
Abstract
Objective:
This is a translational science article that discusses copper alloys as antimicrobial environmental surfaces. Bacteria die when they come in contact with copper alloys in laboratory tests. Components made of copper alloys were also found to be efficacious in a clinical trial.
Background:
There are indications that bacteria found on frequently touched environmental surfaces play a role in infection transmission.
Methods:
In laboratory testing, copper alloy samples were inoculated with bacteria. In clinical trials, the amount of live bacteria on the surfaces of hospital components made of copper alloys, as well as those made from standard materials, was measured. Finally, infection rates were tracked in the hospital rooms with the copper components and compared to those found in the rooms containing the standard components.
Results:
Greater than a 99.9% reduction in live bacteria was realized in laboratory tests. In the clinical trials, an 83% reduction in bacteria was seen on the copper alloy components, when compared to the surfaces made from standard materials in the control rooms. Finally, the infection rates were found to be reduced by 58% in patient rooms with components made of copper, when compared to patients' rooms with components made of standard materials.
Conclusions:
Bacteria die on copper alloy surfaces in both the laboratory and the hospital rooms. Infection rates were lowered in those hospital rooms containing copper components. Thus, based on the presented information, the placement of copper alloy components, in the built environment, may have the potential to reduce not only hospital-acquired infections but also patient treatment costs.
Keywords
Introduction
Healthcare-associated infections (HAIs) are a growing concern that continues to challenge infection control and prevention programs throughout the world. In 2002, it was estimated that 1.7 million people acquired an infection annually while in U.S. hospitals, resulting in approximately 98,987 deaths, or 271 fatalities per day. The U.S. Centers for Disease Control and Prevention reported that HAIs cost U.S. hospitals between 35.7 and 45 billion dollars annually in treatment cost alone (Scott, 2009). Microbes have an intrinsic ability to survive on commonly touched surfaces which facilitates their acquisition and transfer from surfaces to humans. The microbial burden of frequently touched surfaces in healthcare facilities may play a significant role in infection causality (Boyce, 2007). Clinical evidence indicates that copper alloy surfaces may have the potential to reduce microbial burden on surfaces in the clinical setting (Schmidt, Attaway, Sharpe, et al., 2012) as well as decrease hospital-acquired infections (Salgado et al., 2013). Thus, the use of solid copper alloy touch surfaces should be considered as a second line of defense against disease-causing organisms, after hand washing and compliance with infection control policies. The registration of copper alloys with the U.S. Environmental Protection Agency (EPA) permits making public health claims against six disease-causing bacteria (Anderson & Michels, 2008). By killing bacteria, copper alloys may offer passive protection between routine cleaning and disinfection (Anderson & Michels, 2008). In addition to the bacteria covered by EPA registration, the efficacy of copper alloys against a range of important pathogens, including viruses and fungi, is well documented in the literature, as will be discussed. Hand washing, cleaning, and disinfecting are critical in mitigating the transmission of microbes. However, these solutions rely on human behavior. The intrinsic antimicrobial activity of metallic copper alloys is a passive system that requires no human intervention and its action is continuous rather than episodic. A recent clinical trial demonstrated that limited placement of copper alloy surfaces within the built environment resulted in an average 83% reduction of the bacterial burden (Schmidt, Attaway, Sharpe, et al., 2012) and a 58% reduction in the incidence of HAI (Salgado et al., 2013). The specification and deployment of components with touch surfaces made from copper alloys may have the potential to reduce HAIs, lower treatment costs, and save lives. The analysis presented later illustrates that the additional cost of copper components above the cost of those made from conventional materials is recovered within 2 months. A review of the efficacy of solid copper alloy surfaces against a range of important infectious organisms will be provided to illustrate the capabilities of these materials and justify end use applications for copper alloys in healthcare facilities and beyond, in schools, mass transit systems, cruise ships, and the hospitality industry.
Copper Alloys
Copper alloys are metallic materials in which copper is the primary alloying element. Other elements are added to or combined with copper, typically by melting, to form alloys with new and different desirable properties, such as increased strength and corrosion resistance. However, nothing other than copper is needed to provide antimicrobial efficacy in copper alloys. Common alloys include brass (an alloy of copper and zinc), bronze (traditionally copper and tin, but other elements can be used), and copper–nickel alloys. The outer surfaces of U.S. coinage—nickels, dimes, and quarters, among others—are made from copper–nickel alloys.
Antimicrobial Laboratory Research
Tests were conducted at indoor ambient conditions similar to those found in hospitals. Stainless steel Type 304 was used as the experimental control in the laboratory tests since it is biologically inert and has no known antimicrobial effect. Disease-causing organisms were placed on copper alloy samples, and viability was determined following different times of exposure. Although the kill mechanism needs additional elucidation, one possibility is that copper, which is recognized as essential, enters the cell, perhaps as ions. When a lethal dose is reached, copper seems to interfere with normal cell functions and compromise membrane integrity. There is some evidence that copper impedes cell respiration and metabolism and causes DNA damage (Warnes, Caves, & Keevil, 2012; Weaver, Noyce, Michels, & Keevil, 2010). This results in rapid death, which makes it unlikely that the cells will have sufficient time to reproduce.
Methicillin-Resistant Staphylococcus aureus (MRSA)
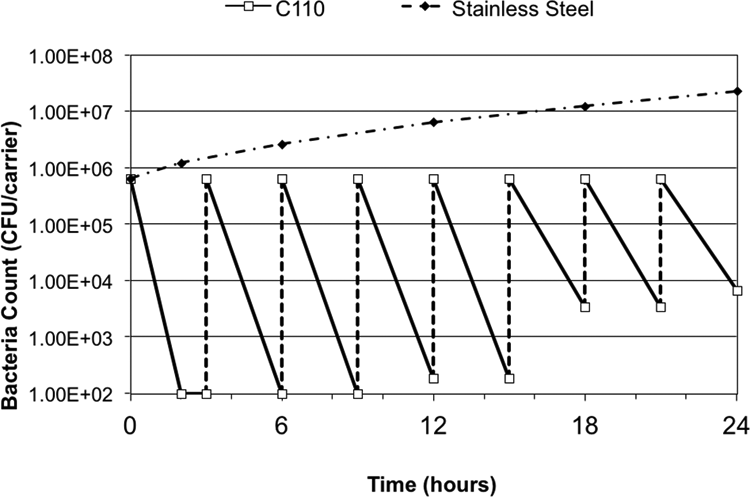
Staphylococci are ubiquitous and easily transferred between individuals, or to objects where they are subsequently acquired by healthcare workers or patients and readily transferred to others. S. aureus is a component of many people’s skin flora. Although anyone can be infected by Staph, some individuals are more susceptible. When these bacteria find a weakness such as an open wound, or when an individual who is immune-compromised is exposed, a deadly infection may occur (Tierno, 2001). Among the antibiotic-resistant bacteria, MRSA is of particular concern. MRSA infections cause about 126,000 hospitalizations each year in the United States (Kuehnert et al., 2005), although many hospitals have successfully reduced the rates in recent years (Jain et al., 2011). Copper’s efficacy against MRSA has been demonstrated in several independent studies (Gould et al., 2009; Mehtar, Wiid, & Todorov, 2008; Michels, Noyce, & Keevil, 2009; Noyce, Michels, & Keevil, 2006a; Weaver, Noyce, et al., 2010). Perhaps the most illustrative representation of copper’s efficacy against MRSA is shown in Figure 1. In this case, a 99.9% copper alloy (C110) and stainless steel (S304) were inoculated with ∼700,000 colony-forming units per square in. (CFUs/in2), a total of 8 times in a 24-hr period, without any intermittent wiping or cleaning. The concentration of each inoculum is at least one order of magnitude higher than the surface contamination levels measured on noncopper surfaces in the intensive care units (ICUs) of three U.S. hospitals, which ranged from a several hundred to the several thousands of CFUs (Attaway et al., 2012; Schmidt, Attaway, Fairey, et al., 2013; Schmidt, Attaway, Sharpe, et al., 2012). As can be determined from the data used to develop Figure 1, greater than 99% of the MRSA were killed by the copper alloy surface after eight equally sized inocula of ∼7 × (105) CFU/in2 of MRSA at 3 hr intervals over 24 hr. However, the stainless steel coupons continued to not only harbor viable MRSA, but also showed substantial and increasing concentrations of MRSA after each inoculation. This figure illustrates that copper alloys can continue to kill MRSA, even after repeated inoculations, while bacteria resident on the stainless steel continue to survive and grow. It has been reported (Gould et al., 2009) that three of the five clinically important MRSA strains tested on pure copper were killed within 60 min, and the remaining two strains were killed within 80–100 min. Furthermore, these authors (Gould et al., 2009) also reported similar efficacy against community-acquired methicillin-sensitive S. aureus (CA-MSSA). All five tested strains were killed within 80 min. These findings are significant because the number of cases of CA-MSSA continues to increase, as healthcare-associated MRSA has spread to non-healthcare settings in the community. It is important to note that most laboratory efficacy tests utilize very high initial inoculation levels, which are typically greater than one million CFU/in2, in order to clearly demonstrate efficacy. Alloys containing lower levels of copper, including brass and bronze, were tested against MRSA and also exhibited greater than 99.9% kill within 2 hr when challenged with these high inoculation levels (Anderson & Michels, 2008). It has also been shown (Noyce et al., 2006a) that lowering the initial bacterial load to levels closer to those found in the clinical setting resulted in a shorter time to kill MRSA (Figure 2). This has practical significance because in the typical clinical setting, copper alloys kill most of the bacteria in a matter of minutes rather than hours.
Continuous reduction test results for methicillin-resistant Staphylococcus aureus on copper alloy C110 (99.9% Cu; Anderson & Michels, 2008).
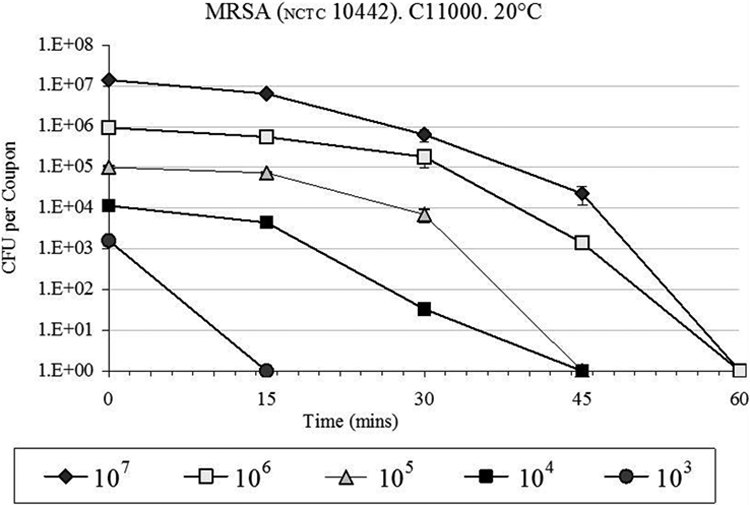
Initial inoculum level shortens the time for copper alloy C110 (99.9% Cu) to kill methicillin-resistant Staphylococcus aureus (Noyce, Michels, & Keevil, 2006b).
Vancomycin-Resistant Enterococci (VRE)
Approximately a third of enterococcal infections in ICUs in the United States are caused by VRE (Warnes, Green, Michels, & Keevil, 2010). VRE is primarily transferred by touch between patients, healthcare workers, and environmental surfaces (Drees et al., 2008). It was reported (Warnes et al., 2010) that strains of vancomycin-resistant Enterococcus faecalis and Enterococcus faecium were killed by alloys containing 90% or more copper in 1 hr, when initial inoculations were greater than one million CFU/cm2, but survived for several weeks on stainless steel. Other researchers (Gould et al., 2009) reported that approximately 10 million CFU/cm2 of five clinical strains of VRE were killed by a pure copper alloy within 1 hr.
Escherichia coli O157: H7 (E. coli O157: H7)
This virulent strain of E. coli is responsible for numerous food recalls, illnesses, and deaths. Outbreaks are commonly associated with undercooked beef (Noyce, Michels, & Keevil, 2006b), although contaminated drinking water can similarly result in illness. Exposure may result in mild to severe stomach cramps, vomiting, and kidney failure as a consequence of hemolytic uremic syndrome. However, there are many strains of E. coli, and some are found in hospitals (Jarvis & Martone, 1992). Over 30 years ago, another researcher (Kuhn, 1983) reported on a student nurses' project conducted in a hospital that demonstrated that doorknobs made of brass, a copper alloy, showed sparse growth of E. coli, while the stainless steel counterparts were heavily colonized. In a laboratory study, this researcher (Kuhn, 1983) also found that little bacteria was present on copper and brass strips inoculated with E. coli, while heavy contamination persisted on aluminum and stainless steel samples. More recently, Noyce et al. (2006b) inoculated various cast copper alloys with E. coli O157:H7. All of the copper alloys killed the organism in times ranging from 45 min to 6 hr. Several independent studies have confirmed that copper alloys effectively kill various strains of E. coli (Anderson & Michels, 2008; Espírito Santo, Taudte, Nies, & Grass, 2008; Gould et al., 2009; Noyce et al., 2006b; Warnes, Caves, et al., 2012; Wilks, Michels, & Keevil, 2005). A methodology termed a “dry inoculation method” was developed (Espírito Santo et al., 2008). This method better simulates the real-world situation when humans touch surfaces by limiting the volume but not the concentration of an indicator microbe applied to a surface. A volume equal to 1 microliter (µl) containing a known concentration of the bacterium under evaluation is applied to a surface using a swab application. The liquid quickly evaporates placing the microbe in direct contact with the microbicidal copper surface. This method was simplified and made more reproducible for VRE (Warnes et al., 2010) and subsequently E. coli O157: H7 (Warnes, Caves, et al., 2012), by adding 1 µl directly to the surface and spreading with the pipette tip, allowing drying in seconds. When these dry inoculum methods are used, the time required for a substantial reduction in viability of the applied population of bacteria is greatly reduced, when compared to the time to death observed in the widely used wet method of inoculation used in laboratory research and EPA efficacy testing. For example, the kill time for C11000 (99.9% Cu) when challenged with E. coli O157: H7, was significantly shortened where a nine logs reduction in live bacteria was observed in 1 min ( Warnes, Caves, et al., 2012). The dry inoculum method was also used to challenge a copper–nickel–zinc alloy (C75200, 65% Cu) and a brass (C28000, 60% Cu; Espírito Santo et al., 2008). Both alloys resulted in the death of over one billion CFUs of E. coli within 15 min.
Clostridium difficile (C. difficile)
This anaerobic spore forming bacterium is highly resilient and often afflicts patients taking broad spectrum antibiotics. When stressed, vegetative C. difficile responds by forming spores to survive. It was reported (Kramer, Schwebke, & Kampf, 2006) that C. difficile spores can survive on dry surfaces for up to 5 months. Additionally, C. difficile spores are not killed by all hospital-grade disinfectants. It has been observed by other investigators (Weaver, Michels, & Keevil, 2008) that it is easier for copper alloys to kill vegetative C. difficile than its spores. It was found (Weaver et al., 2008) that exposure to alloys containing greater than 70% copper resulted in a significant reduction in both vegetative C. difficile and its spores in 6 hr, and a complete kill of the more resilient C. difficile spores between 24 and 48 hr, while stainless steel displayed no reduction even after 168 hr of exposure. Vegetative C. difficile died faster, although both vegetative bacteria and spores can be shed in infected feces. Although 24 hr may suggest an inefficient kill rate, efficacy demonstrated by copper alloys is potentially significant, considering that C. difficile spores are especially challenging to inactivate and can germinate even after months of exposure to ambient oxygen on inanimate surfaces in the built environment (Kramer et al., 2006). Other researchers (Wheeldon et al., 2008) utilized a germinant to enhance copper’s efficacy against C. difficile spores. A germinant is a chemical that induces the transformation of spores to weaker vegetative cells. By inducing the germinating spore state, these researchers reported greater than a 99% reduction of over one million CFUs/cm2 within 3 hr of exposure to a pure copper alloy surface. This suggests that germinants may enhance the antimicrobial efficacy of copper alloys against C. difficile spores, but this may not be practical in a healthcare setting.
Influenza A
This virus is responsible for numerous hospitalizations. In addition, hospitalized patients with weakened immune systems are susceptible to influenza infection. Vaccination of healthcare workers can reduce the rate of nosocomial infections among patients (Salgado, Giannetta, Hayden, & Farr, 2004). Influenza A is a viral pathogen that causes significant mortality and morbidity in the elderly and other groups at high risk (Noyce, Michels, & Keevil, 2007). These researchers also reported that copper samples inactivated 75% of influenza A (H1N1) in 1 hr and almost 100% after 6 hr. Viruses are referred to as obligate parasites. Thus, they can’t complete their life cycle without exploiting a suitable host and thus are not considered to be alive. They contain a set of instructions that, when introduced into the host, can generate pathobiological consequences. However, copper alloys can inactivate influenza A (Noyce et al., 2007) and thus may have the potential to significantly decrease its pathobiological consequences.
Norovirus
Norovirus is very contagious, causing 267 million cases of gastroenteritis annually worldwide, resulting in five to eight million deaths (Warnes & Keevil, 2013). Approximately 23 million are infected in the United States each year. It is transferred by hand-to-hand contact, touching environmental surfaces, and ingesting contaminated food. Outbreaks do occur in hospitals and are also frequently reported on cruise ships. Several factors explain why norovirus is so contagious. It has a very small diameter relative to other viruses, and as few as 2 to 10 virions can cause an infection. Infected individuals also shed norovirus for up to 3 weeks after symptoms cease. Norovirus has a protective shell or capsid. However, a freshly diluted (1:10) solution of household bleach (5.25%), sufficient to generate a final concentration of 5,000 parts per million of available chlorine is effective and inactivates norovirus. Presently, neither a vaccine nor an effective treatment is available. Human norovirus cannot currently be cultured in the laboratory, which has hindered the development of effective interventions or control measures. Research on a feline surrogate, a respiratory pathogen, has met with limited success. A murine norovirus, MNV-1, a closer surrogate since it is a gastrointestinal pathogen, was kindly provided by Professor Herbert W. Virgin VI of Washington University. It was observed (Warnes & Keevil, 2013) that the infectivity of MNV-1 was lost upon exposure to copper and copper alloys but retained on stainless steel. These researchers were unable to recover infectious virus after as little as 30 min of exposure to copper (99.9% Cu) and 60 min to copper–nickel (90% Cu) surfaces, when using the wet contact inoculum method (20 µl) volume to simulate slow drying vomitus. In the dry inoculum method, which simulates hand-to-hand or hand-to-object transfer, when a 1 µl volume containing norovirus was placed onto sample surfaces (Warnes & Keevil, 2013), the inactivation was found to be 5 min for both copper (99.9% Cu) and copper–nickel (90% Cu) surfaces. They also showed that contact of the virus with copper surfaces destroyed their RNA genome. Subsequently, it was observed (Warnes, Summersgill, & Keevil, 2015) that capsid integrity was compromised upon coming in contact with copper alloys. Thus, copper alloys can inactivate norovirus and have the potential to help control its transmission.
Other Organisms of Interest
In addition to the previously discussed organisms, solid copper alloys have demonstrated antimicrobial efficacy against a range of other significant microorganisms, including Enterobacter aerogenes (Anderson & Michels, 2008), Pseudomonas aeruginosa (Anderson & Michels, 2008; Elguindi, Wagner, & Rensing, 2009), Acinetobacter baumannii (Mehtar et al., 2008), Listeria monocytogenes (Abushelaibi, 2005; Sandra A. Wilks, Michels, & Keevil, 2006), Klebsiella pneumonia (Mehtar et al., 2008; Warnes, Highmore, & Keevil, 2012), Salmonella enterica (Faúndez, Troncoso, Navarrete, & Figueroa, 2004; Warnes, Highmore, et al., 2012), Campylobacter jejuni (Faúndez et al., 2004), and Candida albicans (Mehtar et al., 2008; Weaver, Noyce, et al., 2010), which is an infectious fungus. It was also reported (Weaver, Michels, & Keevil, 2010) that several other fungi, specifically Fusarium culmorum, Fusarium oxysporum, and Fusarium solani, and Penicillium chrysogenum showed a total die off on copper after 24 hr. Copper also has utility in controlling Legionella pneumophila, the etiological agent of Legionnaires’ disease, in hot and cold water systems through inactivating supporting species in the complex polymicrobial biofilm communities growing on the pipes, unlike materials such as stainless steel, polybutylene, or chlorinated polyvinyl chloride (CPVC) where culturable legonellae proliferated (Gião, Wilks, & Keevil, 2015; Rogers, Dowsett, Dennis, Lee, & Keevil, 1994). In summary, copper alloys have shown, in laboratory tests, that they can kill a broad range of bacteria, fungi, and inactivate viruses.
EPA Registration
The EPA’s Antimicrobial Testing Program ensures that EPA-approved sterilants, and disinfectants, meet stringent efficacy standards. Efficacy testing is designed to rigorously challenge the product, at bacterial concentration levels that are orders of magnitude higher than the microbial levels typically found on surfaces in the built environment. The holders of a public health registration can legally make claims of killing specific microbes, provided they are consistent with the submitted efficacy data and approved by the Antimicrobial Division of the EPA. However, there is another EPA classification of antimicrobial pesticides that has the potential to cause confusion. It is the treated article. The EPA defines treated articles as articles or products that are treated with a pesticide to protect the articles or products themselves. The treated article classification is not for public health uses. Thus, products covered by the treated article classification can’t claim to protect humans from pathogens. Typically, no test data are needed to obtain a treated article classification. Specific organisms cannot be identified, and no efficacy statement can be made or implied. An example of a treated article is a paint or plastic containing a pesticide added to protect the product. Allowable treated article claims include the following: This product contains a preservative to protect the product. Antimicrobial properties inhibit the growth of bacteria that may affect the product. This product controls odor and staining.
In contrast, copper alloys hold EPA public health registrations, which permit stating that they kill the specific bacteria tested under three EPA-approved test protocols (Anderson & Michels, 2008). The six specific bacteria evaluated, which are all included in the EPA registration, are S. aureus, Enterobacter aerogenes, E. coli O157: H7, Pseudomonas aeruginosa, MRSA, and VRE. The first test protocol, efficacy as a sanitizer, measures efficacy after 2 hr, which is an arbitrary time. The second test protocol, residual self-sanitizing, which simulated wear, confirms that the surface retains efficacy after repeated dry and wet rubbing, as shown in Figure 3. It is more challenging than the first protocol, but basically reveals no weakness in copper alloys, which have been shown to retain efficacy after decades of use. Typical examples of copper alloys that have shown long-term efficacy are brass doorknobs and railings found in public buildings. The third and last test protocol, continuous reduction, is the most challenging. As can be seen in Table 1, a total of 252 EPA tests were conducted. A greater than 99.9% reduction (>99.9%) of bacteria was realized within 2 hr in all 84 tests conducted under the first protocol, efficacy as a sanitizer. Similarly, >99.9% reduction was also seen on all 84 tests conducted under the second protocol, residual self-sanitizing. In the third protocol, continuous reduction, the most challenging test, 72 of the 84 tests had a >99.9% reduction, while the other 12 attained reductions ranging from 99.3% to 99.9%. This tabulation of the results of tests conducted under EPA-approved Good Laboratory Practices (GLP) protocols illustrates strong efficacy and demonstrates the ability of copper alloys to kill bacteria under conditions designed to simulate the hospital environment. These regulatory tests establish credibility because they were conducted in an independent third-party laboratory, and the results are subjected to EPA evaluation. Furthermore, the second protocol, residual self-sanitizing, where the surface is rubbed by a cloth, and the third protocol, continuous reduction, in which the surface is repeatedly inoculated, are designed to simulate the conditions seen by environmental surfaces in hospitals. Finally, this regulatory approval is necessary for products to be made available to hospitals, which are needed in a translational science project to “carry science from the bench to the bedside.”
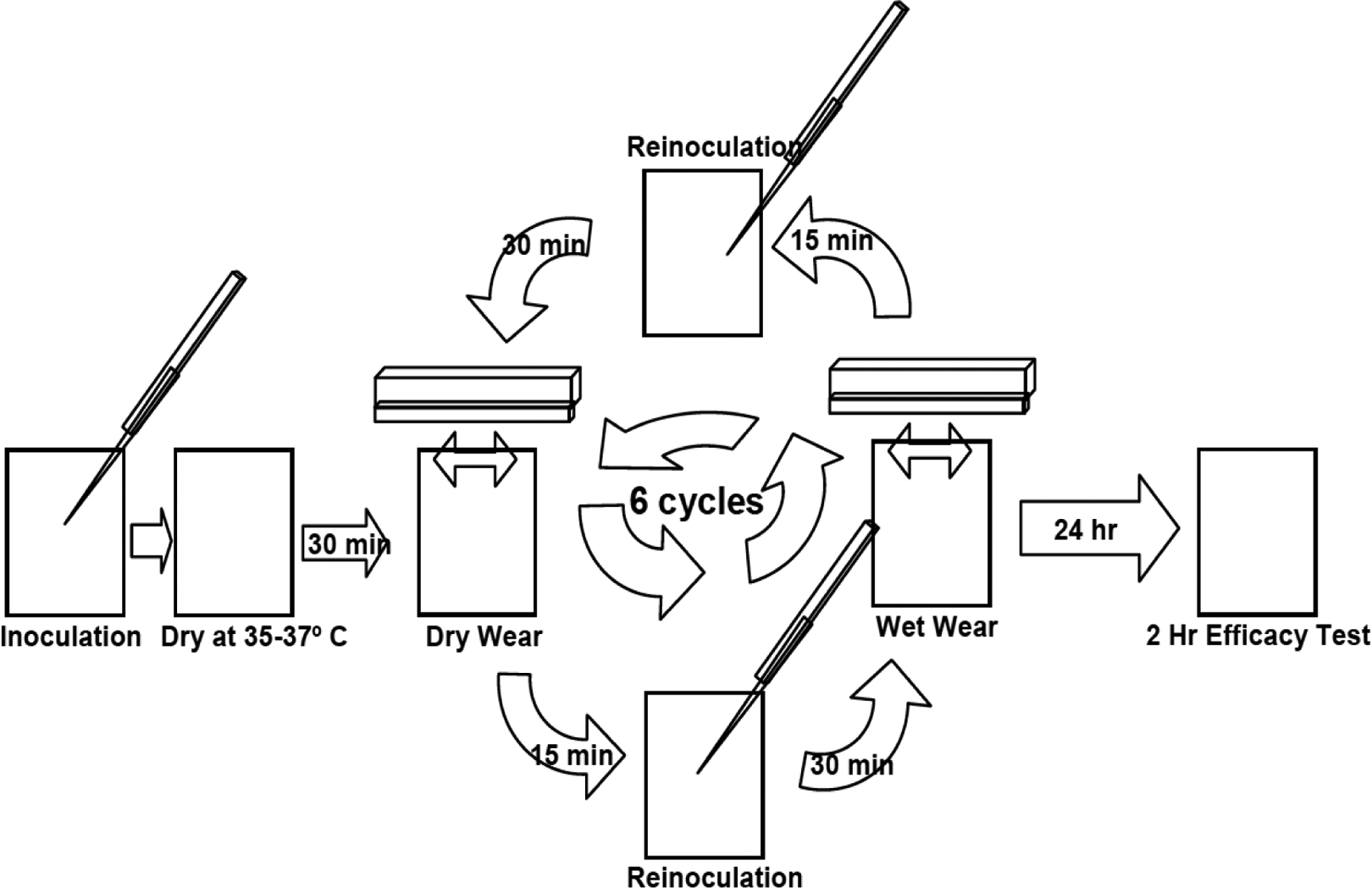
Residual self-sanitizing test, where bacteria counts are measured before and after six alternate wet and dry wear cycles, and the surface is reinoculated with bacteria before each cycle (Anderson & Michels, 2008).
Summary of EPA Test Results Conducted Under Three EPA-Approved Test Protocols on Six Copper Alloys Against Six Bacteria (Anderson & Michels, 2008).
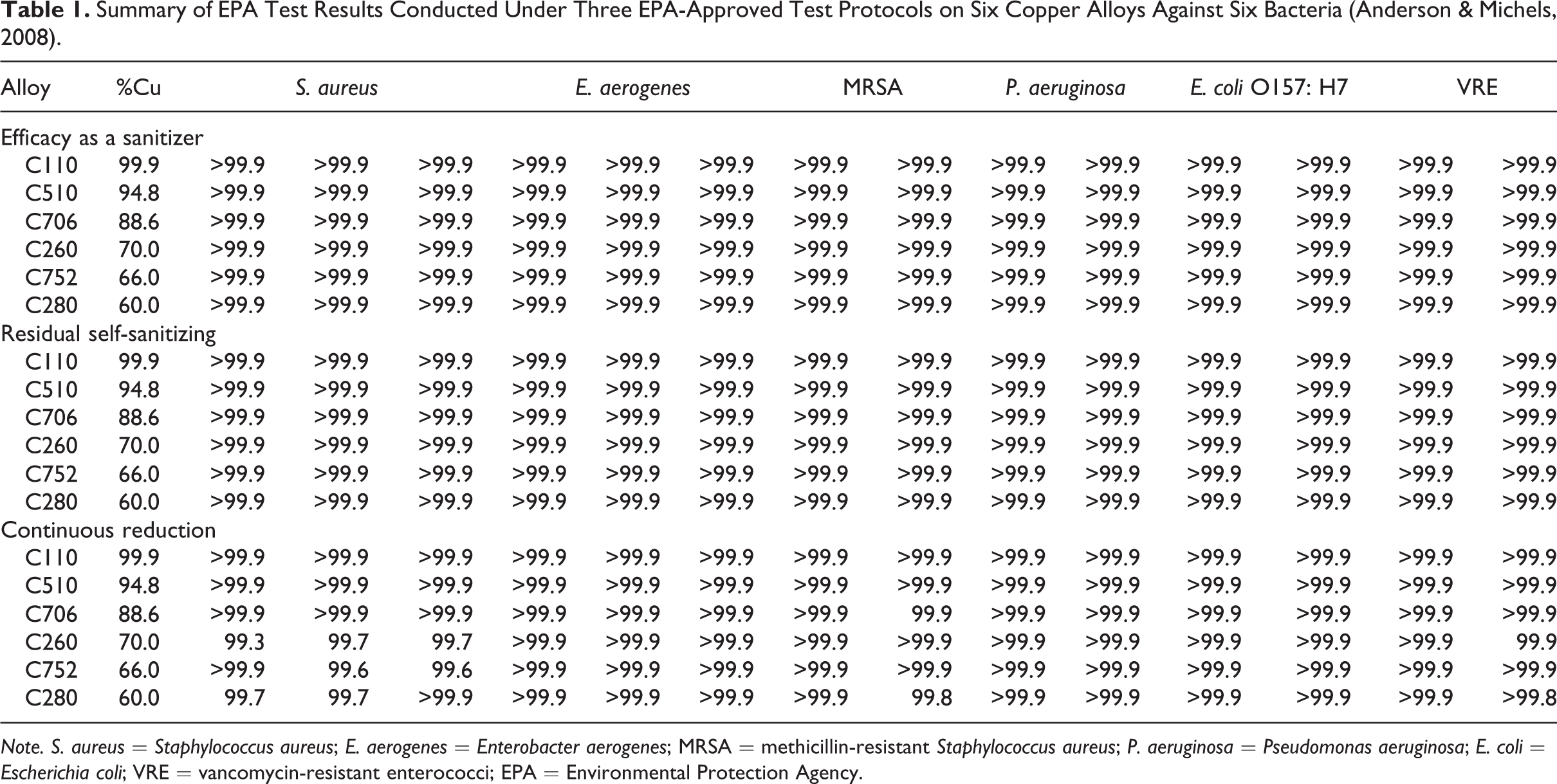
Note. S. aureus = Staphylococcus aureus; E. aerogenes = Enterobacter aerogenes; MRSA = methicillin-resistant Staphylococcus aureus; P. aeruginosa = Pseudomonas aeruginosa; E. coli = Escherichia coli; VRE = vancomycin-resistant enterococci; EPA = Environmental Protection Agency.
Clinical Trial
The clinical trial was designed as an intention to treat randomized control trial to answer several basic questions. Do the components that harbor bacteria contribute to HAI and, if copper alloy surfaces are introduced into the built environment, will their intrinsic antimicrobial properties result in a reduction in microbial burden? If a reduction in microbial burden is observed, will this translate into a reduction in hospital acquired infections? In order to answer these questions, a multihospital clinical trial was conducted in the Medical Intensive Care Units (ICUs) of three hospitals: Memorial Sloan Kettering Cancer Center, in New York City, NY; Medical University of South Carolina, in Charleston, SC; and Ralph H. Johnson Veterans Administration Medical Center, Charleston, SC. Each hospital’s institutional review board for the conduct of studies involving human subjects, as well as the U.S. Army’s Office of Risk Protection, approved the study as was indicated in the initial publications of the clinical trial results (Attaway et al., 2012; Salgado et al., 2013). The trial was conducted in three phases: Phase 1: Determine the baseline microbial burden on objects in existing patient rooms containing components made from standard or conventional materials. Phase 2: Install copper components and compare the microbial burden on conventional components to those found on the copper components. Phase 3: Compare infection rates of patients in standard rooms and copper rooms.
The following six components, which are the closest to the patient, were found to be the most contaminated in Phase 1: bed rails, nurses’ call button, arms of the visitor’s chair, overbed tray tables, data input device (mouse, laptop, and touch screen monitor bezel, which varied by institution), and intravenous (IV) pole.
Clinical Trial, Phase 1: Baseline Microbial Burden on Standard Components
During Phase 1, sampling techniques were developed and refined, including the selection of an optimum method to acquire and then quantitatively and reproducibly release the maximum concentration of bacteria from the sampled surface. The measurements were developed in the setting where the majority of the sampling would occur, the medical ICU. The ICU consists of single-patient rooms containing a variety of components fabricated from plastics (e.g., polypropylene, polyester, and melamine resin), wood, coated steel, aluminum, and stainless steel. A sterile template was placed over each surface, and the exposed area was wiped 5 times horizontally and 5 times vertically (Attaway et al., 2012). These standard rooms subsequently served as experimental control rooms in Phases 2 and 3.
Clinical Trial, Phase 2: Comparison of Microbial Burden
Patients admitted to the ICU were randomly placed in available rooms, without regard to which rooms contained copper surfaces. Bed control personnel were not informed as to which rooms contained copper, but treatment teams were. Information on patient demographics and clinical characteristics was recorded by personnel who were also masked as to which rooms contained copper. The facilities continued to follow existing cleaning protocols, including those prescribed for terminal cleaning. No additional cleaning measures were adopted during the trial. Each hospital also monitored hand hygiene. In addition, no outbreaks of HAIs or epidemiologically significant organisms occurred. Samples were taken weekly from the six objects associated with the copper intervention (eight rooms) and control rooms (eight) from the three hospitals. The microbial burden on the surface of the components made from copper alloys in copper rooms, as well as components made from conventional materials, including plastics, coated carbon steel, aluminum, and stainless steel, in the standard rooms, were sampled and analyzed. It should be noted that one noncopper object, the bed footboard, was sampled in both the copper and the noncopper rooms, unbeknownst to the participating clinicians, environmental services, or the healthcare teams, to control for bias. As can also be seen in Figure 4, the bed rail is the most contaminated item in the standard room, followed by the call button, chair arms, IV pole, tray table, and data input device. A microbial burden below 250 CFU/cm2 is generally accepted as benign (Dancer, 2004; Lewis, Griffith, Gallo, & Weinbren, 2008; Malik, Cooper, & Griffith, 2003; Mulvey et al., 2011; Schmidt, Attaway, Sharpe, et al., 2012; White, Dancer, Robertson, & McDonald, 2008). However, the average microbial burden in the copper rooms, at 465 CFU/cm2, is somewhat above that level, while the average amount measured in the standard rooms, at 2,674 CFU/cm2, is significantly higher. Minor differences in microbial burden can be seen between the components in the copper rooms, as shown in Figure 4. For example, the copper call button has the highest level of contamination, followed by the copper chair arms, copper data input device, copper bed rail, copper tray table, and copper IV pole. The bed rail is a major area of interaction between the patient, healthcare workers, and visitors. Thus, the difference in the microbial burden on copper and noncopper bed rails is very important and most dramatic. This difference in microbial burden decreases in the following order: the bed rail, the call button, the chair arms, IV pole, and tray table. The data input device shows an unexplained anomaly, in that the microbial burden on the copper is slightly higher than that seen on the noncopper counterpart. The contamination levels on both the copper and the noncopper data input devices are quite low, plus the difference in contamination levels is the smallest when compared to the other five objects. The use of the data input device is restricted to healthcare professionals, which is not the case for the other five objects. Healthcare professionals as a group are more cognizant of consequences of patients acquiring infections, which we believe may account not only for the low contamination levels seen on both the noncopper and copper data input devices, but also for the above mentioned anomaly, rather than any difference in frequency of cleaning. The average reduction in microbial burden, when comparing the copper to the noncopper components over 21 months, was 83% (Schmidt, Attaway, Sharpe, et al., 2012). This result is similar to that of another recent study conducted in a pediatric ICU in Chile, where a 88% reduction in microbial burden was observed (Michael G. Schmidt, private communication, January 23, 2015).
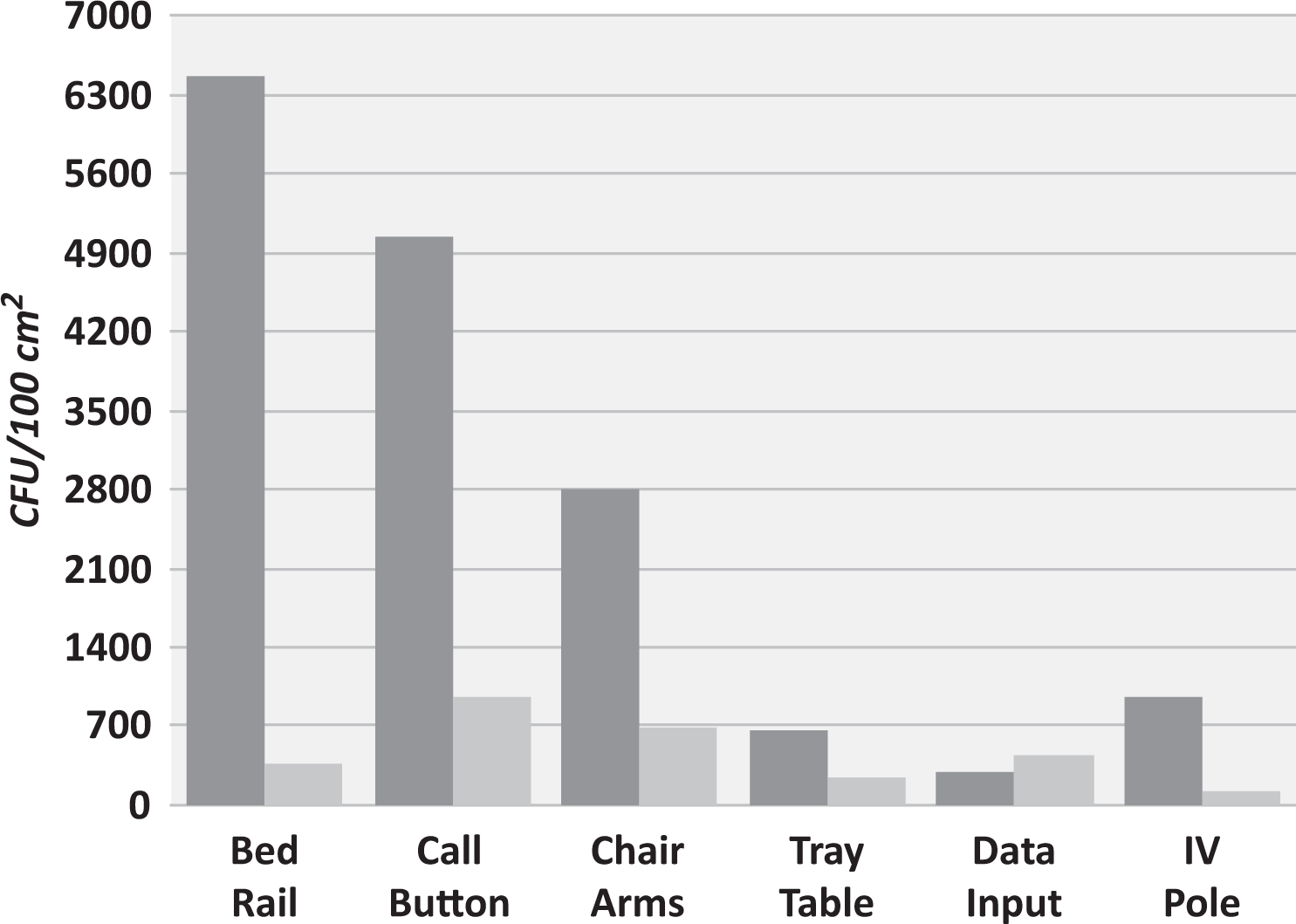
Microbial burden measured on six objects, in the noncopper rooms (dark gray bars) and copper rooms (light gray bars; Schmidt, Attaway, Sharpe, et al., 2012).
Clinical Trial, Phase 3: Infection Rates
The question that Phase 3 asks is will the reduction of microbial burden, measured on the copper components in the copper rooms, result in fewer HAIs, when compared to the number of infections observed during the same period in the control rooms without copper surfaces. Clinicians at each hospital determined incidents of HAIs according to National Healthcare Safety Network definitions. They made a determination regarding infections after examining relevant clinical information. However, they were blinded as to the type of room, copper or noncopper, to which the patient was assigned. Demographics and clinical characteristics between patients admitted to copper and noncopper rooms were comparable.
The infection data recorded in the copper rooms and noncopper or standard conventional rooms at the end of Phase 3 were: treated in copper rooms: 10 infections of the 294 patients, or 10 ÷ 294 = 0.034 = 3.4% and treated in noncopper rooms: 26 infections of the 320 patients, or 26 ÷ 320 = 0.081 = 8.1%.
The infection reduction (Salgado et al., 2013) on a percentage basis is:

It should be noted that a high-level statistical significance was achieved, as indicated by the low p value of .013 (Salgado et al., 2013). Thus, the infection reduction of 58% was achieved by introducing six copper components into the copper rooms. It should be noted that the six copper components comprised less than 10% of the surface area of the room. This 58% reduction in HAIs is seen as a strong testament to the ability of antimicrobial copper surfaces to continuously kill bacteria in the clinical setting between routine cleanings. Note the relationship between microbial burden and risk of HAIs shown in Figure 5. It illustrates that the risk of acquiring an infection increases as microbial burden increases, or dirty surfaces favor acquiring an infection. It applies to all rooms, both copper and noncopper, and is statistically significant (p = .038). The cumulative microbial burden was lower in the rooms containing the copper components. Only 17% of the total 4,450,545 CFUs of bacteria were recovered from the copper surfaces. This is consistent with the infection reduction in the copper rooms, in that a lower microbial burden was observed on the copper components relative to the noncopper components.
This 58% reduction in HAIs is seen as a strong testament to the ability of antimicrobial copper surfaces to continuously kill bacteria in the clinical setting between routine cleanings.
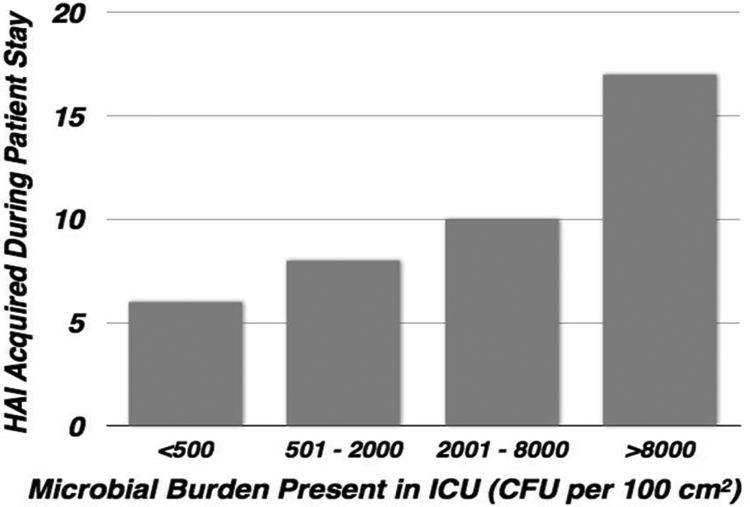
Distribution of healthcare-associated infection versus microbial burden measured in the intensive care unit rooms during the patient stay (Salgado et al., 2013).
Clinical Trial: Time Needed to Recoup the Cost of Antimicrobial Copper Components
Upon normalizing the results due to the slight difference in the number of patients in copper and noncopper rooms, the number of infections in the control rooms is reduced from 26 to 24:

Since the normalized number of infections in the noncopper rooms is 24 and the number in the copper rooms is 10, then 24 – 10 or 14 infections were prevented by use of copper components.
In order to estimate the time to recoup the cost of installing antimicrobial copper components in this particular study, several factors need to be considered:
The average annual direct cost to treat a hospital acquired infection, according to the Centers for Disease and Prevention (Scott, 2009) is US$28,400 to US$33,800. The number of infections prevented by installing copper components, which is = 14. The number of days over which the 14 infections were prevented, which was 338 days.
The extra cost of copper components over the cost of standard components, for fabrication and installation the copper components in all the rooms, which was US$52,000.
Assuming that the cost to treat is at the low end, US$28,400, the time to recoup the extra cost can be calculated as shown below:
Using the same calculation methods as shown above but assuming that the cost to treat is at the high end, US$33,800, the time to recoup the extra cost is 37.1 days. Thus, the time to recover the cost of the copper installation is 37–44 days, or less than 2 months.
Clinical Trial Limitations
To the best of our knowledge, this was the first study of its kind that demonstrated that the deployment of an active environmental surface could improve patient outcomes. Additional studies are needed to determine whether reduction in bacterial burden is a key factor in reducing HAIs. The study was designed as an intent-to-treat randomized control trial. Blinding healthcare workers is impractical because of the unique appearance of copper alloys. However, the copper objects were in place for 9 months prior to the collection of clinical data related to infection status, and the ICU staff was not told that the study had commenced. The collection of samples from surfaces continued during this period. Thus, the ICU staff and others had no indication that the last phase of the trial, related to HAIs, had started. For additional information, it is suggested that the original paper be consulted (Salgado et al., 2013).
Taken collectively, these studies clearly make a strong argument for incorporating this durable material into infection control practices in hospitals.
Conclusion
There is a considerable body of published research demonstrating the antimicrobial properties of copper alloys. Each study presents a case for the use of copper alloy surfaces to control human pathogens. Taken collectively, these studies clearly make a strong argument for incorporating this durable material into infection control practices in hospitals. Publication of the study demonstrating that copper surfaces control the acquisition of HAIs and represents the first instance in which a continuously active antimicrobial material is shown to significantly reduce the rate at which infections are contracted by hospitalized patients. In addition, it is the first illustration of the correlation of microbial burden with infection rates where an increased microbial burden leads to more infections. Incorporation of copper into essential items within the built environment of hospitals offers the potential for a unique passive solution to control and limit HAIs in an
Incorporation of copper into essential items within the built environment of hospitals offers the potential for a unique passive solution to control and limit HAIs in an efficient and cost-effective manner, without the need for training personnel or other human intervention.
efficient and cost-effective manner, without the need for training personnel or other human intervention. Registration with the U.S. EPA has stimulated the supply channels to manufacture components that they can now legally market with public health claims. Thus, components are now commercially available, which was not the situation when the above clinical trial was conducted. Given the extensive body of laboratory evidence, and promising clinical trial results, copper alloys should be deployed in applications where their inherent antimicrobial property can potentially benefit human health by reducing HAIs and treatment costs and hopefully even saving lives. This article may be viewed as an example of translational science, which is intended to “carry science from the bench to the bedside.” It started with a review of in vitro laboratory experiments, or bench science, moved through legally required regulatory testing needed before products can be marketed, and into a the clinical trial, which provided a real-world proof of the concept. The results of the clinical trial provided the stimulus for manufacturers to develop product, so that hospitals can now obtain commercial products in their facilities, which they are beginning to deploy.
Given the extensive body of laboratory evidence, and promising clinical trial results, copper alloys should be deployed in applications where their inherent antimicrobial property can potentially benefit human health by reducing HAIs and treatment costs and hopefully even saving lives.
Implications for Practice
An increase in microbial burden favors an increase in infection rates. Antimicrobial copper has been shown to reduce microbial burden. Reducing microbial burden has resulted in a concomitant mitigation in the rates of HAIs in rooms fitted with copper components as frequently touched surfaces. Components incorporating antimicrobial copper are now commercially available. Once antimicrobial copper components are installed, neither human intervention nor behavior changes are required for copper alloys to continuously reduce microbial burden (however, copper alloy surfaces, like any other surface, should be routinely cleaned). Incorporating antimicrobial copper into frequently touched components in the built environment offers a unique solution to reduce HAIs, save lives, and reduce costs. The additional cost for the copper components for the trial was recovered in less than 2 months.
Footnotes
Acknowledgment
We would like to acknowledge all our colleagues who have participated in the many studies discussed in the article, but space does not permit me to name all of them. However, we would be remiss if we did not name just a few, Peter Sharpe of Irwin P. Sharpe & Associates; Adam Estelle, Wilton Moran, James Michel, Andy Kireta Jr., and Andy Kireta Sr. of the Copper Development Association Inc.; Sandra Wilks, Jonathan Noyce, Louise Weaver, and Sarah Warnes of the University of Southampton; and Dennis Simon, Kathy Zolman, and Chuck Stark of the South Carolina Research Authority.
Authors’ Note
Any public health claim must be consistent with the submitted efficacy data and approved by the Antimicrobial Division of the EPA. This article includes some conclusions that do not necessarily reflect EPA approved product registrations. This includes reference to organisms that have not been evaluated against copper alloys under EPA-approved testing protocols. Any stated or implied effectiveness in controlling disease or reducing infections in humans have not been approved by either the EPA or the U.S. Food and Drug Administration (FDA). Copper alloys have been shown to reduce microbial contamination and to kill the following six EPA registered bacteria that are known to cause infections (S. aureus, MRSA, VRE, E. coli O157: H7, P. aeruginosa, E. aerogenes) and are covered by EPA Registration Numbers 82012-1 through 82012-6. The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as an official Department of the Army position or policy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the EPA regulatory testing was provided by both the International Copper Association Ltd. (ICA) and Copper Development Association Inc. (CDA). In addition, both of these organizations provided funding for laboratory research for two of the authors, H. T. Michels and C. W. Keevil. The U.S. Department of Defense funded clinical trials and were supported by the U.S. Army Medical Research and Materiel Command under Contract No. W81XWH-07-C-0053.