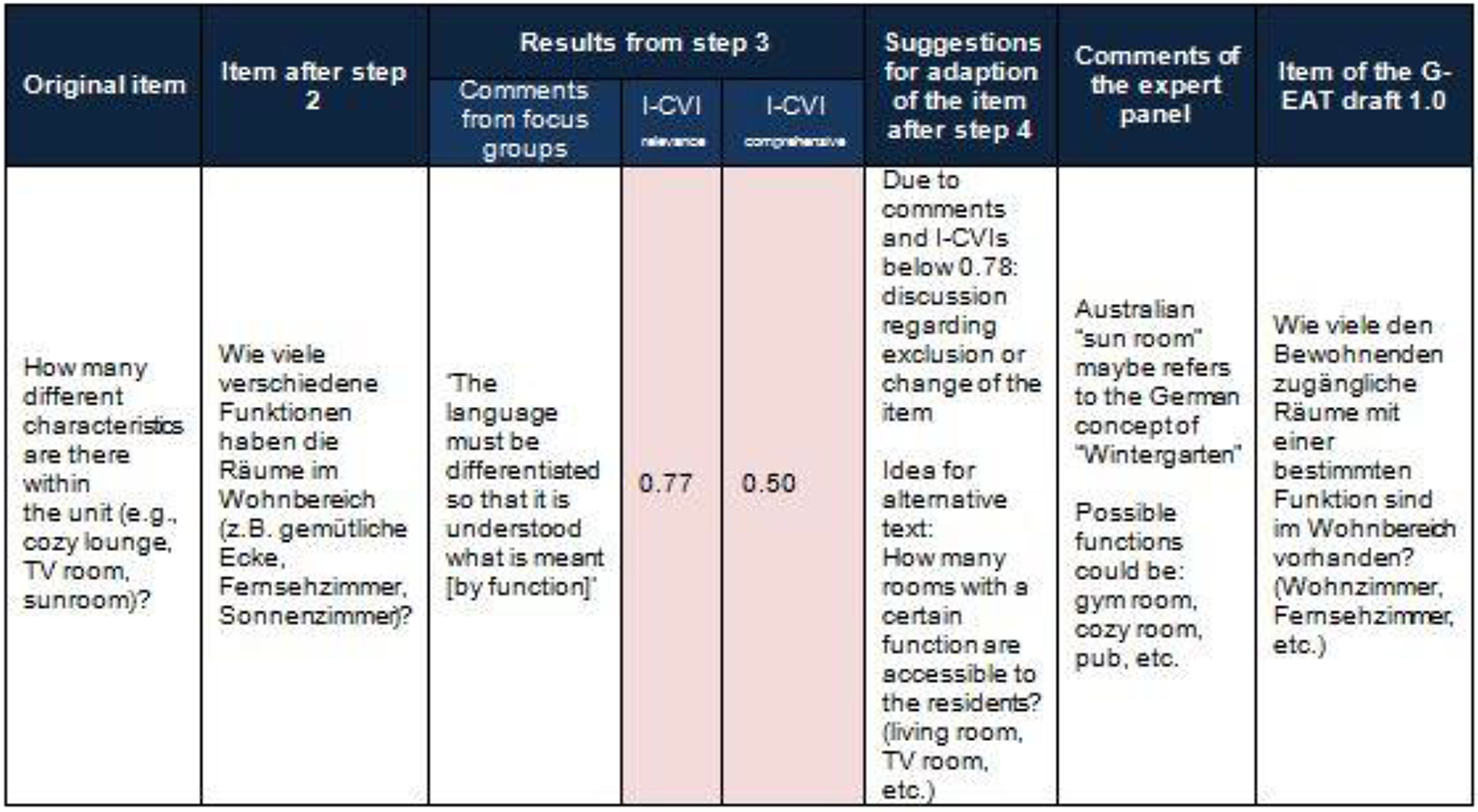
Example documentation of the process step results.
Implications for Future Users of the G-EAT
In the four FGs, a total of 43 of the 77 items were discussed by the experts. Items from all 10 key design principles were critically reviewed. The main criticism of the practitioners was ambiguity regarding information that was needed for using the assessment and the unclear or inappropriate content of the items. For example, a lack of definition of terms was frequently noted: “What are ‘unnecessary things’?” (FG4) or a missing frame of reference for answering the question: “Well, I only find it subjective when there are no reference values. So I have written reference values for myself. The question is how I determine that” (FG2). In terms of content, the focus on security through environmental safety features rather than on autonomy of the residents was questioned across all items. The practitioners found that the original Australian items placed emphasis and focus on security. By contrast, in Germany, freedom of movement would be a focus to maintain autonomy for residents, even for those with dementia. Scoring of the instrument was not congruent with these beliefs: The problem with the item is that if I fulfil it […] I get a point. But the trouble is that I can’t use this intervention because I’m committing deprivation of freedom, which is actually a negative point. (FG2)
At the scale level, only dimension VI was considered highly relevant (S-CVI ≥ .90) by the experts for T0. Another three dimensions (V, VII, and IX) showed a value of ≥.80 and are close to the limit value. In the re-evaluation of the CVIs at T1, again only dimension VI could be categorized as highly relevant (S-CVI = .99). However, after comprehensive adjustments to the instrument, six dimensions showed S-CVI ≥ .80 (I, II, IV, V, VIII, and IX). At the item level, the experts assessed 46 of the 75 items (61.3%) as highly relevant (I-CVI ≥ .78; Lynn, 1986) in the first survey. After incorporating the knowledge from the mono- and bilingual panels, at T1, 51 items (68,0%) were judged to be highly relevant. Some items that were classified as highly relevant at T0 were no longer relevant at T1 and vice versa. However, 21 items did not show sufficient relevance at either time. They are allocated to the dimensions I, II, III, IV, VII, and VIII and differ in terms of the stimuli they address and the spaces to be assessed.
Regarding the comprehensibility of the translation, an improvement from T0 I-CVI ≥ .78 was apparent for 54.7% of the items (n = 41) to 82.7% (n = 62) at T1.
Content Validity Indices of the German Environmental Audit Tool.
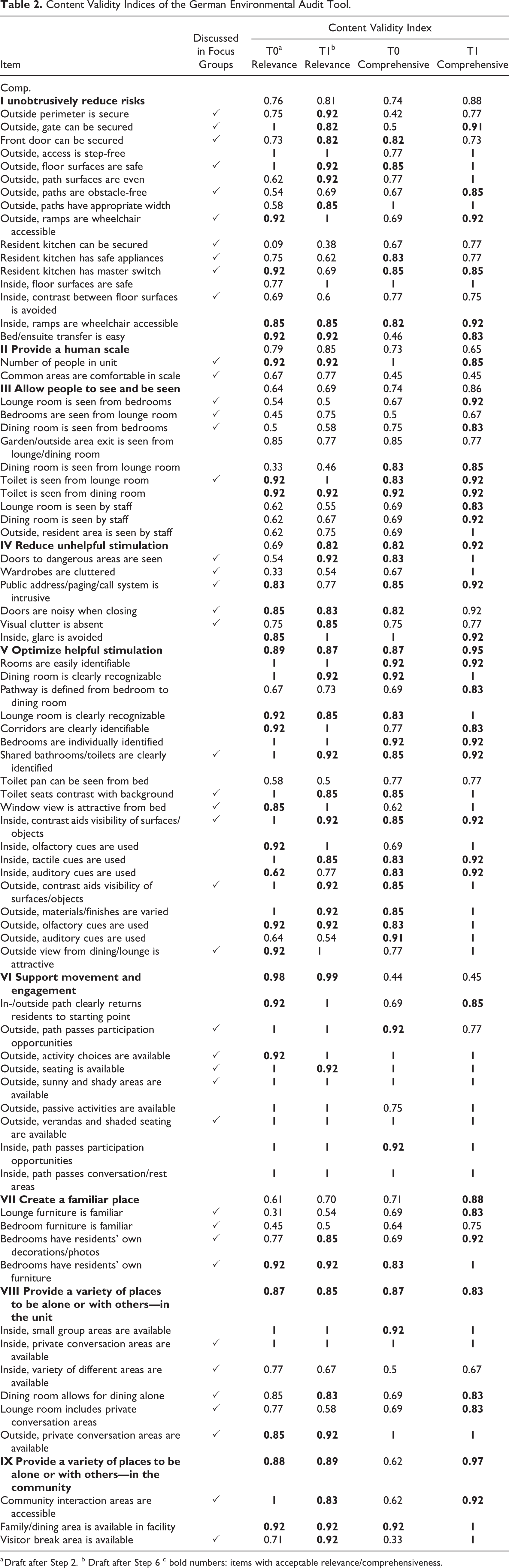
a Draft after Step 2. b Draft after Step 6 c bold numbers: items with acceptable relevance/comprehensiveness.
Characteristics of the German Version
Like the original instrument, the German version is based on 10 key design principles. At this level, only one major modification was made to adapt to the new cultural background. Since the denomination of a principle as “design in response to vision for way of life” was too abstract for the new target group in Germany, the terminology was reformulated to use words from everyday life in the nursing home; in addition, the phrase “design as part of the nursing concept” was used. Additionally, the instrument’s name was adapted with regard to the translation as “G-EAT.”
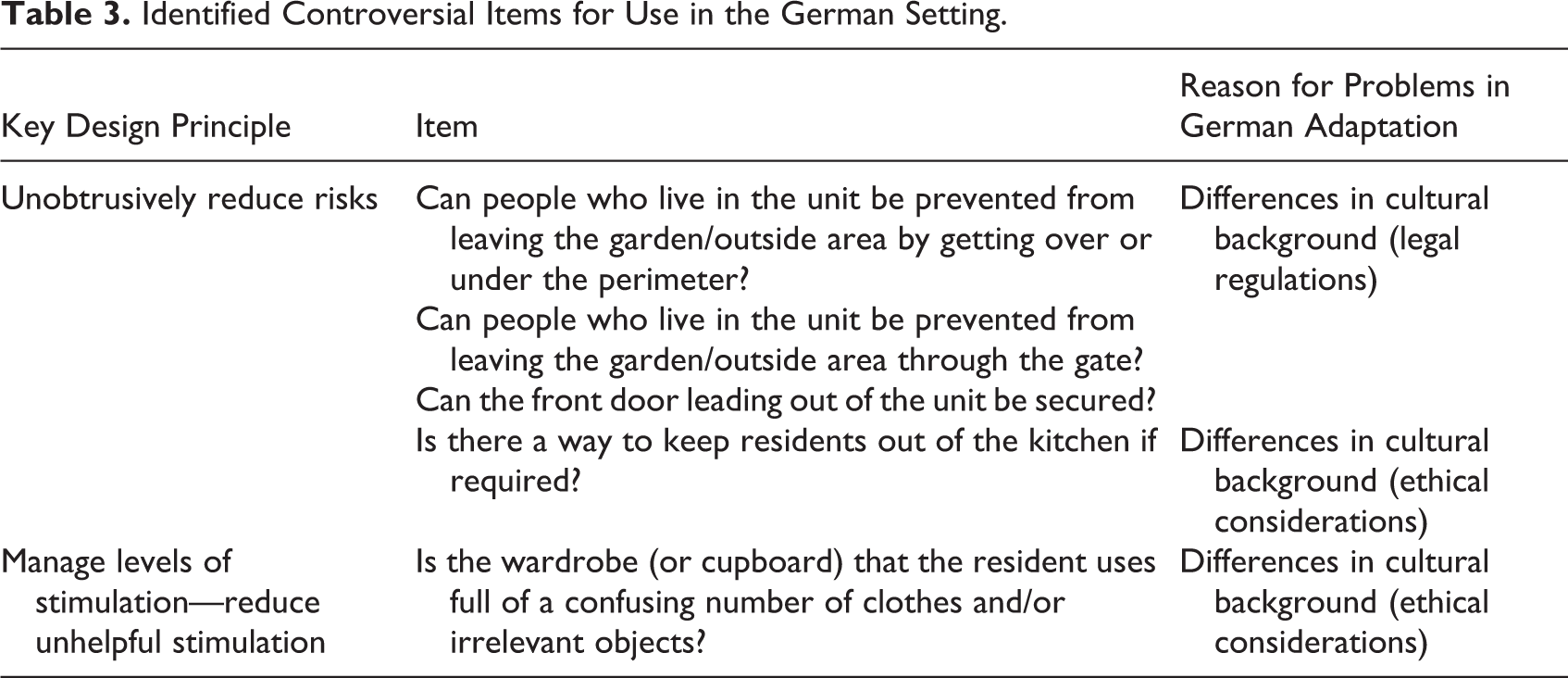
Because of cultural and legislative differences, four items were identified as controversial during the multistep adaptation process (Table 3).
Identified Controversial Items for Use in the German Setting.
Discussion
This study aimed to translate the EAT-HC for the German setting, as the first stage in the applying of an instrument that enables a systematic assessment of aspects of the physical environment of the living situation of people with dementia in long-term care.
A multistep process that included translation, linguistic validation, and cultural adaptation was performed and involved several groups of experts. Through the broad involvement of potential G-EAT users, items were identified that appeared challenging in application. These issues could be attributed to cultural differences between Australia and Germany and also to the complexity of dementia-specific environmental design.
Dealing With Controversial Items
Some items that stirred attention through their CVIs and reservations by healthcare professionals were identified as controversial in the new cultural context. The question must be raised as to how to deal with these items. Acquadro and colleagues (2008) described that the exclusion of an item from the theoretical construct must be followed by new testing. Since the German-language instrument has not yet been extensively tested and the change of the theoretical construction could therefore lead to a bias in the representation of the physical environment, the items should be left in the instrument. However, the challenges they pose must be addressed. First, the reasons for reservations against these items must be investigated more thoroughly. Thus, the legal framework and differences in the understanding of care, but also a lack of understanding the underlying concept, can form the basis for examining these items.
Long-term care in Germany and in Australia is regulated by different laws at the municipal and state levels and by internal institutional policies. A major difference between the two countries lies in the legal regulation of the accommodation of residents with cognitive impairment. In Germany, it is defined by law that people may only be accommodated in secure living units by a court order (§ 11 GG, § 239 StGB). However, the legal situation in Australia does not grant the same freedom of decision to residents with cognitive impairment (Steele et al., 2019). As a result, three questions from the key design principle “Unobtrusively reduce risks” can only be applied in secure units in Germany (see Table 3). This leads to two versions of the instrument for the German setting: one version with 74 items for non-secured units and one with all 77 items for secure units.
There were also differences in the attitudes of nurses between countries regarding resident privacy, leading to reservations about one item. In Germany, the resident’s room is regarded as private and can be arranged according to their preferences, even if this does not correspond to the facility’s philosophy of architecture and environmental design, because it helps to provide person-centered care. This can be seen as a cultural phenomenon which must also be taken into account in further adaptation of the assessment tool. Comparable adaptation requirements have already been mentioned in another translation of the EAT-HC for Singaporean long-term care (Sun & Fleming, 2018).
It also became apparent that some aspects of the design of the environment in Germany do not seem to be established yet, for example, a guest room for visiting families or places to meet the community in the facility. The existence of these places is a political and social objective in Germany against the background of the deinstitutionalization and the philosophy to open up nursing homes to the community (Michell-Auli, 2011). To show how places for interactions have already been created, a commentary field was added to the dichotomous answer option (yes/no) for these questions. Furthermore, in the further testing of the G-EAT, photos of places where these interactions already occur will be taken. In this way, the assessment will be able to ascertain whether these places already exist but are just not labeled accordingly. This example also illustrates how difficult it is to distinguish the physical from the social environment, as previous studies have shown (de Boer et al., 2018).
Strengths and Limitations
There are diverse ways of adapting instruments for healthcare research (Acquadro et al., 2008; Maneesriwongul & Dixon, 2004). For the G-EAT, an existing adaptation protocol was extended to include the views of experienced researchers and the instrument’s developers. Both the existing and the extended methods should be discussed regarding their ability to adapt healthcare research instruments and they should undergo methodological critique.
The involvement of the scientific experts followed the established CVI that has been used in previous studies (Halek et al., 2017; Palm et al., 2014). Nevertheless, it should be mentioned that this method may be criticized owing to possible random agreements (Glarcher, 2018; Polit & Beck, 2006; Polit et al., 2007). We tried to address this critique by not using I-CVIs and S-CVIs as decision criteria for the acceptance or rejection of an item in the new instrument. Together with the remaining reliability test, the I-CVIs and S-CVIs formed the basis of the final decision of which items would remain in the evaluated German version of the instrument.
The interviews with healthcare professionals not only supported the cultural adaptation of the G-EAT but also identified the knowledge requirements of future users. It must be still considered that not all instrument questions could be fully included by the FGs and that unidentified information needs could emerge in further testing. This is due to the complexity of the instrument and its underlying construct (Fleming & Bennett, 2015).
As a strength of our approach, we can emphasize our collaboration with the developers of the EAT-HC. This collaboration provided comprehensive insights into the theoretical foundation of the instrument and its practical application. For this reason, we would recommend such an exchange for further translation processes in research projects.
Conclusion
With the adaptation of the EAT-HC for the German setting, a first step has been taken to be able to assess the structural environment in residential long-term care facilities in Germany. The extensive adaptation process has also revealed initial problems in the use of the research tool in this field. An evaluation of interrater reliability should provide more information about the tool’s real-world applicability and the necessity for developing new questions. A test phase with the G-EAT should also be conducted to determine whether the results can be used in a research-oriented as well as in a practice-oriented manner. Furthermore, the ability of the G-EAT to assess person-centered environmental adaption needs must be discussed in the upcoming process of instrument development.
Implications for Practice
The key design principles of the EAT-HC are suitable for the assessment of the environment in German nursing homes.
Cultural adaptation showed that the issue of security through environmental safety features and segregation of residents with dementia is very controversial in the German setting.
Based on the results, the German version of the EAT-HC is ready to be tested in the field of long-term care.
Footnotes
Acknowledgments
We would like to thank all scientific experts and healthcare professionals for their participation in our study. We also want to thank the team of Dementia Training Australia for their support in helping us understand the cultural background of the instrument as well as Christina Manietta and Christiane Pinkert for their critical internal review of this article.
Author Contributions
AF, RP, and BH were involved in the study design and data collection. AF drafted this article. RP, BH, HV, and RF made substantive contributions to this article. All authors have read, reviewed, and approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.