
Abstract
Background:
A predominant notion among researchers is that hospital room design and decor are subject to the designer’s expression of self, which is contrary to evidence-based studies showing that design and decor can impact patient health. The aim of this study was to examine whether improvement in quality of healthcare provided in hospitals could be achieved through the convergence of expertise of healthcare professionals and hospital room designers.
Methods:
This was a prospective study to identify the impact of hospital interior design features with a focus on single occupancy rooms. Volunteers were recruited through advertisements and the study was conducted at the Tripoli Medical Center. Responses were analyzed using a three-dimensional computer-aided design software to help respondents accurately map their preferences and visualize outcomes.
Results:
Participants preferred an aesthetically pleasing hospital room environment that included art and bright colors, window views, and the need for personalization, technology, mobility, and flexibility, all of which improved satisfaction and happiness. Of these, participants’ preference for technology as a cause for satisfaction and happiness was a novel finding.
Conclusion:
Designers of hospital room interiors should plan and create an appealing single occupancy room for increasing user satisfaction and patient wellness.
According to Fischi (2004), human health can be impacted either negatively or positively by the material environment characterized by the design of buildings, its color, lighting, and materials. Although this notion has been particularly felt in a hospital environment (Fischi, 2004), it has received little attention and remains sterile and lifeless, despite rapid progress in medical science. It is ironic that a hospital where patients are admitted to recover and recuperate should actually cause them to be sick. Sickness enhances anxiety, and according to Dijkstra et al. (2008), it is also associated with a great degree of uncertainty, fear, and stress. In addition to the stress caused by medical procedures, patients’ sickness is compounded by poorly designed healthcare facilities (Fischi, 2004) and hospital rooms with inappropriate decor (Dijkstra et al., 2008). The development of a strong scientific basis for the need to build healing environments was set in motion several decades ago (Dovjak et al., 2018). Studies on the impact of healing environments on patients, staff, and visitors showed benefits such as improved medical treatment, patient healthcare, increased productivity, and perceived comfort of users (Dovjak et al., 2018).
Until about 10 years ago, the medical need of patients was the primary objective of healthcare facilities, but patient satisfaction surveys revealed that the hospital environment constitutes an important aspect of the complete healthcare experience (Fottler et al., 2000). Research from the Centre for Health Design has shown a direct correlation between an attractive healthcare facility and perceived quality of care, thereby lowering anxiety among patients (Geimer-Flanders, 2009). Telephone interviews conducted with 380 discharged inpatients to determine the relative contribution of hospital design and ambience on overall satisfaction with the hospital experience by exploring differences in satisfaction across four departments (medical, obstetrics, orthopedics, and surgical) in six hospitals found that interior design, architecture, housekeeping, privacy, and ambience were perceived as sources of satisfaction (Harris et al., 2002). More recently, evidence-based research has shown that design features related to the physical environment contribute significantly to the well-being of patient families and hospital staff (Huisman et al., 2012).
Healing Environment
Healing environment refers to the ambience which conveys a message of calmness that support healing within institutions such as hospitals, though aesthetically pleasing environments are seldom found (Kerfoot & Neumann, 1992). From a Western perspective, “healing environment” is a relatively new concept. However, this concept is rooted in studies performed in various disciplines over the last 50 years examining the impact of institutional environments on human behavior.
The term “healing environments” is used to describe the factors that positively affect (both physically and psychologically) the community served by a healthcare facility (Ampt et al., 2008). This includes its physical setting and the organizational culture. The authors further emphasized the importance of humanizing and improving healthcare facilities in order to create or add value to a “user-centered” healthcare environment (Ampt et al., 2008). Such well-designed healing environments have the potential to increase positive emotions, which positively affect health and well-being of patients (Malkin, 2008) because it makes patients feel welcomed, balanced, and in harmony with the world (Venolia, 1988).
As far back as 1859, Florence Nightingale asserted that the hospital environment has an effect on health and recovery. She is quoted as saying, The effect in sickness of beautiful objects, of a variety of objects and especially of color is hardly at all appreciated. I have seen in fevers (and felt, when I was a fever patient myself) the most acute suffering produced from the patient not being able to see out of a window and the knots in the wood being the only view. I shall never forget the rapture of fever patients over a bunch of bright colored flowers. (Palmer & Nash, 1997), p. 148.
Even before a patient enters the doctor’s office, there are environmental factors that affect their psychological and emotional responses to the upcoming clinical encounter, which can predetermine the patient’s health outcome. Moore (2000) has been quoted as saying “the interface of doctor and patient occupies a small part of the time during which a person is hospitalized; yet the patient is interpreting the data in his or her sense all of the time.” Therefore, stimulating the senses through the arts, including architecture design and landscaping, affords endless opportunities for recovery and well-being. This argues for the practicality (and economy) of incorporating arts into healthcare environments at the outset, when designing the facilities. Seemingly simple elements as lighting, wall covering, and paving, for example, may have as much aesthetic impact as sculptures or a fountain. Indeed, Florence Nightingale, in her 1863 book, “Notes on Hospitals” (Glanville, 2004), said that the first requirement of a hospital is that it should do the sick no harm. She included guidance on issues such as sanitary conditions, principles of construction, and the impact of the building on patient care.
Beginning in the 1960s, designers began to believe that, “If a man can manipulate his surroundings to improve his physical well-being…he can manipulate it to foster desire behavior and to eliminate negative responses” (Chaney, 1973). This concept plays a dominant role in the design of hospital facilities. Normally, people outside a healthcare facility can either leave or adapt to an uncomfortable physical environment (Malkin, 1992). Unfortunately, patients in healthcare facilities are not afforded this option and are forced to adapt, which can have negative effects on their recovery. Previous studies on the effects of hospital room windows on patients’ well-being showed that proximity to a window and the view outside had a positive effect on the patient (Ulrich, 1984; Verderber, 1983). These findings contributed to evidence-based design that is now deemed essential for hospital design (see Table 1).
Overall Evidence-Based Design and Research.
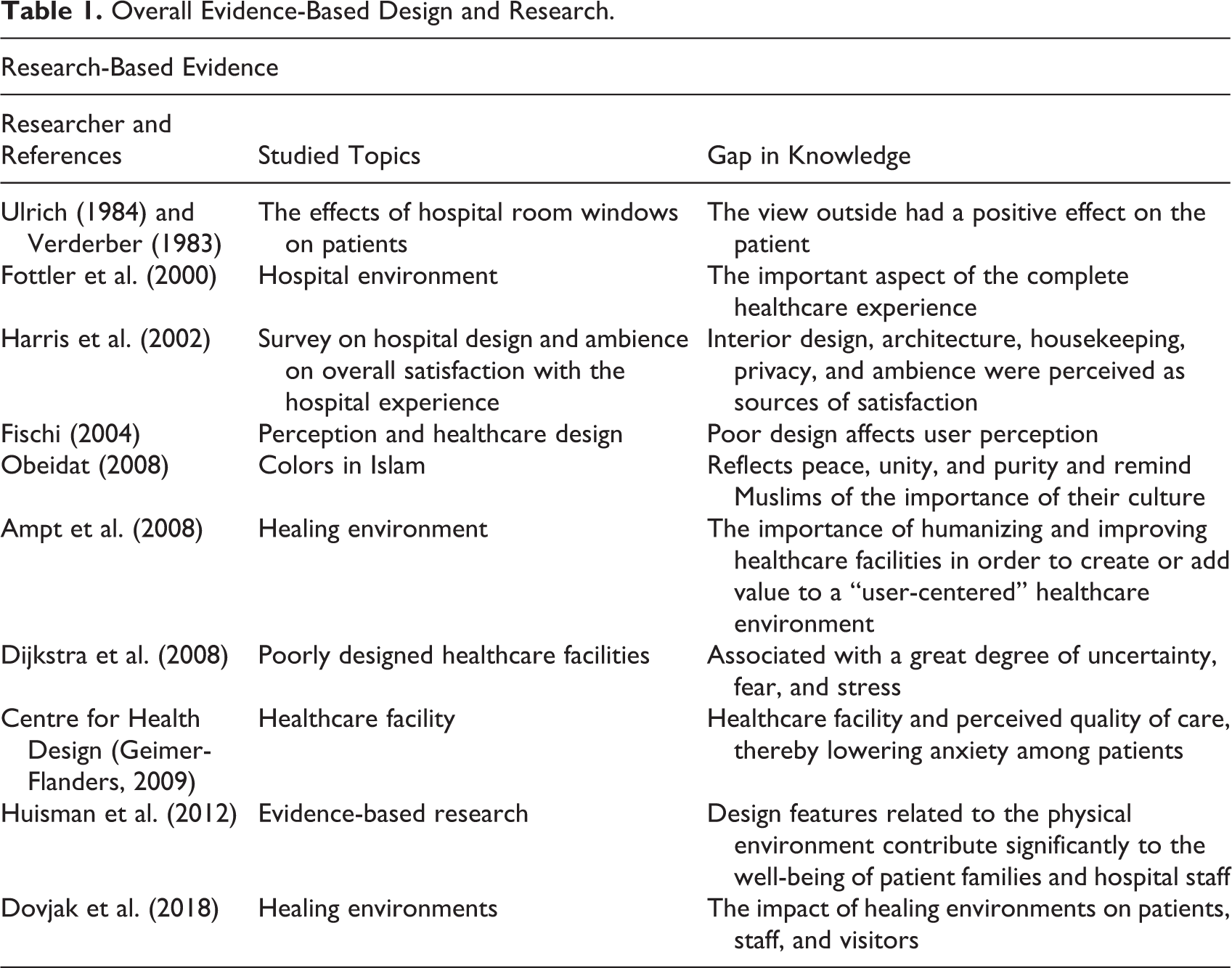
Despite the wealth of knowledge citing its benefits, the lack of properly designed facilities providing healing spaces that allow patients to recover is a limitation. Roslyn Lindheim, a critic of the modern hospital facility says, The adjectives used to describe hospitals include: dehumanizing, depersonalizing, neutering, frightening, uncaring. I have neither heard anyone describe a hospital as beautiful, peaceful, healing, warm, joyous…indeed, a look at the modern hospital speaks not of human healing but of our technological progress, not of caring but of an increase in the GNP (Gross National Product), not of generating health but of saving jobs and institutions. (Vererber, 1983), p.17.
Positive responses lead to approach behavior (satisfaction) and negative responses lead to avoidance (Bitner, 1992). For example, if a patient is hospitalized to be healed but cannot sleep because the bed is uncomfortable or the furniture in the hospital room is unsuitable, then these factors may affect the patient, leading to a negative emotional response (Gashoot, 2012).
Perception and Islamic Aesthetic Elements
The “appealing setting effect” in the field of psychology is an effect that occurs when an individual is brought into a setting that is more appealing than normal. It is hypothesized that the effect of an appealing setting can also be true of hospital rooms that have Islamic design elements (Swan et al., 2003) because user satisfaction inherently increases within that setting. An understanding of the “appealing setting effect” and how it affects patient satisfaction with hospital rooms is important, as well as to move beyond the acute care setting.
To better communicate the design plan to its user, interior designers should fully understand the concepts of beauty and aesthetics; the latter at a universal level (Edwards, 1992). The design concepts go beyond the functionality of the space and are associated with specific techniques to connect the human senses with their environment (Hall, 1992), such as a picture of the Makkah in the hospital room. When the user views the interior objects and the physical appearance of an environment, it triggers a sensory experience that affects their behavior (Edwards, 1992).
Due to its aesthetic value, Islamic art, with its high-quality portrayal of motifs and ornamentation, may fulfill the psychological needs of hospital users in Middle Eastern countries and elsewhere (Othman, 2011). The use of symbolic and religious elements in Islamic culture is ordinarily meaningful to Muslims, and because they have a therapeutic effect on hospitalized patients, Islamic art and design that influence a believer’s health and wellness should be considered when designing Middle Eastern hospitals (Obeidat, 2008). Indeed, the holy book of Qur’an emphasizes that surreal art portraying animals and humans in healing space could disturb a patient seeking healing and comfort, whereas art depicting nature will remind patients of the outside world and encourage rapid healing and return to normalcy.
Symbolic Aspects
Islamic symbols in the Middle East include colors, shapes, and pictures of Al-Masjed Al-Haram and inscriptions of Qur’an recitations and Athan for prayer, all of which are of significant consequence to a believer (Obeidat, 2008; see Figure 1).
Example of Islamic botanic patterns.
Shapes
Islamic art is associated with four basic shapes: circle and interweaved circles, square, the star pattern, and multisided polygons; the square shape refers to the Ka’ba (The house of Allah) in Mecca (Obeidat, 2008; see Figure 2).
Plant motifs in Islamic art.
Islamic color
Green and white are the two important colors in Islam. Green, significant because it was the color of the first flag of the Islamic state used by Prophet Mohammed, and white, which reflects peace, unity, and purity, are the colors that remind Muslims of the importance of their culture and are believed to be therapeutic for Muslims during difficult times (Obeidat, 2008; see Figure 3).

The name of Prophet Mohammed in Green and White.
Theoretical Approaches for Environmental Behavior
Bitner (1992) reviewed the effects of the physical setting on human behavior, which was largely ignored by psychologists up until the 1960s, and concluded that human behaviors are remarkably influenced by the physical setting.
The human perception of, and response to, various environmental elements is affected by mood, personality, and experience (Fottler et al., 2000). The internal responses that define individual behaviors may be divided into emotional, cognitive, and physiological responses (Mika, 2008). Because of an individual’s unique response, their behavior can be challenging for the healthcare provider and the designer tasked with creating healing environments. According to Fottler et al. (2000), a patient responds physiologically, cognitively, and emotionally to the hospital environment.
Physiological response
The body’s reaction to external stimuli (e.g., cold or heat) is the physiological response, which includes the mind’s limitation in processing information (Fottler et al., 2000). In the context of the current study, some designs may elicit a certain physiological response that can impact patient preference for the hospital and/or hospital room.
Cognitive response
A person’s expectation of the environment based on prior experiences and nonverbal communication evoked by physical cues in the environment forms the cognitive response. The general tendency for humans is to seek a point of similarity between their observations and experiences in life, and accordingly, familiarity of a hospital room can reduce patient’s confusion and unhappiness (Fottler et al., 2000). A patient who cognitively associates the hospital room wall color with either past healing or their own home design will opt for similarities in design and decor during the hospital stay.
Emotional response
Patient preference for design and decor is significantly affected by emotional factors associated with past emotional distress, which can affect the choice of hospital design. Therefore, it is the imperative for designers and healthcare providers to facilitate conditions that promote patient healing and satisfaction. Patients respond positively to good experiences in the past and negatively to bad experiences, and these emotional responses dictate their preferences. For example, patients may have a positive emotional response to music and caring staff, both of which can affect their preference toward the environment of a hospital single occupancy room (Fottler et al., 2000).
The lack of studies on culturally appropriate auditory, visual, and tactile tastes as components of the overall healthcare plan has been concerning (Kopec & Han, 2008). Therefore, the objective of this study was to identify patient preferences to draft guidelines for designers of single occupancy hospital rooms with implications for a healthcare setting in parts of the globe that adheres to equity in healthcare, particularly catering to Islamic design.
Research Questions
Method
Ethics
Ethics approval to conduct this study was obtained from the ethics committees of Bournemouth University. Permission to conduct research was obtained by the Tripoli Medical Center.
Database Search
A literature review was undertaken using the Cochrane collaboration method (Allderson & Niggins, 2004), by combing through Athens, PsychInfo, MedLine, Knowledge bank, Science Direct, Info4education, and Center of Health Design databases. A previously described qualitative approach (Myers, 1997) was used for data extraction since a subjective approach that includes examining and reflecting on perceptions enabled an understanding of social and human activities.
Participants
Participants in the study were ≥18 years, provided written informed consent and were not receiving active treatment. Volunteers were excluded if they were <18 years of age since the law required parental approval for participation.
Recruitment
An invitation poster calling for volunteers to participate in the research showing study inclusion and exclusion criteria was displayed on the notice boards of the Tripoli Medical Center. Volunteers were invited to participate in the study conducted at the Tripoli Medical Center between January 21 and February 28, 2011. The center is a teaching hospital that provides support to research activities. However, due to the war in Tripoli and concern for the safety of staff and participants, the number of participants was restricted.
Data Collection
To obtain descriptions of various aspects of hospital room design, a qualitative research consultation was undertaken with the study participants. This collaborative approach helped in discovering, defining, and developing a plan to solve problems in the target area (consultee’s environment) that was appropriate for individual consultations (Kurpius & brubaker, 1976). Data were collected through open-ended questions during the consultation session.
Participant’s views on preferred room design were captured using a three-dimensional (3D) computer-aided design (CAD) program (ARCHI-CAD) and transformed into a 3D image. In consultation with the participants, and with the aid of a consultation guide, different room layout and color schemes were experimented with, notes were taken and, on two occasions, voices were recorded for political reasons.
Thematic Data Analysis
Descriptive details of several elements of the design aspects were collected through participant consultations and data were analyzed thematically based on conceptual analysis of the two main objectives—participant satisfaction and preferred architectural and interior designs and ambience of the room. The analytical methodology adopted was in line with the need to satisfy patient needs for a better room interior design (Ås, 1975) and to allow the designer to obtain patient data in the designed environment (Intille et al., 2003).
For the purpose of this study, the authors thoroughly familiarized themselves with transcripts of each consultation. Thematic analysis is a qualitative method for identifying, analyzing, and reporting patterns (themes) through minimal organization and rich description and interpretation of data related to various aspects of the research topic (Boyatzis, 1998; Braun, 2005; Patton, 1990). Ely et al. (1997) stated that the language of “themes emerging” can be misinterpreted to mean that themes “reside” in the data, and if we just look hard enough, they will “emerge” like Venus on the half shell. If themes “reside” anywhere, they reside in our heads from our thinking about our data and creating links as we understand them. (pp. 205–206)
Phases of Thematic Analysis.Phase
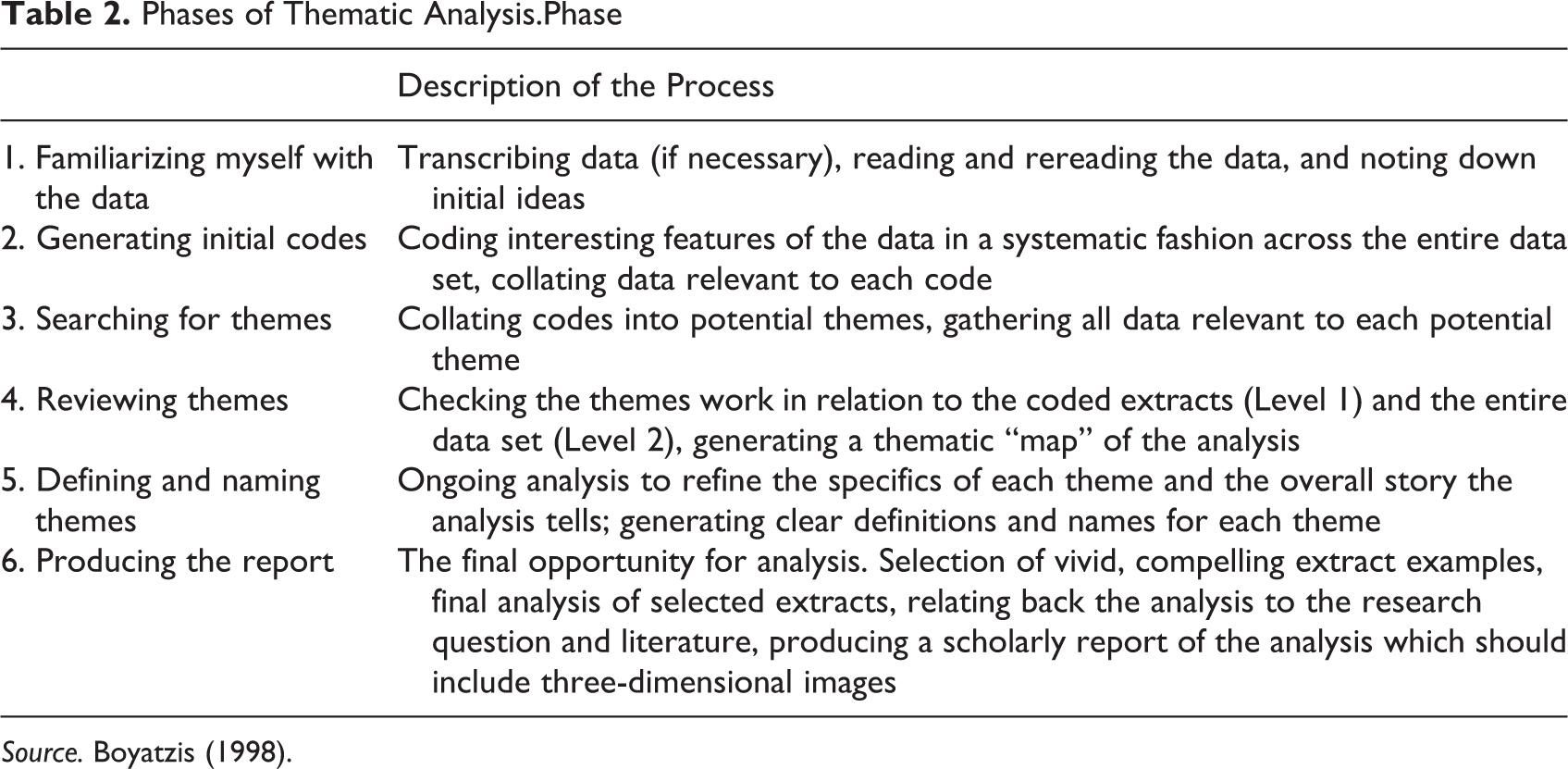
Source. Boyatzis (1998).
Results
Participants
Although 18 participants were included in the study, data saturation was achieved with 10 participants who were consulted for the purpose of this study, and therefore, data from 10 participants were analyzed.
Thematic analysis and finding
The key findings relating to preferred single occupancy identified from this study include environmental aesthetics, technology, personalization, mobility, and flexibility (see Table 3).
Samples of Thematic Finding (Environmental Aesthetics and Technology).
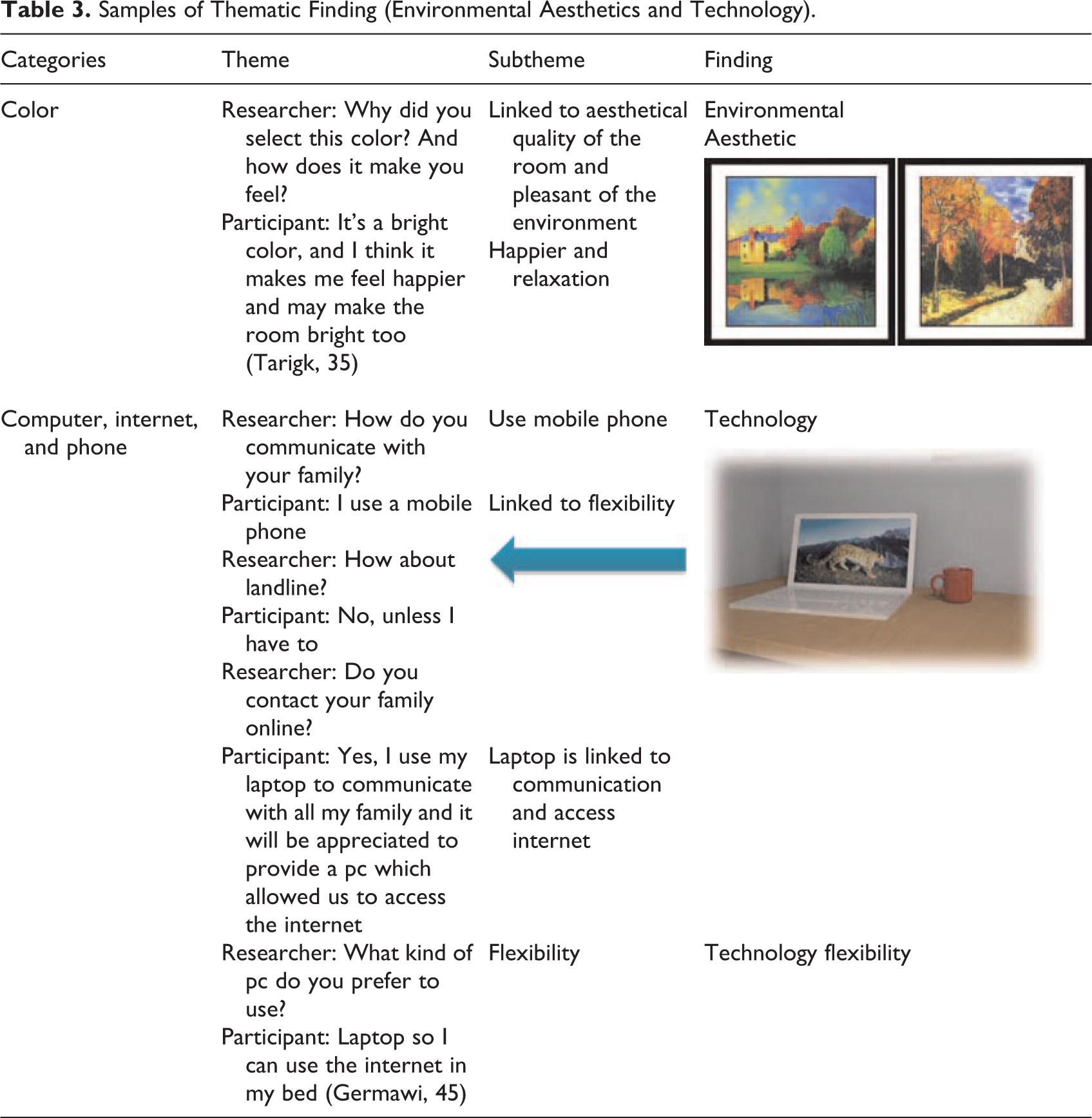
The views and suggestions made by the participants were considered as one analysis unit. The views, suggestions, and the notes taken were read several times in order to achieve a sense of the content and then divided into interior features categories. Each time a new idea arises and was noticed in the content, a new view was started. The views and suggestions were both condensed and divided according to aspects of the focus of the discussion (see Figure 4).
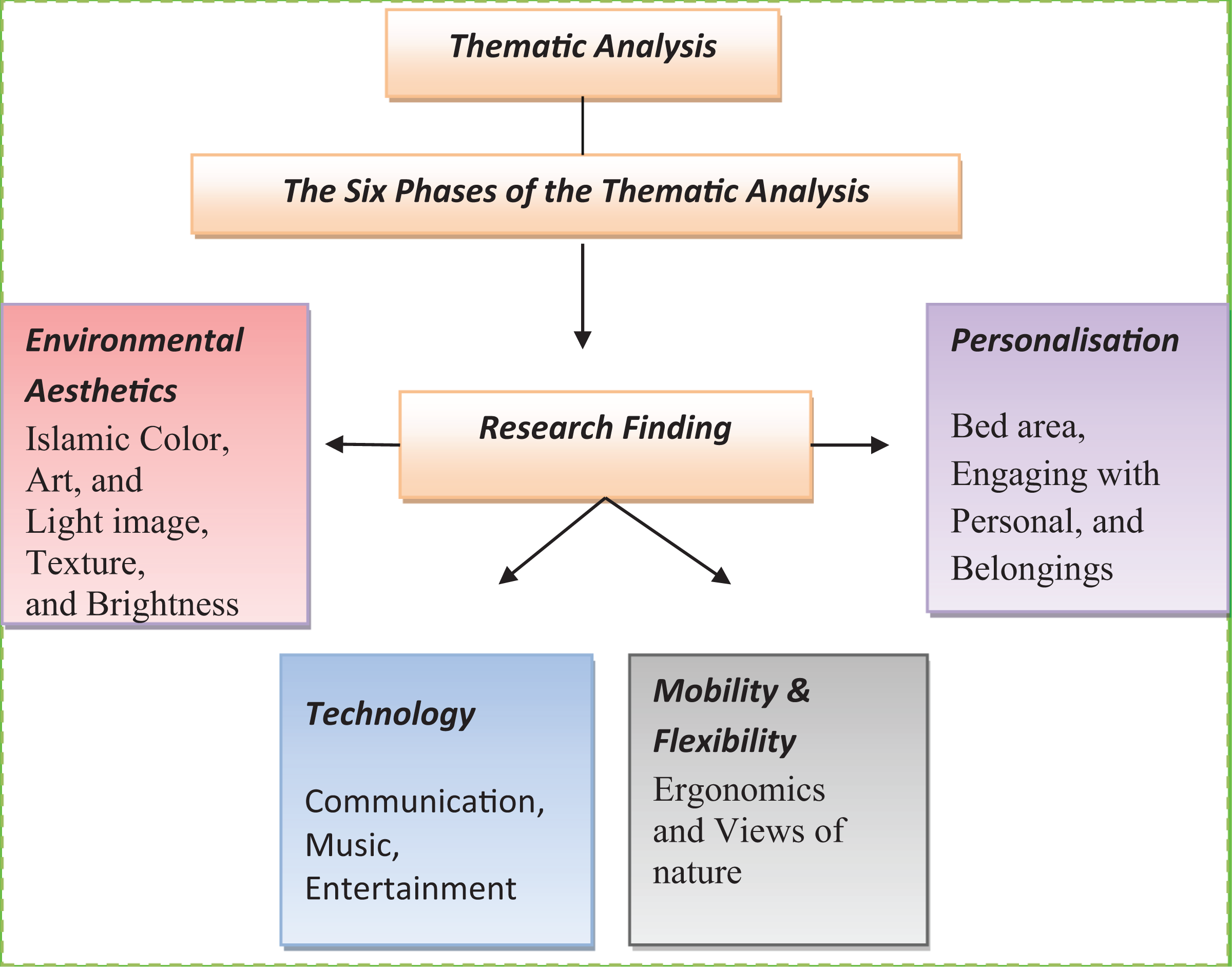
Keys of thematic analysis.
Environmental Behavior Theory
The conceptual framework developed in this study addressed the question of how planning and designing a single occupancy room in a hospital enhanced user satisfaction and well-being with the environment (see Figure 5).
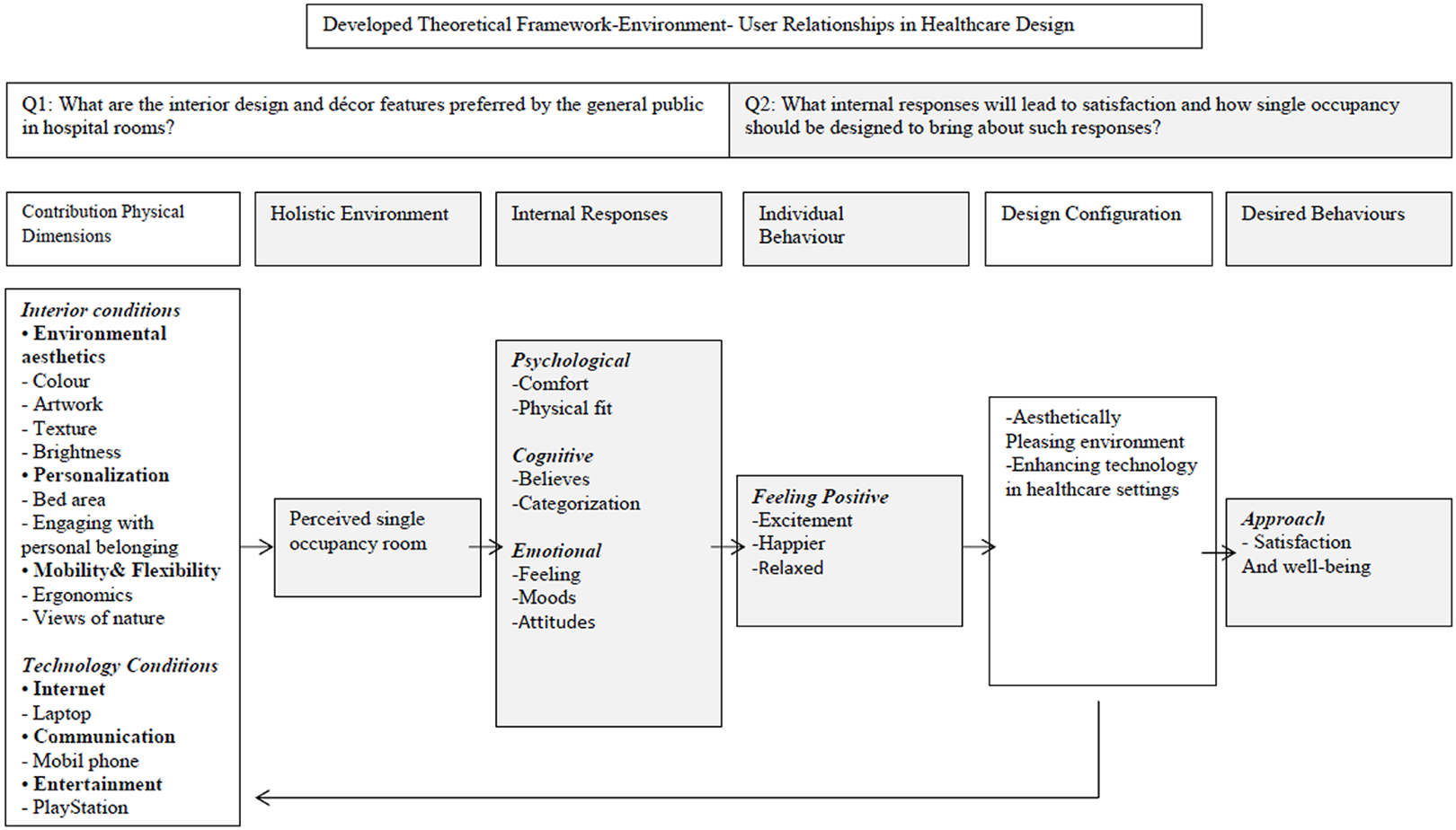
The developed conceptual framework by the author.
The findings of this study revealed four major aspects that mainly influenced satisfaction environmental design aesthetics, personalization, technology, and mobility/flexibility.
Environmental Aesthetics
Despite the lack of research, many design and healthcare professionals believe that aesthetically pleasing decor and artwork can influence and increase satisfaction with the environment (Fottler et al., 2000).
Islamic artwork, color, texture, and brightness were identified as the four aesthetic components that were particularly important to participant satisfaction. Creating aesthetically pleasing environments can enhance the healing process and improve patients’ well-being. The aesthetic characteristics identified as being particularly important to user preferences and satisfaction with hospital single occupancy in this study included wall color, use of artwork, texture, and brightness, all of which helped the participants maintain a positive frame of mind and remain positively engaged during their hospitalization. The four components in the room created a friendly and welcoming atmosphere for the participants. Art influenced participants in a pleasing and uplifting manner, as demonstrated from the excerpt presented below, which revealed the association between art and the way participants felt.
One participant said, “High quality art in healthcare pulls a person’s attention to the art and creates a positive distraction. Beautiful art is calming and uplifting.”
Thus, participants perceived art to increase happiness, and excitement, and helped them relax because the sentiments were linked to emotional responses. Therefore, instead of satisfying their own preferences and tastes, interior designers must select art chosen by participants, preferably art depicting nature, to adorn hospital rooms. Thus, enhancing positive internal emotional responses is vital to achieve desired behavior in single occupancy rooms.
Majority of participants (16 of 18) preferred light or cool color, which was associated with feelings of happiness, calmness, and made them feel welcomed. Participants indicated that brightness made them happy and relaxed. These internal cognitive responses to color and brightness of the room led to feelings of comfort, belief, and excitement.
Personalization
Allowing participants to personalize their bed areas such as having their own family photos, books, and a blanket brought from home allowed participants to experience a familiar environment during hospitalization in a single occupancy room.
Consistency in space, function, quality, and atmosphere of the hospital room promoted satisfaction, maintained a positive frame of mind, and enabled participants to remain positively engaged. Personalization with meaningful, familiar, and valued objects and aesthetic alterations of the room allowed participants to express their identity and reveal their interests.
One participant revealed that touching personal belongings provided pleasure and happiness. This finding emerged during a discussion on the type of furniture the participant preferred in the hospital room that was not planned in the consultation schedule. Participants indicated that personalization is a vital element that may help them adapt quickly to their new environment and pointed to having family photos or something of sentimental value increasing their satisfaction and happiness through their cognitive responses. Participants therefore responded through their perception of their hospital surroundings, which led to emotional responses that are important for healing in single occupancy rooms.
Mobility and Flexibility
Allowing participants to have wheeled furniture provided mobility and flexibility enabled participants confined to the hospital room to have control, express their interests, and feel comfortable with the room layout. Improved mobility and flexibility influenced patient behavior and having control over the environment led to relaxation and increased satisfaction. Since these psychological responses are affected by user comfort and physical fitness, the interior designer should consider these elements when designing the room so as to achieve the desired behavior and satisfaction in patients.
Technology
The use of the internet, mobile phone, and computer games connected participants to the outside world, reduced the strangeness of hospitalization, and made them feel less detached from their normal lives outside the hospital. Technology influenced behavior through internal physiological responses and in this study, led to participant comfort, which was a novel finding.
Discussion
The purpose of this study was to understand the preferences among participants of this study with regard to the interior design based on Islamic religious themes in hospital single occupancy rooms with the goal of using the data from the thematic analysis to propose transformation in the healthcare environment. To achieve this goal, data from 10 participants on aesthetics of a single occupancy hospital room including color and brightness based on Islamic religious themes, personalization, mobility, flexibility, and technology were included in the thematic analysis.
Summary of Finding: Research Question 1
Overall, the thematic analysis showed that participants made relevant, unique, and useful suggestions concerning Islamic design concepts that may have an impact on interior designs of hospital rooms in the Middle East. The use of 3D-CAD during consultations allowed participants to visualize their concepts, thereby simplifying the task. Key among the findings were participants’ preference for an aesthetically pleasing hospital room, which included art and bright colors associated with Islam, window views, and the need for personalization, technology, mobility, and flexibility. These features improved participant satisfaction and happiness. Of these, participants’ preference for technology as a cause for satisfaction and happiness was a novel finding, since no corresponding observation has been previously reported in the literature. Previous studies have shown the use of technology only for treatment purposes (MacAllister et al., 2016). The ability to use a laptop, personal computer, and play online games provided entertainment and created a positive frame of mind. Therefore, based on the data from this study, it can be proposed that achieving comfort, positive distraction, excitement, and well-being is relatively easy with participant’s access to technology in the hospital room.
Summary of Finding: Research Question 2
The findings of this study revealed that participants perceived and responded to the hospital room design in three dimensions—physiological, cognitive, and emotional responses, which is supported by studies in environmental psychology (Fottler et al., 2000). Participants who viewed Islamic artwork in the hospital room responded emotionally, which was manifested as happiness and a positive frame of mind, suggesting that their perceptions of interior design features based on Islamic concepts led to emotional responses. Research within a hospital setting in Liverpool, UK, also showed an improvement in patient health, which was attributed to art in patient’s rooms (Cintra, 2001). There is evidence that images within abstract art, for example, make people feel positive and contribute to well-being (Ho et al., 2015).
Therefore, participant’s preference for certain facilities, furniture, materials, equipment, finishes, and features in a hospital room are functional requirements that should be considered for compatibility during the planning and designing stages since it leads to physiological responses in participants and results in improvement in health and well-being.
Diversity, inclusion, and health equity are considered vital to society’s well-being, and in order to understand the relationship between the Muslim patient and the healthcare environment, it is essential to understand that Muslim tradition requires a high degree of auditory and visual privacy (Kopec & Han, 2008). Importantly, because Islam requires followers to face a certain direction for prayer, designers can accommodate the needs of Muslim patients by keeping the northeast sections of the room free from clutter and distraction (Kopec & Han, 2008). Thus, adapting the patient’s spiritual and cultural needs to build flexibility into the hospital room design speaks into the core values of the organization entrusted with patient care.
The findings from the present study show that an interdisciplinary approach that integrates Islamic designers of hospital rooms and architects of hospital buildings can improve an understanding of how external factors such as culture and religion can affect health outcomes in the built environment. Similar to strides taken to understand the effect of built environment on mental health (Hoisington et al., 2019), the results of the current study emphasize the need to pursue this research for a comprehensive understanding of how Islamic art supports healing in a hospital setting.
Beauty is dependent on user knowledge, taste, and culture background, and thus, interior design may affect users’ senses (Dilani, 2001). Undoubtedly, the findings of the present qualitative study are generalizable to other environmental contexts. Individuals may react toward the environment by sifting impressions through their cultural backgrounds, and therefore, the interior designer should recognize cultural aspects that are relevant to the patients using hospital rooms. For example, cultural aspects of North Africa should be carefully considered during the planning stage for hospital rooms design include (i) the aesthetic value of Islamic art that portrays beautiful and high-quality motifs and ornamentation fulfills the psychological needs of hospital users (Othman, 2011); (ii) Islamic culture includes symbolic and religious elements that are ordinarily meaningful to Muslims since they have a therapeutic effect on the occupiers of hospital rooms (Obeidat, 2008); (iii) Ka’ba shapes: Islamic art is associated with four basic shapes: circle and interweaved circles, square, the star pattern, and multisided polygons—the square shape indicates the Ka’ba shape (The house of Allah; Obeidat, 2008); (iv) color: There are two important colors in the Muslim culture—green and white. For Muslims, it is considered highly important to remember their culture during difficult times, and it is believed that those colors are therapeutically positive for Muslims (Obeidat, 2008); (v) symbolic aspects: Symbolic aspects in the Middle East include colors, shapes, and pictures of Al-Masjed Al-Haram. Religious aspects include the inscriptions of Qur’an recitations and Athan for prayer that are extremely important for raising Muslims’ spirits and must be considered during the design stage (Obeidat, 2008); and (vi) pictures of mosques: Al-Masjed (Al-Haram) and Al-Masjed (Al-Aqsa) are associated with Islam and are believed to have a therapeutic effect (Obeidat, 2008).
Cultural differences within hospital single occupancy room between Libya and western nations such as the United Kingdom and United States are unknown and further research is needed to make cross-cultural comparisons, since the present study is the first of its kind ever conducted that focused on public preference in hospital single occupancy room.
Strengths and Limitations
An interpretive approach was adopted in this study, which is associated with the philosophy of meaningful interaction between the subject and the researcher (Neuman, 2003). Neuman (2003) defined the interpretive approach as the systematic analysis of socially meaningful action through the direct and detailed observation of people in their natural setting in order to arrive at understandings and interpretations of how people create and maintain their social worlds. Thus, the interpretive paradigm is based on the fact that human beings create meaning in their world and this meaning is constructed as a result of interaction between humans and their surroundings. The interpretive approach adopted in this study took into account the relationship between the subject and the researcher, who come into “communal contact” that is not possible under traditional research (Denzin, 1998). Next, the findings from this study can be implemented in hospital rooms within a community, provided that resources required for its implementation are identified and perhaps a microcosting approach can be utilized in future studies as demonstrated previously (Aldridge et al., 2020). A limitation of this study was the small number of participants due to the war in Libya and concern for the safety of staff and participants.
Design Guidelines for Healthcare Practitioners
The guidelines of this study were design for practitioners and hospital to consider in order to improve patients satisfaction and well-being (Gashoot, 2012). The basic design principles are incorporated into this study recommendation. Those are proportion, scale, harmony, rhythm variety, contrast, and balance. An outline of those basic standards was given in this article. Designing a single occupancy room required a consultation with the user of the environment. In this research study, the necessary information was gathered during the consultation session that contributed to the important information.
3D Design of Hospital Rooms
A 3D design of single occupancy rooms was created (see Figure 6, which was guided by the findings of this research). User preferences are incorporated along with the findings into a set of recommendations for interior designers to use for the future design of hospital rooms.
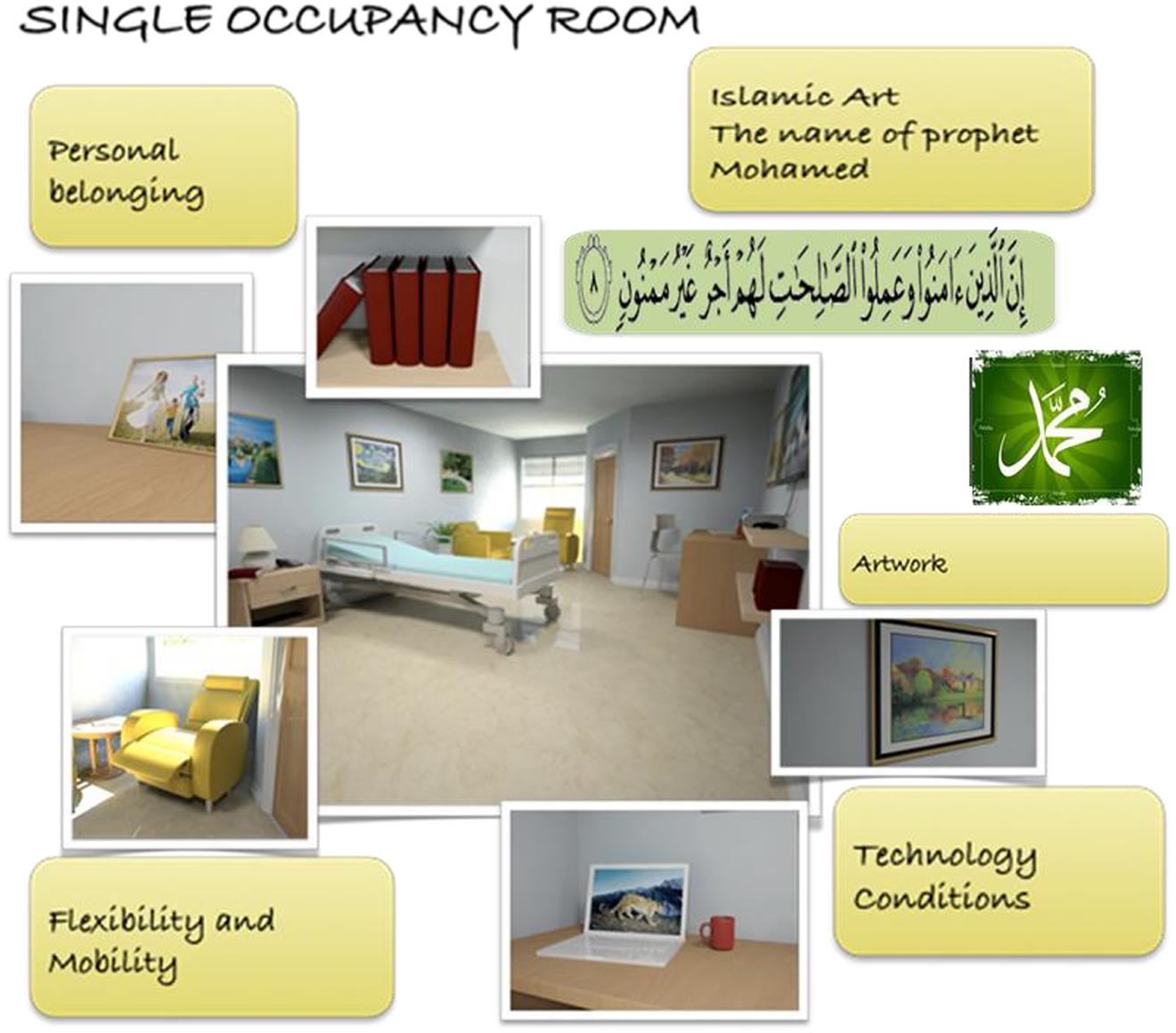
Overall findings of design in 3D.
The recommendation and guidelines are described for interior designers to use as follows. This list of design elements will be combined together to create room design for user activities. Design theory of the physical environment served as a foundation for the design.
Furniture
Utilizing old furniture (style, material, and color) may not satisfy its user and may suggest to the user that the healthcare designer does not care about the occupier, and this can lead the user to lack of satisfaction with the hospital rooms. Light color furnishing interior is preferred in hospital room such as, sofa, bed, chest of drawers, bedside table, locker, television, bookcase, small dining table, and shelves for photographs.
Technology
The participants also preferred to have a TV point, video channel, PC laptop computer, and smoke detector as sources of satisfaction with hospital room design.
Lighting
Light is a very important element which enhances user satisfaction within the environment. Full attention must be given to the type and level of light. For example, sunlight maintains a balanced light which is essential for the growth and health of living things, including man therefore natural light should be provided in hospital rooms, and windows are a fundamental element in providing natural light
Color
Color should be used in single occupancy based on deep understanding of its message to the user of the environment. A cool color (blue, light green, and white) is a favored color because those colors create room brightness. A warm color such as (orange, red, or yellow) seems to be not the preferred color for hospital room. Overall, a blue green is a favored color for background and wall color.
Window views
Garden, nature views are preferred if possible. If the view from the window is a building or a car park, then an interior solution should be made by the interior designer, for instance, using digital views which can be seen from the inside and not from the outside.
Painting and art display
Visual art and light images are considered significant to the user’s satisfaction with the environment. Art is very important for two reasons; color can easily improve the excellence of the environment and art can improve the emotional feeling of well-being through supporting social interaction (Hesham, 2006). For example, using illuminating art murals mounted on the room ceiling over the beds could increase user satisfaction and provide pleasing environment and create positive distraction. Illuminating art on the ceiling could draw user attention away from thinking of being in hospital. Nature artwork painting is the user’s favorite, since it provides a source of entertainment and engagement, and colorful type of art that represents clear sky, river, and views of sea or harbor is user’s favorite.
Layout Arrangement of Single Occupancy
Layout arrangement of single occupancy hospital rooms should consider places for reading and writing, Islamic design, comfortable place for patient visitors, place for playing games within the room as requested by user, place for watching TV and relaxing, place for internet and laptop computer, light arrangement, wall color, artwork and painting, floor color and material, and accessories. The finding of this proves that providing the above could enhance the well-being, satisfaction of user.
Personalization as Design Element
The interior designer has to focus on modification to improve the hospital room design, which may promote healing and increase user satisfaction. Design modifications may include new ideas that may serve personalization in hospital room. Design interventions to personalize hospital rooms may have an impact on user satisfaction and well-being. Room should reflect the user’s personality; room furniture needs to convey user’s territory and personality; providing an area or shelves for personal belongings and family photos by utilizing digital frame and providing space for greeting cards will also provide a place attachment.
Design Practitioners and Design Transferability to Other Cultural
This refers to the possibility that what was found in one environmental context by qualitative research is applicable to another environmental context. In this research study, people may react toward the environment by sifting impressions through their cultural background (Farbstein & Kantrowity, 1978). What we consider to be beautiful is dependent on environmental user knowledge; tastes, culture background, and interior design may affect users’ minds and senses (Dilani, 2001). From culture perspectives, interior designer should consider cultural aspects which must be recognized, for instance, it is important to know how patients are using hospital rooms and how the design can assist its user. For example, in Libya, and North Africa, there are many cultural aspects that should be carefully considered during the planning stage for hospital rooms design (Gashoot, 2012), which has been discussed in the following section.
Culture Islamic design elements
Islamic art contains aesthetic value in its high quality portrayal of motifs and ornamentation (Othman, 2011). This kind of art is believed to have the aesthetic quality of beauty which fulfills the psychological needs of hospital users (Othman, 2011). Islamic culture includes symbolic and religious aspects. These elements are ordinarily meaningful to Muslims since they have a therapeutically positive effect on the occupiers of hospital rooms (Obeidat, 2008). Ka’ba shapes: Islamic art is associated with four basic shapes: circle and interweaved circles, square, the star pattern, and multisided polygons. The square shapes indicate the Ka’ba shape (The house of Allah; Obeidat, 2008).
Islamic preferred color
There are two important colors for Muslim culture, green and white. For Muslims, it is considered highly important to remember their culture during difficult times, and it is believed that those colors are therapeutically positive for Muslims (Obeidat, 2008).
Symbolic aspects
Symbolic aspects in the Middle East include colors, shapes, and pictures of Al-Masjed Al-Haram. On the other hand, religious aspects include the inscriptions of Qur’an recitations and Athan for prayer. These aspects are extremely important for raising Muslims’ spirits and must be considered during the design stage (Obeidat, 2008).
Pictures of mosques
Al-Masjed (Al-Haram) and Al-Masjed (Al-Aqsa) are associated with Islamic enhance culture and these are believed to have a therapeutic effect (Obeidat, 2008).
Cultural differences between North Africa and others country, such as United Kingdom and United States, are unknown and further research is needed to make a cross cultural comparisons, since my research study was the first of its kind ever conducted that focused on public preference in hospital single room occupancy.
Conclusions
Physical setting in a single occupancy hospital room was found to influence participant behavior during hospitalization. Pleasant Islamic artwork, bright colors, window views, technology, personalization, mobility, and flexibility were significant factors that improved satisfaction by evoking physiological, cognitive, and emotional changes (see Figure 6).
A novel finding of this study was the use of technology as a physiological support that was deemed an essential requirement for physical comfort. Planning and creating an appealing single occupancy room is important for increasing user satisfaction and improving the quality of healthcare. Therefore, hospital room interior designers should be aware of and address the issue of aesthetics of single occupancy rooms to improve patient health and wellness.
Implications for Practice
The readers will be exposed to the concept of healing environments, specifically in a single occupancy hospital room.
The influence of Islamic art, particularly color, shapes, and pictures of mosques, in providing a healing space for believers admitted to hospitals in the Middle East is explored.
A qualitative analysis of thematic data from participants in Tripoli Medical Center revealed the outcome of aesthetically designed hospital single occupancy room on health and wellness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was a self-funded study.