
Abstract
Aim:
To use Value-Focused Thinking to investigate what is important in the design of inpatient stroke rehabilitation facility buildings.
Background:
Many stroke patients require inpatient rehabilitation in a dedicated facility. Rehabilitation facilities are healthcare spaces, but they are also learning spaces where patients practice targeted tasks to acquire new skills and to reacquire skills and abilities that were compromised as a result of their stroke. There is currently no consensus regarding how the design of inpatient rehabilitation facilities could be optimized for patients’ learning.
Method:
We used Value-Focused Thinking to develop a framework of what interdisciplinary experts consider important for inpatient stroke rehabilitation facility design. Two workshops were conducted. The following experts were invited to participate: past patients with experience of stroke rehabilitation; stroke rehabilitation clinicians; stroke rehabilitation academics; healthcare environments academics; learning environments academics; architects, designers, and wayfinders with experience designing healthcare or learning environments; and healthcare design policy makers.
Results:
Thirty experts participated. The experts’ final framework included 16 criteria that were considered fundamentally important for inpatient stroke rehabilitation facility design, and 14 criteria that were considered instrumentally important. Inpatient stroke rehabilitation facility design should maximize efficiency, maximize effectiveness (i.e., patients’ clinical and functional outcomes), foster emotional well-being, and maximize safety. Opportunities to practice physical, cognitive, and social activity were considered important for patients’ outcomes.
Conclusions:
Value-Focused Thinking was an effective and equitable means of engaging experts from multiple disciplines. Designers, planners, and developers of inpatient stroke rehabilitation facilities should consider the rehabilitation-specific framework developed in this study alongside evidence from other healthcare settings.
Keywords
Each year, over 50 million people worldwide have a stroke (Thrift et al., 2017). After receiving acute care in hospital, 75% of stroke survivors have ongoing rehabilitation needs, which are often provided in a dedicated inpatient rehabilitation facility (Stroke Foundation, 2017). The aim of this study was to describe what should be prioritized in the design of inpatient stroke rehabilitation facilities.
Rehabilitation is defined as “a process of active change by which a person who has become disabled acquires the knowledge and skills needed for optimal physical, psychological and social function” (British Society of Rehabilitation Medicine, 2003, p. 7). This definition emphasizes that rehabilitation is a learning process. The impact of stroke can be wide-ranging, and no two strokes are the same; commonly, patients in stroke rehabilitation may need to relearn motor skills (e.g., walking and/or arm-use) and/or cognitive abilities (e.g., speaking or understanding speech, planning and execution of everyday tasks). In addition, they may need to learn entirely new skills in response to their changed condition (e.g., learning to use a walking frame). Clinical guidelines for stroke rehabilitation recommend cognitive stimulation, physical exercise, and repetitive goal-directed practice to promote optimal relearning (Stroke Foundation, 2017; Winstein et al., 2016). Unfortunately, stroke patients in inpatient rehabilitation facilities are largely inactive and alone (West & Bernhardt, 2012) and frequently bored (Kenah et al., 2017). When designing this study, we took the novel position that stroke rehabilitation facilities could be reconceptualized as learning environments as well as healthcare environments where patients are enabled to engage in and practice the necessary physical, social, and cognitive functions to achieve optimal recovery after stroke.
Most healthcare design research is conducted in acute settings (Ulrich et al., 2008). General hospital design guidelines and regulations should inform rehabilitation facility design, but rehabilitation-specific recommendations are also needed. Only a handful of empirical studies have considered the built environment of inpatient stroke rehabilitation facilities (Anåker, von Koch, Sjöstrand, Bernhardt, & Elf, 2017; Blennerhassett, Borschmann, Lipson-Smith, & Bernhardt, 2018; Janssen et al., 2014; Katrak et al., 2011; Khan et al., 2016; Mackey, Ada, Heard, & Adams, 1996), so the unique requirements of these environments for people who have had a stroke are not well documented or understood.
Many stakeholder perspectives must be considered if we are to develop a shared understanding of how stroke rehabilitation facility design could be optimized for learning. We followed the definition of interdisciplinarity adopted by Choi and Pak (2006)—to “analyze, synthesize and harmonize links between disciplines into a coordinated and coherent whole” (p. 354)—and aimed to synthesize the perspectives of stroke patients, clinicians, policy makers, architects and designers, health environments researchers, and learning environments researchers. Importantly, we involved learning environments experts in this research to help to reconceptualize rehabilitation spaces as learning spaces. The design of schools and universities is shifting from classroom-based learning to innovative spaces that encourage collaboration and social participation and consider issues of health, comfort, safety, and stimulation (Organisation for Economic Cooperation and Development, 2011). The original contributions of this study were to (1) develop a framework of what experts think is important in the design of inpatient stroke rehabilitation facilities, (2) reconceptualize rehabilitation facilities as learning environments, and (3) apply Value-Focused Thinking to facilitate systematic, interdisciplinary design research.
The Value-Focused Thinking Approach to Decision-Making
Value-Focused Thinking is an approach for making better decisions (Keeney, 1992). It encourages decision makers to consider what they want (i.e., what they value) before considering how they can get what they want (i.e., the possible alternatives; Keeney, 1992). “Values” are defined as the things decision makers think are important in a particular decision-making context (Keeney, 1992). The decision-making context for this study was: What is the optimal design of inpatient stroke rehabilitation facilities? A person taking an alternative-focused approach to this decision would compare different existing rehabilitation facility designs and decide which one is best. A person taking a Value-Focused Thinking approach would first define what is important, or of value, in the built environment of rehabilitation facilities before comparing alternative designs.
Value-Focused Thinking requires users to articulate their values as “objectives,” where an objective is a statement of what would ideally be achieved in the decision-making context (Keeney, 1992). Keeney (1992) described a distinction between fundamental objectives and means objectives. Fundamental objectives are fundamentally important in and of themselves. Means objectives are instrumentally important because they help to achieve one or more of the fundamental objectives. Fundamental objectives are organized into a hierarchy, and means objectives are organized into a network that feeds into the hierarchy of fundamental objectives.
Method
Value-Focused Thinking was used to identify what interdisciplinary experts consider important in the design of inpatient stroke rehabilitation facilities. The Value-Focused Thinking process was conducted over two workshops in late 2017. This project received ethical approval from the University of Melbourne, Australia (ID: 1648218.1).
Workshop Participants
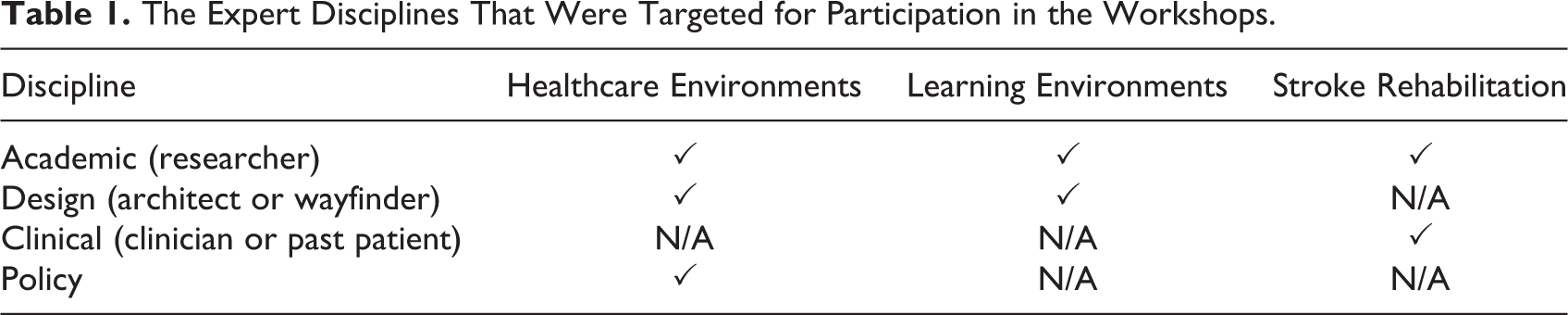
The workshop participants were selected using impressionistic modal instance sampling (Salkind, 2010). Target disciplines were chosen, and experts in these disciplines were invited to participate, so that all of the predetermined disciplines were represented in the final sample. The target disciplines were patient consumers with lived experience of stroke rehabilitation; stroke rehabilitation clinicians; stroke rehabilitation academics; healthcare environments academics; learning environments academics; architects, designers, and wayfinders with experience of designing healthcare environments or learning environments; and healthcare design policy makers (see Table 1). Experts were identified through existing collaborative networks known to the researchers. Preference was given to people with expertise in two or more of the target disciplines. All participants completed a consent form and a questionnaire about the nature and extent of their expertise.
The Expert Disciplines That Were Targeted for Participation in the Workshops.
Workshop Format
The workshops ran for 4.5 hr each and were facilitated by authors Lipson-Smith (student researcher) and Churilov (Value-Focused Thinking expert). Prior to Workshop 1, participants were given a prereading document with background on stroke rehabilitation and Value-Focused Thinking, links to key references, and a glossary of jargon specific to the participants’ various disciplines. Glossaries are needed in interdisciplinary research to recognize and explain discipline-specific language and ways of knowing (Newton & Fisher, 2009). The glossary was added to throughout the workshops, and participants were encouraged not to use acronyms or jargon. The workshops were audio-recorded to assist with analysis.
Workshop 1
The priority for Workshop 1 was to develop a hierarchy of fundamental objectives. Participants were divided into four interdisciplinary workgroups and were asked to brainstorm what they value as important in the design of inpatient stroke rehabilitation facility buildings. Participants were encouraged to focus on concepts rather than be constrained by specific design solutions or features. Each workgroup articulated their values as objectives and then interrogated each objective using the four questions in Figure 1 (Clemen & Reilly, 2014). These questions were thus used to identify the fundamental objectives and to organize them into a hierarchy. The participants’ goal was to define a set of fundamental objectives that were mutually exclusive of each other (i.e., no overlap in meaning or content between the objectives) and collectively exhaustive (i.e., the final set of objectives should together cover everything that is fundamentally important in the design of inpatient stroke rehabilitation buildings). Each workgroup’s hierarchy was refined iteratively throughout the workshop in response to feedback from other participants. After Workshop 1, the four workgroups’ hierarchies were combined into one synthesized hierarchy by Lipson-Smith (see Analysis section) and circulated to all participants. Participants were encouraged to review the hierarchy before Workshop 2 and provide feedback. Experts who participated in Workshop 2 but not Workshop 1 were given a summary prior to Workshop 2.
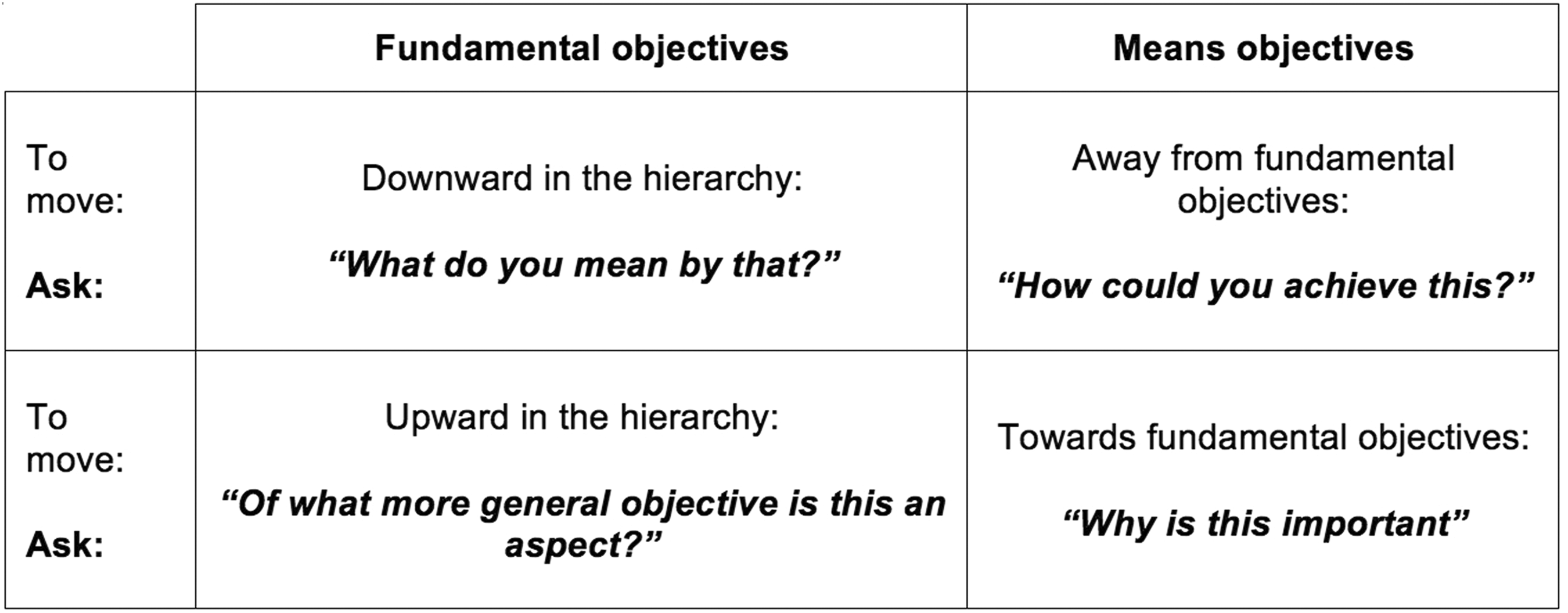
Four questions to structure the Value-Focused Thinking process. This figure shows the four questions that were used in the workshops and during analysis to identify the fundamental objectives and to organize them into a hierarchy. This figure is adapted from Clemen and Rielly (2014).
Workshop 2
A final version of the synthesized hierarchy of fundamental objectives was presented, and the participants discussed the means objectives that may be important in achieving each of the fundamental objectives. For each means objective, the participants identified which other objective/s it may impact and thereby developed a draft network. The draft network was refined after Workshop 2 (see Analysis section) and circulated to all participants.
Analysis
Synthesizing the hierarchy of fundamental objectives
To synthesize the four workgroups’ hierarchies, Lipson-Smith studied the written output and audio recordings from Workshop 1. Identical or similar fundamental objectives were combined, and the questions in Figure 1 were used to confirm the position of each objective in the hierarchy or to relegate it to the network of means objectives. All of the fundamental objectives identified in Workshop 1 were represented within the final, synthesized hierarchy. The workshop audio recordings were used to create detailed definitions for each of the fundamental objectives. The hierarchy was reviewed by authors Churilov and Bernhardt before being sent to participants for feedback. Disagreements were discussed until consensus was reached.
Refining the network of means objectives
Lipson-Smith referred to written output and audio recordings from Workshop 2 to refine the network of means objectives. Identical or similar means objectives were combined, and objectives that were considered subsidiary were incorporated into the definition of another objective or represented by connections between objectives. Everything that was discussed in the workshops was thereby included in the final network. The hierarchy, network, and accompanying definitions together constitute the framework of what is important for inpatient stroke rehabilitation facility design. The framework was reviewed by Churilov and Bernhardt before being sent to participants for feedback. Disagreements were discussed until consensus was reached.
Results
Workshop Participants
Thirty-seven experts were invited to attend the workshops. One expert in a policy/government role did not respond when approached. Six experts declined due to scheduling conflicts (two architects, two clinician/researchers, one architect/researcher, and one architect with a clinical background). People with similar expertise were then approached to replace them. Thirty experts consented to participate, and all attended at least one workshop. Table 2 shows the primary expertise of the participants, and Table 3 details the nature and extent of their expertise.
The Number of Participants Representing Each Target Discipline.
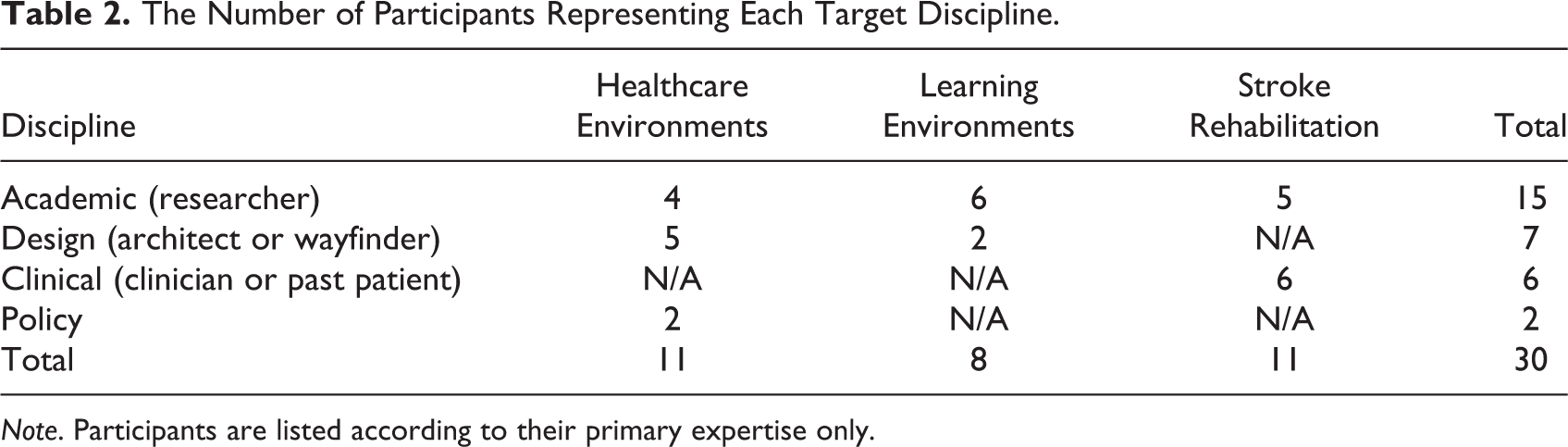
Note. Participants are listed according to their primary expertise only.
The Type and Extent of the Workshop Participants’ Expertise.
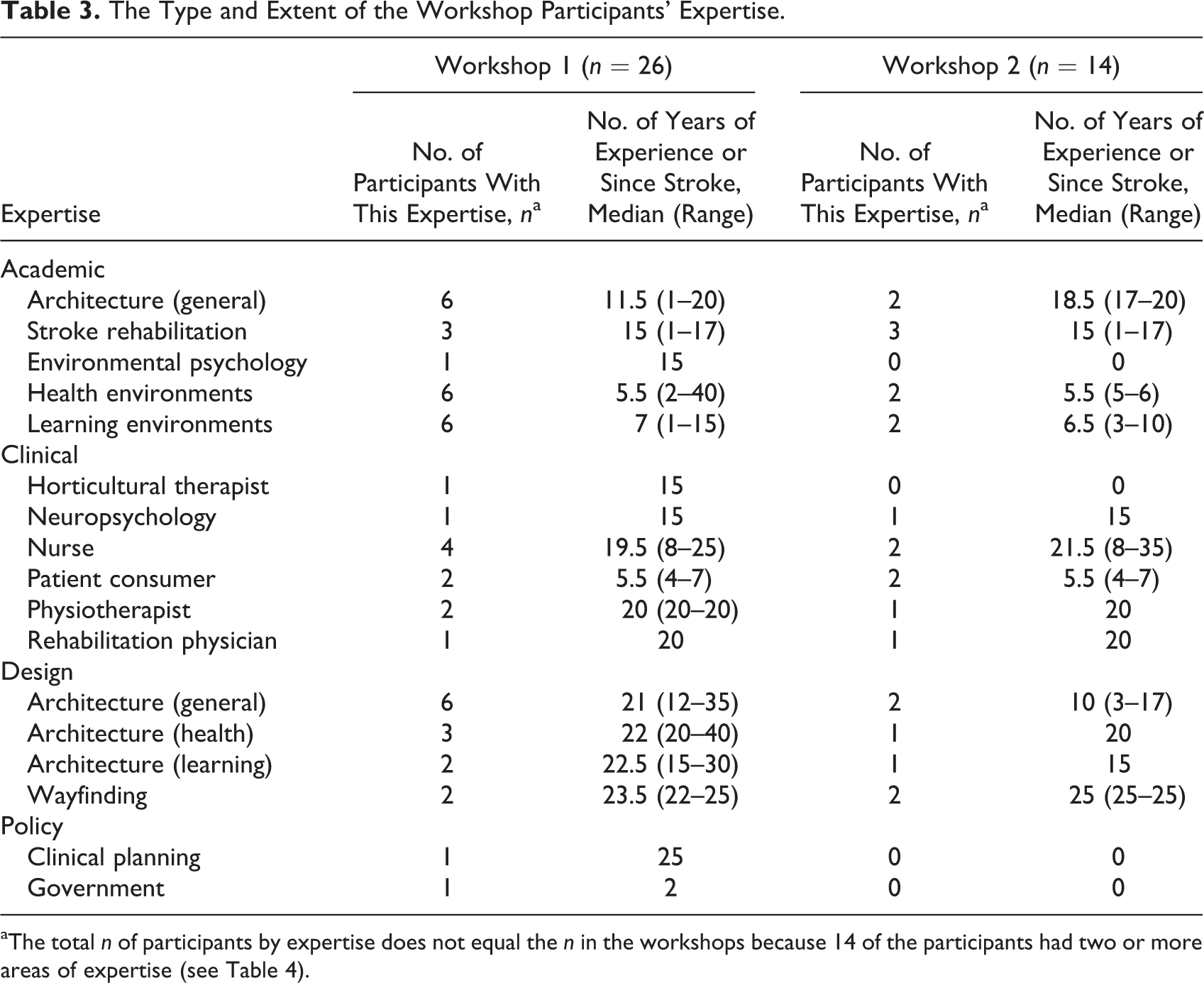
aThe total n of participants by expertise does not equal the n in the workshops because 14 of the participants had two or more areas of expertise (see Table 4).
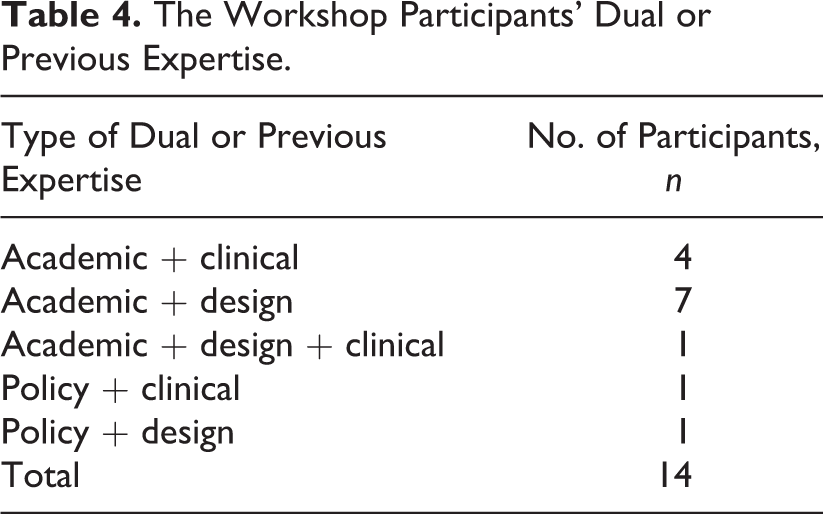
Three of the participants are authors of this manuscript (Bernhardt, Newton, and Zeeman), and the remaining participants are thanked in the Acknowledgments section with their permission. Of the 30 experts, 16 attended Workshop 1 only, 4 attended Workshop 2 only, and 10 attended both. Although some of the participants had previously worked internationally, they all lived and worked in Australia at the time of participation. Most were residents of the state of Victoria, one from Western Australia, one from South Australia, and one from Queensland. Fourteen of the experts had dual expertise or previous careers relevant to the project (see Table 4).
The Workshop Participants’ Dual or Previous Expertise.
A Framework of What Is Important in the Design of Inpatient Stroke Rehabilitation Facility Buildings
Figure 2 shows the hierarchy of fundamental objectives that participants identified as important in the design of inpatient stroke rehabilitation buildings and interiors. The four top-level fundamental objectives state that an optimal design for these buildings should maximize efficiency, maximize effectiveness, foster emotional well-being, and maximize safety. The fundamental objectives are defined below with illustrative quotes from participants.
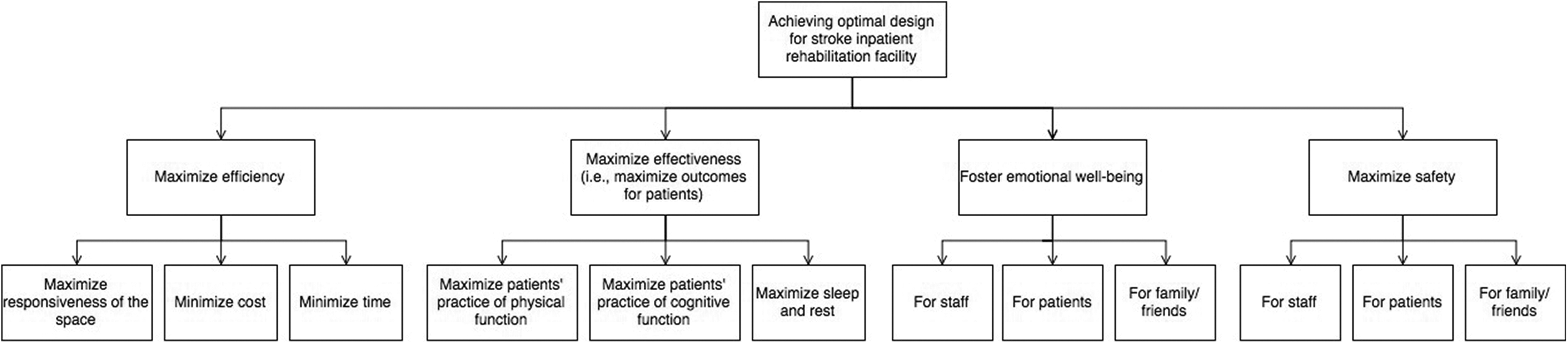
The hierarchy of fundamental objectives from the framework of what is important in the design of inpatient stroke rehabilitation facility buildings. This figure shows the connections between the 4 first-tier fundamental objectives and the 12 second-tier fundamental objectives that were identified in the workshops.
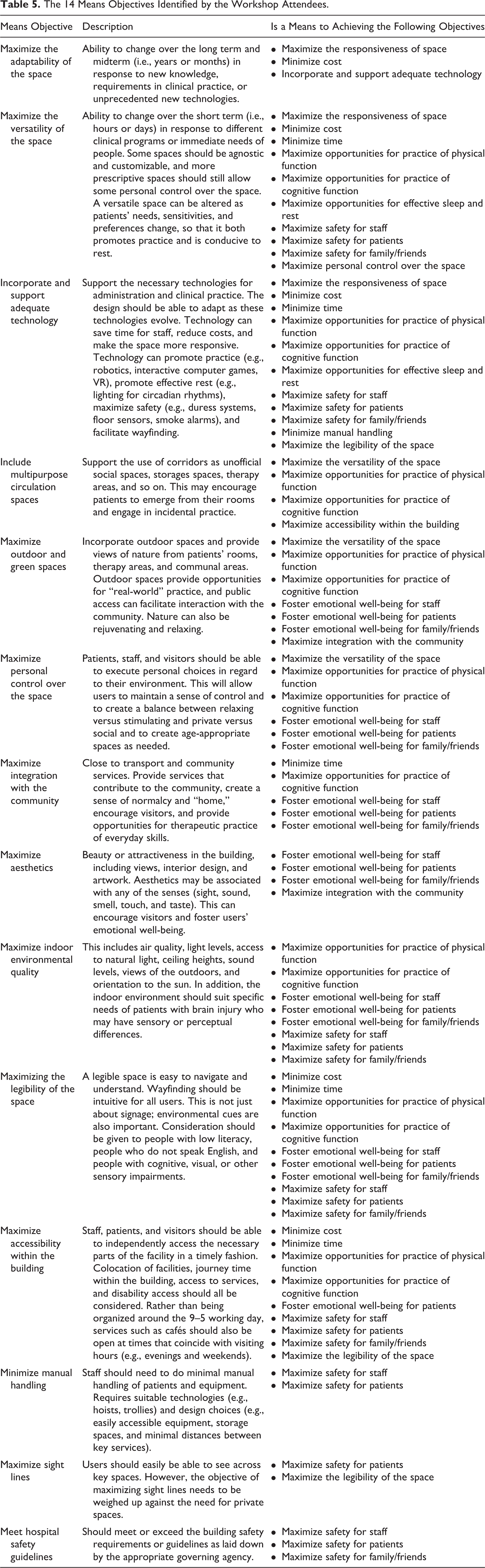
Fourteen means objectives were identified. Some criteria that were originally suggested as fundamental objectives were later reconsidered as means objectives instead. For example, maximize the legibility of the space was originally considered a fundamental objective but was then relabeled as a means objective because the legibility of the space was considered important due to its role in achieving the fundamental objectives in the hierarchy, not because it was fundamentally important in and of itself. The means objectives are listed in Table 5 and described in detail in the Supplementary Material. Some examples of the means objectives are included in-text below to demonstrate how they relate to the fundamental objectives in the hierarchy.
The 14 Means Objectives Identified by the Workshop Attendees.
Maximize efficiency
The workshop participants decided that it is important that inpatient stroke rehabilitation facilities maximize efficiency of care delivery (see Figure 2). A rehabilitation physician noted that “Efficiency drives everything for us… the value is around managing the resources that you have in order to get extra things….” The concept of efficiency incorporates objectives relating to cost, time, and the responsiveness of the space.
The objective to minimize cost refers to costs incurred over the lifetime of the building. This objective emphasizes sustainability and recognizes direct and indirect costs related to design. Direct costs may be up front (e.g., land purchase) or ongoing (e.g., building repairs). Examples of indirect costs may include salary cost of staff giving directions to lost patients or visitors, or recruitment costs due to staff turnover. The optimal design of a rehabilitation facility should also minimize time for all aspects of care delivery including administrative tasks. The location of services within the building, and the location of the building itself, may impact the efficiency of communication between services, travel time to and within the building and therefore the time taken to execute all tasks.
The participants decided that an efficient rehabilitation facility should also maximize the responsiveness of the space. A responsive space was defined as a space that can change in response to users’ changing needs. Different cohorts of staff, patients, and visitors will have different needs, and these needs may change over time. A rehabilitation nurse noted, “We get some patients that are so cognitively impaired…and then we have other types of patients that have just got speech issues…but their cognitive and mobility function is high. So it [the design] would have to be adaptable….” The participants agreed it would be most efficient for the building to respond to changes as they occur, hence the means objectives to maximize the adaptability of the space and maximize the versatility of the space (see Table 5 and Supplementary Material).
Maximize effectiveness
The participants agreed that an inpatient stroke rehabilitation facility should maximize the clinical effectiveness of rehabilitation (see Figure 2). The participants felt that an optimal rehabilitation facility should therefore maximize patients’ incidental and deliberate practice of any activity that promotes recovery, so that they can reach their optimal physical, psychological, and social function. In other words, the built environment should facilitate guided practice while in therapy but also encourage patients to voluntarily or incidentally participate in recovery-promoting activities (physical, social, cognitive) outside of the limited formal therapy time.
In addition, the built environment should be designed to maximize patients’ effective sleep and rest. Sleep disorders are common poststroke, and disturbed sleep may negatively impact short- and long-term recovery (Duss et al., 2017). Many aspects of the built environment, including noise, light, temperature, and the presence of other people, may negatively affect sleep, and so should be considered in the design of rehabilitation facilities.
The means objective to maximize personal control over the space (i.e., allow patients, staff, and visitors to execute personal choices about their environment) may be instrumental to maximizing clinical effectiveness (see Table 5 and Supplementary Material). Having personal control would allow patients, staff, and visitors to adjust the space to respond to changing and varied needs in therapy. In addition, a sense of agency may help patients to feel motivated, and, according to the Theory of Supportive Design, may reduce stress (Ulrich, 1991).
Foster emotional well-being
The workshop participants specified that the design of inpatient stroke rehabilitation facilities should foster the emotional well-being of all users. The term “emotional well-being” in this context encompasses feelings of self-confidence, self-worth, self-determination, belonging, optimism, happiness, and dignity. Critically, by fostering emotional well-being, detrimental cognitive or emotional states such as boredom, anxiety, and stress may be minimized (Luker, Lynch, Bernhardsson, Bennett, & Bernhardt, 2015). A stroke survivor highlighted the importance of patients’ emotional well-being, and its connection to effectiveness and efficiency, by stating that, “There were days when I was too down in the dumps to even do as much physio [physiotherapy] as I could be doing, so your physio [physiotherapist] is spending a bit more time sitting there talking with you, rather than getting up and doing the physical things, so I think that emotional well-being is really important….”
The participants emphasized that the emotional well-being of any one group of users (patients, visitors, and staff) can influence the emotional well-being of the others. Critically, “the staff have to feel good in order to do a good job” (stroke rehabilitation researcher and physiotherapist). The participants reported that the means of achieving emotional well-being may differ between cohorts (e.g., patients may respond to different things compared to staff), so the needs of all three groups must be considered when design choices are made.
The means objective to maximize the legibility of the space (i.e., have good wayfinding and ensure the space is easy for all users to navigate) may help to reduce stress and improve emotional well-being. Getting lost or disorientated and having to walk further can sap energy and impact pain levels. Maximize integration with the community was also included as a means objective that may help to promote emotional well-being (see Table 5 and Supplementary Material).
Maximize safety
All workshop participants agreed that the safety of patients, visitors, and staff was fundamentally important in the design of a rehabilitation facility. The design should ensure the basic safety of all occupants (e.g., fire safety and evacuation, heating/cooling). A stroke survivor remarked that “Safety is one of those things where there’s got to be a minimum level, [because] things just don’t work below that level.”
The participants emphasized that some threats to safety may be of more concern in a stroke rehabilitation facility than in other healthcare settings, and the means of achieving safety may therefore be different too. The workshop participants agreed that patient falls may be the biggest threat to patient safety in a stroke rehabilitation facility. Stroke patients can experience physical and cognitive changes that may increase their risk of falling, including impaired balance, hemiplegia, muscle weakness, and/or hemi-inattention or extinction in one or more of their senses. Hemiplegia, for example, may prevent a patient from self-protecting upon falling.
However, the workshop participants emphasized that the balance between safety and activity restriction is very delicate. Restricting patient activity and practice in order to prevent falls could be counterproductive and detrimental to patients’ recovery and safety in the long run. A rehabilitation nurse noted that, “in rehab they take risks. They’re [patients are] not going to learn without it….” An architect and researcher in learning environments similarly noted that, “safety, while it’s important, it’s kind of like with children in school settings as well, a little bit of risk is okay as long as people understand it….”
Participants agreed that safety measures that confine patients to their rooms, or somehow limit patients’ control over their movement through the facility, would be detrimental to patients’ clinical outcomes and emotional well-being, and so would not meet the fundamental objectives to maximize effectiveness and foster emotional well-being. Facility design should provide opportunities for learning and recovery in addition to the necessary health and safety requirements. The means objectives associated with achieving patient safety were therefore carefully chosen to ensure patient safety without discouraging patient activity and practice (see Table 5 and Supplementary Material).
Discussion
This study is novel in its methodology and its outcomes. We have made the following original contributions to the literature: (1) We have developed a framework of what experts think is important in the design of inpatient stroke rehabilitation facilities, (2) we have begun to reconceptualize rehabilitation facilities as learning environments, and (3) we have applied Value-Focused Thinking to facilitate systematic, interdisciplinary design research.
A Framework for Inpatient Stroke Rehabilitation Facility Design
According to our framework, it is fundamentally important that the design of inpatient stroke rehabilitation facilities maximizes the efficient running of the facility, patients’ clinical outcomes, the emotional well-being of all users, and the safety of all users. The 14 identified means objectives suggest how these fundamentally important things could be achieved. Many of the objectives identified in this study are backed by previous healthcare design research and theory in nonrehabilitation health settings (for a scoping review protocol of theories used in healthcare design research, see Shannon, Nordin, Anåker, Bernhardt, & Elf, 2017). For example, the Theory of Supportive Design emphasizes the importance of personal control, social support, and positive distraction (Ulrich, 1991), and these concepts are represented in our framework by the means objectives to maximize personal control, maximize integration with the community, and maximize aesthetics, respectively.
Our framework has been designed to be specific to inpatient stroke rehabilitation, and it therefore includes concepts that do not appear in existing healthcare design frameworks (Zhang, Tzortzopoulos, & Kagioglou, 2018). The unique position of rehabilitation facilities as learning environments was emphasized in our framework by the importance assigned to opportunities for incidental and deliberate practice of physical, cognitive, and social activity. This importance was emphasized by health environments experts and learning environments experts. Self-directed learning is a central tenant of adult learning theory (Merriam, 2001), and rehabilitation guidelines emphasize the importance of the patient’s input in repetitive, goal-directed practice poststroke (Winstein et al., 2016). The concept of flexible spaces, and the distinction between adaptability and versatility, is also emphasized in learning environments research (see, e.g., Cort, Cort, & Williams, 2017), and this contribution to the framework was made by a participant with expertise in learning environments research.
A review by Luker, Lynch, Bernhardsson, Bennett, and Bernhardt (2015) found that although stroke patients recognize that physical activity is important for their recovery, they feel that their physical activity (both in structured therapy and in free time) is negatively impacted by their boredom, lack of motivation, and their perceived lack of autonomy. Many of the means objectives in our framework could facilitate stroke patient autonomy and promote their physical and cognitive practice, for example, maximize personal control over the space and maximize accessibility within the building. Our framework therefore suggests that rehabilitation environments should be designed to draw patients out of their bedrooms and to support patient autonomy and activity, while ensuring that they remain safe. Safety is fundamentally important, but it should not preclude opportunities for practice, as this is essential for patients’ recovery.
Our framework suggests that design choices that are usually standard in acute healthcare settings may need to be rethought for rehabilitation. Patient room occupancy is an example of this. Evidence from acute healthcare populations suggests that single-occupancy rooms are beneficial for infection control, patient–clinician communication, noise reduction, and that they are preferred by patients (Ellen, Alan, & Melissa, 2018). Stroke patients are not usually at high risk of infection, are often well enough to access spaces beyond their room, and many stroke patients value camaraderie with their peers (Bennett, Luker, English, & Hillier, 2016; Lewinter & Mikkelsen, 1995). According to our framework, a patient’s room in an inpatient stroke rehabilitation facility should encourage physical, cognitive, and social activity; be conducive to sleep and rest; promote well-being; be responsive to the user; reduce travel time; reduce costs; and maximize safety (primarily falls risk). There is no clear evidence to support whether single-occupancy or multiple-occupancy rooms are the optimal way to meet these fundamental objectives in rehabilitation facilities (Shannon et al., 2018). Architects and designers may choose to design rehabilitation patient rooms to meet the objectives in our framework—whether they be single occupancy or multiple occupancy—instead of routinely applying the patient room model that is accepted in acute care.
Benefits of an Interdisciplinary, Value-Focused Thinking Methodology
Healthcare environments are complex. The interdependence of clinical processes, the built environment, and human behavior presents a challenge for traditional approaches of isolating variables and identifying causation (Stichler & Hamilton, 2008). Hamilton (2013) has argued that the field of evidence-based design has been done a disservice by attempts to confine it to reductionist philosophies of science. Rather than attempting to simplify the topic, we embraced the complex, subjective nature of rehabilitation facility design. We recruited an interdisciplinary team of experts ranging from academics, to stroke survivors, to clinicians, to architects. Many of the experts had relevant dual expertise, which reinforced the interdisciplinarity of the cohort.
Interdisciplinary research carries challenges in terms of language and communication (Bracken & Oughton, 2006). We therefore incorporated measures to ensure that everyone was understood, such as the glossary of jargon (and permission to call it out) and the Workshop 1 prereading. Compared to alternative-focused thinking, Value-Focused Thinking encourages the decision maker to think beyond specific design features (Keeney, 1992). This encouraged unconstrained, nontechnical thinking that was accessible to all participants. Value-Focused Thinking presented the experts with a cohesive, inclusive approach that minimized the impact of discipline biases and ensured that all opinions were heard.
Rather than focusing on one variable (e.g., social support or integration with the community), the framework acknowledges that many interconnected variables are important for inpatient stroke rehabilitation facility design. Each of these objectives is important in its own right despite conflicts or interdependencies between objectives. Healthcare architects, designers, and stakeholders should consider combinations or “bundles” of design solutions to collectively meet desired outcomes in the built environment (Hamilton, 2010). Value-Focused Thinking can aid this process by articulating priorities and organizing them into a framework, so that they can be considered systematically.
Limitations
The choice to have many disciplines represented at the workshops meant that there were between two and six experts from each discipline in the final sample (see Table 2). A key strength of this study lies in its interdisciplinarity. Future studies could consider repeating each workshop and increasing the total number of participants in order to include more experts and more disciplines, such as occupational therapists, speech pathologists, health administrators and managers, educators, and the full complement of rehabilitation staff. There was generally a high level of agreement between participants in this study, so whether adding more disciplines would raise additional themes to those found to date is unknown.
Some participants in this study had collaborated previously. This familiarity may have helped to stimulate discussion, but a downside is that this sample may not represent the views of an international, varied cohort. Future studies could consider alternative methods of recruitment (e.g., advertising on social media or academic networking websites) to widen the pool of experts and bring an international perspective. Such recruitment methods would require a selection process to ensure expertise.
Future Directions
This study presents only the first step in an ongoing process to reframe stroke rehabilitation spaces and inform their design. Expert elicitation could be further utilized to rank the fundamental objectives identified in this study in order of their relative importance to indicate how potentially conflicting objectives should be prioritized in design (Belton & Stewart, 2002).
The current framework could inform postoccupancy evaluation protocols or detailed case study research on-site at existing rehabilitation facilities. Future research could refine the framework by considering specific spaces (e.g., bedroom, gym, corridors) as well as the overall facility design. Critically, the priorities identified in this study are relevant for the built environment of rehabilitation facilities and do not necessarily reflect clinical priorities for rehabilitation. Future research should acknowledge the clinical priorities and culture of the facilities. Future research could provide and test design exemplars of how objectives could be met.
Conclusions
The Value-Focused Thinking methodology used in this study could be applied to any complex built environment, including other healthcare environments and other rehabilitation environments, such as community rehabilitation or the patient’s own home. The objectives in the framework reflect the unique needs of stroke rehabilitation as both a healthcare space and a learning space. The challenge for providers compiling design briefs is to emphasize the importance of these objectives in stroke rehabilitation environments, and the challenge for architects and designers is to find design solutions that collectively meet these objectives.
Implications for Practice
Inpatient stroke rehabilitation facilities are unique healthcare environments, and design choices that are standard in acute healthcare settings may need to be reframed for rehabilitation settings. Designers of stroke rehabilitation facilities should consider how designs can provide opportunities for physical, cognitive, and social activity. Rehabilitation environments should allow for carefully monitored risk-taking to promote patient autonomy and activity while maintaining patient safety. Rehabilitation facility design may benefit from interdisciplinary input from learning environments research and healthcare environments research. Value-Focused Thinking is an effective methodology to facilitate interdisciplinary research, bring together varied perspectives, and consider complex problems in a design context.
Supplemental Material
Supplementary_Material - A Framework for Designing Inpatient Stroke Rehabilitation Facilities: A New Approach Using Interdisciplinary Value-Focused Thinking
Supplementary_Material for A Framework for Designing Inpatient Stroke Rehabilitation Facilities: A New Approach Using Interdisciplinary Value-Focused Thinking by Ruby Lipson-Smith, Leonid Churilov, Clare Newton, Heidi Zeeman and Julie Bernhardt in HERD: Health Environments Research & Design Journal
Footnotes
Authors’ Note
Some data from this project have been presented as a poster and published in abstract format at the European Healthcare Design Conference (June 11–13, 2018), London, England.
Acknowledgments
The authors thank the workshop attendees: Lesley Alway, Katie Bagot, Isabella Bower, Finn Butler, Ben Cleveland, Jane Conidaris, Maria Crotty, Jo Dane, Kevin English, Dominik Holzer, Wesley Imms, Jessica Keating, Warren Kerr, Tom Kvan, Kirra Liu, Robert Luxford, Rebecca McLaughlan, Heather Mitcheltree, Natalie Pitt, Robert Polglase, Alyce Raine, Kerryn Rim, Stefano Scalzo, Michelle Shannon, Sarah Smith, Michel Verheem, and Steven Wells. Special thanks to Jessica Keating and Kirra Liu for aiding with workshop facilitation and to Kenn Fisher, Wes Imms, Tom Kvan, and Heather Mitcheltree for their input into the initial study concept. The Florey Institute of Neuroscience and Mental Health acknowledges the support from the Victorian Government and in particular the funding from the Operational Infrastructure Support Grant. Ruby Lipson-Smith is supported by a Research Training Program PhD scholarship from the Australian federal government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a seed grant from the Hallmark Ageing Research Initiative (HARI) at the University of Melbourne.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.