
Abstract
Objectives:
Gaining an understanding of postoperative patients’ environmental needs, barriers, and facilitators for optimal healing.
Background:
An optimal hospital environment (the “healing environment”) can enhance patients’ postoperative recovery and shorten length of stay. However, insights lack into patients’ lived environmental needs for optimal healing after surgery and how these needs are being met.
Method:
A qualitative study was conducted between August 2016 and August 2017 with 21 patients who underwent elective major abdominal surgery in a Dutch university hospital. Data were collected through context-mapping exercises and interviews to capture patients’ lived experiences and explore the meaning of these experiences. Data were systematically analyzed according to the principles of thematic content analysis.
Results:
Three themes were identified. First, participants want a sense of control over their treatment, ambient features, privacy, nutrition, and help requests. Participants described the need for positive distractions: personalizing the room, connecting with the external environment, and the ability to undertake activities. Finally, participants expressed the importance of functional, practical, and emotional support from professionals, peers, and relatives. According to participants, the hospital environment often does not meet their healing needs while being hospitalized.
Conclusion:
The hospital environment often does not meet patients’ needs. Needs fulfillment can be improved by practical adjustments to the physical and interpersonal environment and considering patient’s individual preferences and changing needs during recovery. Patient narratives, pictures, and drawings are valuable sources for hospital managers in their efforts to design evidence-based environments that anticipate to patient-specific needs for achieving early recovery.
Keywords
Patients recovering from elective abdominal surgery usually spend several days on the general ward. During this period, they often suffer from postoperative pain accompanied by increased stress, sleep deprivation, and immobility (Apfelbaum et al., 2003; Kehlet & Dahl, 2003; Rosenberg-Adamsen et al., 1996). These conditions amplify each other, increase postoperative complications, and affect well-being and recovery of patients. For example, pain after surgery can lead to stress or anxiety (Desborough, 2000), altered sleep (Chouchou et al., 2014; Rosenberg-Adamsen et al., 1996), functional decline (Gan, 2017; Peters et al., 2007), and respiratory complications due to ineffective breathing (Chouchou et al., 2014). Inversely, disrupted sleep and anxiety may contribute to increased pain perception and hinder effective pain management (Chouchou et al., 2014; Vaughn et al., 2007). Moreover, psychological stress is associated with the disruption of biomarkers associated with wound healing (Walburn et al., 2009). Finally, minimal postoperative mobilization is associated with a higher probability of prolonged hospitalization (Daskivich et al., 2019). Altogether, effective management of pain, stress, sleep, and mobility is essential for patients’ well-being, optimal recovery, and shortening of hospitalization (Daskivich et al., 2019; Walburn et al., 2009).
Traditionally, pharmacological and therapeutic interventions are used to relieve postoperative pain and support the patient’s recovery process (Rawal, 2016). However, fueled by the limitations and potential side effects of these interventions (Oderda et al., 2007), there is increased attention for the need to design healthcare environments that positively affect the healing process and well-being of patients (Dijkstra et al., 2006; Ulrich et al., 2008), also known as healing environments. A healing environment is the complete environment of a patient that contributes to a whole person’s (physical, mental, social, and spiritual) healing (Jonas et al., 2014).
The movement of evidence-based design emerged to justify the adoption of healing environments in hospitals. Evidence-based design is, according to Ulrich et al. (2004), “a process for creating healthcare buildings, informed by the best available evidence, with the goal of improving outcomes” (p. 26). The design process starts with developing a hypothesis for which experiments and literature reviews are conducted to find correlations between the design of the environment and improved healthcare and patient outcomes. Design decisions are consequently made based on the best available knowledge (Stichler & Hamilton, 2008).
The creation of hypotheses as a basis for evidence-based design requires understanding of what patients themselves describe as environmental needs for achieving optimal healing and the factors that help patients in achieving those needs. However, few studies have examined the needs of hospitalized patients. Those studies used different methods to identify patient needs: retrospective analysis of surveys (MacAllister et al., 2019), literature reviews (Rigby et al., 2010), asking healthy participants to imagine being a patient and questioning their hypothetic needs (Andrade & Devlin, 2015), cocreation with patients (Lavender et al., 2020), discussing different environmental prototypes with patients (Patterson et al., 2017), and asking directly patients their opinion on design characteristics (Douglas & Douglas, 2004; Schreuder et al., 2016). All studies focus only on patients’ environmental perceptions in hindsight or do not even involve patients. As such, they fail to capture the actual, lived experiences of patients. The concept of lived experience flows from the philosophical tradition of phenomenology that aims to study experience from a first-person “embodied” point of view in its current environmental context (Ellis & Flaherty, 1994; Smith, 2013). To understand lived experience, it should be captured by the individual at the moment of experience. This could be done via context-mapping exercises (i.e., diaries, drawings, and photographs) and subsequent interviewing (Clandinin, 2006). This study aimed to identify patients’ environmental needs for postoperative healing, particularly of the ward and patient room, and the barriers and facilitators related to fulfilling these needs based on patients’ lived experiences and perceptions.
Method
Study Design, Setting, and Participants
We conducted a qualitative study at the Radboud university medical center, a Dutch university hospital, between August 2016 and August 2017. Standards for Reporting Qualitative Research (O’Brien et al., 2014) were followed to ensure study trustworthiness. Study participants were patients meeting the following criteria: (1) 18 years of age or older; (2) able to speak, read, and understand the Dutch language; (3) had elective major upper open abdominal surgery; and (4) were hospitalized for at least 3 days at the surgical nursing ward. Eligible patients were recruited at the surgical ward 1 or 2 days after surgery. We used purposive sampling to ensure a diversity of patients based on age, gender, type of hospital room (private vs. shared with other patients), and expected length of stay. The local ethics committee approved the study (study identification number: 2016-2693). Each participant provided written consent before study participation.
Data Collection
To capture the lived experiences of patients, they received at the beginning of their hospitalization a package containing a small booklet and a disposable camera. The booklet contained context-mapping exercises, including open-ended diary-like questions and drawing assignments (e.g., “please, draw your ideal patient room”; Figure 1 and Online Appendix 1). The camera was used to record experiences from a first-person point of view.
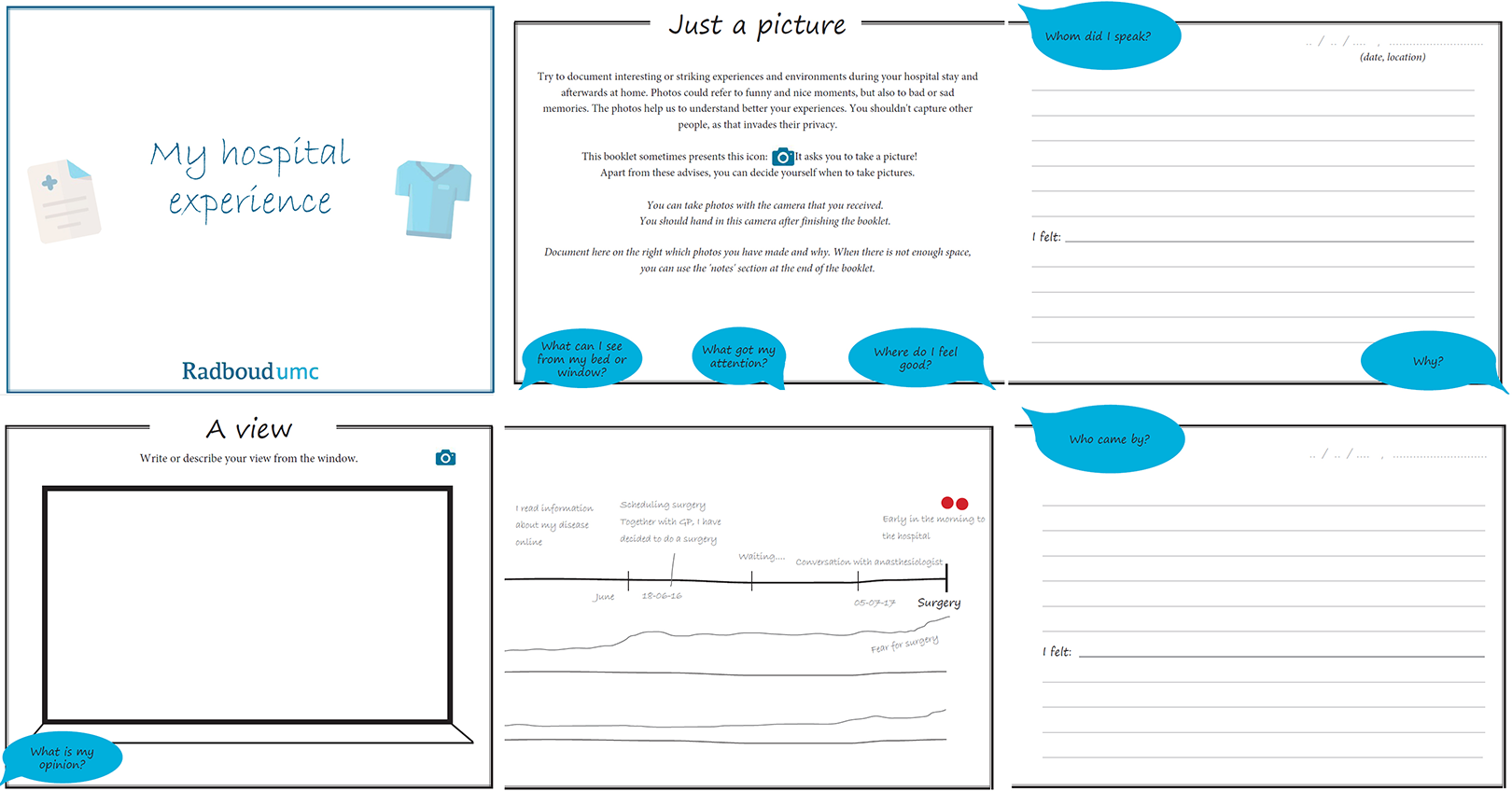
Selection of pages of the booklet with context-mapping exercises.
Subsequently, we conducted narrative interviews in the period from August 2016 to January 2017 to better explore patients’ lived environmental healing experiences during hospitalization. Nine narrative interviews were held at the patients’ homes, on average 2 weeks after hospital discharge. Two narrative interviews were held during admission. The interviews consisted of four phases to minimize interviewer impact on patient’s generated narrative: that is, introduction of the initial central topic, main narrative, questioning, and concluding talk (Wong & Hogan, 2016). The narrative interviews were conducted without prearranged questions except for one initial question: “Can you tell me what happened from the moment you were admitted for surgery until hospital discharge?” The context-mapping exercises helped during the interviews to better reaccess and reexpress experiences (Visser et al., 2005).
Finally, we conducted 10 in-depth interviews with another group of patients in the period from June to August 2017. All interviews were held during hospital admission. They were facilitated by a guide with open-ended questions and probes derived from the digitalized contents of the context-mapping exercises, the narrative interviews, and input from literature on conditions for an optimal healing environment (Dijkstra et al., 2006; Ulrich et al., 2004; Online Appendix 2). The narrative and in-depth interviews lasted 30–90 min. Researchers with a background in biomedical sciences (S. M. N.) and industrial design engineering (D. v. B.) conducted the interviews. Audio recordings of the interviews were transcribed verbatim.
Data Analysis
Context-mapping data and interview transcripts were systematically analyzed according to the principles of thematic content analysis (Braun & Clarke, 2006). Relevant data were identified and structured by open, a priori, axial, and selective coding. Coding is the interpretative process in which conceptual labels are given to data fragments. Two researchers (S. M. N., M. D.) independently coded the data to minimize subjectivity of findings. During the iterative analysis process, researchers frequently shared and discussed the meaning and uniqueness of the generated open codes. In consultation with two experienced qualitative researchers (G. H., T. H. v. d. B.), a codebook was developed and refined, codes belonging to the same concept were grouped into categories, and finally, themes were identified from the data. Data analysis was supported by using a qualitative data analysis software program (Atlas.ti Version 7.1.4).
Results
Forty patients were approached for this study. Nineteen did not participate for various reasons: that is, too sick, full focus on recovery, no interest, already participating in another study. Twenty-one patients participated in the study. All 21 completed the context-mapping exercises. Eleven participated in the narrative interviews and 10 in the in-depth interviews (Table 1). Interviewees’ perceptions and experiences were based on 2 weeks of hospitalization on average. Interviewees were evenly distributed across age. Eight shared a four-bed bay with three others; three of them spent the early postoperative days in a private room. Thirteen patients stayed in a private room for the whole hospital stay.
Baseline Characteristics of Study Participants.
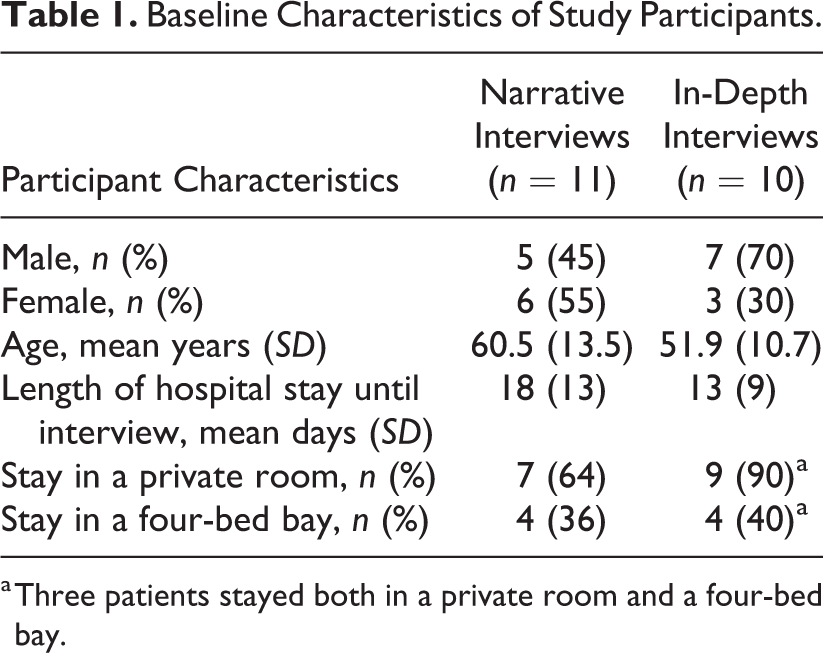
a Three patients stayed both in a private room and a four-bed bay.
Three themes, each with multiple categories, emerged from the data representing patients’ perceived environmental needs for postoperative healing and experienced barriers and facilitators related to fulfilling these needs: (1) sense of control, (2) positive distractions, and (3) an interpersonal healing environment. Table 2 provides an overview of the needs, barriers, and facilitators identified in this study.
Environmental Needs for Postoperative Healing and Related Barriers and Facilitators as Described by Patients.
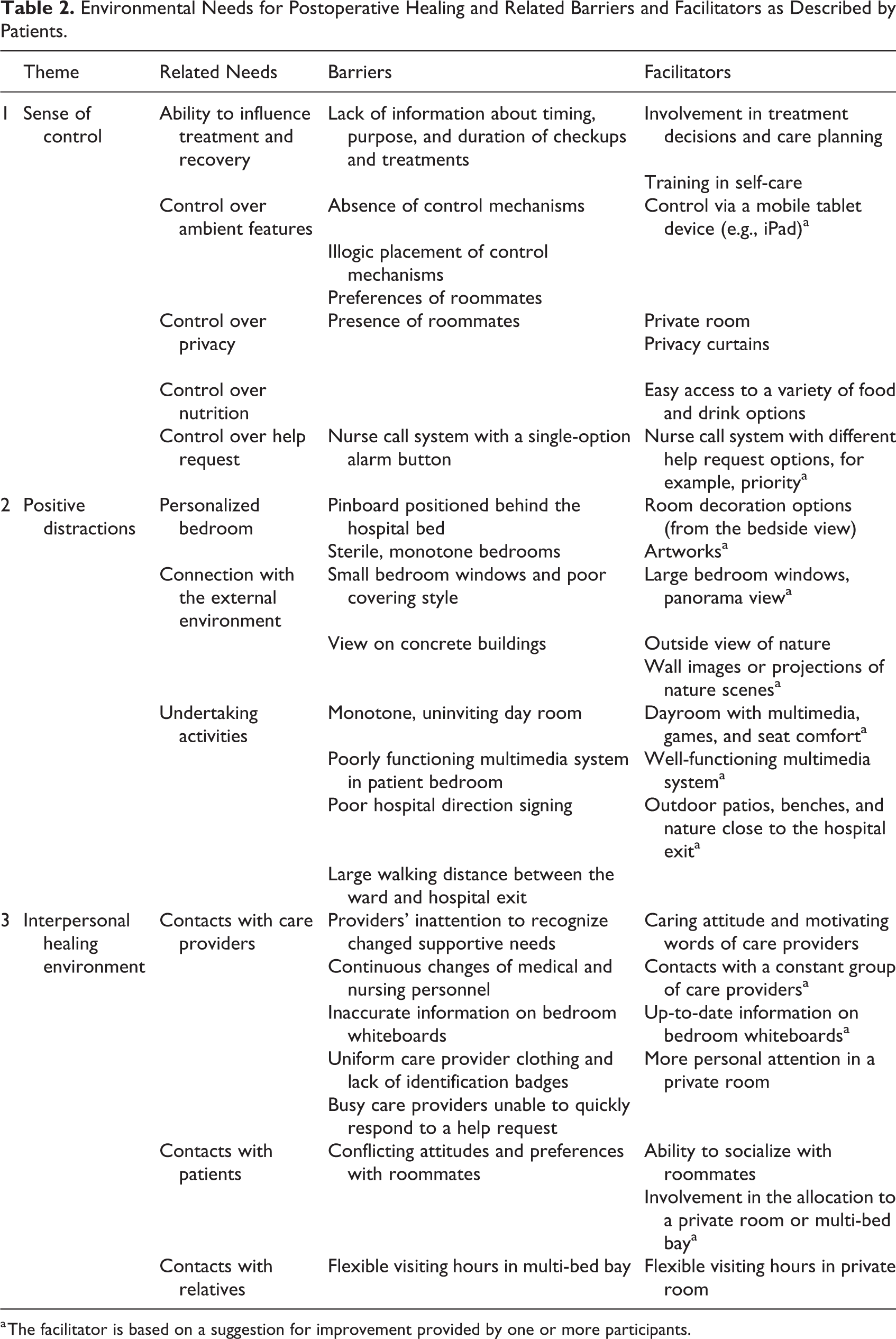
a The facilitator is based on a suggestion for improvement provided by one or more participants.
Theme 1: Sense of Control
Ability to influence treatment and recovery
Patients expressed that they were well-informed by their care providers about their health situation. They also felt involved in decisions regarding the treatment process. This involvement gave patients a sense of being able to influence their recovery. In addition, the support and encouragement received from care providers to learn self-care activities were valued as these activities increased levels of independence. “I want to do the stoma care myself. I know some people [other patients] don’t want that, but I insisted on doing it myself, because I want to be in control. I don’t want to depend too much on others” (SSI08). They expressed a preference for greater involvement in the planning of medical checkups and medication rounds to reduce the level of stress. Unexpected visits and treatments often left patients surprised and induced stress. Patients noted that more clarity in the timing and purpose of activities and in the estimated duration of visits and checkups probably would have made their recovery more comfortable.
Control over ambient features
The recovery of patients was positively and negatively influenced by several ambient factors such as light, sound, and temperature. The appreciation of ambient factors varied based on interviewees’ personal preferences and state of recovery. For example, hearing constant sounds from the hallway could give a sense of safety, whereas the sounds of medical devices (e.g., the beeping of an infusion pump running low), conversations, or footsteps could as well create irritation. Furthermore, sunlight entering the patient rooms could give energy to patients, while it could also disturb patients’ rest. “Sensing the presence of staff in the evening and night, because you hear them talking and working. This reassures me and gives me a comfortable feeling” (SSI01). Patients felt that they had limited possibilities to regulate or modify important ambient factors in their room in accordance with their preferences. Patients described depending on an automatic sunblind system and on the assistance of nurses to adjust the lights or room temperature or to close the door. The constant need for help from nurses and the preferences of roommates in shared rooms made patients reluctant to seek assistance and discouraged them from proactively changing ambient factors.
The illogical placement of light switches and devices hindered control, for example, managing the temperature or illumination. Switches or control devices in patient rooms were often perceived as difficult to access, especially when patients were confined to bed. Therefore, suggestions were made on alternative locations for switches and control devices closer to the bed and the use of a comprehensive and portable device (e.g., a mobile tablet device) to increase control over the ambient environment.
Control over privacy
Patients perceived privacy as an important aspect of recovery. Those who were hospitalized in a private room described the comfort of having their own bathroom and being able to do certain activities without worrying about being overheard or seen by others. They also felt in control of deciding when to isolate themselves from others. On the contrary, all interviewees who stayed in a four-bed bay experienced limited to no privacy, both in audio and visual privacy. They mentioned that their personal information could be easily overheard by others. This poor level of privacy could induce stress. “It’s like you are in the worst student dorm ever. No privacy and you are bothered all day long. But it’s part of the game, and after a couple of days you adapt” (NI04). Patients described isolating themselves from roommates, if needed, with the limited means they possessed in a four-bed bay. For instance, they closed the curtain to create privacy around their bed. Despite more visual privacy, this did not prevent them from possibly being overheard by others and created a feeling of being “locked up.” The lack of privacy, however, did not withhold patients from sharing personal information with care providers if needed.
Control over nutrition
It was felt that recovery benefited from the ability to make own choices about when and what to eat and drink. Patients liked the fact that they could select their preferred meal from a large variety of options and that food and drinks were offered multiple times per day. “The food service system is great. Food tastes good, it looks good (…) but also showing what is offered to you is fantastic” (NI10).
Control over help request
The nurse call button nearby was valued as important for control. Being able to quickly call the nurse for help provided them with a sense of safety. However, frustration was expressed on the “single-option” feature of the device which made patients sometimes hesitate to ask for help. Due to the device’s design and functionality, a nurse cannot distinguish between a life-threatening event and a simple question from the patient. Being able to indicate the urgency level of their help request could improve the use of such a device (Figure 2). “I would prefer an additional button. One for urgent matters and another one for help requests such as: ‘I’m hungry and I would like something to eat’” (NI03).

Impractical nurse call button—NI05: “The nurse call button is not practical for me.”
Theme 2: Positive Distractions
Personalized room
The need was expressed for positive distractions during hospitalization to be less focused on pain, worries, and stress. For example, it was much appreciated that patients could decorate their own room with presents or postcards received from friends and family. However, as the pinboard was positioned behind the bed, patients could not see the decorations and kind messages themselves. Therefore, the wall or door opposite of their beds was sometimes decorated (Figure 3).

Personalized door—SSI05: “A pinboard would have been nice.”
Patients expressed needs to personalize their room or personal space. Rooms were often negatively described as sterile, monotone, and white. A room with a warm ambience was preferred with a feeling being at home. This could be facilitated by artworks, for example, particularly intriguing ones that are worth looking at for a longer period. “I think you’ll go slightly mad when you have to stare at a white wall for 6, 7, 8 days or longer” (SSI09).
Connection with the external environment
Patients expressed their preferences concerning the window and the outside view. In general, they prefer to be better connected with the external environment. Without an outside view, the natural view was missed, which was perceived as missing a potential powerful distraction. Moreover, the current window size and covering style were mentioned to contribute to even more isolation. Large (panorama) windows were suggested as a better connection to the outside environment. Windows larger than the current ones would give patients a more comprehensive view of the outside world. Nevertheless, patients often accepted and understood that the size and shape of the hospital building made it impossible to answer to the view preferences of all patients (Figure 4).

The outside view (A) SSI06: “I can see over the trees (…) The view is good and calming.” (B) SSI05: “The outside view can be better (…) looks like a prison room.”
When a natural view from the window is not possible, it was suggested to use images or dynamic projections of natural scenes on the wall as an alternative to providing distraction. “Opposed to the bed there should be a depth effect, allowing you to look away. Something peaceful. A sea, forest, or mountains (…) allowing you to relate to nature and the outside world” (NI02).
Undertaking activities
To improve recovery and as a form of distraction, patients also expressed the need to undertake activities. This need was mostly expressed by patients during later phases of recovery in contrast to patients immediately after surgery. These patients mentioned needs for activities such as going for a walk to mobilize, getting some fresh air, and finding social distractions, either by talking to other people or just by observing people in the corridor. Although the hospital provides several opportunities to distract patients, each was considered to have its own flaws. For example, activities outside the hospital were difficult to undertake due to the large distance patients had to cover between the hospital ward and its nearest exit and the poor direction signing of the hospital. One patient, for example, mentioned being afraid to get lost, which discouraged him from leaving the ward. “You have to take the main hospital exit and cross a crowded square to find a few benches. And first, you have to get through a curtain of smoke because many people are smoking outside of the hospital” (NI10).
Moreover, patients expressed the need for a room to undertake social activities as having lunch with other patients or playing games (e.g., board games, jigsaw puzzles). Although such a “dayroom” already exists within the hospital, patients describe the room as monotone and uninviting (Figure 5).

Design of the dayroom—SSI10: “The dayroom looks rather sterile. Could be cozier and look like home.”
Finally, where the hospital offers a multipurpose device with TV, radio, and Internet access to facilitate entertainment and distraction from pain and worries, the technology was not always functioning well which could be frustrating for patients.
Theme 3: Interpersonal Healing Environment
Contacts with care providers
Patients perceived the contact with care providers as very important for their well-being and healing. They indicated that a caring attitude and the motivating words of providers helped to relieve stress, anxiety, and pain. Contact with physicians mostly helped to gain medical information and guidance to obtain a better understanding of and more confidence in one’s own health, medical treatment, and recovery. Contact with nurses was considered a very important first contact offering practical, informative, and emotional support. Furthermore, having contact with a constant group of familiar care providers helped patients to trust providers and know what they could expect from them. Interestingly, it was mentioned that more personal attention was perceived in a private room compared to that in a four-bed bay.
Where patients experienced benefits from the contacts with care providers, they also mentioned several factors that hinder healing support. First, due to the high workload of care providers, the providers were sometimes not able to quickly respond to a help request. Not knowing when they would receive support after requesting help was experienced as stressful. Patients also mentioned that seeing their care providers in a rather stressed state made them refrain from seeking help or care when needed. “I had to get used to how things work here. Super structured. (…) I noticed that because of the high administrative burden, there is less time for people in beds.” (SSI03).
Second, it was felt that care providers were inattentive to their changed supportive needs during the recovery process. While the need for functional support decreased during recovery, patients indicated that they could have benefited from an increase in emotional support by care providers. Patients mentioned that it took a while for them to realize what had happened and how their illness/surgery affected them physically and emotionally. They indicated that they had to bring better specific needs to the attention of their care providers.
Third, constant changes in medical or nursing personnel turned out to be confusing and worrisome for patients. For example, patients felt insecure about whom to address with their problems and complaints. They sometimes did not know whom to turn to in case of questions or whom they had spoken to after a visit. It was also found hard to discern the different types and roles of care providers, for example, due to the lack of identification badges or specific provider uniforms. Furthermore, it was felt irritating to repeat the same information to different care providers. “You have to find out yourself who is doing what. Who will bring you towels in the morning? (…) stuff like that. We see so many new faces. For us [patients] all faces are new when we wake up” (SSI09).
Finally, patients were confused by the inaccurate and outdated information on their whiteboard (e.g., describing today’s on-duty staff, patient’s nutrition status, special remarks).
Contacts with other patients
The need for contact with other patients seemed to depend on the phase of recovery and personality of a patient. Especially during the initial postoperative phase—when they felt sick and in need of rest—patients did not experience a need to have contact with other patients. There were also patients who wanted minimal contact because they disliked listening to other people’s problems or stories.
Other patients—often referring to their later phase of recovery—preferred communication with peers. They pointed out the benefits of staying with multiple patients in a hospital room: being able to support each other emotionally and practically, sharing experiences, and keeping an eye on each other. The possibility to interact with fellow patients or relatives was also seen as a positive distraction from their current health situation and a helpful way to pass time. These positive experiences, however, largely depended on the personality, health condition, and preferences of the people the patients had to share their room with. Patients described that more involvement in the allocation or relocation from or to a private or four-bed bay could reduce stress and fasten recovery. “I do not want to exaggerate but I think that being in a four-bed bay resulted in three to four days of extra recovery. It takes so much energy, all the stimuli” (NI07).
Contacts with relatives
The contacts with family and friends during hospitalization were valued. Aside from being a positive distraction from pain, anxiety, and boredom, talking with relatives helped patients to cope with their health situation. Patients who stayed in a private room appreciated having autonomy in deciding when to receive visitors. In their view, the flexible visiting hours at the ward allowed visitors to come from distant places, and it allowed patients to plan their rest moments themselves. On the other hand, patients in a four-bed bay mentioned that the flexible visiting hours induced stress and fatigue because visits were allowed the whole day. They indicated not having the courage to ask visitors from other roommates to leave even when they needed to rest (Figure 6).

Crowded room by patient visits—NI08: “It’s often very crowded, while I really need more rest.”
Discussion
Our study findings contribute to an increased understanding of postoperative recovery by emphasizing that—besides a clinical perspective—a broader perspective is needed to improve postoperative recovery. Participants’ descriptions of healing needs including sense of control, positive distractions, and support from professionals, peers, and relatives are congruent with theories of healing environments (Hole et al., 2015; Laursen et al., 2014; Ulrich et al., 2008). These theories identify stress and pain reduction as primary pathways to healing and suggest that the physical and interpersonal environment should support patients in achieving their healing needs. Through their lived experiences, we learned that these healing needs of patients are not always met. First, practical limitations related to the physical environment (e.g., poor positioning of controls, inefficient design of alarm buttons, and lack of privacy) can hinder the patient’s sense of being in control. These practical limitations are relevant since lack of control is often associated with stress-induced symptoms such as depression, passivity, and elevated blood pressure (Ulrich, 1991). Second, the design and interior of patient rooms can hinder patients in finding positive distractions. Previous studies have underlined the importance of distraction to reduce pain and stress (Dijkstra et al., 2006; Huisman et al., 2012; Laursen et al., 2014; Ulrich et al., 2008). Current hospital infrastructures can also limit positive distractions. Wayfinding and acceptable walking distances for patients are important to avoid frustration and disorientation, which in turn may lead to stress (Pati et al., 2015). Third, constant work shifts, high workload, and care providers’ main focus on clinical issues at the ward can hinder a patient’s feeling of receiving sufficient and timely practical and emotional support. Moreover, it can also obstruct patients from being well-informed on issues related to their recovery. All are important mechanisms for enhancing healing and well-being (Miller & Crabtree, 2005; Sakallaris et al., 2015) and engaging patients in their recovery (Gillis et al., 2017). In addition to a better insight into environmental needs, barriers, and facilitators for optimal healing, this study contributes to the understanding that patients’ healing needs often change during the postoperative period. Moreover, effects of environmental stimuli on healing may vary per person as they also largely depend on patient-specific factors such as personality, cultural background, and cognitive and affective capacities (Dijkstra et al., 2006). It is, therefore, not possible to develop an “one-size-fits-all” healing environment. Professionals need to anticipate on these shifting needs by taking into consideration the optimal healing environment for a specific patient in his or her recovery phase (i.e., need for activities, focus on functional or emotional support, sound or silence).
Limitations
Our study has several limitations. First, the relatively small sample of participants from only one tertiary referral hospital limits an immediate generalizability of our findings to other (types of) hospitals with a different patient population. Although this was a major limiting factor, we deliberately chose to use budgeted research time and capacity for one setting to perform a multimethod in-depth inquiry. This allowed us to capture our patients’ lived experiences and perceptions, increase the trustworthiness of our findings, and gain a comprehensive understanding of our patients’ healing experiences (Carter et al., 2014). Nevertheless, as many hospitals in developed countries have private rooms and two-bed and four-bed bays and share commonalities in their designs, nursing wards, and contacts between patients and healthcare professionals, our findings may apply outside the Netherlands and to nonacademic hospitals.
Second, although we purposively sampled participants to ensure diversity of opinions and experiences, we were only able to include patients who stayed in a private or four-bed bay. Insights from patients who stayed at a room with only one other patient could have provided a more nuanced view on preferences for a private versus multiperson room. Moreover, most of the participants were aged 50 years and older and had a relatively long hospital stay due to several postoperative complications. This population may have a different recovery process and may desire a different healing environment than younger patients and/or patients with a shorter hospital stay. Finally, as we aimed to understand patients’ lived experiences, we have not gained evidence yet on the efficiency of changing environment design for optimal healing.
Conclusion
This study contributes to the increased understanding of what surgical patients experience with respect to and need from their environment to optimize healing. The fulfillment of patients’ healing needs can often be facilitated by very practical adjustments to the physical and interpersonal environment they are recovering in. To create an optimal postoperative healing environment, hospitals and professionals also need to anticipate on patient’s individual preferences and shifting healing needs while being hospitalized. We believe our study findings are valuable for managers and professionals in a variety of hospitals and surgical wards in their efforts to support their patients during recovery after surgery. Following evidence-based design, more research is now needed—involving quantitative methods, a larger study sample with patients varying in ages and multiple study sites (e.g., different bedroom sizes, types of hospitals)—to determine associations between patients’ postoperative recovery and perceived healing environmental factors and to find explanations for potential differences among hospital and patient types. As a result, hospital management and professionals will be better able to make evidence-based decisions on changing or maintaining hospital layout and equipment.
Implications for Practice
An optimal hospital environment can enhance patients’ postoperative recovery and shorten length of stay. Careful consideration of the design of the hospital environment is therefore required.
The hospital environment should provide patients with control over their treatment and recovery, ambient features, privacy, nutrition, and help requests.
The hospital environment should provide patients with positive distractions via a personalized bedroom, connection with the external environment, and ability to undertake activities.
Good contacts between patients and care providers, other patients, and relatives are an important element of the interpersonal healing environment.
Needs fulfillment of patients can be improved by practical adjustments to the physical and interpersonal environment and considering individual preferences and changing needs of patients during the recovery process.
Supplemental Material
Supplemental Material, sj-doc-1-her-10.1177_1937586719900885 - Environmental Needs, Barriers, and Facilitators for Optimal Healing in the Postoperative Process: A Qualitative Study of Patients’ Lived Experiences and Perceptions
Supplemental Material, sj-doc-1-her-10.1177_1937586719900885 for Environmental Needs, Barriers, and Facilitators for Optimal Healing in the Postoperative Process: A Qualitative Study of Patients’ Lived Experiences and Perceptions by Gijs Hesselink, Merlijn Smits, Mariël Doedens, Sharon M. T. Nijenhuis, Denise van Bavel, Harry van Goor and Tom H. van de Belt in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-docx-1-her-10.1177_1937586719900885 - Environmental Needs, Barriers, and Facilitators for Optimal Healing in the Postoperative Process: A Qualitative Study of Patients’ Lived Experiences and Perceptions
Supplemental Material, sj-docx-1-her-10.1177_1937586719900885 for Environmental Needs, Barriers, and Facilitators for Optimal Healing in the Postoperative Process: A Qualitative Study of Patients’ Lived Experiences and Perceptions by Gijs Hesselink, Merlijn Smits, Mariël Doedens, Sharon M. T. Nijenhuis, Denise van Bavel, Harry van Goor and Tom H. van de Belt in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_1937586719900885 - Environmental Needs, Barriers, and Facilitators for Optimal Healing in the Postoperative Process: A Qualitative Study of Patients’ Lived Experiences and Perceptions
Supplemental Material, sj-pdf-1-her-10.1177_1937586719900885 for Environmental Needs, Barriers, and Facilitators for Optimal Healing in the Postoperative Process: A Qualitative Study of Patients’ Lived Experiences and Perceptions by Gijs Hesselink, Merlijn Smits, Mariël Doedens, Sharon M. T. Nijenhuis, Denise van Bavel, Harry van Goor and Tom H. van de Belt in HERD: Health Environments Research & Design Journal
Footnotes
Authors’ Note
Gijs Hesselink and Merlijn Smits shared first authorship. All authors had full access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.