
Abstract
This explorative paper aims to test a model of operationalized subindicators that allows for a simplified analysis of the social bond between therapists and clients in violence therapy. A theoretical premise of this work is that a stable social bond is a prerequisite for the client’s building a positive self-image and becoming reintegrated into society as nonviolent. The research entails the comparison of two different therapy treatments. A psychodynamic therapy against men’s violence, undertaken voluntarily and frequently used in Nordic countries, is compared to a compulsory cognitive behavior therapy used for men in correctional settings. Although the therapists in both treatments attempt to balance the relationship between themselves and the clients, both therapies tend to alienate the parties from each other, thereby preventing the development of a stable social bond of solidarity. For both treatments, an awareness is needed of those parts of the therapy that evoke shame and pride, thereby permitting an evaluation of the treatment so that the positive quality of the social bond can develop.
Introduction
This study is an attempt to improve our understanding of the relationship between the institutionalized power of therapists, the quality of the social bond between therapists and clients, and ways these dimensions influence the success of therapeutic interventions for violent men. More specifically, this article analyzes the Norwegian therapy commonly used in Nordic countries to treat violent men, known as Alternativ Til Vold, or “Alternative to Violence” (ATV), and compares the result with a prior analysis of a cognitive behavior therapy (CBT) used in treating violent men in correctional facilities.
The theoretical starting points are given by Scheff (1999, 2003), Retzinger and Scheff (2000), Scheff and Retzinger (1997, 2000, 2001), and Retzinger’s (1995) further development of Lewis’s (1971) fundamental work on shame and defense mechanisms. Retzinger and Scheff have played a major role in elucidating the emotional content of social bonds and have developed a successful method to read and interpret verbal, nonverbal, and paralinguistic cues in communication. The validity of their method is not in question, but as the method is time-consuming, technically complicated, and not designed for use outside a research context, it needs to be adapted to suit a therapeutic context. A new model, based on the work of Jansson and Saxonberg (2013) and aligned with the central aspects of Scheff’s and Retzinger’s theories, has been developed and operationalized in a pragmatic way that also includes consideration of power (Barbalet 1998). Therapists using this model are made aware of the impact they have on the client’s self-esteem and opportunities to influence clients positively in the context of therapy (see Figure 1). The theoretical model tested in this study analyzes only the social bond between the therapist and the client, not the actual content of the therapy.
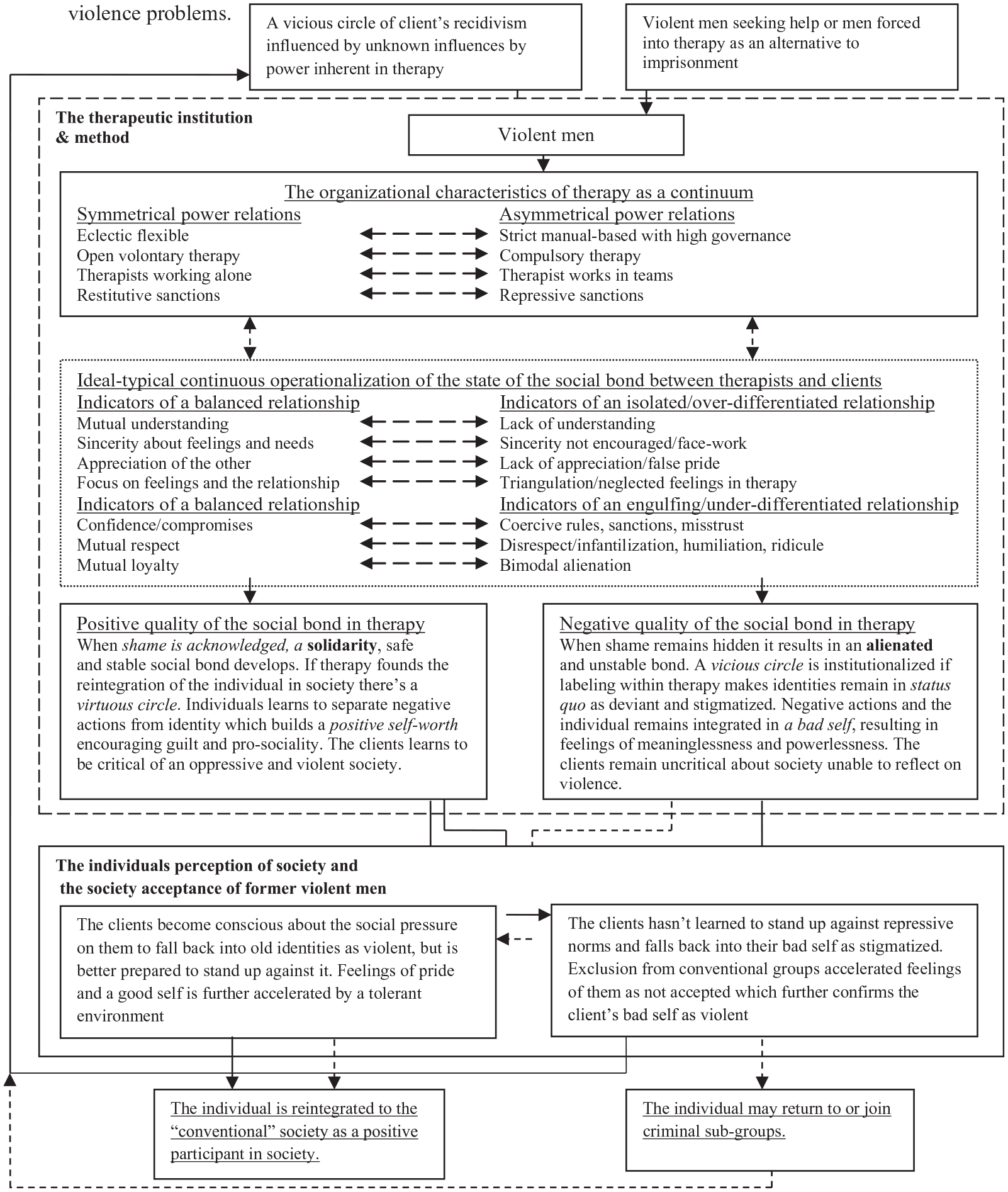
Ideal-typical model of the tensions between different kinds of emotional content in therapy for men with violence problems.
The subindicators of balance or isolation (over-differentiation) and balance or engulfment (under-differentiation) (Scheff 2003) that are an integral part of this new model refer to a pragmatic approach to highlighting what affects the quality of the social bond between the therapist and the client. Although power is relational, and clients have the power to influence therapists, starting with the therapist’s perspective in this research study is important because this approach has not been taken before.
This article’s theoretical approach to understanding the relationship between shame, low self-esteem, and violence against partners is further based on the findings of Gilligan (2003), Brown (2004), Harper et al. (2005), Mills (2008), and Wei and Brackley (2010), which concern the relationship between traumatic and violent childhood experiences and high sensitivity to situations as an adult that bring back memories of being mistreated and unloved.
The theoretical premise of the model (Jansson and Saxonberg 2013) used in this study is that therapies dominated by shame result in an isolating and/or engulfing social bond that alienates therapist and client from each other, which prevents the creation of the stable social bonds of solidarity that are central to a positive self-image and the client’s reintegration as nonviolent into conventional society. Therapy dominated by shame tends to worsen poor self-esteem, which afflicts many clients. In contrast, pride-building therapy, embedded in a stable social bond of solidarity, develops the good sides of the client’s identity and gradually reconstructs their self-image. Being aware of this distinction allows therapists to manage factors that may otherwise determine a negative therapeutical outcome. This model highlights the dynamic interplay between the organizational power aspects that frame the therapy and the quality of the social bond produced by the interaction between the client and the therapist. As Scheff and Retzinger’s (2001) research generally focuses on micro-sociological relationships, it has become equally important to focus on the social power relationship between the parties as it can provide insight into how it affects the quality of social bonds. The model illuminates mechanisms (Sayer 1992) that—in accordance with theoretical premises—might contribute to or prevent an effective therapeutic outcome. It also provides insight into the dysfunctional mechanisms that result in unintended effects of the treatment of violent men.
Theory
The Organizational Characteristics of Therapy as a Continuum
Figure 1 presents a detailed overview of the theoretical model and the framework that is the theoretical foundation for the comparison of the two case studies. As the power imbalance between the therapist and the client affects the quality of the social bond, it is important to focus on the organizational setting within which the therapy occurs. The ideal-typical symmetrical power relation between the therapist and the client is characterized by the following indicators: eclectic flexible therapy and open voluntary therapy, therapists working alone, and restitutive sanctions. The asymmetrical power relation in contrast is characterized by these indicators: strict manual-based, compulsory therapy, therapists working in teams, and repressive sanctions.
These dimensions are central to therapeutic practice. Manual-based therapy is less flexible in its ability to adapt to unique client needs than is eclectic. Clients who are compulsorily remitted to therapy have no choice but to adapt to therapy or miss out on benefits, which means that positive changes in the client’s attitudes or behavior may mistakenly be considered real. Compulsive treatment may also remind clients of negative childhood experiences, reducing trust between the therapist and the client. Teamwork among therapists increases the power of the therapist and could make the client feel less autonomous. It is also important to consider whether rules and repressive sanctions are manifestations of authoritarian power and whether punishments have the client’s best interest in mind.
The Tension between Solidarity and Alienated Relationships
According to Scheff (1990, 2003; Retzinger 1995; Retzinger and Scheff 2000; Scheff and Retzinger 1997, 2000, 2001), a relationship between two parties can be based either on a solidarity social bond and feelings of pride in belonging or on an alienated social bond and feelings of shame in not belonging. Along the same lines, the relationship can lead to both parties being isolated from the other (i.e., over-differentiated) or being compelled to belong, as engulfed by the other (i.e., under-differentiated). Both alternatives create an unsafe social bond with the other person or group.
Depending on whether the relationship between the therapist and the client falls under the category of balance or isolation/over-differentiation, the following subcategories have been developed, which have the therapist’s perspective in mind. Mutual understanding refers to the parties understanding each other’s feelings and thoughts. Lack of understanding results from unfocused emotions and the parties not sharing the same experience. Sincerity about feelings and needs is present when parties are honest about their feelings and thoughts toward each other. Sincerity not being encouraged occurs when hidden conflicts and motives prevent clients and therapists from meeting each other as individuals, instead meeting as roles, producing facework. Appreciation of the other is present when therapy emphasizes the client’s strengths and positive qualities, although the client may be dominated by their own bad experiences. Lack of appreciation and False pride both occur when parties overemphasize their positive qualities to compensate for the other’s lack of respect. Focus on feelings and the relationship occurs when parties realize that the quality of the relationship is a prerequisite for the positive effect of therapy and when therapists see the relationship as valuable and not only as a professional tool. Triangulation and neglected feelings in therapy will be the result when clients are allowed to talk about other things and people as a defense against the pain of talking about their own feelings and experiences.
Depending on whether the therapist-client relationship is categorized by balance or engulfment/under-differentiation, the following subcategories have been developed, which also have the therapist’s perspective in mind. Confidence and compromises will result when there is trust, which makes compromise possible. Mistrust results in coercive rules and sanctions with rewards/penalties that regulate the relationship. Mutual respect exists when the therapist respect the client’s right to control their autonomy. Disrespect is characterized by infantilization, where clients are reduced to diagnoses/disorders or their negative actions, and overprotective therapists, using normative statements, suggest clients have a lower value. Mutual loyalty dominates when therapist and client see their relationship as more important than the relationship with their respective group. Bimodal alienation prevails when the parties primarily live up to and are loyal to the expectations of their group.
Method
In contrast to the ideal-typical case study that is heuristic and inductive, this study has a deductive design and has been preceded by work on the development of a theoretical model (Jansson and Saxonberg 2013) for understanding emotions that are relevant to the effect of therapy. That review article summarized the sociology of emotions and the literature that laid the foundation for the theoretical model used in this empirical study comparing two therapeutic approaches. This study focuses on the meaning therapists ascribe to their practice and what they do, but not on the direct perspective of reality itself (e.g., inductive), but through a deductive model that is applied to therapy. Furthermore, this study does not address therapy in its complex context and does not relate to the treatment facility’s history or its relationship to other institutions (Chadderton and Torrance 2011), which limits the way social practices can be understood in their entirety. The unique qualities and experiences of the individual therapists are not the focus, but rather the gestalt of them as a collective whole. The quotes below are inserted in the text to demonstrate both the variety and the commonalities among the therapists. The small sample size is not an issue since all therapists in both therapy settings participated. The therapist’s description of the therapy content gives us secondary access to the social reality they construct together with clients. The client’s reality is described indirectly through their therapist’s statements about the therapy, which limits our understanding of the power relationship, but is a necessary starting point as this type of research has not been carried out before. For a more complex understanding, clients’ perspectives must be included. The main aim is to explore whether the theoretical model (see Figure 1) is functional and adaptable to different therapies. The results of this study’s theoretical model as applied to the two types of therapy compared in this paper cannot be generalized, even if the therapy is based on clear manuals. The intention here is the first test, to create a more generalized picture of the way of working of different therapies requires a larger sample. These limitations are necessary to develop the core theoretical aspects. The study uses the identical theoretical framework, data collection procedure, and analysis method as the previous study of a CBT treatment (Jansson 2013) that the result compares.
Ethical Considerations
The study follows the ethical standards developed by the Swedish Research Council (2020) and processed by the University’s local research ethics committee. The research does not address sensitive subjects or vulnerable research participants as it focuses on the daily therapeutic work practices and content, and no regional ethics committee approval is required for a study of professional therapists (SFS 2003:460). Informed consent was obtained from each participant in advance of the data collection, and each participant was informed that they could withdraw at any time. Participants are anonymized and data are processed confidentially so that no unauthorized person can access them.
Selections of Treatments
The result from this study of a single ATV treatment for violent men is compared with the result of a prior analysis of a CBT treatment used in treating violent men (Jansson 2013). ATV, commonly practiced in Nordic countries, provides a fruitful comparison to the cognitive therapy practiced in correctional facilities. The result from the previous study shows that CBT treatment generally produced a power relation between the therapist and the client that was unbalanced. The extensive control generated an isolated/over-differentiated or an engulfed/under-differentiated relationship, and the cognitive focus produced unacknowledged feelings and an isolated or engulfed relationship, a point returned to in more detail below.
A Swedish ATV treatment center was selected in which clients enroll voluntarily. The male clients had used violence against their female partners and the treatment is essentially based on the ATV therapy founded by Jonas Isdal (Råkil 2006) and conducted through group therapy sessions supplemented with individual therapy. ATV therapy is influenced by the psychodynamic school and, based on the client’s childhood experiences and emotions, focuses on the generation of the client’s empathy. An important theoretical premise is that violence is goal-oriented and a means of achieving and maintaining power and dominance over others. Although violence is rationally driven, it has emotions behind it, which are influenced by men’s experiences of being unable to live up to cultural and social expectations. The violence is therefore driven by a sense of helplessness or powerlessness, where the feeling of powerlessness in the current situation may be caused by childhood experiences such as violence, abuse, a lack of care, rejection, and loss.
ATV consists of four phases in which both moral reasoning and emotional development are in focus. In the first phase, clients learn to acknowledge the violence without making any denials and/or excuses. In the second phase, clients must learn that the violence is always a voluntary decision they made among several options and that they, therefore, are fully responsible for it. In the third phase, clients must understand the causes of violence, which can originate in childhood, in social contexts, and in their living conditions. Finally, in the fourth phase, clients must empathically understand the consequences of their violence and take full responsibility for it. As ATV aims to end men’s violence and is needs-driven, it allows the treatment to range from 10 weeks to 2 years, with at least one treatment per week. The group therapy consists of one therapist and four to six clients discussing the different themes related to the phases. In ATV, it is generally important to identify the clients’ progress in the recovery process; therapy that does not match the client’s readiness is therefore likely to create resistance.
Choosing ATV therapy as a comparison permits a challenge to the theoretical hypothesis that therapies without extensive governance and control will generate a balanced and solidarity social bond between the therapist and the client. The emotional focus in ATV therapy may counteract the development of an isolated and/or engulfed relationship between therapists and clients.
Data Collection Procedure
The interviews and summarization of the results were conducted by the author. Both therapists who work at the ATV treatment site, which is in a mid-sized Swedish municipality, were included in the study. Therapist 1 (T1) is male, middle-class, Caucasian, in his mid-50s, and a licensed psychologist and an accredited psychotherapist with extensive experience. Therapist 2 (T2) is male, middle-class, Caucasian, in his mid-40s, and an accredited psychotherapist and licensed nurse with extensive experience. (In Sweden, strict requirements are placed on accredited psychotherapists/psychologists concerning confidentiality and record-keeping.)
The data collection was conducted in two phases. First, one 3-hour interview with each therapist was conducted based on themed semi-structured open-ended questions. To reach saturation for each theoretical theme, all respondents’ answers were included. The respondents were not equally active in their responses to each theme, but each theme did receive answers. In Phase 2, all transcribed interviews were condensed into meaningful units that captured the essence of the larger pieces of text and returned to the two therapists as a member-check to allow them to complete the data, reflect on the accuracy of the preliminary analysis, and tie up loose ends. The results from Phase 2 formed the basis for a deeper discussion of the therapy in accordance with writ large (e.g., Creswell 2007). The final coding of the therapists’ statements was verified by a blind intercoder reliability design (Creswell 2007), where a researcher, without knowledge of the original coding, coded the transcribed data in accordance with the predefined subindicators. The percentage coded the same was about 70 percent. After discussion, an intercoder agreement with a consistency rate of about 85 percent was reached.
Analysis Method
Qualitative deductive oriented content analysis was used to systematically analyze the interviews with a level of theoretically derived subindicators. According to Hsieh and Shannon (2005), directed content analysis is a successful method for the exploration of the applicability of coding schemes derived from theory and empirical research. According to Patton (1990), content analysis is generally useful both to inductively identify and categorize basic patterns or themes that emerge in empirical material and to systematically categorize content based on predetermined categories. Both approaches use the condensation method (Creswell 2007) to reduce long interview answers to pithy excerpts and quotes. However, the use of theoretical preconceptions could be a problem, which must be dealt with by making room for new categories that do not match the theoretical framework. In this study, the focus was not on theory development but to test the applicability of the model used in this study. The therapists’ statements were related to the organizational power aspects that are assumed to influence the social bond between the therapist and the client. In the final step, the statements from the therapists were interpreted in accordance with the given figure of a continuum between solidarity and alienated (e.g., isolated/engulfing) social bonds. No new naturalistic category or concept emerged alongside the theoretical preconceptions.
Results
Organizational Power Aspects of ATV Therapy
Based on the theoretical model used in this study, the following organizational areas have been selected as central for therapists to relate to as these areas represent power structures that influence therapists and clients and the treatment itself.
Eclectic or manual-based
According to the therapists, ATV therapy is eclectic as it is based on both psychotherapy and manual-based therapy techniques. T2 states, “ATV is supplemented by psychodynamic, cognitive and pedagogical features . . . and therefore differs from the CBT therapy that is prospective.” Regarding a question about ATV manuals governing their work, T1 states, “In addition to the general knowledge gained in the training to psychologist and an accredited psychotherapist it is possible to deviate from the manual.” T1 continues, Obviously we want to highlight the important issues . . . tricky persons talk a lot about irrelevant issues . . . and we have structured tasks that we address that is good to use so they do not chatter away . . .
T2 adds, Other therapists can rely on therapeutic manuals. We are not that insecure. Perhaps they are more insecure in CBT therapy? I give myself the freedom to customize the therapy . . . and the model provides much freedom even though it is a model.
Open or compulsory
According to the therapists, clients align themselves with the open therapy form of ATV voluntarily. ATV therapy lacks the character of compulsion, as there are no correctional rules that the clients can violate. T1 states, “Therapy is voluntary and for it to be successful, clients must attend to therapy regularly. Therapy will not work otherwise.”
Therapists working individually or in teams
The therapists explain that they work individually but clients’ situations and problems are discussed in consultation with colleagues. This routine helps therapists deal with the atrocious violent acts that their clients have committed in the past. When the client’s female partner is participating in therapy, it becomes critical to consult with other colleagues to establish whether the client continues to use violence.
Restitutive or repressive sanctions
In contrast to therapies that are conducted under the supervision of the prison administration, ATV therapy is voluntary. The clients who are participating in therapy are at no risk of sanctions if they drop out.
Summary of the organizational power aspects
In summary, the therapists’ statements do not indicate an alienation from the clients. The eclectic psychodynamic approach and less extensive guidance provided by the ATV manual seem to increase the scope for personalization of therapy. The therapy does not need repressive sanctions for rule violations as the therapy is entirely voluntary. As the organizational aspects of power do not subordinate the clients, therapists may be better prepared to distinguish between superficial adaptations and real changes.
The Social Bond between Therapists and Clients
The developed level of subindicators within each area aims to increase knowledge of the social bond and the emotional aspects of ATV therapy. In what follows, we will look at the tension between the balanced relationship and the isolated/over-differentiated relationship and the balanced and the respective engulfed/under-differentiated relationship that indicates when the therapy results in solidarity or an alienated social bond between the therapist and the client.
The balanced or isolated/over-differentiated relationship in ATV therapy
The social bond between therapists and clients can ideal-typical be balanced
Mutual understanding or lack of understanding
The therapists’ efforts to understand the clients at a deeper level tend to balance therapists and clients in relation to each other. The therapists highlight the importance of being receptive when it comes to interruptions in communication, as it indicates misunderstandings. T1 says, “ . . . you get a response . . . or you notice when somebody has not quite understood . . . apparent in an interruption and when the dialogue comes to a halt . . . ” T1 believes that by continuing with the therapy, you can acknowledge the client as a person: “ . . . say that you understand the clients fear . . . he will feel understood and acknowledged . . . it encourages him to be frank about it . . . ” T2 states that differences can be seen from body language and at times of silence: “Sometimes, at an intense moment, the whole group can become quiet, but it is not an uncomfortable silence. It signifies that what has been said has been heard and that the group will together understand what has been said.” Both therapists state that when there is a misunderstanding, it becomes a case of recognizing the two sides of the client: the one who is violent and the one who takes responsibility. T2 states, . . . it is frightening to see that side of him that acts like a torturer, terrorizes and hits, yet at the same time; the man is unhappy, guilt-ridden, and rueful and wants to take responsibility. We need to get these two parts to meet.
The therapists further argue that some of the clients’ problems are related to their inability to put the different parts of themselves into a whole. They are not another person when they use violence. But the violence is difficult to accept because it is so shameful. T2 states, “ . . . in the case of the clients’ experiencing trauma, they may go back and think about what they felt and was thinking when they acted violently.”
In summary, this dimension is dominated more by the therapists’ understanding than their confusion which, according to the theoretical preconceptions used in this study, contributes to a balanced social bond.
Sincerity about feelings and needs or sincerity not encouraged/facework
The therapists believe that there may be a lack of honesty and sincerity from clients within the group sessions. Group sessions do not address delicate individual experiences. T2 states, . . . they openly admit that they have beaten women by enrolling into the therapy, but in the group sessions, it is difficult to make them speak about the assaults they have committed. They feel ashamed to acknowledge this in front of the others
The therapists argue that group therapy still opens up something. T2 states, “They might hide it at first . . . they are in denial . . . which can be processed later instead.” In summary, the lack of sincerity in the group session tends to isolate the parties from each other.
Appreciation of the other or lack of appreciation/false pride
Therapists state that they show appreciation for a client’s progress, even when small, which balances the relationship and contributes to building the clients’ positive qualities, a prerequisite for their leaving their old identities as violent. T2 states, “Their self-esteem is at the very lowest when they enter therapy, and they are often ashamed . . . therapy is about creating a positive self and value as a person.” Both therapists argue how important it is to ensure that clients take responsibility and change their old negative behavior. The clients have to learn to act in a way that makes them proud of themselves, for example, by taking care of their children. T2 believes that this kind of positive change strengthens them: “ . . . it gives them enough self-esteem to not end up with a bad relationship that led to violence . . . ” The therapists state how important it is to prioritize the negative behavior so that it disappears; otherwise, the negative behavior can adversely affect therapy. Both therapists recognize that their having extensive training and representing the therapeutic profession may exacerbate the distance between them and the client. T2 states, I think this has two sides, on the one hand . . . we do convey that we do not hold any kind of magical knowledge that they have to adapt to . . . but we state, nevertheless, that we make use of a method that works
The therapists appear not to minimize their importance, however, since they do have both knowledge and expertise. T2 continues, “They expect that we have some kind of expertise and that we will be able to help them.” Both therapists state that clients sometimes take the therapists’ help for granted, but T2 argues, “There is something in the relationship that makes me believe that they also express gratitude . . . ” The results from this dimension indicate a predominance of elements that are associated with an appreciation of the other and a balanced social bond.
Focus on feelings and the relationship or triangulation/neglected feelings in therapy
The therapists describe how clients sometimes adopt psychological defenses and triangulate/talk about irrelevant topics instead of the experiences that are sensitive and painful for them. T1 also concludes, “ . . . the ATV method tends to reduce the bullshit between therapist and client.” Furthermore, the clients triangulate when they focus solely on their female partners and not on themselves. T2 states, “ . . . he says that she is doing this and that and that she behaves inflexibly in a particular manner.” The clients seem to be in a kind of separation phase when they realize that the relationship may come to an end; T2 further says, Generally speaking, the men’s fear that the relationship with the partner will end increases their motivation to seek help . . . they want someone to listen to them . . . the clients often highlight the relationship between physical and psychological violence.
T2 continues, “The clients often argue that the woman, by the way she behaves towards them, exerts psychological violence . . . ” The therapists argue for the possibility of bypassing the client’s psychological defenses by teaching them how to interpret what happened in the concrete situation and what caused their violence against their partner. T1 states, “ . . . so that the clients can see a context . . . this reduces both shame and guilt . . . ” The therapists also believe that clients, through the ATV method, learn to use an alternative approach toward their partner, one that has strong potential for making constructive communication with the partner possible. T2 states, “They learn how to communicate instead of hitting . . . they learn to put words to feelings and to tell their partner what they want to do . . . ” Both therapists state that one major cause of male violence against women is men’s inability to be frank about what makes them feel bad in a relationship and explain why they get “pissed off.” T2 continues, “They are not so good at putting words to feelings; however, they can quickly learn it.” To sum up, the therapists report that clients tend to use triangulation as a defense when it comes to violence against the partner. Clients divert the conversation from themselves when they emphasize psychological violence from her side. A balanced relationship is a prerequisite to making the clients talk about their violence, but despite the therapists’ many efforts to balance the relationship, their statements indicate that the parties are isolated from each other.
The balanced or engulfed/under-differentiated relationship in ATV therapy
The subindicators below give us enhanced knowledge about whether the social bond between therapists and clients is balanced
Confidence/compromises or coercive rules, sanctions, mistrust
The therapists state that the balance between freedom and responsibility primarily depends on ATV therapy being voluntary. Clients decide independently how many times they attend therapy. T1 states, “ . . . they have the opportunity to go to therapy on 24 occasions . . . and it varies in length depending on the clients’ motivation.” T1 describes clients who are very motivated but still drop out. He believes that it has to do with how the clients perceive them: “As a threat when I am perceived as someone who will touch upon vulnerable sides of the client . . .” On questions about whether there are sanctions against those who drop out of therapy, T2 states, No, there is a difference between those who are convicted to therapy within a prison sentence and when they participate voluntarily. We are a voluntary organization . . . thus we do not have those worst offenders . . . those with denials do not come to us.
T2 continues, . . . the most important is the clients’ responsibility . . . and them realizing that their violence is their responsibility . . . and not society’s fault. It forms the basis of the client’s motivation and our treatment . . .
Both also point out their responsibility as therapists. When the client commits a crime, they do not regard it as a private matter anymore. T2 says, “Only if there is no apparent danger . . . and when the children are not harmed, it may continue to be a private matter.”
On questions of confidence and trust, the therapists argue that the clients respond positively when the therapists have confidence in them and if they perceive the relationship to be based on empathy. However, T1 adds, . . . if it concerns clients who previously have not experienced trust in a person it could, of course, be more difficult. Many of the clients are in a crisis and want help. They tell you that they want your help. If you are willing to help them, trust is created along with the hope of obtaining the help.
T2 further states, “Some clients are more genuine, and you can trust them, but some others use a façade and are hiding something.”
On questions about whether ATV therapy can adjust to the unique client with tailored treatment, T2 claims, “In group therapy, you must stick more to the form, especially as we made it official that we are based on the ATV model. We may feel a bit restricted by that.” The therapists further argue that there is a trade-off if hurtful experiences and topics are left alone or not in the group therapy. T2 continues, This is about the subtleties in therapy, about people’s psychological defenses and when you should respect their integrity and when you should not. Sometimes you have to respect the client’s defenses and not go any further, it is important to be observant.
The therapists agree that clients often anticipate the expectations of them. T2 argues that this kind of process involves identification: “It is part of their transformation, and adaption to norms, but are they lying to us, yes they are!” The therapists want to see straight through the lies, but do not believe they can. T2 adds, Yes that is what you want . . . group processes contribute to this . . . and in this group, you want to capture this kind of thing in some kind of way. They express what we longed for . . . maybe it is unconscious, but it feels genuine.
On the question of whether there are unrealistic expectations of the clients, T2 claims, “The treatment is sufficiently long to find out what is realistic. We try to address this by starting each week with the ‘week’s violence’ and return to their violence in every therapy session.”
Overall, the therapy is voluntary and without sanction. On a basic level, it counteracts an engulfing over-differentiation between the parties. The therapists’ statements, however, suggest that this is not enough to assert a balanced relationship. For example, complete trust between the client and the therapist cannot be achieved because the “secrets” that clients disclose in confidence must be reported when it comes to serious crimes committed. Furthermore, when the psychodynamic element in group therapy enters sensitive areas that clients do not want to share with others, some choose to drop out.
ATV’s eclectic orientation is based on a manual, which prevents it from being completely tailored to clients’ needs. The clients are additionally in a position of dependence as they are in need of help which may result in the relationship becoming over-differentiated. Overall, this dimension is a mixture of engulfing elements, which restricts the possibility of increasing trust between the therapist and the client. Both under- and over-differentiation hamper the achievement of balance between the parties.
Mutual respect or disrespect/infantilization, humiliation, ridicule
On the question of the therapist’s influence on what feelings clients display during therapy, T2 states, “Psychotherapy can be both provocative and manipulative . . . and involve people in processes that they do not want to participate in.” Both therapists state that this is a dimension that is related to their professionalism and their ability to respect what individual clients can cope with. T2 also states, “The clients can join this ATV therapy whenever they want but also quit whenever they want. No compulsion element here.”
The therapists admit that they sometimes take up more space in their interaction with the clients than they should. T2 says, This is the therapists’ responsibility . . . you have to keep an eye on how much space you take up . . . an inner observer. I think therapists tend to take up more space than they should. I have to ensure that the clients get enough space to talk about their problems.
In sum, despite the efforts of the therapists to allow the clients to manifest themselves in a new way, the dimension is dominated by engulfing aspects since the therapists are not entirely able to respect the client’s autonomy.
Mutual loyalty or bimodal alienation
On the question of whether therapists are loyal to colleagues or clients, the therapists argue that there are risks to being allied with the client, the greatest being the loss of objectivity. T2 states, We therapists sometimes have different perspectives on how to treat our clients, but we also have some sort of common reference. In our case, it is ATV as our working method. However, we balance not relying too strongly on only one single method and becoming too eclectic.
The therapists also note the importance of all colleagues collaborating within the ATV therapeutic setup, as both the male perpetrator and the female victim could be participating in therapy. T1 states, “ . . . if violence or a threat of violence take places among the couple, we must have an open dialogue about it.” The therapist stresses that confidentiality is compromised in that they must act against the client when the female partner is subjected to violence. The clients show no indication of being loyal to each other during group sessions, and engulfment/under-differentiation between them is absent. The balance between the parties in the relationship is enhanced when the therapist has control over the method of treatment and not vice versa. In summary, therapists appear to be loyal to and under-differentiated with one another, thus negating loyalty between the therapist and the client.
Conclusion Regarding ATV Therapy
The overall organizational principles of ATV therapy are that the therapy is voluntary for clients, predominantly eclectic, with more than one theoretical approach in use, and with therapists who work individually in therapy and use restitutive sanctions. In summary, the power balance between the therapist and the client is predominantly symmetrical. The efforts of therapists within this ATV framework are an important contribution to the reduction of the men’s violence; however, not enough is done to ensure the creation of the ideal-typical stable solidarity social bond.
The dimension balance-isolation is characterized by an understanding of the clients’ feelings. Sincerity is inhibited by group therapy, as it does not go as deep into sensitive areas as individual therapy does. The therapists, however, try to identify every bit of progress clients make, no matter how small, which is a way of showing appreciation to the clients. The focus on feelings is hampered as the clients tend to use psychological defenses such as triangulations instead of uncovering their inner feelings. In sum, therapists and clients are isolated from each other in two out of four dimensions, which contribute to an alienation between them.
In the dimension of balance-engulfment, the therapist and the client having confidence in each other is restricted because of a mixture of engulfing content in the therapy. Respect for the client is limited since the therapist tends to take up too much space, which engulfs the client. Therapists’ loyalty to each other tips the balance away from clients. The clients appear to be engulfed by ATV therapy in all three dimensions, which contributes to alienation. In conclusion, there is a tendency for ATV therapy to alienate the therapist and the client from each other and prevent the development of a solidarity social bond, which is a prerequisite for a client being able to build a positive self-image and then reintegrate as a positive member of society.
Results from the Single Case Study of a CBT
The CBT treatment we consider here for comparison is practiced at a compulsory Swedish treatment center where clients are remitted for therapy as an alternative to prison (Jansson 2013). All four active CBT therapists were interviewed. In Sweden, fewer strict requirements concerning training, confidentiality, and record-keeping are placed on psychotherapists with basic training. The CBT treatment at this site is manually based and uses group sessions and lectures, supplemented with components from aggression replacement therapy and motivational interviewing. Table 1 presents a summary of the results from the study of ATV therapy compared with the results from this previous study of CBT (Jansson 2013). As mentioned before, both studies used identical methods and procedures.
Semantic-Differential Illustrating the Continuum between Pride and Shame Building Factors in Two Therapies Against Violence In Sweden.
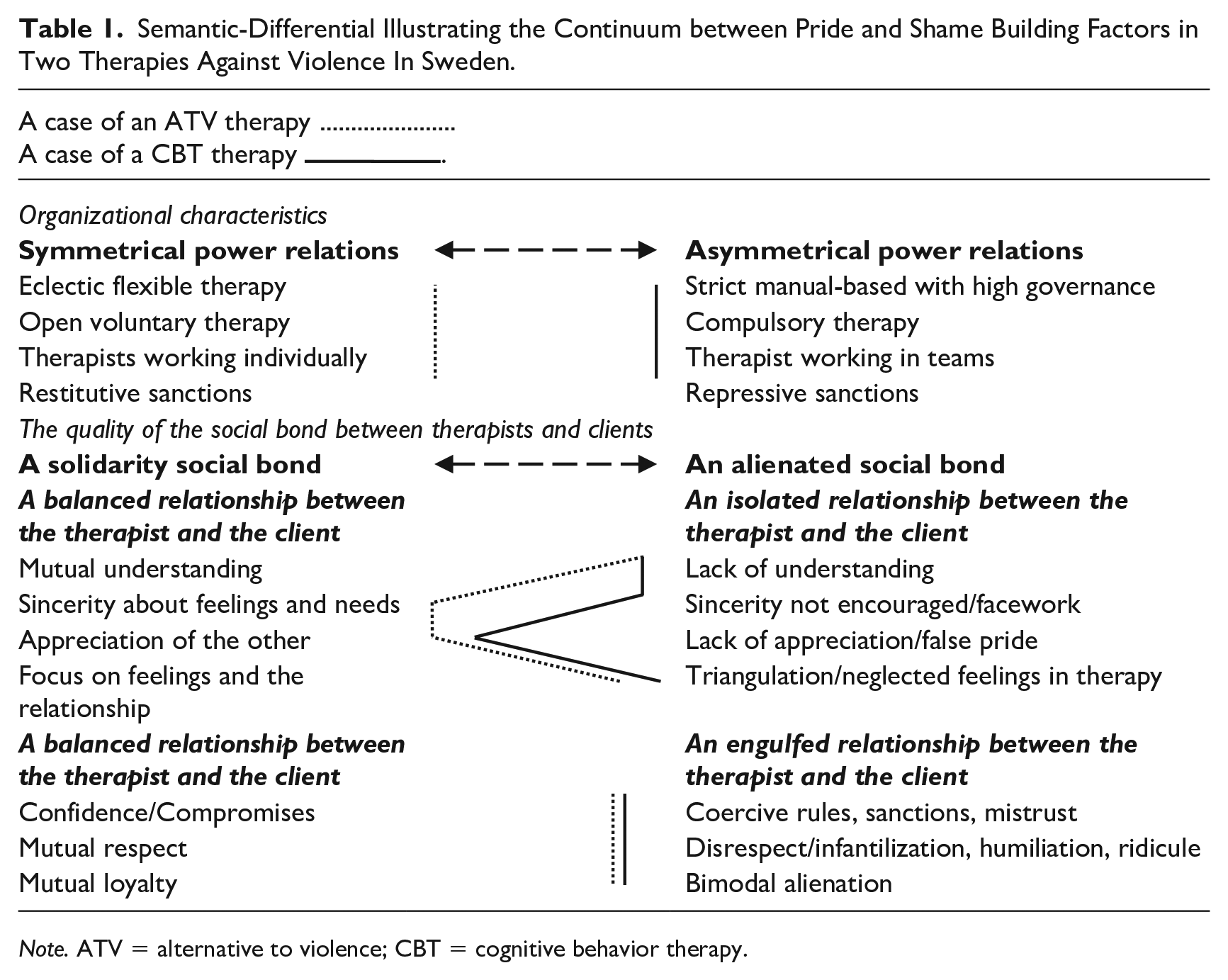
Note. ATV = alternative to violence; CBT = cognitive behavior therapy.
Preliminary conclusion regarding the CBT treatment
The study of CBT (Jansson 2013) indicates that, with regard to organizational power, the therapy uses manual-based techniques, is compulsory, with therapists who work in teams, and with the frequent use of repressive sanctions. With regard to the tension between balance and isolation, the therapy has a tendency to isolate the parties from each other as it is dominated by a lack of understanding of emotions and a lack of sincerity, with the CBT therapist arguing that is harmful to delve too deeply into feelings. The CBT therapist tends to produce fewer processed emotions. The therapist does, however, show appreciation of the client’s progress so that their positive qualities are highlighted. Within the tension between a balanced or engulfed relationship, CBT treatment tends to produce engulfed relationships as confidence in clients is limited, which negatively affects the possibility of compromise. Clients tend to be engulfed and might be infantilized by diagnoses that deprive them of their unique individuality. Therapists are loyal and under-differentiated to each other. Furthermore, there is bimodal alienation from the therapists’ side, which alienates therapists and clients from each other in six out of seven dimensions of the theoretical model, complicating the development of a solidarity social bond.
The ATV Therapy in Conjunction with CBT Treatment
A basic comparison between the two therapies indicates that the organizational power relationships between the client and the therapist are quite different in each case. ATV therapy is based on an almost symmetrical power relationship between the therapist and the client, while CBT treatment is based on an asymmetrical one.
In the dimension of balance-isolation, CBT treatment is characterized by a lack of understanding, in general, and by the exclusion or minimization of the client’s feelings, in particular. ATV therapy is the opposite in considering feelings as central. Sincerity in both cases is inhibited by group therapy, as it does not delve as deeply into sensitive areas as individual therapy. Both therapies try to identify every small step of progress a client makes, which is a way of showing appreciation to them. The focus on feelings is somewhat restricted in CBT treatment as the therapists avoid getting too close to the clients’ sensitive areas. This limits the space for acknowledging shame. In ATV therapy, the acknowledgment of shame is complicated by the clients’ use of psychological defenses/triangulations that work against uncovering genuine feelings. In summary, with CBT treatment, the therapists and clients tend to be isolated from each other in three out of four dimensions, and with ATV therapy in two out of four. In the dimension of balance-engulfment, confidence each party has with respect to the other is limited within CBT treatment because of the clients’ diagnoses, the strict rules, and the atrocious acts the clients may have committed in the past. In voluntary ATV therapy, confidence is hampered because clients may drop out whenever they want and the therapists have to report clients’ violent offenses to the police. Respect for the clients’ ability to be rehabilitated is moderate in CBT given that diagnosed mental disorders are considered more or less irreversible. Within ATV therapy, respect is more cumbersome as the therapists tend to take up a lot of space. The loyalty among therapists, within both therapies, disadvantages loyalty toward clients. In conclusion, both therapies seem to be engulfed in all three dimensions.
Conclusion
For CBT therapy, the results seem to be in line with several of the theoretical assumptions. The results from ATV therapy, however, are not as expected. Concerning the quality of the social bond between the therapist and the client, the two therapies report almost identical results. However, it is only by taking into account the organizational conditions that we can thoroughly understand the results. The voluntary and psychodynamic-oriented ATV therapy is organizationally based on a symmetric relationship between the therapist and the client and focuses on emotions that are crucial for building a solidarity social bond. The CBT treatment analyzed here is compulsory, forward-looking, and focused on cognitive and behavioral changes, which theoretically may counteract the building of a stable social bond. The ATV therapy fails to attain a stable social bond in five out of seven dimensions and appears to be better at combating over-differentiation/isolation than under-differentiation/engulfment.
ATV therapy is midway between being eclectic and manual-based therapy, whereas CBT therapy is entirely manual-based. The use of group therapy is prescribed in both therapies. However, the group therapy method reduces clients’ desire to be sincere about their shameful experiences and behaviors, which tends to isolate the parties from each other. The manuals guide the emotional focus in ATV and the cognitive one in CBT, and lay the foundation for the therapist’s understanding of the clients. ATV is voluntary and has restitutive sanctions; despite this, confidence and the focus on feelings are complicated because clients may drop out of therapy at any time, particularly when the therapists address hurtful emotions and succeed in bypassing the clients’ defenses and triangulations. CBT is compulsory with repressive sanctions and has a prospective cognitive focus that reduces respect and confidence and infantilizes and engulfs the clients. It uses a team-oriented approach which negatively influences mutual loyalty and confidence. However, both therapies show appreciation for the clients’ progress.
Both therapies are generally inadequate in acknowledging shame and are therefore unable to develop solidarity and a stable social bond between the therapist and the client. Although both therapies are influenced by their different organizational prerequisites, there is still large room for maneuvers to foster the development of a stable social bond, especially when it comes to increasing the proportion of individual psychotherapy.
This comparison of two case studies has been informed by an interest in improving the situation indicated by prior research that violence therapy does not have the intended effect. This study could be used as the basis for an intervention project and after the completion of an intervention to evaluate the effectiveness of the interventions. The therapist’s clinical expertise is of equal importance to research in changing the direction of an existing treatment. In addition, the clinical use of a sociological emotional approach can help practicing therapists understand the importance of improved communications and the emotional experiences of therapy. However, disciplinary experts do not always know best, we also have to consider the client’s decision of what is useful and relevant to their own experience (Cavanagh 2021). By acknowledging shame, thereby improving the quality of the social bond in therapy, clients may increase their feeling of pride and lead to an improved self-image. The need to do so is particularly acute in the dimensions in which both therapies seem to counteract a stable social bond. Today, there is a widespread and unacceptable degree of relapse in violence after completion of violence treatment. In addition, Guy (2009) highlights the importance of learning-based therapy occurring in a nonthreatening environment in which the client/offender has the opportunity to reinforce new behaviors. If the theoretical premises used in this paper are true, other therapy models can be examined and further development of the therapy considered. If clients are encouraged to feel pride in their good qualities, they can more easily separate themselves from the negative actions they have taken. Furthermore, therapies that correspond to the requirements of this paper’s theoretical model must be developed, tested, and evaluated. One possible hypothesis for why the two therapies examined in this paper show similar negative results is that emotions generally avoid discovery when they are not systematically operationalized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.