
Abstract
Research on stigma management techniques often emphasizes reducing and challenging negative associations with stigmatization. How do people manage stigma in social groups where negative associations may be socially or professionally advantageous? We answer this question with a case study of the emerging industry of “Recovery Coaching,” where firsthand experiences with drug use and recovery are part of a credentialing system that offers entry into a professional field. Drawing on interviews with 22 participants, 15 of whom were certified recovery coaches, we demonstrate the presence of a unique stigma management technique: the professionalization of stigma. Recovery coaches explicitly leverage revealing stigmatized associations to establish and justify their membership in a professional group. We distinguish the professionalization of stigma from conventional management techniques that reduce stigma and discuss the implications of this concept for the study of destigmatization under neoliberal social and economic conditions across different subfields of sociological research.
Introduction
Sociologists working on a wide range of problems are concerned with stigma—“the mark, condition, or status that is subject to devaluation” and “the social process by which the mark affects the lives of all those touched by it” (Goffman 1963; Pescosolido and Martin 2015:91). Stigma limits collective action because social devaluation limits access to the redress and resources that might solve problems (Link and Phelan 2001), keeps people from seeking help (Henderson, Evans-Lacko, and Thornicroft 2013) and reduces the general will to offer help to others (e.g. Mohr 1994; Steensland 2006). As a result, sociologists have called for renewed attention to destigmatization—the “process by which low-status groups gain recognition and worth” (Lamont 2018).
Most strategies for stigma management involve reducing stigma by recontextualizing social interactions so that people or groups experience less stigma. Management techniques such as denial, confrontation, demonstrations of self-worth, integration into social groups, and self-isolation facilitate this process (Goffman 1963; Lamont et al. 2016). We address a research question that runs counter to these trends: how do people manage stigma in social groups where negative associations may be socially or professionally advantageous? This is an important question because inequality and marginalization in the contemporary era is accompanied by an economic transformation toward neoliberalism that increasingly encourages people to leverage identities and relationships in novel ways to generate capital (Brown 2006; Stewart and Hartmann 2020). In this climate, efforts toward destigmatization could be challenged by social structures in which managing stigma might also include leveraging stigma to a new degree and in new ways than previously theorized.
Our study has identified a different strategy of stigma management, one where actors leverage stigmatized identities to facilitate building economic and social capital. We call this strategy the “professionalization of stigma.” The professionalization of stigma occurs when people emphasize a stigmatized identity to (1) claim unique insight into the lifeworld of a stigmatized group and (2) use that claim to establish social capital that is valuable to a specific institutional or professional environment. The goal of this technique is not to reduce or to eliminate stigma, per se, but rather to claim its negative effects and turn them into credentials. Our goal is not to say that this is the only or the dominant technique of stigma management, but rather to name it as an additional management technique among others and to draw out its implications for sociological theory, professional practice, and empirical studies that examine the experiences of stigmatized social groups.
Our evidence for the professionalization of stigma comes from interviews conducted during a case study on long-term recovery with individuals who self-identified as being in recovery from a substance use disorder. During this research we identified the presence of the emergent professional field known as “Recovery Coaching.” A Recovery Coach is a “non-clinical person who helps remove personal and environmental obstacles to recovery, links the newly recovering person to the recovery community, and serves as a personal guide and mentor” (White 2002). In the face of the opioid crisis (Foglia, Kline, and Cooperman 2021) a new collection of organizations has emerged as part of a new field of Recovery Coaching in the United States. Recovery Coaches use their own lived experience of recovery from drugs or alcohol to help others navigate substance use treatment care across a variety of different institutions (Byrne et al. 2020; Hansen et al. 2022; Magidson et al. 2021). This requires them to accept and leverage their own experiences of stigmatization for both personal and professional purposes. The field of Recovery Coaching presents a set of professionalized credentials, namely, the certified addiction recovery coach (CARC) certificate, which provides training and social skills that position Recovery Coaches to help people who use drugs (PWUD) navigate substance use treatment, harm reduction, and/or recovery opportunities (Recovery Coaches International 2022).
Our research demonstrates the professionalization of stigma in action by documenting how Recovery Coaches discuss their stigmatized identities. Not everyone in this study exhibited the professionalization of stigma, but the comparison between those who did and those who exhibited other management techniques is particularly useful for documenting and defining this concept. In what follows, we define this concept in detail and situate it in conversation with previous research on stigma management techniques. We then provide background context for the study of Recovery Coaching and discuss the interview and analysis methodology. Our results provide three findings that are central to distinguishing the professionalization of stigma. First, some Recovery Coaches also used other stigma reduction techniques well-known in sociology, but those techniques often come with a focus on recovery itself, rather than professionalized Recovery Coaching. Second, Coaches employing the professionalization of stigma technique are aware of their position in the social field and use stigma as a professional credential in that field. Finally, Coaches using this technique understand stigmatized experiences as an asset, rather than a deficit. This evidence gives us good reason to distinguish the professionalization of stigma from other stigma management techniques. We close by discussing the implications of this distinction not only for the continued study of Recovery Coaching but also for sociological research in other areas.
Background
Theory—The Professionalization of Stigma
Research has identified many different approaches to managing stigma (Goffman 1986; Link and Phelan 2001; Pescosolido and Martin 2015) that fall into two broad categories. Techniques for concealing stigma, including passing and other forms of concealment, generally involve presenting oneself as a non-stigmatized individual by dissociating the self from stigmatized social categories. Techniques for revealing stigma, in contrast, disclose stigmatized identities to carry out impression management and exercise control in one’s social relationships.
The practice of these two categories of stigma management varies across different social situations and different local and global contexts. In a major synthesis of these techniques focused on racialized stigma and racism, Lamont et al. (2016:10) note five management techniques that respondents recount: confrontation, management of the self, not responding, focusing on hard work and demonstrating competence, and self-isolation. Importantly, their cross-national study emphasizes that cultivating positive evaluations, such as demonstrating a strong work ethic and competence, is a “less common form of response across sites” (p. 11), whereas confrontation, concealment, and management of negative evaluations are more common. Most of these techniques for revealing stigma involve some degree of hiding, mitigation, denial, argument, or correction, such that stigmatized individuals work to normalize their status, challenge negative associations with that status, or differentiate themselves from others with that status. What each of these techniques have in common is that they, in whole or in part, attempt to attenuate a negative association with a particular status. This would place the majority of stigma management techniques in the broader category of work that conceals stigma, rather than revealing it (see Figure 1).
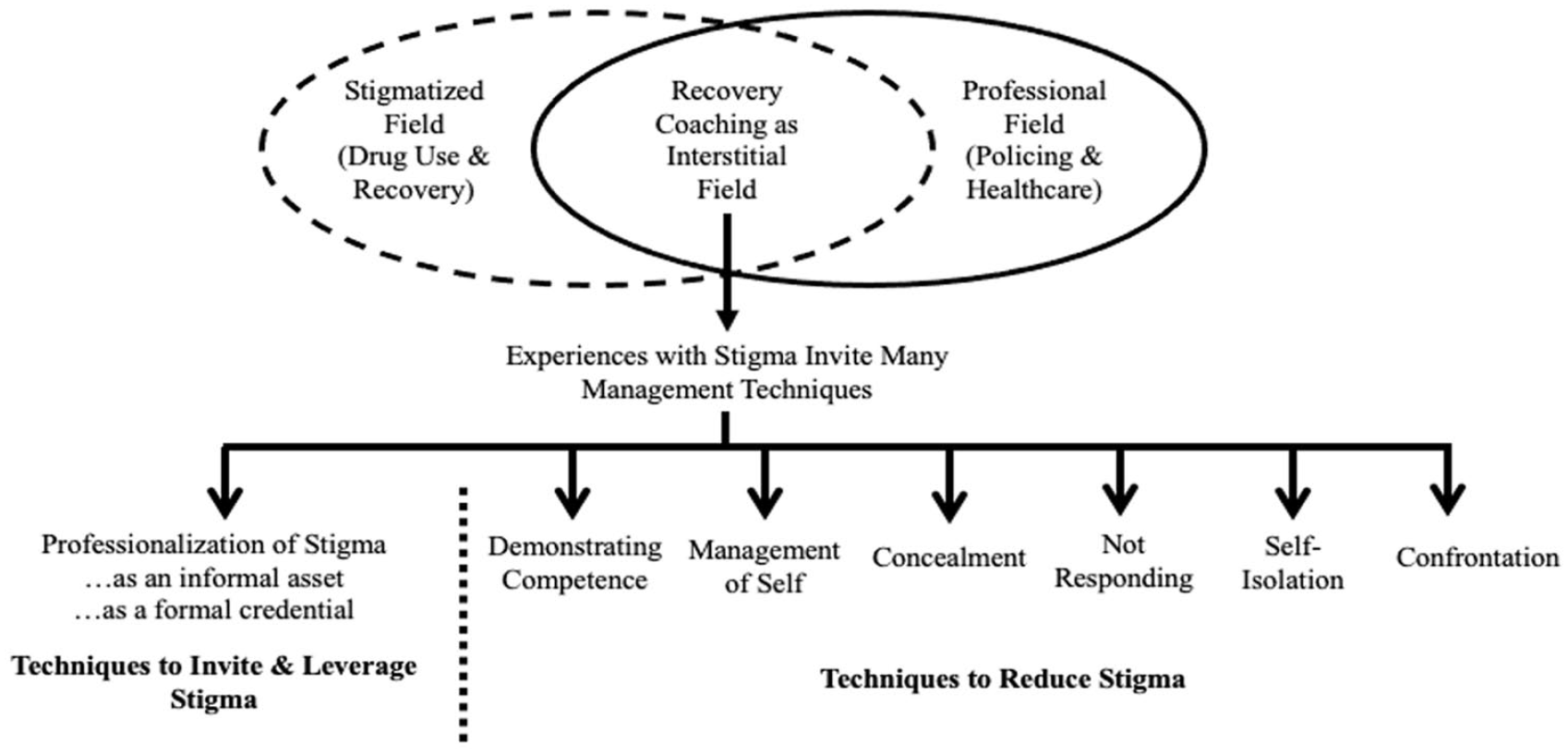
Recovery Coaching Stigma Management Techinques.
In contrast to dominant approaches to minimizing stigma by reducing negative associations, we argue that the professionalization of stigma belongs to the less common class of techniques that reveal stigma to leverage attention toward negative associations with a stigmatized identity. This management technique has two key parts. First, a person reveals a stigmatized identity to others, rather than attempting to minimize or distance themselves from that identity. A key part of this revelation is the claim that a stigmatized identity indicates a person has unique insights into the lifeworld of the stigmatized group. Second, a person claims that those insights provide qualifications and social capital that they can leverage in particular professional environments related to the stigmatized group. The goal of this new technique of stigma management is not necessarily to reduce or to eliminate stigma, nor is it simply to demonstrate competence, but rather to leverage prior negative associations by encouraging others to understand those negative associations as an asset and a credential.
People may leverage stigma into informal assets such as insight into the nature of a job or unique access to social capital from a particular group. For example, if a person involved with the criminal justice system is re-entering the workforce after a period of incarceration, they may engage in a variety of stigma management techniques while interacting with potential employers (Vuolo, Schneider, and LaPlant 2022), including avoiding anticipatory stigma by opting out of specific job applications, demonstrating reform to minimize stigma, or strategically applying only to specific positions. In our theory, a hypothetical person strategically engaging what Vuolo et al. (2022:577) call “targeted applying” could also make the claim that their experience with stigma through incarceration gives them unique insight into the requirements of the job and thus provides a unique set of qualifications for that job. If they make this argument, we claim they are engaging in the professionalization of stigma.
This example demonstrates how the professionalization of stigma is different from existing concepts in the field, such as professionalized stigma management (Dobransky 2019). In professionalized stigma management, people in professional roles—such as counselors, social workers, and clinicians— provide formalized frameworks to help members of stigmatized groups engage in stigma management techniques. Erving Goffman’s original treatment of the topic (1963:108) called this “professional presentations”—“a desirable pattern of revealing and concealing” stigma with guidance from others to disclose in a proper, socially normative way. Professionalized stigma management provides new ways for clients to address stigma, including minimization. In contrast, the professionalization of stigma does not seek to minimize stigma, but rather to leverage it in order to access that professionalized status itself.
The professionalization of stigma is also different from the demonstration of competence as stigma management technique, especially in the way that some people try to “establish their equality through competence” (Lamont 2018:97). The professionalization of stigma is not a technique to claim equal status to non-stigmatized groups through hard work, but rather a technique to claim unique status in a professional role setting by drawing attention to stigma. The professionalization of stigma is a unique cultural repertoire for stigma management (Lamont and Thevenot 2000; Swidler 1986; Lamont 2018) that involves particular ready-made scripts (Lamont et al. 2016) created by institutions that carry particular assumptions about identity, work, cultural membership, and professional qualifications. What makes the professionalization of stigma unique, in our view, is that current late-modern social conditions have exacerbated Goffman’s “professional presentation” to an extent that now merits additional, renewed consideration from sociologists to map new forms of revealing stigma alone.
We have good reason to expect that the professionalization of stigma is uniquely salient in late modernity for two reasons. First, it is particularly useful in interstitial social fields—emerging sets of institutional and social relationships that operate between established social fields where actors can gain benefits from innovative combinations of social capital drawn from those established fields (Fligstein and McAdam 2012; Medvetz 2012). For example, the case of Recovery Coaching that we discuss below operates between the stigmatized field of drug use and recovery and the professionalized world of substance use treatment (see Figure 1). As we will show, this provides unique opportunities and incentives to manage stigma.
Second, the impulse to leverage stigma as a resource is elevated under economic conditions that incentivize maximizing every facet of one’s potential social capital. Neoliberal capitalism encourages economic thinking in every facet of social life (Brown 2006; Stewart and Hartmann 2020), and this provides a motive to begin thinking about the potential revelation of a stigmatized identity to provide entre into new forms of competitive advantage. For example, one might consider cases where institutions and markets incentivize the disclosure of stigma (and, in some cases, trauma) such as formal application essays to scholarships or prestigious schools. In such cases, disclosure is incentivized to provide a unique and compelling story and access social capital or commercial success. Under these conditions, we may expect to see emergent behaviors in which people attempt to leverage their stigma in novel ways, as we do in the following case study.
The Case of Recovery Coaching
Research has continuously documented that PWUD belongs to stigmatized social categories (Biernacki 1986; Goffman 1963; Granfield and Cloud 1996; Kellogg 1993; Livingston et al. 2012; McIntosh and McKeganey 2000). In most cases, people who share their challenges with substance use and/or subsequent recovery often report engaging in different techniques of stigma management to mitigate the negative perceptions of their identity (DeLucia et al. 2015; Dingle et al. 2015; McNamara and Parsons 2016; Shinebourne and Smith 2009). Often, these techniques are derived from participation in recovery-based groups including self-help groups (e.g., Alcoholics Anonymous), faith-based organizations, cognitive-based therapy (CBT) approaches, and other community-based organizations that aim at providing tools for coping with and transforming stigmatized identities (Dingle et al. 2015; McNamara and Parsons 2016; Stansfield 2018). These pathways often encourage individuals to accept—rather than deny— their stigmatized identity as a means to facilitate their recovery by identifying with a community of people that share that stigmatized identity.
In this study, we focus on an emerging professional field situated at the intersection of public health and safety: Recovery Coaching. Over the last 20 years, peer-to-peer support systems have begun to capitalize on the lived experiences of those who have found recovery themselves and are now positioned to help engage others in treatment and navigate recovery resources (Killeen 2013; Mendoza et al. 2016). The ideal Recovery Coach is a person in recovery themselves who can share their experiences with overcoming addiction and navigating the recovery system through processes such as detox, housing support, harm reduction, and other recovery-oriented activities.
The process of recruiting Recovery Coaches and placing them in organizations is not a simple matter of implementing voluntary service. Instead, an emerging field of organizations is professionalizing Recovery Coaching with formal training and certification processes. In 2008, at least 30 states had formally developed criteria and training programs that aim at supporting the profession of Recovery Coaching and peer-support specialists (Killeen 2013). Since the advent of formal Recovery Coaching in 2008 with the founding of the Recovery Coach Academy (RCA) by the Connecticut Community for Addiction Recovery (CCAR), Coaches increasingly receive specialized training on the field’s best practices. The RCA is a 5-day intensive training program that is aimed at providing Recovery Coaches with the knowledge, tools, and resources needed to become effective Coach (CCAR Training 2022).
Throughout their training, recovery coaches learn how to meet clients’ unique needs to best support PWUD in navigating the complexities of substance use treatment and recovery. This means that Recovery Coaches need to have a comprehensive understanding of different approaches to recovery to help their clients develop personalized methods for sustaining sobriety (Recovery Coaches International 2022). The formal certification process also includes training that encourages Coaches to integrate their lived experience into their professional practice of coaching. In this case, the formal credential itself is an indicator that the Coach has sufficiently enacted the professionalization of stigma in the context of the training program. Certification and training are now commonly used as prerequisites for Recovery Coaching roles. These credentials aim to legitimize the field of Recovery Coaching, by providing agreed upon coaching methodologies that focus on navigating recovery and substance use treatment resources.
The professionalization of Recovery Coaching stems from specific incentives in the larger field of substance use and recovery organizations. Today, Coaches are embedded within many kinds of institutions, including police departments, community health centers, substance use treatment facilities, and hospital emergency departments. These institutions require Coaches to draw on their personal experiences with recovery while also being mindful of bureaucratic expectations that are not always empathetic to the experiences of people in recovery. Because of the stigma attached to drug use, these institutions often create conditions in which those in recovery lack the appropriate forms of social capital to succeed in other conventional master’s level social work or clinical roles. In turn, recovery coaching provides a platform to use what Connolly and Granfield (2017) refer to as “recovery capital”—the resources that one may access to help maintain recovery such as social networks, employment, or religious support—as an essential component for the formalization of the industry. It can also provide an alternative pathway to enter the criminal justice or healthcare fields and access professional roles within those fields without other conventional means of certification through social work or clinical experience. Working as a Recovery Coach can provide opportunities for advancement into senior management roles that are often inaccessible within the broader context of substance use treatment.
Therefore, Recovery Coaching sits between the stigmatized world of drug use and recovery and the professionalized world of criminal justice, public health, and healthcare institutions. It relies on the lived peer-to-peer experience of people in recovery, including the stigma that comes with that recovery, but it also requires a high degree of stigma management to build and maintain professional relationships and credentials within formal institutional systems. In our analysis below, we assert that the professionalization of stigma is a unique management technique that people with extensive experience in Coaching employ to navigate this environment.
This case leads us to three research expectations. First, we expect to observe the professionalization of stigma, in which Coaches (a) reveal stigma and then (b) leverage that stigma as grounds for a professional status as a Recovery Coach. Second, we expect that we will be able to distinguish this technique of stigma management from others defined in previous literature. Third, we expect that one core explanation for these distinctions is the degree of exposure to and integration with professional training in Recovery Coaching programs. We expect to see the professionalization of stigma more often and more prominently among respondents who have more experience as Recovery Coaches, and we expect to see other stigma management techniques more prominently among newer Coaches or those with less established professional identities in the field.
Methods
Sampling
This current study was part of a larger project interviewing people who self-identified as being in long-term recovery from a self-defined substance use disorder. Participants were initially identified for this study through a non-profit organization that we call Addiction Recovery Coach Services (ARCS) that served to reinforce and develop public health and public safety partnerships by embedding Recovery Coaches into police departments and other community-based organizations. Subsequently, participants were recruited for interviews through their affiliation with ARCS and additional interviews were leveraged through participants’ social networks through snowball sampling. To be eligible for the study, participants had to meet the following criteria: (1). English speaking, (2). Age 18 or older; and (3). Self-identified as being in recovery for one year or longer.
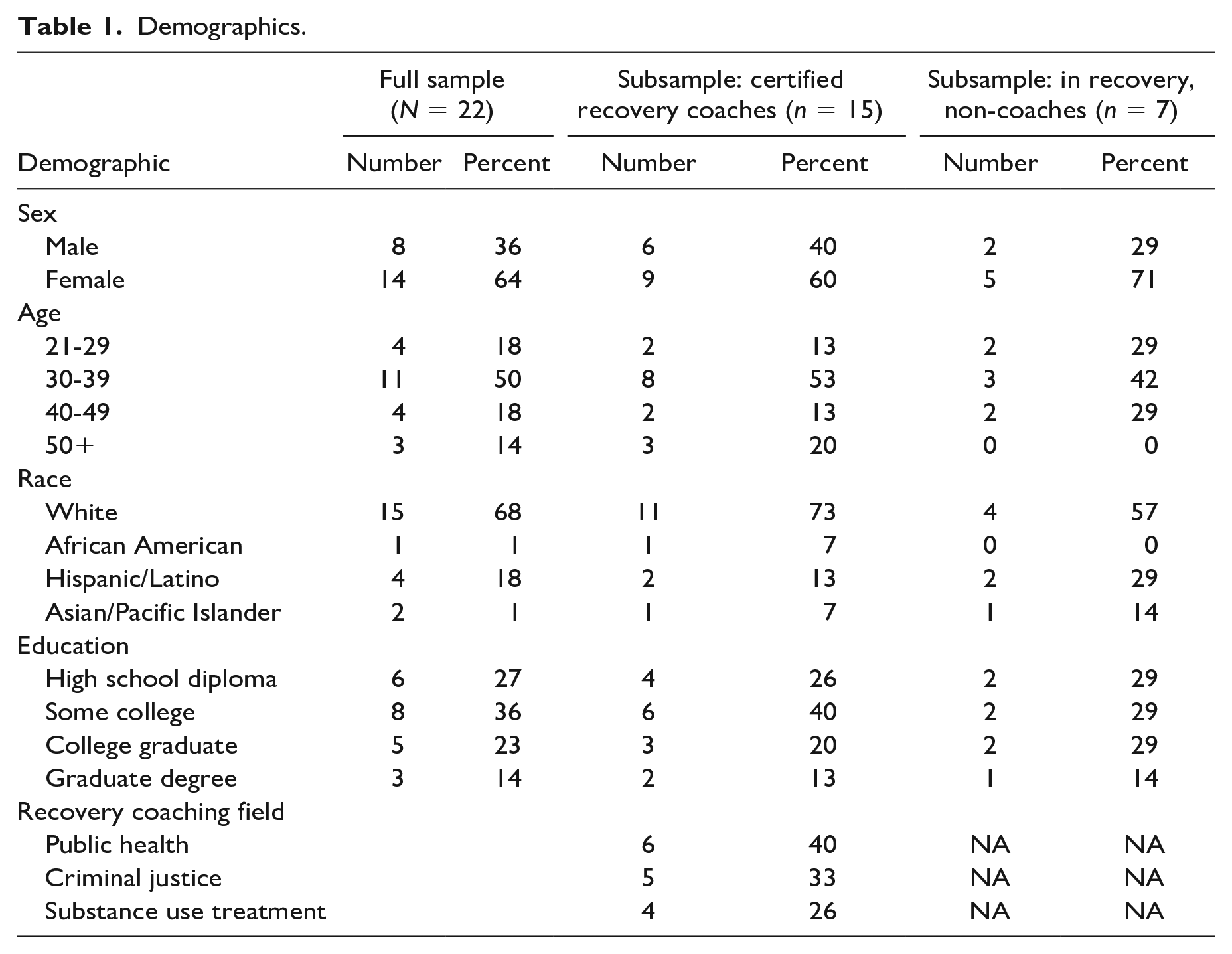
In total, 22 participants participated in interviews, 15 of 22 participants identified as Recovery Coaches, and the remaining seven participants belonged to more traditional recovery-based groups (e.g., Alcoholics or Narcotics Anonymous). The participants who acknowledged their professional experience working as a Recovery Coach also reported being trained and certified as a CARC. Table 1 details the demographic characteristics of our sample, including a comparison between certified Recovery Coaches and respondents who were not Coaches. Our sample has more male-identified Recovery Coaches (40%) than non-Coaches (29%), and Recovery Coaches tend to be older and more predominately white (73%) than non-Coaches (57%). We obtained a balanced sample of Recovery Coaches working across three institutional sites in the fields of public health (40%), criminal justice (33%), and substance use treatment (26%). Although this is a small sample of Recovery Coaches, these demographics provide a snapshot that can help to contextualize the demographics of people who are likely to be selected for these roles.
Demographics.
Interviews
Interviews were audio-recorded, transcribed, and deidentified by a professional transcription service. The collection of interviews (by Author 1) varied in length from about 30-45 minutes and were conducted in-person or over the phone. Interviews focused on topics such as history of substance use, the recovery process, stigma management techniques, and self-expressed definitions of long-term recovery. The sub-sample of interviewees were selected for this analysis because each of these individuals had shared their professional experience as a Recovery Coach either in public health or public safety setting.
Researchers (Authors 1 and 2) examined the subset of interviews to identify and understand accounts of stigma management techniques among participants who shared professional experiences of Recovery Coaching. An initial set of themes was identified independently by (Author 1) after a reviewal of transcripts using open-coding and a priori knowledge of the field. Interviews were then coded independently by (Author 2), and then refined in dialogue between both authors to produce a set of thematic codes and codebook. Researchers imported the codebook into NVivo version 12 (QSR International, Melbourne, Australia) for analysis. The study protocol was approved by the Institutional Review Board at the University of Massachusetts Boston.
Results
Interviews with Recovery Coaches and those in recovery who were not working as Recovery Coaches in this study revealed three important themes. First, respondents who were less experienced with Recovery Coaching handled stigma management differently, showing us how the professionalization of stigma is a novel alternative to other conventional stigma management techniques that treat Recovery Coaching as recovery as opposed to a profession. Second, participants grappled with the challenges of working between two different social fields—a stigmatized field of being in recovery and a professionalized field of formal recovery institutions—which created many experiences with stigma and opportunities to use stigma management techniques. One novel response to this environment was to creatively manage stigma by using that stigma as a credential. Third, participants who used the professionalization of stigma in the face of this challenge discussed leveraging stigmatized roles and experiences for their professional qualifications – treating these stigmatized roles and experiences as assets, not deficits.
Conventional Routes to Stigma Management
First, it is helpful to establish a baseline by outlining our observations of conventional stigma management techniques. In our sample, not every Recovery Coach exhibited the professionalization of stigma. Some Coaches, and some people who were in recovery but not actively coaching, exhibited more well-known stigma management techniques in the sociological literature that aimed to reduce stigma rather than leverage it. This is most evident in the way some Coaches avoided using terms like “addict” or “junkie.” Others attempted to challenge preconceived notions about addiction. However, they were well aware of the influence of stigmatizing language, and took steps to challenge and minimize that stigma.
I mean, I hear it all the time with Cops, and they don’t realize I can overhear them when they’re like, “Oh this recovering addict.” At the HUB [Community Policing Organization] this week, “This recovering addict said to me that it’s all about insurance.” What do you mean this recovering addict? This is a person, not a recovering addict. It should just be this person. Why is it a recovering addict said this to you? I’m pointing this out to you, and this is so eye-opening. Recovering addict that told you that insurance runs recovery. But I mean, I don’t take offense to certain terms, but I’m cautious of using them.—Christy,
1
37 White Woman
Another participant shared similar challenges in defining herself through her addiction and her feelings about the pervasive stigma she experiences.
I got sober through AA, identified as an alcoholic and an addict. I think through this work [Recovery Coaching] and learning about stigma and stigmatizing words, at this point it kind of makes me cringe. Whereas before I didn’t because I have learned it to be a negative or demeaning word. I don’t ever use it anymore. I just discussed this with other people who still do participate in AA and still, do identify as that (Addict). I mean, my addiction doesn’t define me. Whereas other people might not agree. Like that’s who they are. That’s fair.—Veronica, 29 White Woman
Contrasting these statements highlights two important points: Recovery Coaches could choose from many stigma management techniques, but those who did not choose professionalization tended to conceptualize Recovery Coaching primarily as recovery, rather than a profession. Consider Christy again, who recounted avoiding certain professional opportunities for purposes of stigma concealment: I’m pretty honest about it now. I work in the field [Recovery Coaching]. I didn’t go back to be a medical assistant because I didn’t want to feel like I couldn’t tell the doctor that I was working for that I was in recovery again. . .That’s just my opinion. It doesn’t necessarily mean medical assistants around the world shouldn’t be in recovery. It’s just for me it was too hard to come clean with the truth. For me at the end, working in recovery helps me stay in recovery because I see what I was, and I don’t want to go back to that. I don’t want to be that. It helps me working in the field.—Christy, 37 White Woman
Or, consider May, who became more careful about stigma disclosure and concealment over time. May was less concerned about employers perceiving stigma because of legal protections against discrimination. But May also reinforced a clear boundary between personal disclosures and professional disclosures, where other Coaches invoking the professionalization of stigma would be more likely to blend the two: I don’t tell the nanny families that I work for [that I’m in recovery] . . .that’s different then an employer, an employer can’t stigmatize you it’s illegal. But nanny families can be like “oh you’re in recovery, from what?” There’re no laws against that. But when my mom tells her friends at the bar that I am in recovery, I think it’s an honor and it shows people that it’s possible. I might have told people for attention when I was in early recovery, it made me feel cool because I am chasing self-esteem but now, I think I’m more mindful when I share that information.—May, 37 White Woman
In supplementary analysis, we also reviewed the other seven interviews with respondents who self-identified as being in long-term recovery, but were not employed or certified as Recovery Coaches. Many of these respondents also discussed specific experiences with stigma and stigma management techniques such as concealing or not responding to stigmatization. This was especially prevalent with respect to the stigma associated with taking medications for opioid use disorder (MOUD) such as methadone, suboxone or vivitrol. For instance, one participant discussed her experiences in navigating the stigma of receiving MOUD treatment at a treatment clinic. She stated: “There was one place [Substance Use Treatment Clinic] I would go to and I hated going there because pulling in and like seeing the people out in the parking lot, you just kind of put your head down and just walk past them. . .They [Clinical Staff] have to watch you pee and it's definitely very different from being told you have to go there versus being like oh I wanted some help. . .So, I went into the vivitrol doctor and I saw her and she made me give her the rest of my suboxone because you have to be off of suboxone for two weeks before you get the [vivitrol] shot. So, I knew I would be seeing her every other day so she could do a urine screen on me. There was no backing out at that point.” —Kerry, 29 White Female
Similar to some sentiments from Recovery Coaches, participants in the comparison group continued to challenge the labels typically associated with recovery. Some participants discussed distancing themselves from recovery terminology or abolished labels all together. One participant shared: “I don’t think the term addict is a right word to call them [people in recovery], you know? So, anybody in recovery, even the word “in recovery,” I don’t think they’re even should be a word. I don’t think we should be identifying people like myself as someone in recovery you know? Let’s say your friend had cancer, would you constantly say he’s in remission? No. It would just be like, “Oh my buddy, he had cancer.” He doesn’t have it anymore. Its not brought up.”– Ben, 29 White Male
None of the respondents in this comparison group expressed the professionalization of stigma but instead exhibited traditional stigma management techniques such as concealment, self-isolation or confrontation. This comparison raises an important piece of preliminary evidence that experience in the field of Recovery Coaching facilitates the learning of professionalization as a specific and unique stigma management technique.
Stigma as Credential
The integration of Recovery Coaches into daily professional workflow has required public health providers and public safety partners to rely heavily on the lived experiences of Coaches who have successfully found recovery and chosen to receive training to work in the field (e.g., CLEAR Program 2022; Essex County Outreach 2022; Perrone, Malm, and Magana 2020). People working as Recovery Coaches have to carefully navigate a broad range of social contexts, and they discussed these experiences with novel approaches to stigma management. Recovery Coaches learn to both embrace and mitigate the stigma associated with their history of substance use in the course of their career.
Recovery Coaches recognize both continuity and change as they take on the coaching role. They observe taking their own lived experiences into the role, but also mark the distinctions between personal experience and the professional role. One respondent observed: I’m always helping people, but I’d never gotten paid for it.
2
Now I’m getting paid for it [Recovery Coaching]. I mean, it’s not a salary that I’m accustomed to, but it, you know, so I sort of feel like I’m cheating on my recovery in the beginning, now work to that. But the God that I believe in put me here to do this specifically for that purpose.—Ken, 32 Asian Male
It is important here to observe that the respondent’s idea of recovery was initially troubled by the transition to Recovery Coaching (“I sort of feel like I’m cheating on my recovery”), but also that they now contextualize their experience both as paid work and as a vocation they have “always” done in accordance with a divine purpose. The use of vocational framing here provides a way to integrate the Coach’s labor with their identity and sense of self in conventional terms in accordance with Weber’s classic Protestant Ethic (Weber in Kalberg 2009).
In the course of their jobs, Recovery Coaches reported that the visibility of stigma was crucial in helping to advocate for PWUD and those in recovery within criminal justice and healthcare institutions. Recovery Coaches were well aware of stigma in their field and often spoke about it explicitly. They also observed a key difficulty in getting police and healthcare providers to recognize the challenges behind achieving sustainable long-term recovery. In doing so, they implicitly recognize the challenge posed by conventional stigma management techniques that reduce or eliminate stigma—by eliminating stigma, they also eliminate the legibility of struggle to others: I’ve seen so many different ways [of achieving recovery]. Actually, the first one that opened my eyes to it was, I was in the RCA [Recovery Coach Academy] training with this girl. She was an awesome girl, very successful girl. She led a program for pregnant mothers that were addicted who were about to give birth, and then she was getting them on methadone. You always have that negative stigma to MAT [Medicated Assisted Treatment] and everything . . . Oh, church can only keep you but so much sober, you still need AA and all that type of stuff. Towards the end of the week, she revealed to me that she was on methadone herself. I was just mind blown. I was like, “Wait, what?” Because you think methadone. . .I think of the millions of kids that I sold dope to that were on methadone and suboxone, the same thing, the kids that would sell their suboxones. I didn’t know all the success stories. The reason we don’t hear the success stories is because they are successful and you don’t see them anymore, you know what I mean.—Ken, 32 Asian Male
The visibility of stigma presented a “double bind” for Recovery Coaches. On the one hand, they want to help their clients manage stigma and reduce stigmatizing behavior from authorities. On the other hand, a key strategy Coaches use to get professional recognition from authorities requires successfully making recovery cases visible by re-introducing their own experiences of stigma. In this case, a dominant strategy among Recovery Coaches was to take on stigmatized roles in order to make such recovery visible and invoke empathy. For example, one Recovery Coach disclosed their personal experiences with Narcan—an opioid antagonist medication that reverses the effects of an overdose: Until they [Police Officers] learn differently, I don’t know how they’re going to accept or lose their stigma. When I worked at the police department, I would hear crazy things from certain officers. They did not realize. There were some officers that thought we should just not be giving NARCAN because it was enabling. I spoke to them about how I was NARCANed. I overdosed many times. They could not picture that. They were like, “You overdosed?” I’m like, “Yes. What do you think I’m doing here? Why do you think I’m a Recovery Coach? You think I just wanted to be a Recovery Coach one day? No, I was a drug addict. They don’t always picture people that have gotten better as addicts anymore.—Dave, 42 White Male
Notice here that this Recovery Coach discusses both accepting and losing stigma, and they imply that it might be possible or even preferable for a person in recovery to experience stigma in specific places and at specific times. The participant discloses their personal experiences of overdose and the application of the harm reduction tool Narcan to situate themselves in relation to people who are actively using drugs. Why might this be the case? Our respondents observed how stigma, revealed in certain cases and under specific conditions, could serve as a credential to establish the validity of their professional identity as a Recovery Coach, the legitimacy of their vocation in Recovery Coaching as a person in recovery, and the certification of a “successful” recovery in the eyes of authority figures. In this way, Recovery Coaches learn to frame their lived experience of addiction and recovery, and the stigma that accompanies it, as a conditional asset rather than an unconditional deficit.
Stigma as Asset, Not a Deficit
For Recovery Coaches, stigma can be an asset in two ways. First, it can help facilitate mutual understanding among PWUD or those in recovery and strengthen their own recovery experiences. In this sense, the field of Recovery Coaching leverages stigma to provide recovery capital (Connolly and Granfield 2017). Second, it can help to facilitate material relationships and social capital in the professional field. In both cases, Coaches discuss these assets as things that make them particularly good at their jobs, and they emphasize the role of formal training in cultivating their skill sets. For instance, Recovery Coaches learn to leverage their personal recovery network as recovery capital to connect with PWUD in professional settings. One participant stated: Being in the role, being a Recovery Coach or in the treatment field, it’s almost like an advocate for those people [PWUD]. So, it’s like having the right training knowing what is out there for services, having resources. Most of my networking and outreach was already kind of internal, prior to me getting into the field just because of knowing people in recovery. Because guess what? A lot of people that I consider to be in long-term recovery also work in the field. So, like, we all kind of continuously have kept up these relationships on a personal level that’s also helped in a professional setting. Crystal, 31, Mixed Race
The quote exemplifies the important role that lived experiences plays in positioning oneself to be a Recovery Coach. By relying on strong social ties this Recovery Coach has an existent network of recovery capital to connect her clients with when needed. This demonstrates that decisions to enter into or work in the field, are uniquely shaped by the experiences in overcoming past drug use.
Recovery Coaches also discussed the importance of the peer-to-peer process in order to position themselves as the most appropriate options to assist PWUD. A noteworthy part of the profession itself is the focus on one’s own recovery—being stable and successful in recovery to effectively fulfill the responsibilities as a Recovery Coach. This was indicated by several participants who shared that working on their own recovery, through their role as Recovery Coaches, was instrumental in maintaining both their personal connection with PWUD but also in legitimizing their unique qualifications as Recovery Coaches. For instance, one participant shared: Going through the Recovery Coach Academy [RCA], all of that stuff has really allowed me to like practice that open mindedness that I’ve been hearing about in 12-step but haven’t always seen. So, my message is very much also now has shifted towards this is my experience [of recovery] and if it’s useful for you, I’m happy to share it. But like what’s your experience? And like, let me learn from you, even if you are still struggling, like I can still learn from you. Um, and like there’s many options and not everyone’s going to have the same success with different options.—Amy, 30 White Woman
Another participant similarly stated: Using people’s lived experience as an asset, not a deficit. Allowing people, because we hear in AA [Alcoholics Anonymous] and NA [Narcotics Anonymous], the therapeutic value is helping one another. Allowing somebody with two or three years [in recovery], I feel just as long as they’re stable in their recovery, to help the next person come out of active addiction. I think everybody deserves a chance. My thing with recovery coaching is because you’re really getting in tune with somebody else. It’s different. There’s not that boundary like a desk in between you all. You’re really walking alongside somebody. I feel like with recovery coaches, they need to be on the healing side themselves, because they could just as well hear their story, and if they’re not healing from it, they could be triggered, and they could relapse.—Uma, 51 African American Woman
The quotes above illustrate some of the ways that Recovery Coaches can leverage their own experiences of recovery in order to help others. This is evident in this discussion by sharing that “there’s not that boundary,” which implies that the degree of social distance between PWUD and Recovery Coaches can be mitigated if Recovery Coaches are stable and confident in their own recovery. Though, this demonstrates that Recovery Coaches understand the stigmatized experiences of PWUD and because of this are well-positioned to provide their guidance. This in turn also allows Recovery Coaches to rely on their own experiences as professional assets and to extend themselves to others as “sober companions” to help guide others through the complexities of treatment and recovery (Killeen 2013). Scholars have noted the importance of these practices, particularly for individuals coming out of substance use treatment (White, Boyle, and Loveland 2003). What we also need to further consider is how Recovery Coaches view and leverage their stigmatized identity. Uma explained her perspective on sealing off her criminal record, she stated:
It’s just my opinion. They say at a certain time, you should seal your CORI (Criminal Offender Record Information), so when your CORI is run for a job, it’ll look like you never had a CORI. I feel that, this is just my feeling, and I hope it doesn’t come out wrong, I feel that people who seal their CORI are living a lie, because that’s part of your past. For me, I never wanted to seal my CORI, and I could’ve had my CORI sealed for the last five years. But I want to show this employer, yes, I’ve had a past. You know what I mean?—Uma, 51 African American Woman
Here, the Recovery Coach explains how sealing a CORI is a form of revealing one’s stigmatization to maintain authenticity and relatability as a Coach. These types of disclosures are viewed as a uniquely qualifying a person with lived experience to work in the professional field of Recovery Coaching as they embrace past experiences of stigmatization.
Discussion and Conclusion
As new social fields and professional organizations emerge, they do so under a logic of late modern capitalism that encourages people to leverage many unique aspects of their lives for economic gain and competitive advantage. This neoliberal economic logic (Brown 2006) intersects with other large-scale social changes in the United States. The opioid crisis means that more Americans are attempting to find recovery from their challenges with substance use (McCormick and Holleran Steiker 2021). At the same time, mass incarceration and the deinstitutionalization of mental health care create conditions where the new field of recovery organizations sits in an interstitial position between the stigmatized field of criminalized drug use and the professionalized field of criminal justice and healthcare organizations. These structural conditions have given rise to a unique professional field of Recovery Coaching.
These conditions motivated our research question: how do people manage stigma when there may be specific professional and economic advantages to leveraging that stigma? We used the field of Recovery Coaching as one empirical case study to address this question, and this case study has important implications for refining sociological theories of stigma management under late modern social and economic conditions. These previous theories emphasized social strategies that manage stigma primarily by reducing it, leaving cases where people intentionally draw attention to stigma underemphasized in the literature as rare cases. In contrast, our work identifies a potential novel stigma management technique: our interviews demonstrated that some people leverage stigma in order to access both formal credentials and informal assets as part of their professional status as a Recovery Coach, and we call the technique they use to do this the professionalization of stigma. In contrast to other stigma management techniques, this approach seeks to draw attention to stigma as a means to establish legitimacy, rather than minimizing it. It conceptualizes stigmatized experiences as an asset, rather than a deficit. Recovery Coaches also drew upon other techniques to reduce stigma that are well-known in the sociological literature, but, importantly, we found that those other approaches were more common when they were more focused on recovery itself, rather than Recovery Coaching as a job or a vocation.
This insight has several important implications for sociological theory and future research. First, in terms of our specific empirical case, this study establishes a first foray into the study of the emerging industry of Recovery Coaching as a way to understand the increasingly complicated intersections of multiple social fields in the United States: the criminal justice system, the healthcare system, and the economic system. Recovery Coaching is a novel industry built on the foundation of peer recovery specialist roles that sits in a unique interstitial field between these larger social fields (Fligstein and McAdam 2012; Medvetz 2012), and such interstitial fields are useful for sociological theorizing because they allow us to observe innovative behaviors as actors combine different forms of social capital. Recovery Coaching has recently grown substantially in response to the ongoing opioid crisis in the United States and continues to adapt in response to other emergent drug related crises. Training programs have emerged that aim to further professionalize the industry and to provide people in recovery with opportunities for social advancement. Literature on Recovery Coaching has established the important role that Recovery Coaches can serve with respect to client’s engagement with services following drug treatment (Byrne et al. 2020) and connecting clients to treatments such as MOUD primary and mental health care (Austin et al, 2023). Because Recovery Coaches operate in their roles at the intersection of fields dedicated to public health and safety it is worth continuing to study how Recovery Coaches do this in novel ways so that they are both stable and secure in their own recovery and signaling to others that they are best suited to help others navigate these processes.
The establishment of Recovery Coaching has also served to further address the complicated nature of the opioid crisis. As fatal and nonfatal overdoses continue to rise in the United States, there is a need to continue to invest in a workforce centered around and trained in the principals of “harm reduction” (Marshall et al. 2015; Sue and Fiellin 2021). But harm reduction itself is also a stigmatized concept, and it is worth further investigating sociological processes that produce destigmatization (Lamont 2018, 2023), even if they may do so in unexpected ways like the professionalization of stigma. Fields like Recovery Coaching have the opportunity to integrate commonly known harm reduction approaches into their workflow. For instance, as indicated in our results, Recovery Coaches can advocate for carrying medications like Narcan that reverse the effects of overdose. Embedding mechanisms like this into Recovery Coaching practices and training will expand the scope of services provided to PWUD. As a result of professionalizing Recovery Coaching, many of these methodologies can further be normalized as effective public health and safety responses. This is because in sharing their own experiences with these resources, Recovery Coaches can destigmatize different kinds of approaches that promote the health and safety of PWUD.
More broadly, the professionalization of stigma may provide one route to further explain social processes of re-entry after involvement in the criminal justice system. The stigmatizing effects of a criminal record are well documented empirically (Pager 2003; Stewart and Uggen 2020). In many cases, people who have these records engage in stigma reduction efforts, such as avoiding applying to jobs that require a background check or actively managing stigma in interviews. Recent work shows, however, that some people do engage in other strategies, such as “targeted applying” to jobs (Vuolo et al. 2022). Here, the professionalization of stigma provides one additional stigma management strategy that certain people with records may employ during re-entry. To be clear, it may not be the dominant strategy, but it may also emerge under specific institutional conditions that reward (or coerce) this particular presentation of self.
Second, in terms of broad sociological theory, this study provides a means to update classic literature on stigma management to evaluate how management techniques may be evolving under contemporary social conditions (Lamont 2018). As our theoretical diagram in Figure 1 demonstrates, we don’t expect other conventional approaches to stigma reduction to disappear in late modernity, but we do identify a novel and unexpected way that people are using stigma for professional ends. This insight reaches well beyond our case study at hand and has implications for several streams of future sociological study.
We expect the professionalization of stigma to be common under a few unique late modern conditions that are worthy of further sociological study. First, we expect it to be more common in interstitial social fields—emerging sets of relationships that operate between long-standing institutional fields where actors are more likely to combine different kinds of social capital in unique ways. The literature typically treats stigma management techniques as a means to maintain normative social status (Goffman 1963). In newly emerging fields like Recovery Coaching, among others, sociologists observe how specific kinds of norm-breaking become institutionally advantageous because they serve to differentiate the fields from their more established counterparts (Medvetz 2012; Stewart and Hartmann 2020). More empirical research on other interstitial fields may be able to highlight other unique practices in those fields that expands existing sociological theory, because they appear to be places where structural conditions favor innovative social behavior.
In addition, we expect that the professionalization of stigma to be a useful theoretical tool for better understanding the way that these specific institutions and fields encourage the leveraging of stigma for entre. Some institutional fields have developed toward professionalization as a way to manage and minimize stigma, such as the tattoo industry (Adams 2012). But our results show that professionalization is not necessarily always about minimizing stigma. For example, when candidates from marginalized and stigmatized backgrounds have to decide what they wish to disclose in a job application or a “diversity statement” to establish qualifications to join an organization, it is possible that those institutional conditions invite and encourage specific kinds of professionalized stigma disclosure beyond merely hiding stigma. Racialized organizations, for example, (Ray 2019) may not simply reward concealing stigma, they may also manifest specific incentives for revealing stigma in specific ways. The professionalization of stigma may also appear differently in different national contexts outside the United States (Lamont et al. 2016). More sociological research is necessary to map the relationship between these institutional conditions and novel norms for the presentation of self.
Third, these institutional observations have implications for future research concerned about how individuals present their identities to the world. Sociology is concerned with the process of destigmatization (Lamont 2018) in order to address inequality by addressing recognition gaps between people. To address this issue, research can better map the full range of techniques that individuals use, and institutions encourage, to mitigate stigma. One understudied possibility is the social construction of stigma as a professional asset, which is an ambiguous practice under conditions of capitalism. For example, when people claim a typically-stigmatized identity as a professional asset, such as a mental health diagnosis, learning disabilities or previous gang-involvement (Moore, Kinnear, and Freeman 2020; Waterfield and Whelan 2017), there are many open questions as to whether such a claim is ethical or effective in reducing stigma or achieving professional goals.
Our goal in this analysis was not necessarily to evaluate whether the professionalization of stigma “works” to achieve any particular aim, or whether it is right, just, or good to make such a claim. Instead, we note in closing that it is important for sociologists to understand these kinds of claims are part of a larger socially constructed process worthy of future study about how individual actors within institutions might be trying to “get respect” or legitimize identities in novel and potentially unexpected ways.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.