
Abstract
Objective:
The objective of this study is to investigate a development project initiated and led by midwives.
Background:
The aim was to design an environment that could accommodate the wish to support professionalism while creating better and more cohesive patient treatment, improved patient safety, greater efficiency, higher quality, and stronger focus on the patient.
Theory:
The theoretical and analytical account is conducted within the framework of design thinking (DT), replacing the traditional evidence-based design approach with an evidence-based design thinking (EBDT) process underpinning participatory DT and co-creation.
Method:
Based on a longitudinal case study on a participatory design process, interviews are conducted. DT principles are used in the analysis of the interviews.
Results:
Genuineness arises when all users experience that the physical setting optimally underpins the birthing situation. It is essential to make visible the importance of the physical setting to human behavior in any situation.
Conclusion:
This study shows that midwives intuitively do EBDT. EBDT commands awareness of both research, design, midwifery care, and perspectives on space from women giving birth and their relatives. Collectively, that can provide the genuine scope of a healing birth environment.
Keywords
The aim of this article was to inform our understanding of design thinking (DT) based on a case study of the development of a modern birth environment. During this process, we moved from a traditional evidence-based design (EBD) approach to one that may be characterized as evidence-based design thinking (EBDT) emphasizing participatory DT. This design process is characterized by a transformation of roles and processes through the creation of new spaces and environments for birthing, focused on human healing processes. In earlier projects, we found that the EBD process encompasses multiple processes involving research, design, and treatment innovation, all of which are closely intertwined and affected by users, that is, staff, patients, and relatives (Folmer & Jangaard, 2016). It is suggested that these intertwined processes affected by users are conceived as keystones in a social sustainability approach to birth environment design (Folmer & Jangaard, 2016). The present research is conducted within a context where new large emergency care hospitals are constructed in the five Danish hospital-administrative regions.
In our case study, staff members were involved in the planning of the maternity ward of a new emergency care hospital (Figure 1[1]). The midwives together with other staff members and architects did an experimental, full-scale mock-up for a new delivery room equipped with furniture and physical equipment from the existing maternity ward to determine and optimize the size and internal design of the rooms (Figure 1[2]). The midwife head of department and her assistant midwife responsible for quality improvement were the leaders, drivers, and decision makers of the design process.
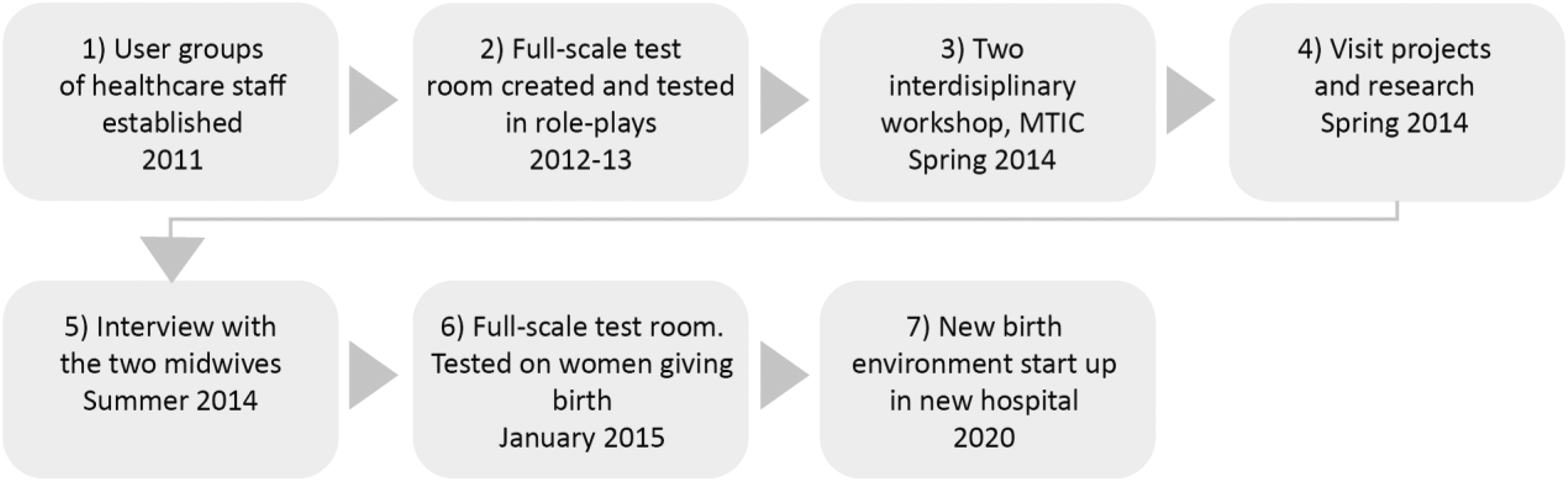
Flow diagram of different activities of the design process.
In this case, the head of department and her assistant set the team of staff members; they took all the initiatives for collaboration with external partners and made all final decisions concerning the development and furnishing of the experimental birth room. These two midwives serve as interviewees (informants) for this study.
In workshops, the professionals’ experiences from traditional Western birth rooms were challenged by the architects’ ideas about modern healthcare design; clinical emergency situations were tested in role-playing, featuring different scenarios of labor, delivery, and infant resuscitation, to test different applications and arrangements of furniture and equipment during critical situations (Figure 1[2]).
The enthusiasm of the midwives participating in the birth environment design process was rooted in several previous studies and theories suggesting that supporting birth environment tends to influence laboring women to give birth spontaneously and with less medication and surgical interventions. Studies of the influence of birthing environments on birth suggest that a physiologically supportive birth environment should feature calming physical space; it should also provide continuity of care in the context of a safe personal relationship with the midwife and the woman’s partner (Foureur et al., 2010; Hammond, Foureur, & Homer, 2014; Kjaergaard, Olsen, Ottesen, & Dykes, 2009; MacDonald, Johnson, & Warwick, 2017; Overgaard, Fenger-Grøn, & Sandall, 2012; Shah, Galvin, Plough, Henrich, & Ariadne Labs, 2017; Symon, Dugard, Butchart, Carr, & Paul, 2011; Uvnäs-Moberg, 1998).
During the spring of 2014, the midwives of the teaching hospital initiated activities, paid visits, and developed professional relationships outside the hospital to get inspired by the so-called creative disturbances of their usual views to further investigate and develop principles for the design of the future birth environment (Figure 1[4]). They attended a student’s workshop on birth unit design and obtained models and reports from students’ work on application of zones for activity, relaxation, and privacy in the birth space. To get further inspiration, two workshops were conducted by the midwives (Figure 1[3]). The participants represented different professions and skills—a zookeeper, a design psychologist, an ethnographer, a game developer, a healthcare app developer, an architect and manufacturer of furniture and equipment, health professionals, and first and second author of this article. Four main principles for the future design process were established during these workshops. The birth room should offer opportunities for calmness, protection, and privacy for the laboring woman and her partner; visual update on the progression of birth; involvement of the father; and physical activity for the laboring woman (Jangaard, 2015). These principles became the guideline for the construction and design of the experimental setup of a new birthing room in the existing maternity ward. The midwives were assisted by an interior designer for the planning of the experimental birth room. In January 2015, the full-scale test room was opened to laboring women for a testing program (Figure 1[6]). The new birth environment is expected to be operational from 2020 (Figure 1[7]).
The case represents a window of opportunity for the staff, mainly midwives of the maternity ward in a teaching hospital, to participate in the design process to accommodate the political wish for better and more cohesive patient treatment, improved patient safety, greater efficiency, higher quality, and stronger focus on the patient. This context has inspired the following two research questions: How can midwives become active participants in developing and designing a birth environment? And How can EBD and DT inform our understanding and analysis of how midwives may be involved in a creative design process?
In the following sections, we explain how we worked with these research questions, followed by a theoretical section on DT that establishes the analytical framework used in the case discussion. The article ends with a conclusion and reflections on future perspectives.
Method
The present research is part of an ongoing project; this article reports on experiences from the early stages, viz., the design processes and construction of new hospitals in Denmark based on a longitudinal case study of a participatory design process. The case is described and investigated through observation, participation, and interviews. This article includes interviews that were conducted with two midwives leading the design process of birth environment. Three interviews were conducted by the first and second authors of this article.
The interviews were conducted using an ethnographic approach based on previously collected records and case material in the project (Hammersley & Atkinson, 2007; Spradley, 1979; Yin, 1994). The interviews were recorded and transcribed verbatim. Both interviewees read and approved the transcriptions. The study and research meet the legal criteria for use of personal information (Regulation [EU] 2016/679 of the European Parliament and of the Council, 2016).
The interviews all started with an introduction with information about purpose and structure. Ex “midwives’ experience with the design process,” followed by a three-part structure: (a) general experience, (b) time course and incidents in the design process, and (c) advice to other midwives. Both authors read the transcriptions and revealed key themes based on the research questions.
Our theoretical approach to the research questions departed from traditional EBD approach and Bryan Lawson’s DT model of design problems. This analysis framework proved insufficient, as Lawson primarily focuses on the architect’s role as creative force. We lacked tools to describe the role of midwives in the creative design process, and subsequently we changed the theoretical framework to Brown’s DT. DT principles are structuring/framing the analysis of the case and the interviews with midwives. The themes examined if the midwives were intuitively using the DT principles as an innovation driver. For this purpose, an analytical framework is used, connecting the DT theory with our real-life case. In the analysis, the relevant DT principle is discussed in light of the midwives’ opinions.
Design Theory—EBD Informed by DT
Our research group implemented a literature review (Jangaard, Folmer, & Buhl, 2018) to examine how literature has investigated midwives doing DT and birth environment design; we examined the healthcare literature on birth environment and design to identify literature addressing the issue of how midwives participate in developing and designing birth space (Jangaard et al., 2018). This resulted in no usable instruction or methodology to inform future midwife designers on what to do or how to design birth environment. This section will create a connection between the concept of design and the relation between EBD and EBDT.
In 1980, Lawson (2005) noted that design is both a noun and a verb and can refer either to the end product or to the process. According to Lawson, Design is a highly complex and sophisticated skill. It is not a mystical ability given only to those with recondite powers but a skill which, for many, must be learnt and practiced rather like the playing of a sport or a musical instrument. (p. 14) Design is a remarkably subtle discipline, amenable to radically different interpretations in philosophy as well as in practice. However, the flexibility of design often leads to popular misunderstanding and clouds efforts to understand its nature. The history of design is not merely a history of objects. It is a history of the changing views on subject matter held by designers and the concrete objects conceived, planned, and produced as expressions of those views. One could go further and say that design history is a record of the design historians’ views regarding what they conceive to be the subject matter of design. (p. 19)
EBD is focused on explaining the nature of research and how research can be integrated into design processes for construction of healthcare facilities like hospitals. This is seen, among others, in the book A Practitioner’s Guide to Evidence-Based Design (Harris et al., 2008). The book seeks mainly to explain EBD research. This is highly relevant as most architects are unfamiliar with the premise of doing research and therefore need to know more. The same holds true for healthcare professionals who basically know little about design processes. This part is not particularly well explained in EDAC (Evidence-Based Design Accreditation and Certification) study guides.
EBD has been developed over the past 20 years (Carr, Sangiorgi, Büscher, Junginger, & Cooper, 2011). It was coined unofficially in the legendary research project by Roger Ulrich in 1983 “View through a window may influence recovery from surgery” (Ulrich, 1984). Ulrich finds a possible connection between the environment and the effect of treatment and highlights the fact that the environment does influence human behavior and healing. In 2004, Hamilton (2004) gave his first version of EBD: An evidence-based designer makes decisions—with an informed client—based on the best available information from credible research and evaluation of projects. Critical thinking is required to draw rational inferences about design from information that seldom fits a unique situation precisely. (p. 1)
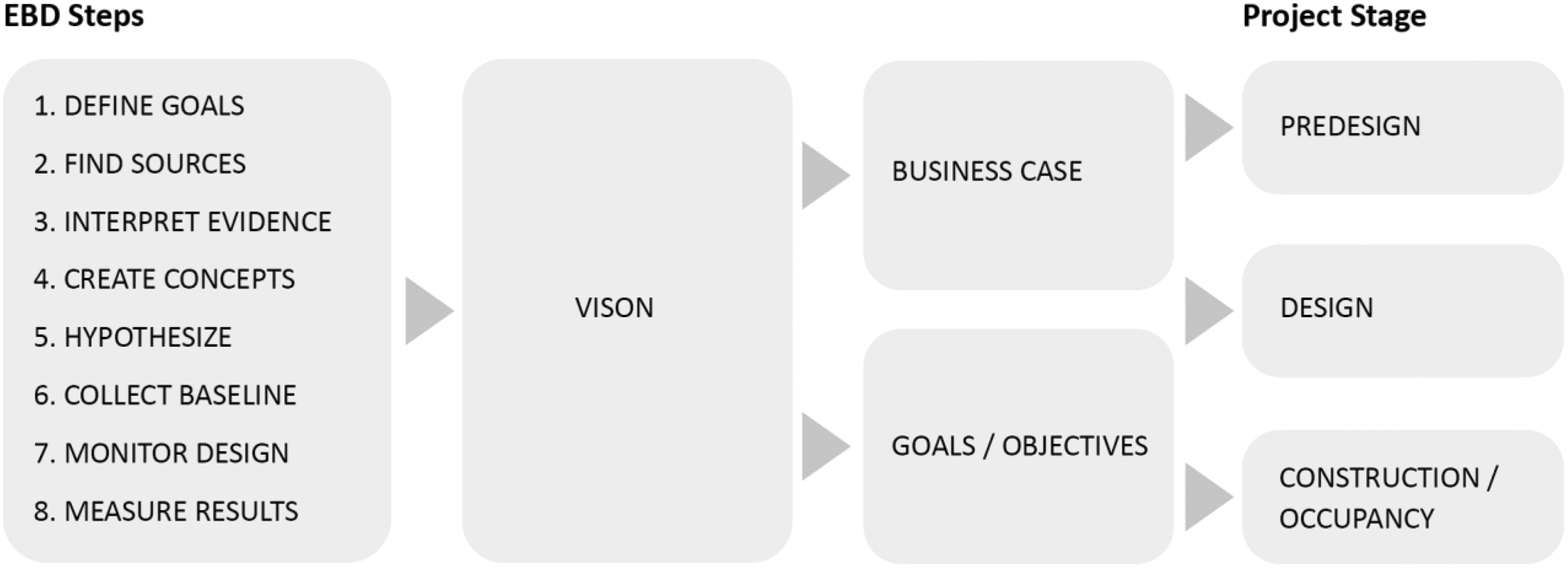
The eight steps in evidence-based design, which are illustrated in EDAC Study Guides 1, 2, and 3 (Goetz et al., 2008a, 2008b, 2008c).
Reviewing previous projects, we found that EBD processes comprised research, design, and innovation of treatment processes (Folmer, 2014; Jangaard & Folmer, 2016). Also, even if EDAC teaching materials (Goetz et al., 2008a, 2008b, 2008c) and Harris et al. (2008) give examples of how nursing and treatment offers may be developed and qualified through EBD processes, no suggestions are offered as to how healthcare professionals, patients, and relatives may be parties to these processes.
An interdisciplinary project team approach to project delivery is another characteristic of an EBD process. Interdisciplinarity emerges from the collaboration between owners, users, consultants, and researchers. This interdisciplinary group, including management, compiles vision, goals, and business cases, that is, they agree on a common goal that binds design and research processes together. The members of the group are active in the programming of functions and space. Yet, in order for such cooperation to be possible, the EBD process requires all partners to understand what they individually represent, that is, healthcare, research, design, and construction (Goetz et al., 2008a). The basics of EBD are seen as a strategic tool in which strategic investments can deliver important benefits (Goetz et al., 2008a). Therefore, the brief made by the interdisciplinary project team is key to the EBD process. Innovation of the physical environment interacts with a range of different factors in achieving the desired outcome and influences the design process. In this setting, the chief executive officer (CEO) plays a crucial role in achieving success (Zimring, Augenbroe, Malone, & Sadler, 2008).
In summary, in an EBD process, it is important that all members of the interdisciplinary project team participate in the work related to the annotation of diagrams, documentation of assumptions, updating of hypotheses, testing of design concepts, selection of the best options, and construction of full-scale test room environments.
The following section presents Brown’s approach to DT and relates his approach to EBD, discussing in particular areas of correspondence between DT and EBD and how instrumental these approaches may be in the hands of healthcare professionals, like midwives, who participate actively in the design of interventions.
Brown’s DT
Tim Brown is a CEO and president of the IDEO and an industrial designer by training. In 2009, he wrote Change by Design and mapped out the principle for DT (Brown, 2009). He states: Design thinking taps into capacities we all have but that are overlooked by more conventional problem-solving practices. It is not only human-centered; it is deeply human in and of itself. DT relies on our ability to be intuitive, to recognize patterns, to construct ideas that have emotional meaning as well as functionality, to express ourselves in media other than words or symbols. Nobody wants to run a business based on feeling, intuition, and inspiration, but an overreliance on the rational and the analytical can be just as dangerous. The integrated approach at the core of the design process suggests a “third way. (p. 4)
DT is a human-centered understanding building on empathy. This is in line with the EBD design process. Still, empathy is not a concept that is mentioned in the EDAC learning books, but we can hardly place humans in the center of a design process without also involving aspects of empathy.
Another central point in DT is to make meaning out of the context—or said with Brown’s (2009) words: “Design thinking relies on our ability to be intuitive, to recognize patterns, to construct ideas that have emotional meaning as well as functionality, to express ourselves in media other than words or symbols” (p. 4). In line with this, Lundin (2015), a Swedish architect and PhD, recently suggested that intuition is an important creative tool. He also suggested that empathy is just as important a tool as evidence in the quest for making healing architecture.
Brown’s DT emphasizes the ability to embrace other professions and hereby be a tool to support collaboration with other professions. DT is interdisciplinary. Brown (2009) says: We ask people not simply to offer expert advice on material, behaviors, or software to be active in each of the spaces of innovation: inspiration, ideation and implementation. Staffing a project with people from diverse backgrounds and a multiplicity of disciplines takes some patience, however. It requires us to identify individuals who are confident enough of their expertise that they are willing to go beyond it. (p. 27) Design thinking is commonly visualized as an iterative series of five major stages. To the left, we see the standard form. To the right, we see something closer to reality. While the stages are simple enough, the adaptive expertise required to choose the right inflection points and appropriate next stage is a high-order intellectual activity that requires practice and is learnable. (Plattner, Meinel, & Leifer, 2011, p. xiv)
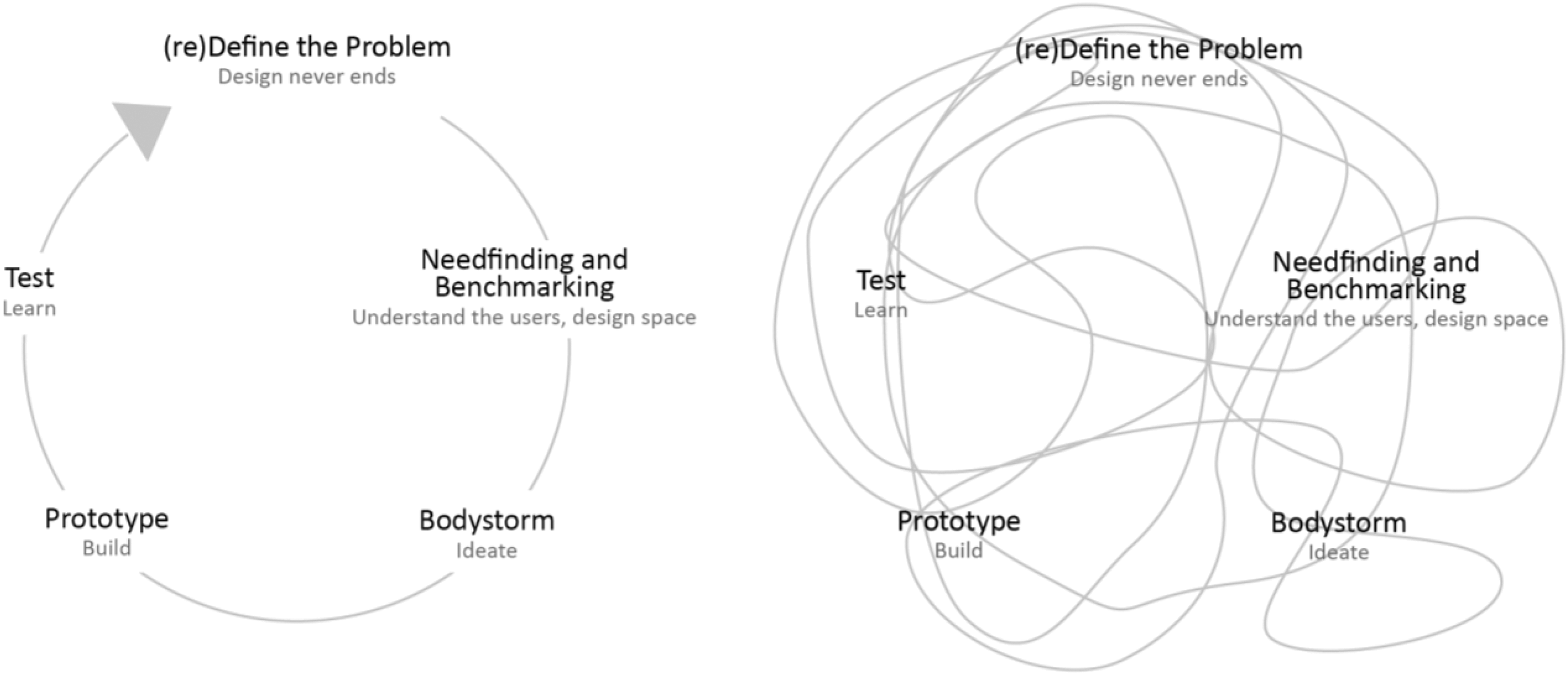
Design thinking—five major stages. The relation between standard form and reality.
Brown describes DT as a set of principles that can be applied by different people to a wide range of problems. Illustrating DT in a mind map (Figure 4), the HOW part focuses on the principles of DT and the WHAT part concretizes the principles of DT using projects made by Tim Brown and his firm IDEO (Brown, 2009).
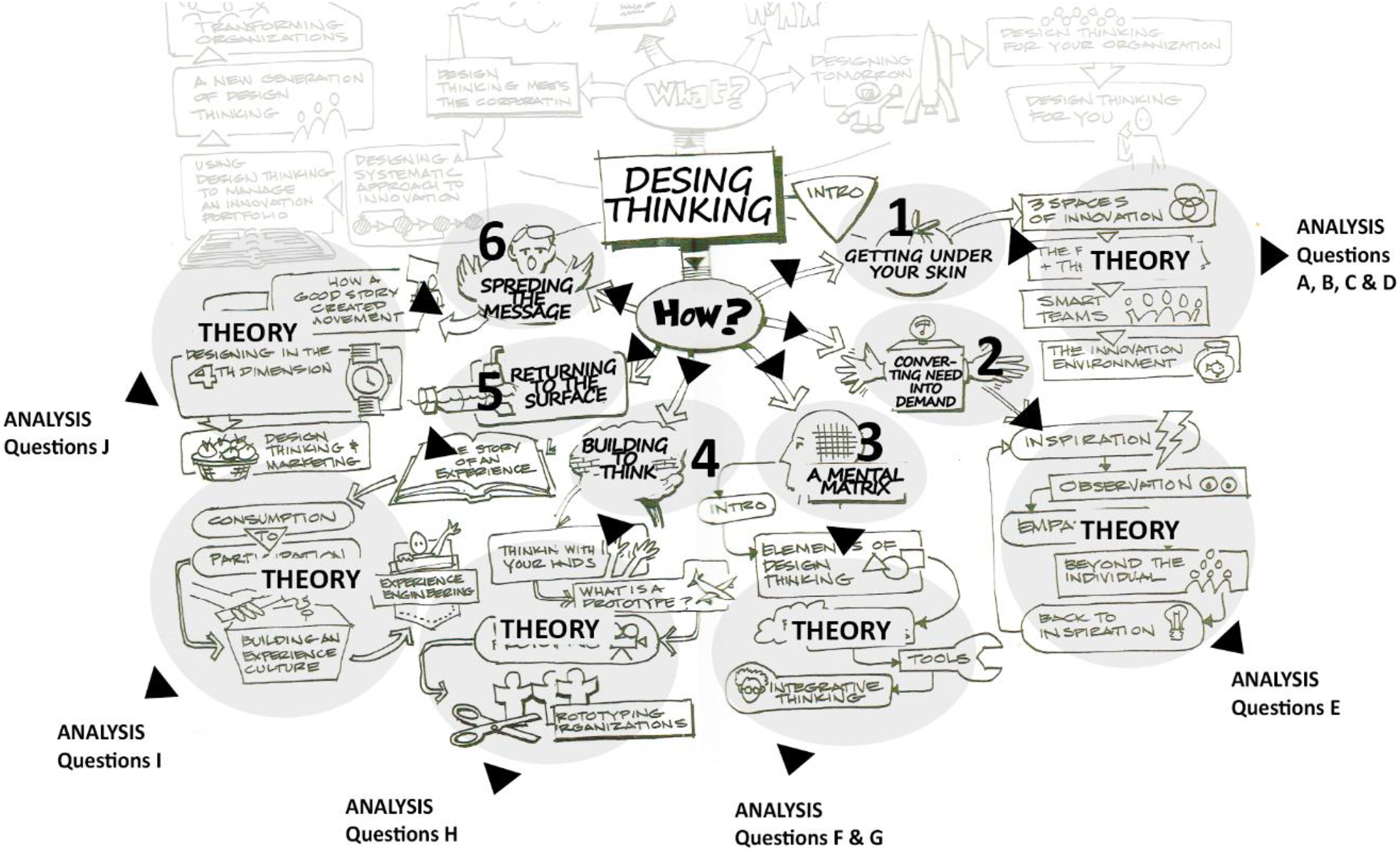
Brown’s design thinking mind map with analysis questions.
Analysis and Results—DT Implications
Brown’s DT principles are used to analyze and report how midwifes can innovate care to women giving birth, creating a new birth environment. The HOW part is used as a framework (Figure 4) for analyzing the interviews with the midwives. Each DT principle was used for generating questions for analyzing the interview (Table 1).
Analytical Framework: Design Thinking Principles and Related Questions.
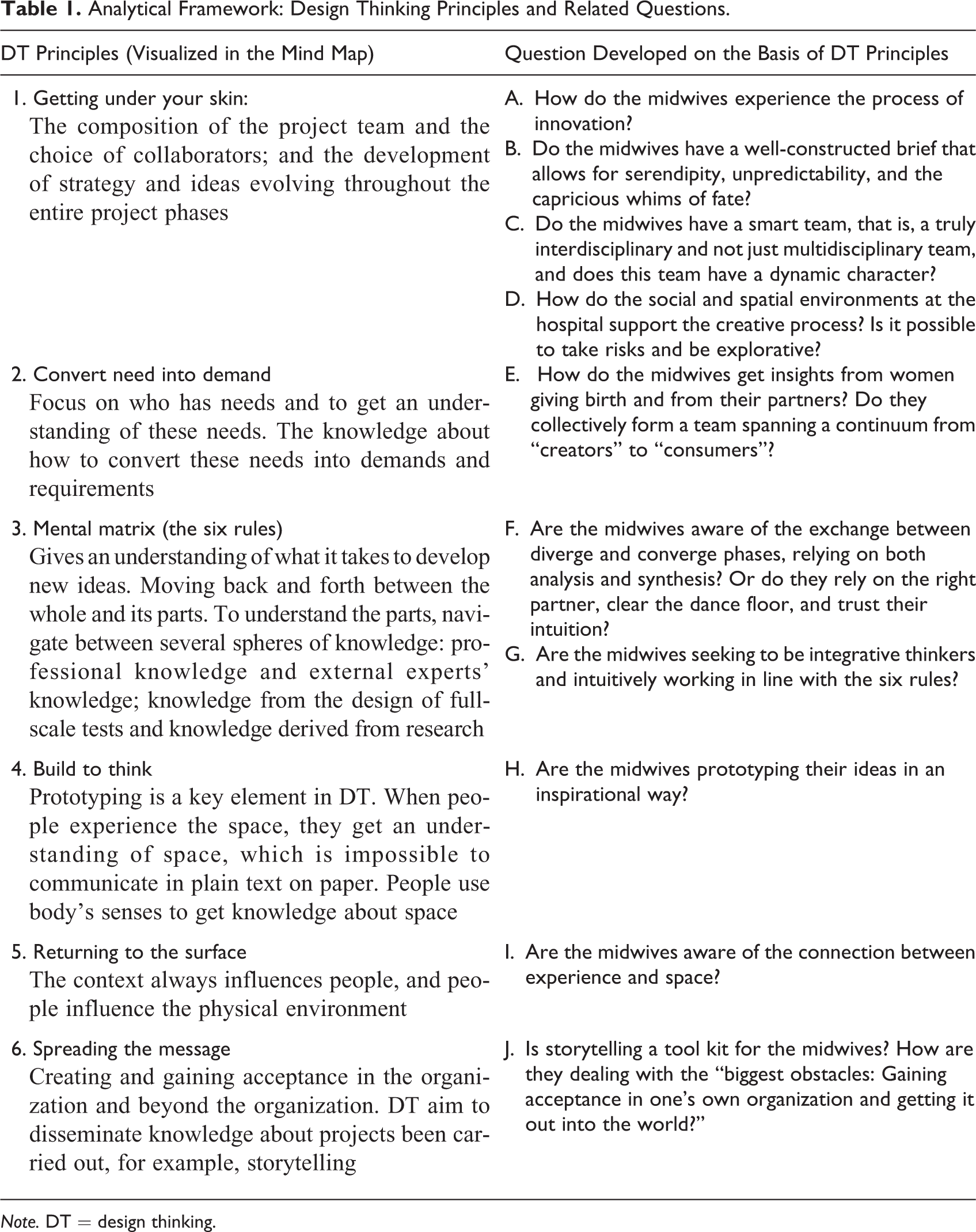
Note. DT = design thinking.
Getting Under Your Skin
How do the midwives experience the process of innovation?
The midwives experienced that they were moving forward and backward in the process and that they created new knowledge along the way. Furthermore, they said that many paths led to nothing and summed up that the processes were not linear. The midwives stated that their project, encompassing selected concrete actions, was unique for birth environments. They experienced that they could not easily transfer tangible physical elements from a completely different room to their room, that is, the birth environment. For example, they could not transfer the effects of red- and green-colored light in an operating theater to the birth environment. But the very process of developing new ways of creating space and design in healthcare could be transferred from one place to another. This is in line with Brown’s thoughts. The way to mix elements in development processes is the same, but the specific and concrete actions and choices made along the way are unique from process to process. The primary focus can be on three different elements: organization, professional development, or specific spatial elements, and this will vary from project to project. The genuine scope of a healing birth environment calls for awareness of all three elements.
Do the midwives have a well-constructed brief that allows for serendipity, unpredictability, and the capricious whims of fate?
The midwives had a kind of brief describing the project, specifically three areas that were to be covered—obstetrics, midwifery care, and spatial atmosphere. The brief was based on the department’s strategy, and the midwives stated that: “Strategy is not a dead piece of paper in a drawer; it is dynamic and should be used actively.” The midwives’ first, nonprioritized advice is: Be clear on your strategy and use it as your professional benchmark. The brief allowed for unpredictability. For example, the head midwife said that it was very important for the project that contact was made with a person who had sufficient technological skills to control light, sound, and picture. This contact came about coincidentally, as they met this technician whose wife was giving birth to their baby at the maternity ward. On the other hand, the midwives were also conservative, as illustrated in the following statement: “From the beginning, we knew that we would have a tub and a sofa.” From the very start of the process, the midwives were determined that two elements they knew beforehand should be present in the room. The two statements reveal a schism between a mind-set harboring the ability to be open-minded and to be conservative at the same time. From a design thinker’s point of view, no elements in a space should be nonnegotiable from the starting point of a project. This means that everything should be welcomed into the process thinking in new ways.
Do the midwives have a smart team, that is, a truly interdisciplinary and not just multidisciplinary team, and does this team have a dynamic character?
This project was gifted with numerous collaborators. According to the midwives, the interdisciplinarity of the collaborators was very rewarding. Several times, they praised getting inspiration from other professions and reported having gained from being shaken and disturbed in their traditional ways of thinking. It was a challenge and it took a long time to find the right collaborators. A very large part of this interview addressed relations with collaborators and, in particular, it was noted that establishing the right partners was important. Second piece of advice: Solicit assistance from other professions than your own.
The midwives emphasized that collaborators needed to display clear professionalism, accept being challenged, and not solely focus on problems. This is reflected in the third piece of advice: Choose collaborators who are ready to contribute their strong skills to your own visions. The close collaboration between the two managing midwives was of pivotal importance, and they regarded it as crucial to the project. This is not an “ordinary” DT approach, where the most important advice is to establish an interdisciplinary team with collective ownership to ideas. However, as mentioned by Brown: “Sometimes just choose the right partner.” This must have been the case in the present project and maybe this team was more truly multidisciplinary than interdisciplinary, with the two midwives being on top of all processes.
How do the social and spatial environments at the hospital support the creative process? Is it possible to take risks and be explorative?
The midwives experienced that the public health system was a bit sluggish and thought that it could benefit from collaboration with the private sector. An example of this is the collaboration with the internal technical department, where they encountered difficulties trying to be innovative when establishing new ways of creating a hygienically safe environment. Bringing in private companies changed the attitude to “of course we can do this.” This is reflected in the fourth piece of advice: Do not hesitate to contact private companies—they also need you.
The midwives had assistance from the MedTech Innovation Consortium (MTIC). The MTIC is an organization founded by University of Aarhus in collaboration with the 16 municipalities of the region to support private firms creating growth through healthcare innovation, bridging between the public and the private sector. For example, the MTIC financed two workshops aimed at generating ideas and presenting the midwives to private firms. Advice Number 4 is probably specific to the Danish healthcare system, which is primarily publically funded. The public healthcare sector is considerably larger than the private healthcare sector, and for many years, the two sectors have been separated, although recent years have seen growing intersectoral collaboration.
Convert Need Into Demand
How do the midwives get insights from women giving birth and from their partners? Do they collectively form a team spanning a continuum from “creators” to “consumers”?
To get inspiration, the midwives visited other departments, among others the department of neurosurgery, the Multidisciplinary Pain Center, the Snoezelen House, and other maternity wards in Denmark and England. They participated in theme days, lectures, and workshops. The fifth piece of advice: Do pay a visit to be inspired.
Together with the MTIC, they organized a workshop matching the criteria of Brown’s “unfocused group.” The only difference was that no individuals were invited only because of their experience of giving birth; however, they subsequently learned that the participants had experience with births in one way or another.
The midwives did not systematically observe the users, viz., the couples giving birth and the staff. The staff participated in a full-scale test of the birth environment. They also participated as observers in one of the workshops and were consulted from time to time in the coffee room. During the interview, one of the midwives mentioned that all midwives in the department had their own private opinion about how the room should be equipped.
The two participating midwives said that they did not want to involve other midwives because they had to establish common ground, which could be achieved only if the midwives’ personal preferences were not taken into account. This explains why the staff was not involved in the decisions.
In an EBD scheme, the midwives appear as users, but in this project, the two midwives were leading the innovation and they were responsible for converting need into demand. They responded to observations and information they had gathered over the years. The end users were women giving birth or about to give birth, and they were not well represented in the workshop or in other sessions. This does not suggest that the midwives were not trying to empathize with the users, but the users’ active involvement was low. In DT, users occupy a key role in development projects. In this case, the midwives were strongly represented, whereas the end users, viz., the woman giving birth and her partner, were largely absent.
Mental Matrix
Are the midwives aware of the exchange between diverge and converge phases relying on both analysis and synthesis? Or do they rely on the right partner, clear the dance floor, and trust their intuition?
The midwives experienced that they were moving back and forth in the process, creating new knowledge along the way. Furthermore, one can say that the midwives did indeed chose the right partner, cleared the dance floor, and trusted their intuition. This is also underpinned in the sixth piece of advice: First find a good friend and the seventh piece of advice: Be faithful to your intuition.
The midwives navigated the entire mental matrix. The workshops facilitated by the MTIC were conducted in the diverge phase. Techniques like brainstorming and visual thinking were used. It is difficult to map how they analyzed and synthesized their thinking and brainstorming activities. In the converge phase, they talked about intuition and knowledge obtained from collaborators. The midwives used research on healing architecture and the hormone oxytocin to support their intuition, suggesting that space made a difference in the birth situation. Moreover, they used research to communicate their project. They stated that “expertise makes it easier to make an impact.” Hence, they used both research and intuition and gave equal rank to both aspects.
In order to develop, you will eventually have to try something you have never done before. But instead of stepping out onto thin ice, you can qualify your design solution drawing on research and experience from other cases. An EBD project is carried out with intuitive thinking.
Are the midwives seeking to be integrative thinkers and intuitively working in line with the six rules?
The midwives are attentive to their management’s priorities and are keen to provide management with knowledge and information to ensure continued commitment. The eighth piece of advice: Include and enthuse your management, notably when big changes are coming up.
Even if one of the two midwives was the head midwife at the department, none of the 10 pieces of advice were aimed at the midwives for whom she was responsible or the birthing women and their partners at the department. The other midwife described that the department’s midwives functioned as sparring partners and said: “They are kind of taking on a supporting role, more so than a decision-making role, deciding whether it should be this or that kind of couch…it has been important to clarify for them that when you have to furnish a room, then you really need to put your personal preferences aside.” It may be questioned whether this approach gives the whole organizational ecosystem room to experiment (Rule 1).
In the present case, the midwives were about to move into a new building, and they were keen to make the best out of it. They were certainly in a position where they were exposed to changing externalities (Rule 2). The midwives said: “We have been involved in all these things; so, in this way, we have been given the opportunity to contribute because it is more difficult to change something that is already there. So, it also about saying that when you get the opportunity, you should grab it when it is there, and you are able to feel that now is now. Now you have only one chance, and it will not be there another time.”
The midwives were very much aware of the good ideas that other people contributed (Rule 3). Several persons were mentioned creating the Snoezelen effect of the room (projecting atmospheric images on the walls) and “birth GPS” (a symbolic Global Positioning System tracker which gives information on birth progress), for example.
Starting the project, the midwives did pitch ideas on how to create future birth environments in many different situations (Rule 4). The feedback they got from people was very positive and everybody found the pitching meaningful. The pitching confirmed their gut feeling about the project. The experience the two midwives had when they visited a Snoezelen room was the thing that gave them the buzz. This led to advice Number 9: You should allow yourself to accept a certain measure of disruption.
The chief midwife had a close relation to the management of the hospital (Rule 5). At a certain point, she needed a loss warranty to get on with the project, and the management gave her the warranty. One of the midwives said many times during the interview that she wanted to challenge status quo. This was supported by hospital management. On the other hand, being a leader herself, it remained unclear how the midwife tended, pruned, and harvested her workers’ ideas.
The project had one overarching purpose (Rule 6) that grew out of the strategy for the midwifery care. It consists of three parts: (1) safety, (2) relations, and (3) atmosphere in space. The strategy was not a dead piece of paper lying in a drawer. It was devised with a main concern for what was best for the patients and not for a certain profession. “It’s about being true to your ideas, and that things should go in one direction and to dare stand up for it. It did provide some unease,” according to the interview with the midwives. The strategy was very important for the project. The strategy connected care with space, that is, the keystones for creating healing architecture. This is supported by the first piece of advice (Be clear on your strategy).
Build to Think
Are the midwives prototyping their ideas in an inspirational way?
The second workshop was a 1:1 mock-up workshop conducted to test the physical setting of the birth environment. At this early stage, the participants at the workshop found that the bed should stand with the bedhead toward the wall like it had always done. This gives the bed a central position in the space. The midwife mentioned that in the following process, the traditional position of the bed was questioned by people outside the project. The midwives trusted the wisdom of this decision because the decision was informed by multiple tests involving different healthcare professionals. However, these tests did not involve end users (women and their partners). It may therefore be questioned whether these tests gave the full and complete picture. The other persons who participated in the test were obstetricians, social and healthcare assistants, and security representatives.
Two midwives visiting a Snoezelen house experienced pictures being projected on the wall and reported this experience to be groundbreaking: “We discovered that you may design a room that changes fundamentally; that was really surprising.” The midwives used the prototyping to gain credibility among their colleagues. They said: “Someone else said it [i.e., made them credible, ed.]. It is not just us saying it.”
The first prototype was primarily developed for testing functionality and safety. The prototype currently being used tested atmosphere in space and was being used daily. However, it is uncertain whether the midwives conducting the 1:1 test were conscious of how the selection of participants affected the understanding of the room. Maybe other perspectives on the birth situation would have been represented if other professions had participated.
Returning to the Surface
Are the midwives aware of the connection between experience and space?
The space is a mock-up for the future space at the new hospital they are about to move into. In that way, the space tests and prepares the midwives on the floor for mowing into a new building, and it gives them the opportunity to discuss what they are doing in the space during the birth situation. One of the midwives said: “I got an SMS from a midwife who wrote: I become a better midwife in room 2 [the decorated space, ed.], and I become a better human. Another midwife recently said that she uses the space for reflection. If she had a birth that concerned her a lot—then she calms down [i.e., in room 2, ed.]. So, the room also influences you as a human.”
Spreading the Message
Is storytelling a toolkit for the midwives? How are they dealing with the “biggest obstacles: Gaining acceptance in one’s own organization and getting it out into the world!”
During the project, video recordings were used to document the process. This was important and is reflected in the last, 10th piece of advice: Use video and pictures to keep and to remember sentiments and important elements along the way.
The midwives said that the space itself was very important as a communication tool. Their management did not see the full potential of the new birth environment beforehand, but having seen the space, they understood its power. They talked to management from other departments and recommended that they visit the new space. So, they shared the story about the new birth facility and said: “There was no need to travel out in the world because we have the nicest and newest birth environment right here.” It served as inspiration for other professional groups and departments at the hospital.
To handle the press, the midwives contacted the hospital’s head of communication. Danish national television reported from the hospital and several newspapers brought the story featuring pictures from the space. DT aims to disseminate knowledge about projects that have been carried out. Depending on the kind of research methodology used to evaluate a construction project, the EBD designer must have a certain amount of patience and await the collection of research data before being able to disseminate the results of the project.
Conclusions and Perspectives
The key contribution of the present article, as argued above, is that the case illustrates how midwives’ involvement in a creative process adds a novel dimension to design processes because EBD and DT are merged into EBDT. Merging EBD and DT into EBDT can facilitate midwives’ involvement in a creative process. DT contributes with process guidance and an analytical stance (Table 2).
From EBD to EBDT.
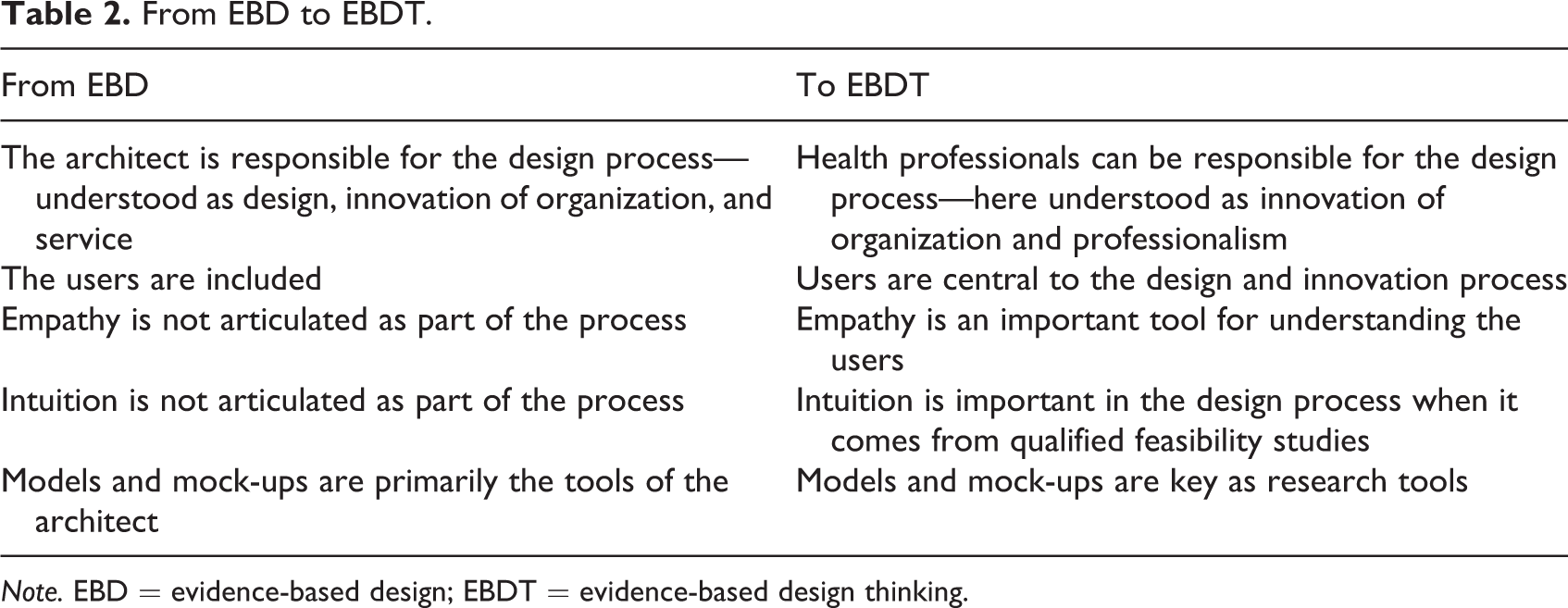
Note. EBD = evidence-based design; EBDT = evidence-based design thinking.
Briefly, the difference between EBD and EBDT lies in several dimensions. First, in EBD, the architect is solely responsible for the design process, which encompasses the creation of form and innovation of organization and services, whereas in EBDT, healthcare professionals may also be involved in the design process, which also involves innovation of both organizational and healthcare professional dimensions. Second, whereas EBD involves users, they take center position in the design process in EBDT. Third, empathy and intuition are not considered part of the EBD process, whereas in EBDT, empathy is a valuable tool for understanding users and intuition is critical to the innovation process, provided it is rooted in adequate preparatory groundwork. Finally, in EBD models and mock-ups tools are primarily used by the architect, while they are also used as important tools of investigation in EBDT.
The midwives became active participants in developing and designing a birth environment while focusing on midwifery care. The process reached beyond research and design to encompass development aimed at optimizing and improving the midwives’ professionalism. The analysis showed what the midwives intuitively did to develop and create innovation, and additionally, which principles they did not use intuitively, but which have a potential to be adapted to make future innovation even better.
EBDT offers an understanding of what it takes to develop new ideas. Moving back and forth between the whole and its parts is important. To understand the parts, the midwives navigate between several spheres of knowledge: their own professional knowledge and that of external experts, knowledge from the design of full-scale test rooms, and knowledge derived from research. The way they combine these parts to form a whole project is governed by their “gut feelings.” This gut feeling may be dubbed qualified intuition. Lundin (2015) explores this issue in his PhD dissertation, where he argues that intuition is part of the design process. A similar situation is seen in nursing where Patricia Benner worked with intuition as knowledge of the highest order (Benner & Tanner, 1987). In EBDT, research and intuition go together.
It is essential to make visible the importance of the physical setting to human behavior in any situation. Several examples from the present case illustrate the association between the midwives’ experiences in particular rooms and what they choose to do design-wise in the project. Particularly, significant is their experience with the Snoezelen room; another example is their experience that a birthing woman who was not at ease was placed in a well-equipped room which actually made her calm down. When DT is integrated into the EBD process, intuition becomes recognized as a fundamental part of the development processes. The experiences from the case support that we use our intuition when synthesizing and creating unity and coherence. Knowledge from research, users, and context ensures that we make choices that are not solely based on gut feelings because they are also informed by qualified intuition.
Prototyping is a key element in DT. When people experience the space, they get an understanding of space, which is impossible to communicate in plain text on paper. We use all our body’s senses to get knowledge about space (Pallasmaa, 2005). This kind of knowledge is crucial to making the right decisions about design solutions.
The knowledge we have developed in this case is based on midwifery but can be extended to other healthcare professions. There is a potential for developing dissemination materials for professionals facilitating their participation in development projects. Health professionals who are basically unfamiliar with design processes could benefit from a Practitioner’s Guide to Design Thinking in EBDT. The guide may help them to describe their role in development projects and provide them with concrete tools.
EBDT calls for awareness of both research, design, midwifery care, and perspectives on space from women giving birth and their relatives. Collectively, that can provide the genuine scope of a healing birth environment.
Current birth environment research devotes hardly any attention to the very process of creating an optimal birth environment. In EBD, the primary focus is on the researchers’ and the architects’ roles, not on those of the healthcare professionals. Combining EBD with DT allows us to focus on the role of the midwife who creates a genuine, healing birth environment in collaboration with the woman giving birth. Genuineness arises when all users experience that the physical setting optimally underpins the birthing situation.
Limitations
Our research is within a new practice domain—midwifery—and has only covered the initiating stage of the case project; more of the collected case material and informants could be drawn in to support the analysis.
Implications for Practice
Research and intuition are equally important for designing genuine birth environment. Going from evidence-based design to evidence-based design thinking empowers midwifes in design and innovations projects. All users of the space are important. Genuineness arises when all users experience that the physical setting optimally underpins the birthing situation.
Footnotes
Acknowledgement
This study is associated with the Birth environment of the future - a research project of the Maternity Ward of The Regional Hospital West Jutland, Herning, Denmark. We thank the Midwife head of department and the Innovation coordinator midwife RM for the maternity ward’s participation in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.