
Abstract
Introduction
Admission of an infant to the neonatal intensive care unit (NICU) is a stressful event for parents. The physical separation and inability to hold their child due to minimal handling protocols or infection control such as in the recent COVID-19 pandemic is a major contributor to parental stress. Knowledge on a contact-free parent administered intervention to reduce the stress of parents whose infant necessitates neonatal intensive care is lacking.
Objective
To assess the effect of a contact-free, Story-Telling Attention-Refocusing (STAR) intervention on the acute stress of parents whose infant is in the NICU.
Methods
A block-randomized controlled single-blind trial was conducted in a level II–III NICU. Parents in the experimental group provided the STAR intervention which consisted of designated prompts to share stories with their infants over a ten-minute period, three times per week, for 1 week. Parent acute stress was measured using the PSS:NICU questionnaire before and after the STAR intervention period, and differences in acute stress between mothers and fathers were assessed as well as parent satisfaction.
Results
Twenty-one parents completed the study. Results revealed that overall PSS:NICU stress scores lowered significantly within the intervention group (p = 0.04), and the intervention mediated acute stress of mothers and fathers differently (p = 0.01). Parents reported feeling overall satisfied with the STAR program and they felt less stressed in the hospital and more connected to their infants.
Conclusion
The STAR program provides parents a unique opportunity to interact with their infant in a positive meaningful manner and may reduce acute stress in parents during their infants NICU stay.
Introduction
Admission of an infant to the neonatal intensive care unit (NICU) can be an extremely stressful event for parents with long-term negative effects on parent well-being, infant development, and infant–parent relationship. 1 Acute stress is defined as a short-term physiological or psychological response to an intrusive event that causes individuals to perceive environmental demands to exceed their adaptive capacity.2,3 One such event is childbirth, which can be an acute stressful event for parents, even when there are no complications. 4 With the addition of preterm labour and delivery along with admission to the NICU, preterm birth can be even more stressful for parents. The admission of an infant to the NICU disrupts the normative transition into parenthood 5 and has far-reaching consequences for parents, infant development, and the parent–infant relationship. 6 The stress from admission can also persist after discharge from the NICU and has been shown to lead to symptoms of depression and anxiety among parents. 7
Prevalence of some acute stress symptoms is nearly universal after NICU admission. A study by Morparia et al. (2019) found that approximately 30% of parents reported symptoms of acute stress, and 20% of parents met the diagnostic criteria for acute stress disorder within 48 hours of NICU admission. 8 Although there are several sources of stress for parents with infants in the NICU, a major source of stress for parents is feelings of isolation from their infants due to barriers in the environment that prevent parent–infant interactions. 9 For instance, an inability to directly hold and care for their infant, such as when minimal handling protocols are implemented in the NICU to reduce the incidence of adverse medical outcomes, is a period of high stress for parents.10,11 Similarly, during the COVID-19 pandemic NICU family visitation policies and parent–infant interaction were restricted to reduce contagion. 12 A qualitative study by Yance et al. (2023) found that the pandemic decreased opportunities for parental care in the NICU, leading to feelings of loneliness and distress amongst new parents. 13 In particular, the study noted parent–infant separation as a major factor in inducing stress symptoms amongst parents in the NICU, recommending that ‘hospitals should… establish ways for parental engagement to be made possible without risk of infection’. 13 The physical environment of the NICU has also been identified by parents as a source of stress, including the bright lights, sounds of monitors, and seeing tubes attached to their infants are all factors that increase parental stress. 14
According to the theory of allostasis and allostatic load by McEwen (2004), failure to deal with stressors or stressful events leads to accumulation of repeated stress, which causes ‘wear and tear’ over time. 15 In this model, individual differences and environmental stressors affect an individual’s level of perceived stress, which can then affect behavioural and physiological responses and, over time, creates an allostatic load. An allostatic load is a continuous activated stress response state, which can influence the morbidity and mortality of an individual by influencing the neurophysiological processes in the body. 15 The stress of childbirth, prematurity, and admission to the NICU can be considered environmental stressors in this case that could affect perceived stress. High levels of perceived stress could then affect parenting behaviours and influence parent–infant relationships as a result. All these factors combined over the period of NICU admission could then result in an allostatic load for parents that can affect not only their relationship with their infants, which can then have downstream effects on infant development, but also their physical and mental health. A parent-administered intervention in the NICU could act as a moderating variable that minimizes the negative effects of environmental stressors on perceived stress. By minimizing the negative effects from that relationship, the intervention could potentially moderate how stress affects parenting behaviours, particularly if the intervention helps parents feel closer to their infants. This could then moderate the physiological responses that result from continuous stress and thus lower the allostatic load on parents. This is in line with evidence that suggests protective factors such as parental bonding, positive affect, and social support can mitigate the negative effects of allostatic load. 16 A parent-administered intervention could elicit these same protective factors and reduce the potential of parents developing allostatic load from NICU admission.
Considering the high occurrence of infants who are admitted to the NICU and the considerable stress parents endure during such times, particularly exacerbated during periods of non-contact, it is imperative to develop contact-free intervention targeting these critical periods to alleviate acute parental stress. Such interventions hold promise for enhancing outcomes for both parents and infants. Despite numerous studies exploring interventions’ effect on parental stress in the NICU, in a recent scoping review we observed a notable gap in research regarding the availability of contact-free interventions to reduce parent stress. 17 Moreover, a meta-analysis conducted by Sabnis et al. on parental stress studies in the NICU (2019) found that only 19 out of 58 studies (32%) included fathers as well as mothers, and that many of these studies failed to report specific outcomes for fathers. 18 This means that much of what we understand about parental stress is largely based on biological mothers only. Hence, this study aims to address the research gap by developing and testing a contact-free intervention aimed at reducing the stress of both parents.
Objective
The goal of this research study is to assess the effect of a contact-free Story-Telling Attention-Refocusing intervention on acute stress of parents during their infant’s stay in the NICU.
Methods
Study design
A block randomized, single-blind, clinical trial was conducted in a level II and III NICU at Kingston Health Sciences Centre (KHSC), Kingston, ON, Canada (NCT 0383632). Block randomization by group was used to ensure blinding of neonatal providers and participants to minimize cross-contamination. A block size of nine per arm was instituted wherein nine participants were assigned to the experimental group, and the proceeding nine participants were assigned to the control group. A computer-generated algorithm determined the sequence for the randomization block allocation.
Setting
The NICU at KHSC consists of a maximum of 26 beds and provides an interdisciplinary approach to standard care based on the Family-Integrated Care (FiCare) model. The interdisciplinary team consists of neonatologists, nurses, dietitians, occupational therapists and social workers. As part of the FiCare approach parents are encouraged to attend daily medical rounds, are active participants in the medical decision-making, and are invited to perform daily self-care tasks such as changing the diapers, feeding, and bathing their child. In addition, as part of the standard care, the unit has a minimal handling protocol, which specifies avoiding several routine medical examinations as well as parent contact within the first 72 hours of life for very low birth weight preterm infants. The rationale for the minimal handling protocol is to decrease stress responses, which can increase cerebral blood flow and thus increase the chance of brain injury in premature infants. Furthermore, throughout the infant’s hospitalization the unit practiced ‘clustered-care’ which consists of grouping several medical or nursing care procedures performed together instead of spacing them out over time. The main goal of clustering care is to allow the infants to rest for longer periods and avoid handling and disturbing their sleep pattern.
Notably, this study was initiated in March 2022 when COVID-19 pandemic related hospital policies were in place at KHSC to reduce infection. When recruitment began for this study, only one visitor was permitted to visit for a three-hour period only. The visitor was required to show proof of vaccination and perform a rapid antigen test each time they came into the hospital. This policy changed throughout the COVID-19 pandemic and study period wherein visiting hours were gradually increased and by February 2023 mandatory screening was not required, and both parents were permitted to visit at any time (24-hour open visitation policy), though there were still restrictions for those who were not registered visitors. The study was approved by the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (HSREB).
Participants
Parents meeting the following eligibility criteria were enrolled: (1) were over the age of 18, (2) were deemed as the primary decision-makers per KHSC policies, and (3) whose infant was born infants <34 weeks and were admitted to the NICU. These eligibility criteria were selected because of the increased likelihood of parents experiencing prolonged periods of separation from their child.
Intervention: Story-Telling Attention Refocusing (STAR)
The STAR program was developed as a contact-free program aimed at enhancing parent–infant interaction to reduce parent stress. The STAR intervention is based on evidence that suggests positive memory recall, or attention-refocusing, has been found to lower cortisol and mood responses to acute stress in humans, 19 as well as attenuate sadness in depressed adults. 20 It is also based on the findings from our previous scoping review which indicates that parent-administered interventions are an effective approach to reduce parental stress in the NICU. 17
The program components and duration were adopted from previous evidence-based programs. 17 The STAR program consisted of a 10-minute contact-free parent–infant verbal interaction, three times over a course of a week. Specifically, participants were asked to speak to their infants continuously over a ten-minute period, while their baby remained in the crib. Participants were asked to avoid touching the infant, while maintaining eye contact with them, to isolate the effects of the intervention. Parents were provided with written instructions and prompts encouraging them to talk about stories related to themselves or their families. They were asked to talk in their native language, since studies have shown that infants as young as 2 days old show a preference for and sensitivity to their mother’s native language.21,22 The program was administered for 10-minute after or before clustered-care, for 3 days, within a 7-day period to allow time for parents who may not always be available. Participants were asked to keep a record on a log sheet each time the intervention was completed.
Both parents were invited, if feasible, to participate in the study and attend the one training session. The training session consisted of the researcher providing the parents with written and verbal instructions on the STAR program administration and completion of the log sheet.
Outcome measures
The primary outcome, acute stress, was defined as level of perceived stress of parents whose infant necessitates neonatal intensive care. The Parental Stressor Scale: Neonatal Intensive Care Unit (PSS:NICU), developed by Miles et al. (1993) was used to monitor parental stress. 23 The PSS:NICU is a 5-point Likert scale that has been extensively used to measure stress in the NICU. There are three subscales: 1. sights and sounds, 2. looks and behaviour, and 3. parental role alterations. The scale was scored using the overall stress level, which includes all items on the scale when the mean score is calculated. 23
The secondary outcomes included acute stress 24 outcomes between mothers and fathers using the PSS:NICU assessment because the literature highlights a differential effect of parental stress interventions in mothers and fathers. 18 Satisfaction with the STAR intervention was also assessed after completion of the program, using anonymous written questionnaire adopted from Holditch-Davis and colleagues (2014). 25
Covariates
A form collecting parent demographic information was administered to participants to ensure results were not influenced by the following variables: age, gender, ethnicity, level of education, employment status, gross family income, children at home, social support, means, and time to travel from the hospital dwelling distance from hospital and social support, since these have been found to be correlated with levels of stress in adults.1,12,26,27 The following infant variables were collected via a medical chart review: gestational age, birth weight, neonatal morbidities, twin, first born, sex, means days on endotracheal tube (ETT), mechanical ventilation, and continuous positive airway pressure (CPAP) as these factors have been found to be associated with increased parental stress.1,12,26,27
Procedure
The researcher reviewed the NICU admissions binder to identify parents and infants that met the inclusion criteria and then reviewed the charts of all potential candidates. All eligible potential participants were initially contacted via telephone when infants were clinically stable to introduce the study and set up an in-person meeting for recruitment. All participants provided written informed consent prior to participating. After written consent was obtained, participants were randomized into the experimental or control group according to the random block allocation. The researcher trained the parents in the experimental group prior to the start of the STAR program. Parent–infants in the experimental group administered the STAR program three times over a 7-day period. The intervention frequency aligned with COVID-19 parental visitation policies during the study recruitment period. Parent–infants in the control group were exposed to standard care only. The outcome measure, PSS:NICU, was administered pre- and post- interventions for both groups by the researcher. The satisfaction survey was disseminated after the completion of the STAR intervention.
Data analysis
An a priori power analysis was conducted to establish sample size, with the mean PSS:NICU score of the reference group being 3.0, the mean of the test group being 2.0, and standard deviation at 0.7, with a power of 80% and alpha value of 0.05. This produced a sample size of 9 per group, for a minimum sample size of 18. However, an additional 30% of participants were recruited to account for missing data, for a total targeted sample size of 28 (14 per group).
Independent samples t-tests and chi-square tests were used to examine whether the continuous and categorical characteristics of participants in the control and experimental groups were equivalent at baseline. Descriptive statistics in the form of means with standard deviations were first calculated for both the PSS:NICU. An unbalanced repeated measures ANOVA was then conducted to compare within and between-group differences in mean pre-test and post-test PSS:NICU total and subscale scores in the control and experimental group. The group*time interaction effect was also assessed to test whether there was a habituation effect of staying in the NICU that would lower parental stress in both groups. A secondary analysis, which involved a repeated measures ANOVA, was conducted to compare differences in the mean PSS:NICU total and subscale score between mothers and fathers. Satisfaction with the STAR intervention was descriptively assessed. IBM SPSS version 28.0 was used to perform the statistical analysis, with an alpha value of 0.05.
Results
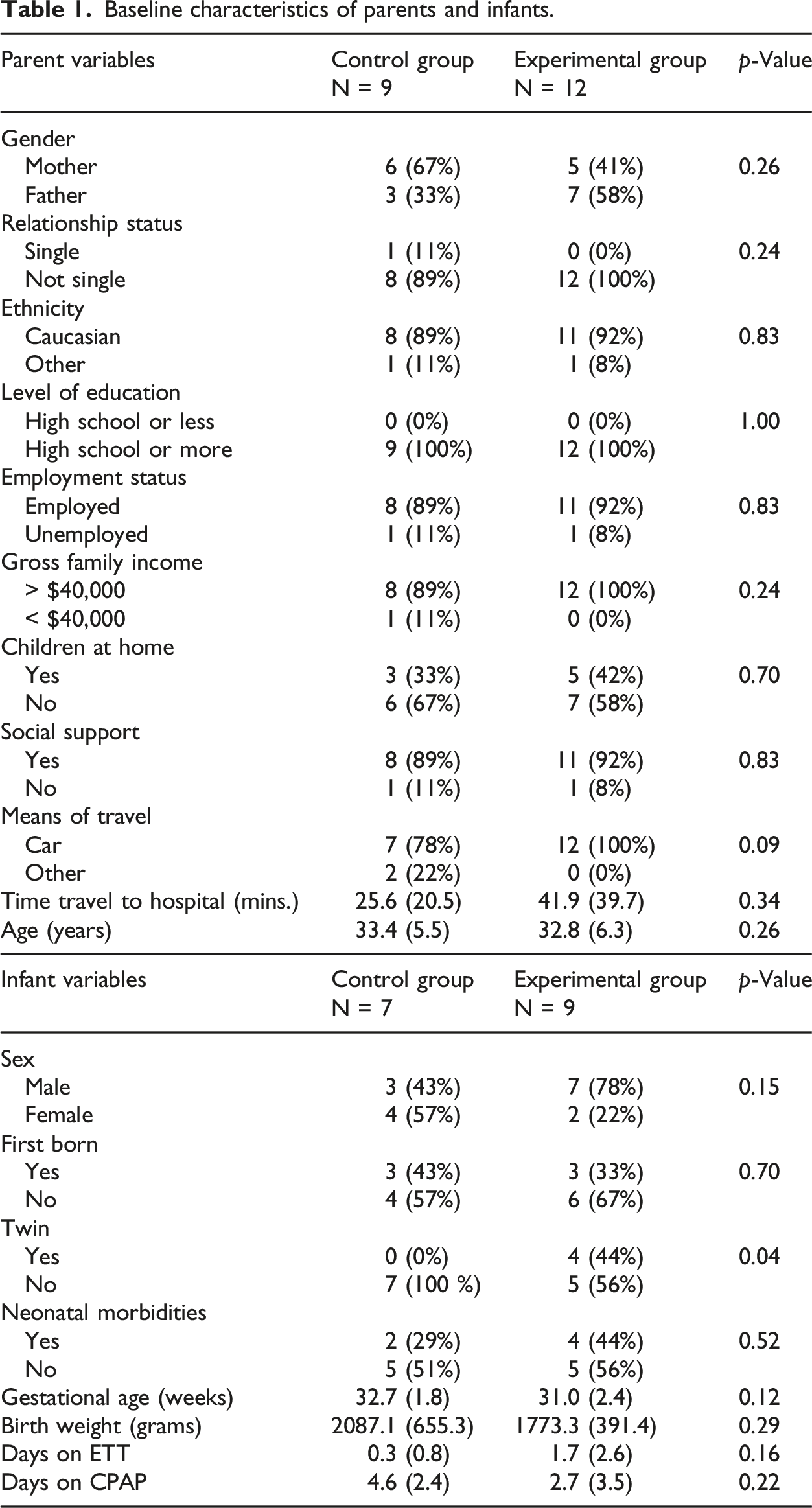
Baseline characteristics of parents and infants.
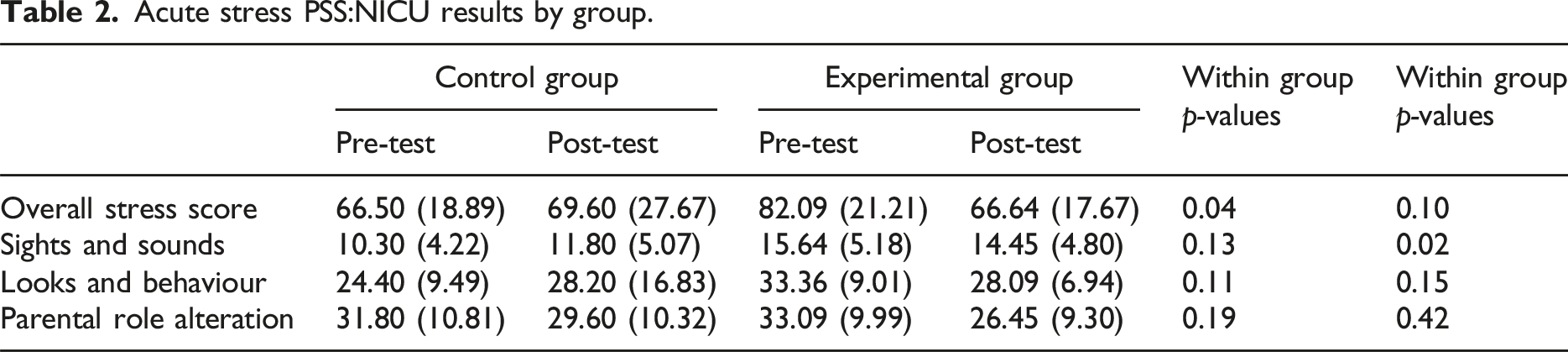
Acute stress PSS:NICU results by group.
Stress PSS:NICU results by parent relation.
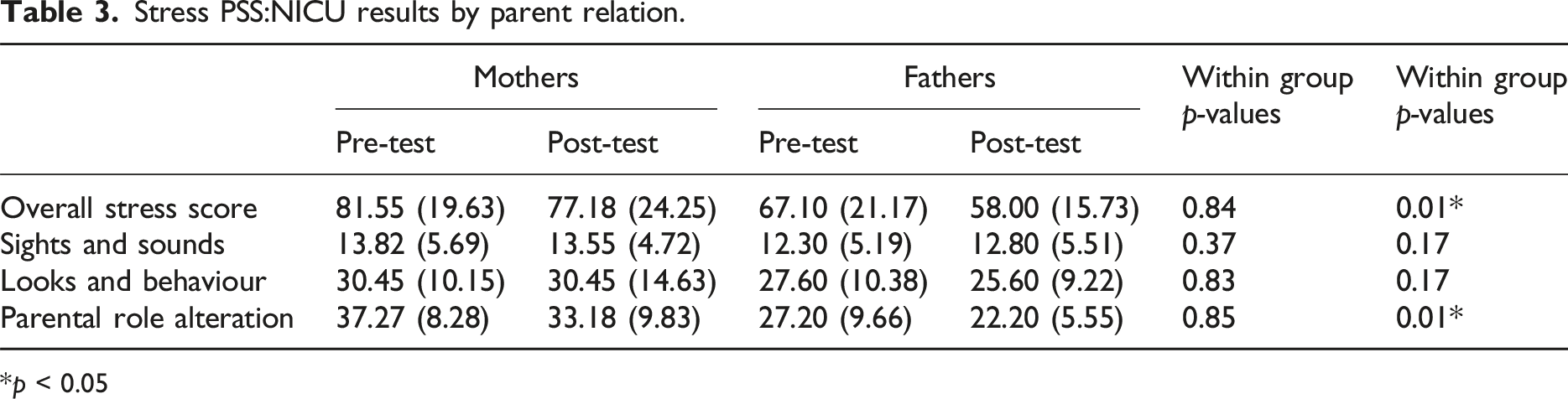
p < 0.05
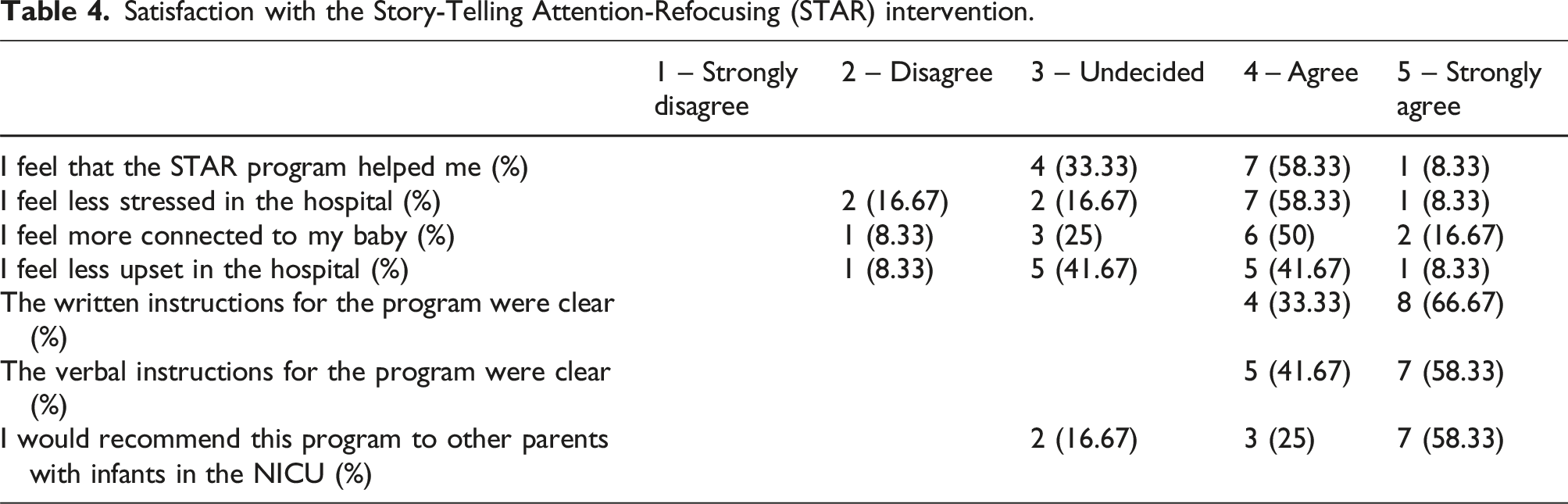
Satisfaction with the Story-Telling Attention-Refocusing (STAR) intervention.
Discussion
Admission of infants to the NICU is a stressful event for parents and can have far-reaching consequences on both parental and infant well-being. This study aimed to assess the effect of a contact-free intervention, the STAR program, on acute stress in parents during their infants’ stay in the NICU.
The findings from this study suggest that the STAR intervention may have been effective at lowering overall parental stress. Results revealed that parents who participated in the STAR program showed significantly reduced parental stress as measured by the pre- and post- PSS:NICU overall Stress Score compared to those in the control group. Moreover, there was no significant group*time interaction effect indicating that it was unlikely that the changes in stress were due to habituation to the NICU environment over time. The effectiveness of the STAR intervention in reducing parental stress is likely due to three reasons: first, the primary source of stress for parents in the NICU comes from limited physical contact with their infants. 12 As such, an intervention that empowers parents to actively participate in bonding with their infant may help reduce feelings of stress and helplessness in the NICU; second, the STAR intervention goes beyond what is considered to be standard care (i.e. bathing and feeding the infant) and may help parents feel more engaged in their parenting roles in a time where they may feel lost; and lastly, the perceived benefit of auditory interventions on infant development may also help reduce stress for parents. The literature supports storytelling as an effective method to foster language, brain, and emotional development in infants and children.28–30 Hence, if parents are concerned with their infant’s developmental outcome, a parent-administered intervention that is perceived to promote infant development may in turn help reduce parent stress. The satisfaction survey indicated that the majority of parents agreed that the STAR intervention helped them feel less stressed at the hospital and feel more connected to their infants. The addition of parents perceived benefits and satisfaction with the STAR program may have contributed to reduction on parent stress within the experimental group.
The sights and sounds subscale of the PSS:NICU showed the only significant difference between the two groups. The difference in the sights and sounds subscale is likely due to differing infant characteristics between the two groups. There was a statistically significant difference in the presence of twins, where there were two pairs in the intervention group and none in the control group. This is consistent with previous research conducted in the NICU which suggests that twin delivery is significantly associated with a higher PSS:NICU score as compared to single infant delivery. Moreover, there was a clinical difference between mean days on endotracheal tube (ETT) between infants in both groups, showing a slightly higher average for those in the experimental group than those in the control group. Since ETT is an invasive procedure which can be visually distressing to parents, it is likely that this clinical difference also contributed to the significant between-group difference in the sights and sounds subscale score.
Previous literature found a differential effect of NICU parental stress interventions on mothers compared to fathers, 24 which led to a secondary data analysis of the results factoring in relation to child. The results showed a significant difference in stress levels for fathers compared to mothers. Mothers showed higher pre-test and post-test PSS:NICU overall stress scores and Parental Role Alteration scores, regardless of if they were in the experimental or control group. This is consistent with previous studies which suggest that while mothers and fathers both experience stress in the NICU, mothers may be more distressed by certain aspects of the experience. 31 A study conducted by Miles et al (1992) showed a similar pattern of results – mothers showed significantly higher overall stress scores and the Parental Role Alteration subscale compared to fathers. This was likely due to mothers are more stressed than fathers regarding being physically separated from their child and the loss of the caregiving role with the infant due to neurobiological processes related to pregnancy and labour that trigger caregiving instincts. 32 This study also showed that the STAR intervention affected mothers and fathers differently. While the overall level of distress was higher for mothers, the magnitude of impact for the intervention was greater for fathers, further supporting the need for more diverse representation in research on parental interventions in the NICU.
Although the minimum sample size was met, the sample of the study was relatively small and limited to preterm infants only. Hence, this limits the generalizability of the study results. Overall, while this study provides a starting point for the STAR intervention, research with larger and diverse sample is needed to confirm the study findings.
Conclusions
The findings suggest that the STAR intervention, a non-contact, storytelling intervention, may help to lower parental stress by offering a way for parents to bond with their infants in a safe and engaging way beyond standard care. Moreover, this study corroborated previous literature that found that parental stress interventions are experienced differently by mothers compared to fathers, supporting the need for inclusive interventions.
Statements and declarations
Footnotes
Acknowledgements
We thank all the parents who participated in this study, Ms. Wilma Hopman for her statistical expertise, and all the KHSC neonatal nurses for their assistance.
Author contributions
Anisia Wong: conceptualization, participant recruitment, ethical submission, trial documentation, data collection, data analysis, writing, reviewing, and editing. Sandra Fucile: conceptualization, data analysis, reviewing, and editing the final manuscript.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an Operating Grant: Early Career Investigator Grants in Maternal, Reproductive, Child & Youth Health, Canadian Institute of Health Research [404710].
Ethical approval
Prior to recruitment, full ethical approval was obtained from the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (HSREB) [TRAQ #: 6025825]. All procedures performed in the study involving human participants were in accordance to the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.