
Abstract
Background
Extubation in preterm very low birthweight (VLBW) infants is a critical step in respiratory management. Accurately predicting extubation success is challenging because of immature respiratory control, surfactant deficiency, and limited pulmonary reserve. The Spontaneous Breathing Evaluation (SBE) has emerged as an important bedside method to assess readiness for successful extubation, although the optimal duration of this evaluation remains uncertain.
Methods
This retrospective observational study included preterm neonates between 26 and 34 weeks of gestation with birthweight <1500 g who required mechanical ventilation for more than 24 h in a tertiary NICU over a 12-month period. Infants who underwent SBE for either 3 min (Group B) or 10 min (Group A) as part of routine extubation readiness assessment were identified from clinical records. Group allocation was determined by a protocol change implemented mid-study period: infants assessed during the first 6 months underwent 10-min SBE, and those in the subsequent 6 months underwent 3-min SBE. The SBE was performed on endotracheal CPAP; failure criteria included sustained oxygen desaturation (SpO2 <88% for >10 s), bradycardia (heart rate <100/min), apnoea requiring stimulation, or a requirement for increased FiO2 >0.1 above baseline. Extubation decisions were based on SBE performance combined with clinical readiness criteria, including stable ventilator settings, acceptable blood gas parameters, and clinician judgment.
Results
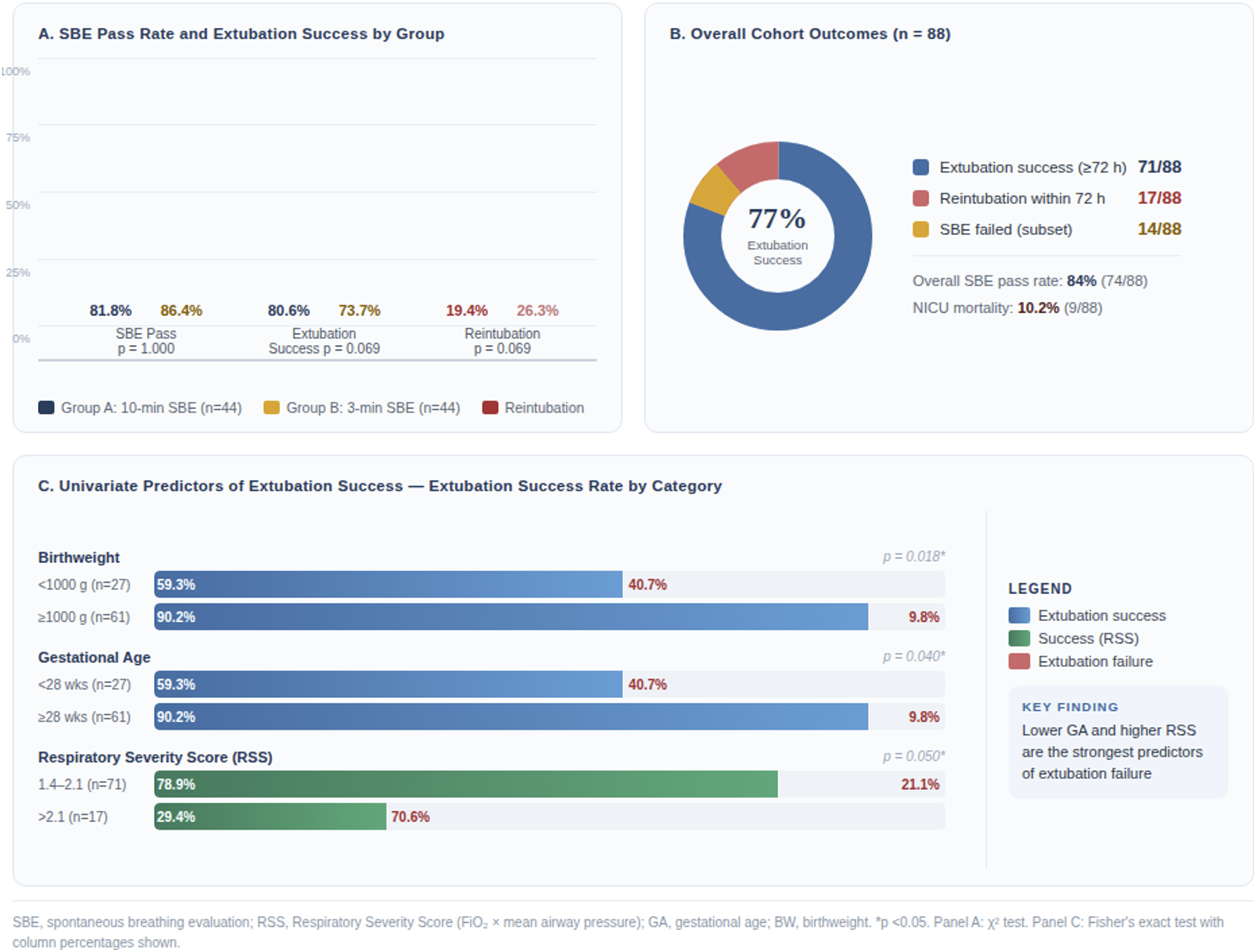
Eighty-eight infants met inclusion criteria (44 in each SBE-duration group). The mean gestational age was 29.9 ± 2.1 weeks and mean birthweight was 1168 ± 258 g. The Respiratory Severity Score (RSS; calculated as FiO2 × mean airway pressure) was significantly higher in the 10-min SBE group (1.85 ± 0.44 vs 1.67 ± 0.31; p = 0.031), indicating greater baseline respiratory severity in that group. Overall, 84% of infants tolerated the SBE and 77% achieved extubation success, while extubation failure occurred in 23%. Most SBE failures occurred within the first 3 min, regardless of total SBE duration. On univariate analysis, birthweight <1000 g (p = 0.018) and gestational age <28 weeks (p = 0.040) were associated with lower likelihood of extubation success, and RSS >2.1 strongly predicted reintubation. Multivariable logistic regression confirmed that gestational age <28 weeks (OR 0.14, 95% CI 0.03–0.61; p = 0.009) and RSS >2.1 (OR 0.09, 95% CI 0.02–0.44; p = 0.003) were independent predictors of extubation failure, while SBE duration was not independently associated with extubation outcome (p = 0.412).
Conclusion
In this hypothesis-generating retrospective study, a 3-min SBE demonstrated comparable performance to a 10-min SBE in predicting extubation success among preterm VLBW infants. Gestational maturity and RSS were stronger independent predictors of outcome. These findings require confirmation in larger prospective studies before definitive clinical recommendations can be made.
Keywords
Introduction
The survival of preterm infants has improved substantially due to advances in neonatal resuscitation, antenatal management, and modern intensive care practices.1,2 Nevertheless, determining the optimal timing for successful extubation remains a critical challenge, especially among very low birthweight (VLBW) and extremely low birthweight (ELBW) neonates who frequently demonstrate immature respiratory drive, deficient surfactant production, and reduced lung compliance.3,4 These physiological limitations contribute to prolonged ventilatory dependency, and nearly 70% of VLBW neonates require invasive ventilation during their NICU admission.5,6
Premature or unsuccessful extubation carries risks including atelectasis, sepsis, airway trauma, prolonged oxygen exposure, and increased mortality.7–12 Extubation failure, defined as the need for reintubation after planned extubation, occurs in approximately 20–30% of preterm infants and is linked to significant morbidity and long-term complications.13–15 Because of these risks, objective and reproducible methods to evaluate readiness for extubation are essential.
The Spontaneous Breathing Evaluation (SBE) is commonly employed to assess whether a mechanically ventilated infant can sustain adequate ventilation without mandatory support.2,16 The evaluation is typically performed using continuous positive airway pressure (CPAP) delivered through the endotracheal tube, allowing clinicians to observe the infant’s capacity for unsupported breathing. 17 Despite broad clinical use, the optimal duration of SBE remains undefined, with reported durations ranging from as brief as 3 min to as long as 30 min.18–20
Some studies indicate that early instability becomes evident within the initial 2–3 min of unsupported breathing, suggesting that prolonged evaluations may not significantly enhance prediction of successful extubation.6,21 Conversely, others argue that longer durations may reveal late fatigue or desaturation episodes.3,22 Given these differing perspectives, determining whether a short or extended SBE better reflects extubation readiness remains an important clinical question. Beyond SBE duration, other potential predictors of extubation readiness—including diaphragm function assessed by ultrasound, spontaneous minute ventilation, and ventilator parameters such as mean airway pressure and pressure support level—have been described in the literature, though their routine clinical application remains variable.6,22,23
The present retrospective observational study compared the performance of a 3-min versus a 10-min SBE in predicting extubation success among preterm infants weighing <1500 g. By analysing routinely collected clinical data, we sought to clarify whether a shorter evaluation is clinically adequate in this high-risk population.
Methods
Study design and setting
This retrospective observational study was conducted in the neonatal intensive care unit (NICU) of a tertiary referral centre in South India. Medical records from 1 January to 31 December 2018 were reviewed. The study protocol was approved by the Institutional Ethics Committee (IEC: 895/2017). Written informed consent was obtained from the parents or guardians of all enrolled neonates for participation and publication of anonymised clinical data. All procedures adhered to the ethical principles outlined in the Declaration of Helsinki (2013 revision). As the study involved retrospective analysis of routinely collected clinical information without a prospective intervention, registration in the Clinical Trials Registry of India was not required.
Participants
All preterm neonates born between 26 and 34 weeks of gestation, with birthweight <1500 g, who received invasive mechanical ventilation for at least 24 h and subsequently underwent a planned extubation, were screened for eligibility. Infants were included if clinical documentation recorded an SBE performed for either 3 min or 10 min as part of routine extubation readiness assessment. Based on SBE duration, infants were categorised into Group A (10-min SBE) and Group B (3-min SBE). Group allocation was determined by a change in unit protocol implemented mid-study: infants assessed in the first 6 months of 2018 underwent a 10-min SBE, while those assessed in the second 6 months underwent a 3-min SBE following protocol revision. All infants in both groups had to meet standard clinical readiness criteria prior to SBE, including haemodynamic stability, adequate spontaneous respiratory effort, acceptable blood gas parameters, and a ventilator rate of ≤10 breaths/min.
Infants were excluded if they had major congenital anomalies, haemodynamic instability at the time of assessment, self-extubation requiring immediate reintubation, or incomplete documentation related to SBE or extubation outcome.
SBE procedure and extubation protocol
SBE was performed on CPAP (5 cm H2O) delivered via the endotracheal tube. Clinical parameters—including heart rate, respiratory rate, and oxygen saturation—were recorded at baseline and at 3 min, and at 10 min when applicable. The RSS was calculated as FiO2 × mean airway pressure and was recorded immediately before the start of the SBE. SBE failure was defined by any of the following criteria: sustained oxygen desaturation (SpO2 <88% for >10 s), bradycardia (heart rate <100 beats/min), apnoea requiring stimulation, or a requirement for an increase in FiO2 >0.1 above baseline. The decision to proceed with extubation was based on SBE performance in conjunction with additional clinical criteria, including stable ventilatory settings (peak inspiratory pressure ≤16 cm H2O, mean airway pressure ≤8 cm H2O, FiO2 ≤0.35), acceptable blood gas parameters, and attending clinician judgment. Infants who failed the SBE were not extubated and returned to their prior ventilator settings for further assessment.
Caffeine citrate was administered to all infants before extubation according to unit protocol. After extubation, all infants were supported with nasal CPAP (FiO2 21–35%, PEEP 5 cm H2O) as the primary mode of post-extubation non-invasive respiratory support. Non-invasive positive pressure ventilation (NIPPV) was used selectively at the clinician’s discretion in infants with recurrent apnoea or signs of respiratory insufficiency following extubation.
Extubation success was defined as remaining extubated without the need for reintubation for at least 72 h following a planned extubation. Extubation failure was defined as the requirement for reintubation within 72 h. For this retrospective analysis, perinatal characteristics, ventilatory settings, Apgar scores, antenatal exposures, SBE tolerance, post-extubation respiratory support, and reintubation events were extracted from electronic and paper medical records.
Outcomes
The primary outcome was extubation success within 72 h of planned extubation. Secondary outcomes included SBE tolerance (pass/fail), physiological stability during SBE, and the association of gestational age, birthweight, and RSS with extubation success.
Statistical analysis
Data were entered into Microsoft Excel and analysed using IBM SPSS Statistics version 27. Continuous variables were expressed as mean (standard deviation, SD) with 95% confidence intervals where appropriate, and categorical variables as frequencies and percentages. Comparisons between the 3-min and 10-min SBE groups were performed using independent-sample t tests for continuous variables and χ2 or Fisher’s exact tests for categorical variables. p values and 95% confidence intervals are reported throughout.
To explore independent predictors of extubation failure, a multivariable binary logistic regression model was constructed. Variables with univariate p < 0.10 were included: gestational age (<28 vs ≥ 28 weeks), birthweight (<1000 g vs ≥1000 g), RSS (>2.1 vs ≤2.1), and SBE duration (3 min vs 10 min). Results are expressed as odds ratios (OR) with 95% confidence intervals. Repeated-measures ANOVA was used to evaluate intra-group changes in physiological parameters across SBE time points, and two-way repeated-measures ANOVA assessed interactions between SBE duration and time. A p value <0.05 was considered statistically significant.
Results
During the study period, 620 preterm neonates born at <34 weeks’ gestation and weighing <1500 g were admitted to the NICU (Figure 1). Of these, 330 required invasive mechanical ventilation. After excluding infants with haemodynamic instability (n = 56), ventilation for <24 h (n = 176), and self-extubation requiring immediate reintubation (n = 10), a total of 88 infants met eligibility criteria for the study. All underwent a Spontaneous Breathing Evaluation (SBE) prior to planned extubation, with 44 receiving a 10-min SBE (Group A) and 44 receiving a 3-min SBE (Group B). Study flow diagram showing participant screening, allocation, and outcomes.
Demographic and perinatal characteristics of study groups (n = 88).

SBE, spontaneous breathing evaluation; RDS, respiratory distress syndrome; SD, standard deviation; IQR, interquartile range. Percentages are column percentages. p values derived from Student's t test for continuous variables and χ2 or Fisher’s exact test for categorical variables. Statistical significance defined as p < 0.05.
Pre-extubation ventilator parameters and vital parameters during spontaneous breathing evaluation.

SBE, spontaneous breathing evaluation; SpO2, peripheral oxygen saturation; SD, standard deviation; RSS, Respiratory Severity Score = FiO2 × mean airway pressure, recorded immediately before SBE; FiO2, fraction of inspired oxygen. *Significant at p < 0.05. 95% CI reported for between-group comparisons.
SBE outcome and extubation success/failure within 72 h.
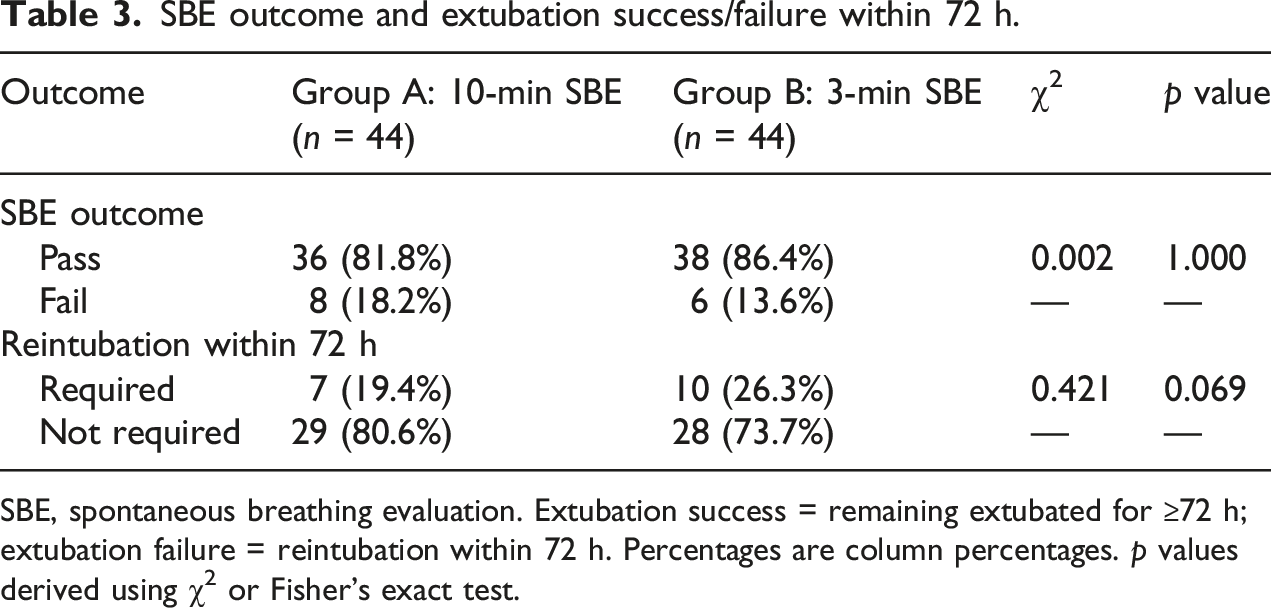
SBE, spontaneous breathing evaluation. Extubation success = remaining extubated for ≥72 h; extubation failure = reintubation within 72 h. Percentages are column percentages. p values derived using χ2 or Fisher’s exact test.
Extubation outcomes and predictors of extubation failure across spontaneous breathing evaluation duration groups.
Univariate analysis of predictors of extubation outcome among preterm VLBW infants.

Extubation success = remaining extubated for ≥72 h. Extubation failure = reintubation within 72 h. OR, odds ratio; CI, confidence interval; RSS, Respiratory Severity Score (FiO2 × mean airway pressure). *Significant at p < 0.05. RSS categories: 1.4–2.1 (n = 71) versus > 2.1 (n = 17).
Multivariable logistic regression analysis of independent predictors of extubation failure.

OR, odds ratio; CI, confidence interval; RSS, Respiratory Severity Score; SBE, spontaneous breathing evaluation. Model adjusted for gestational age, birthweight, RSS, and SBE duration simultaneously. *Significant at p < 0.05.

Forest plot displaying adjusted odds ratios (aOR) and 95% confidence intervals (CI) from multivariable logistic regression analysis of independent predictors of extubation failure.
Reintubation rates by gestational age and birthweight subgroups according to SBE duration.

GA, gestational age; BW, birthweight; SBE, spontaneous breathing evaluation. p values derived using χ2 or Fisher’s exact test comparing reintubation rates between SBE groups within each subgroup. *Significant at p < 0.05.
Discussion
In this retrospective study of preterm VLBW infants, 3-min and 10-min SBEs demonstrated comparable performance in predicting extubation success. Most infants were VLBW and nearly one-third were ELBW, reflecting the typical profile of preterm neonates requiring mechanical ventilation and extubation attempts in tertiary NICUs.3,16 The overall extubation success rate of 77% is consistent with published neonatal cohorts, supporting the external validity of these findings.6,23
The most important methodological consideration in this study is the allocation of infants to SBE duration groups. Group allocation was not based on clinical severity or clinician preference but on a temporal protocol change: infants assessed in the first half of 2018 underwent a 10-min SBE and those in the second half underwent a 3-min SBE. This design reduces individual selection bias, though temporal confounding remains possible. Notably, the 10-min SBE group had a significantly higher RSS at baseline (p = 0.031), suggesting that these infants had modestly greater respiratory severity at the time of extubation assessment. This imbalance was accounted for in the multivariable logistic regression model, which confirmed that SBE duration was not an independent predictor of extubation outcome after adjustment for RSS and gestational age.
The mechanisms leading to SBE failure and extubation failure in this cohort—bradycardia, oxygen desaturation, and increasing respiratory distress—mirror those described in previous studies. 22 These events reflect the intrinsic vulnerabilities of preterm infants, including immature respiratory drive, poor airway tone, and limited pulmonary reserve. Notably, most SBE failures occurred within the first 3 min of the evaluation, regardless of the assigned SBE duration. This observation is physiologically plausible: early failure during unsupported breathing likely reflects these fundamental limitations of extremely preterm respiratory physiology. Kamlin et al. similarly reported that most preterm infants who could not tolerate spontaneous breathing assessments failed within the first 90 s. 6 Together, these findings provide a mechanistic rationale for the potential utility of shorter SBE durations in this population.
Gestational age and RSS emerged as independent predictors of extubation failure on multivariable analysis. Infants born at <28 weeks and those with RSS > 2.1 had significantly higher odds of extubation failure, whereas birthweight did not reach significance independently, likely due to collinearity with gestational age. These findings align with prior literature: Hermeto et al. reported higher failure rates among smaller and less mature infants, 16 and Mhanna et al. demonstrated that RSS is a meaningful marker of respiratory severity and extubation readiness. 22 RSS is particularly appealing because it integrates oxygenation and ventilatory support into a single bedside metric (FiO2 × mean airway pressure). The finding that RSS remained a significant independent predictor even after adjusting for gestational age suggests it captures additional prognostic information about respiratory severity at the time of extubation.
Beyond these measures, emerging evidence supports the role of other extubation readiness predictors, including diaphragm thickening fraction assessed by ultrasound, spontaneous minute ventilation, and ventilator weaning parameters such as pressure support level.6,22,23 These were not systematically assessed in the present cohort due to the retrospective design, and their integration with SBE-based assessment represents a promising area for future prospective investigation.
Antenatal corticosteroid exposure was documented in nearly half of the infants, with no significant difference between groups. While antenatal steroids accelerate pulmonary maturation and reduce respiratory morbidity, 21 our findings—consistent with those of Mhanna et al. 22 and Chawla et al. 23 —indicate that steroid exposure alone does not guarantee extubation success once infants require invasive ventilation. The severity of acute respiratory compromise at the time of extubation assessment appears to be a stronger determinant of outcome than prior steroid exposure.
Post-extubation management was standardised across both groups: all infants received nasal CPAP (PEEP 5 cm H2O, FiO2 21–35%) as the primary mode of non-invasive support following extubation, and caffeine citrate was administered to all infants prior to extubation per unit protocol. NIPPV was used selectively for infants demonstrating apnoea or respiratory insufficiency following extubation. This consistency in post-extubation management reduces the likelihood that differences in respiratory support confounded the comparison of extubation outcomes between groups.
Clinically, these findings suggest that a shorter SBE may not be inferior to a longer evaluation in preterm VLBW infants. In addition to reducing the duration of unsupported breathing, a brief SBE could reduce physiological stress for extremely preterm infants during extubation readiness assessment. Incorporating RSS alongside SBE performance may further enhance clinical prediction. 24 However, it is important to emphasise that the present study is hypothesis-generating. The retrospective design, modest sample size, single-centre setting, and potential temporal confounding limit the strength of conclusions. The RSS imbalance between groups, although addressed statistically, cannot be fully excluded as a confounder. Definitive clinical recommendations should await confirmation from larger prospective, preferably randomised, multicentre studies.
Strengths of this study include a clearly defined cohort, strict eligibility criteria, systematic data extraction, standardised post-extubation support protocols, and the addition of multivariable analysis adjusting for key confounders. Limitations include the single-centre retrospective design, modest sample size, absence of prospective randomisation, and potential unmeasured confounders between the two temporal periods. Exclusion of infants with major congenital anomalies may also underestimate extubation failure rates in broader clinical populations.
Conclusion
In this retrospective study of preterm VLBW infants, 3-min and 10-min SBEs performed comparably in predicting extubation success. Gestational maturity and respiratory severity score were independent predictors of extubation failure, while SBE duration was not independently associated with outcome on multivariable analysis. These findings are hypothesis-generating and require confirmation in larger prospective studies. Pending such evidence, the integration of SBE performance with RSS and clinical maturity indicators appears to be a clinically rational approach to extubation decision-making in this high-risk population.
Footnotes
Acknowledgements
The authors sincerely thank the medical, nursing, and respiratory therapy teams of the Neonatal Intensive Care Unit, Kasturba Medical College, Manipal, for their dedicated clinical care and meticulous documentation. We acknowledge the hospital medical records department for data retrieval, the institutional biostatistics support team for statistical guidance, and the families of the neonates whose anonymised clinical data contributed to this research.
Ethical considerations
The study was approved by the Institutional Ethics Committee, Kasturba Medical College, Manipal (Approval No. 895/2017).
Consent to participate
Written informed consent was obtained from parents or legal guardians. All procedures were conducted in accordance with the 2013 revision of the Declaration of Helsinki.
Author contributions
JG: study conceptualisation, design, data interpretation, manuscript drafting, critical revision. PCS: study design, statistical oversight, manuscript co-drafting, critical revision. MSJ: data collection, organisation, preliminary analysis, manuscript preparation. JP: study supervision, clinical interpretation, critical manuscript revision. SK: results interpretation, methodological refinement, critical manuscript review. All authors approved the final manuscript and meet ICMJE criteria for authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author upon reasonable academic request, subject to Institutional Ethics Committee approval.