
Abstract
Background
The practice of oil pulling has been used for centuries in Ayurvedic medicine and has garnered increased interest as a viable alternative to chemical mouthwash products that maintain oral health in recent years. This study aims to evaluate the efficacy of natural oils as a replacement for chlorhexidine (CHX) mouthwash in treating plaque-induced gingivitis among young adults.
Methods
A total of 90 subjects aged 18–40 years old with plaque-induced gingivitis were recruited for this study and randomly allocated into three treatment groups (30 participants per group). The study design was a randomized controlled trial with clinical assessments of participants’ plaque-control record (PCR), gingival bleeding index (GBI), and STAIN scores collected at baseline, 7, 14, and 21 days. Inter-group and intra-group differences were evaluated using ANOVA with post-hoc Bonferroni corrections and Chi-square tests at the p < 0.05 level.
Results
All three treatment groups showed a statistically significant decrease in intra-group PCR and GBI scores (p < 0.001). On day 21, the PCR scores decreased by 32.9% in the CHX group, 27.6% in the myrrh group, and 26.4% in the olive oil group. The highest reduction in gingival bleeding was observed in the CHX group (36.3%), the myrrh group (30.1%), and the olive oil group (20.2%). There was a statistically significant difference between the CHX and the olive oil groups (p = 0.006), with the CHX group demonstrating greater improvement than either of the natural oil groups.
Conclusion
In comparison to the natural oil pulling agents, CHX was the most effective at decreasing plaque-induced gingivitis. Natural oils provide clinically meaningful benefits, indicating they can play an important role alongside traditional oral hygiene regimens. Additional long-term research is required to assess the effectiveness of natural oils as substitutes for traditional chemotherapeutic agents.
Introduction
As a chronic, multifactorial inflammatory condition primarily caused by microbial biofilms, periodontal disease affects the hard and soft tissues that support the teeth, including the gingiva, periodontal ligament, and alveolar bone.1,2 Gingivitis is the most common of the various periodontal diseases. All ages can be affected, but there is an increased incidence of gingivitis in adolescents, young adults, and older adults. There is also a strong association between gingivitis and poor oral hygiene. Plaque-induced gingivitis can be reversed with proper plaque control and proper oral hygiene, but if left untreated, it can become a major public health issue and a known precursor to periodontitis.3,4 Diagnosing plaque-related conditions, such as gingivitis, and then developing easy-to-use, safe, effective and well-tolerated therapies for long-term use for plaque-related conditions, like gingivitis, will have major clinical implications.
Chlorhexidine mouthwash has long been used for its broad-spectrum antibacterial properties, which help to decrease plaque and prevent gingivitis. However, negative side effects like as mucosal irritation, taste anomalies, and tooth discolouration have been associated to its use. 3
Natural oil pulling has grown more popular as an auxiliary dental care treatment in recent years. Swishing oil—usually coconut or sesame oil—in the mouth for a few minutes is known as “oil pulling,” and it is supposed to help with gum inflammation, plaque, and bad breath. According to some studies, oil pulling may help reduce plaque growth and Streptococcus mutans levels.4,5
Even though oil pulling is becoming more popular, there isn't much scientific evidence that it effectively prevents plaque-induced gingivitis, especially in young individuals. Furthermore, there aren't many research comparing the effectiveness of oil pulling and chlorhexidine in treating gingivitis and plaque.6,7
Chlorhexidine has been identified as an appropriate chemotherapeutic agent when used as a mouthwash at a concentration of 0.2%. It is accepted as an efficient plaque-reducing agent and a preventive agent for Periodontal Diseases. However, its use has been linked to a variety of adverse effects, including taste changes, burning sensations, gingival irritation, and tongue and tooth discoloration. These unwanted side effects hinder the long-term efficacy and patient acceptability of CHX mouthwashes. Thus, the hunt for alternatives continues, with a move towards biogenic agents.8,9
Herbal remedies originating from botanical sources have been used in dentistry for many years to suppress germs, reduce inflammation, soothe irritation, and relieve pain. Among these herbal mouthwashes used to reduce inflammation and relieve pain are Myrrh and virgin olive oil Mouthwashes, but their clinical effectiveness needs to be evaluated. 10
Recent concerns about the negative impact of prolonged chlorhexidine use (eg, tooth discoloration, altered taste, mucosal irritation) have generated increased interest in natural alternatives for controlling plaque/harmful gingival inflammation. Examples of these products are coconut oil and tea tree oil, both of which have shown antimicrobial and anti-inflammatory benefits that may aid in supporting gingival health. Coconut oil, containing lauric acid, disrupts the structural integrity of bacterial cells and alters host inflammatory responses. Evidence suggests that coconut oil can reduce plaque accumulation and associated gingival inflammation when used for oral hygiene. In addition, tea tree oil has broad antimicrobial activity and has been the subject of multiple randomized clinical trials, demonstrating equal efficacy to chlorhexidine with fewer adverse side effects.11,12
Furthermore, myrrh and olive oil, as oil-pulling agents, have attracted research attention for their antimicrobial, anti-inflammatory, and antioxidant effects. Historically, myrrh has been used in oral care formulations to reduce gingival inflammation and inhibit the growth of microorganisms associated with periodontal disease. Similarly, when using extra virgin olive oil varieties high in polyphenols, studies have found improvements to gingival health due to modulation of oxidative stress and inflammatory pathways.11–13 The rationale for selecting these oils for clinical study is based on biological plausibility for their use, known safety, and the clinical relevance of plaque-induced inflammatory diseases.
While these natural agents are believed to be effective tools for controlling plaque-induced gingivitis, there is a lack of evidence on their use for treating periodontal disease, particularly periodontitis, in diabetic patients with other underlying systemic illnesses. Therefore, further investigation into adjunctive antibiotic therapy to improve treatment outcomes following nonsurgical periodontal therapies is necessary for these individuals.14–17
Natural oils such as coconut oil, tea tree oil, myrrh, and extra virgin olive oil are being studied alongside antibiotics for their benefits to gingiva and their potential antimicrobial and/or anti-inflammatory properties for gingival health. To evaluate the uses of these oils, we included them in a review of publications on their antimicrobial properties and potential as a safe, well-tolerated alternative to standard commercially prepared antiseptics.18–20
This study aims to compare the efficacy of myrrh mouthwash and virgin olive oil mouthwash versus Chlorhexidine in reducing gingival inflammation and plaque accumulation. It was a randomized, double-blind, controlled clinical investigation involving 90 systemically healthy participants aged 18 to 30 years.
Methodology
This is a randomized, double-blind, controlled clinical trial involving 90 systemically healthy subjects aged 18 to 30 years. The study was conducted between February 2023 to September 2023 at the College of Dentistry, King Khalid University, Abha, Saudi Arabia. Experimental gingivitis was allowed to develop, and subjects were randomly assigned to three groups: CHX sample (n = 30), myrrh sample (n = 30), and olive oil sample (n = 30). Patients were asked to use mouthwash only for 14 days. The Plaque Index (PI), Gingival Index (GI) and STAIN score were measured at baseline, 7, 14 and 21 days.
The study design was approved by the institutional ethical review board of King Khalid University, Abha, Saudi Arabia [IRB/KKUCOD/ETH/2022-23/028].
The study's aims and objectives were explicitly disclosed to all patients. Written informed consent was obtained from all human participants before their inclusion in the experiment. Participants were requested to complete questionnaires that included medical and dental histories, and healthy patients who met the inclusion criteria were selected for this experimental gingivitis study.
Inclusion criteria were being between the ages of 18 and 30, not smoking, having a dentition with more than 20 teeth and at least 5 teeth per quadrant, no gingival swelling, redness, or bleeding (signs of gingival inflammation), no probing depth greater than 3 mm, and no clinical attachment loss.
Systemic diseases, severely misaligned teeth, patients with orthodontic appliances, mouth breathers, patients receiving antibiotic therapy (within the last six months) or medication such as aspirin or nonsteroidal anti-inflammatory drugs (within the last month), and patients who have used oral prophylaxis in the last six months are all exclusion criteria. Patients who are unable to comply with the study appointment schedule will also be excluded.
Participants were evaluated for the first time to assess eligibility and conduct dental screening and assessment. The initial appointment includes supragingival scaling, if necessary, prophylaxis, and dental care advice, such as brushing and flossing, 14 days before the research to ensure gingival health before the trial period begins. At the second visit, a periodontal examination was performed to ensure gingival and periodontal health, and patients were advised to follow the same regime for two weeks.
Preparation and Composition of Mouthwashes
The chlorhexidine-derived mouthwash used by participants was a commercially available 0.2% chlorhexidine gluconate mouthwash. The olive oil and myrrh oil used for both natural oil groups were pharmaceutical-grade extra-virgin olive oil and pure myrrh oil, respectively. For this study, the olive oil used was an extra-virgin product obtained from a standardized commercial source to ensure purity and that it was free of additives. Pure myrrh oil was obtained from a certified herbal supplier and used in the same manner as the olive oil. The participants in the oil pulling group received instructions stating that they were to use 10 mL of the oil assigned to them, swish it in their oral cavity for 1 min twice daily, then expectorate it and perform their normal oral rinsing with water. The oils were not diluted or supplemented with other excipients to maintain their natural bioactive properties. All participants received the same set of instructions to ensure that each followed the same procedure for administering oil throughout the study.
Plaque and gingival status were evaluated during the third visit of the study period using the Silness and Loe plaque index and the Loe and Silness gingival index, respectively. Participants were randomly assigned to one of three interventional groups using a simple randomization procedure and a random number generator: 1% Commiphora (myrrh) mouthwash, virgin olive oil mouthwash, and 0.2% chlorhexidine gluconate mouthwash.
Patients were asked to continue brushing their teeth and to use 10 mL of the assigned mouthwash twice daily for 1 min in an opaque, identical unlabelled bottle. The bottles were given to the patients by a dentist different than the examiner. The examiner and helper do not have access to the patient's code. Patients were asked not to use any other mouthwash and to refrain from eating or drinking for 30 min after using the mouthwash. They were given a measuring cup and advised to shake the bottle before using it. Patients’ compliance was measured using a follow-up form provided to them.
After 7, 14 and 21 days, the patients were re-examined by the same examiner, and the PI GI and STAIN score were measured again. Throughout the trial, patients were asked to document any concerns or side effects. Professional scaling, prophylaxis, and fluoride treatment were performed at the conclusion of the trial, and the acquired data were statistically analyzed.
Statistical Data Analysis
Data on categorical variables are displayed as n (percentage of cases), whereas data on continuous variables are presented as the mean and standard deviation. For multiple group comparisons, the Chi-Square test or Fisher's exact probability test with Bonferroni post-hoc test was used if more than 20% of cells had an anticipated frequency of less than 5.11–13
ANOVA with the Bonferroni post-hoc test was used to compare the means of normally distributed continuous variables between groups. Before analysing the research variables using ANOVA, the underlying normality assumption was checked. To better visualise statistically significant differences, all data were presented in both tabular and graphical formats.11–13
In the entire investigation, p-values less than 0.05 were considered statistically significant. The full dataset was statistically analysed using the Statistical Package for Social Sciences (SPSS version 24.0, IBM Corporation, USA) for Microsoft Windows. 11–13
Results
The distribution of sample size among the three study groups was 30 cases each, representing 33.3% of the total sample: group A consisted of CHX samples, group B of myrrh samples, and group C of olive oil samples, all equally distributed to ensure balance. The sample comprised 90 cases, representing 100% of the population studied. This equal allocation across groups indicates a carefully managed experimental design that minimizes bias from varying group sizes and enables equitable comparisons of treatment effects (Table 1).
The Distribution of sample Size Studied Across Three Study Groups.

The results of inter-group comparisons of mean age among three study groups were as follows. The mean ages are similar across the groups: 26.87 years (SD 4.34) for Group A, 25.70 years (SD 6.38) for Group B, and 26.87 years (SD 5.62) for Group C. The statistical evaluation, employing ANOVA with post hoc Bonferroni correction, yielded P-values of 0.999 for each pairwise comparison (Group A vs Group B, Group A vs Group C, and Group B vs Group C). The average age difference among the groups is not statistically significant, as all P values exceed the 0.05 significance threshold, suggesting that the groups are comparable in age and that age disparities are unlikely to influence the study results (Table 2).
Inter-Group Comparisons of Mean age.

P-value by ANOVA with post-hoc Bonferroni's correction for Multiple group comparisons. P-value<0.05 is considered to be statistically significant. NS – Statistically non-significant.
The mean ± SD of cases in Group A, Group B, and Group C was 26.87 ± 4.34 years, 25.70 ± 6.38 years and 26.87 ± 5.62 years respectively. The mean age of cases studied did not differ significantly between the three study groups (P-value > 0.05 for all).
Table 3 presents the inter-group comparison of gender distribution across the three study groups. Group A and Group C each have 63.3% males (19 participants) and 36.7% females (11 participants), while Group B has 70.0% males (21 participants) and 30.0% females (9 participants). Statistical analysis using the Chi-Square test with a post-hoc Bonferroni adjustment yields P-values of 0.999 for each pairwise comparison (Group A vs Group B, Group A vs Group C, and Group B vs Group C). All p-values exceeded the significance threshold of 0.05, indicating that the differences in gender distribution among the groups were not statistically significant, suggesting that the groups were well matched in gender distribution and thereby diminishing the likelihood of gender bias in the study results.
Inter-Group Comparisons of the Distribution of Gender.

P-value by Chi-Square test with post-hoc Bonferroni's correction for Multiple group comparisons. P-value < 0.05 is considered to be statistically significant. NS – Statistically non-significant.
Of 30 cases studied in Group A, 19 (63.3%) were male and 11 (36.7%) were female. Of 30 cases studied in Group B, 21 (70.0%) were male and 9 (30.0%) were female. Of 30 cases studied in Group C, 19 (63.3%) were male and 11 (36.7%) were female. The distribution of gender of cases studied did not differ significantly between the three study groups (P-value > 0.05 for all).
The % change at Visit 4 and the average Plaque Control Record (PCR) values for the three groups (A, B, and C) over the four visits. All pairwise comparisons showed no statistically significant differences (P-values > 0.05), and the mean PCR results for each visit are comparable across the groups. At Visit 4, Group A's PCR change was 32.91%, Group B's was 27.65%, and Group C's was 26.41%. Even though the mean values and percentage changes varied somewhat, the P-values for these comparisons (0.853, 0.561, and 0.999) remain nonsignificant (Table 4).
Inter-Group Comparisons of Mean Plaque Control Record (PCR).

P-value by ANOVA with post-hoc Bonferroni's correction for Multiple group comparisons. P-value < 0.05 is considered to be statistically significant. NS – Statistically non-significant.
The mean PCR at visit 1, at visit 2, at visit 3, and visit 4 among the cases studied did not differ significantly between the three study groups (P-value > 0.05 for all). The mean % change in PCR at visit 4 with reference to PCR at visit 1 among the cases studied did not differ significantly between the three study groups (P-value > 0.05 for all).
The table compares the mean Gingival Bleeding Index (GBI) values for the three groups (A, B, and C) across four visits, as well as the percentage change at visit 4. There were no significant differences in mean GBI levels between visits (p-values > 0.05). At Visit 4, however, Group A saw the largest percentage decrease in GBI (36.32%), followed by Group B (30.11%) and Group C (20.19%). While other comparisons were not significant, Group A showed a statistically significant difference from Group C (P = 0.006), suggesting that Group A reduced gingival bleeding more than Group C. This highlights the superior effectiveness of the intervention in Group A in reducing gingival bleeding over time (Table 5).
Inter-Group Comparisons of Mean Gingival Bleeding Index(GBI)

P-value by ANOVA with post-hoc Bonferroni's correction for Multiple group comparisons. P-value<0.05 is considered to be statistically significant. **P-value<0.01, NS – Statistically non-significant.
The mean % change in GBI at visit 4 concerning GBI at visit 1 among the cases studied did not differ significantly between Groups A and B as well as between Groups B and C (P-value>0.05 for all). The mean % change in GBI at visit 4 concerning GBI at visit 1 among the cases studied is significantly higher in Group A compared to Group C (P-value<0.05).
The following represents the percentage change at Visit 4 and the mean STAIN scores for the three groups (A, B, and C) across four visits. Over time, all groups’ STAIN scores decreased, but Group A's decline by Visit 4 was the largest at 67.29%, followed by Group C's at 52.44% and Group B's at 45.73%. Although the statistical analysis demonstrated no statistically significant differences in the percentage decrease at visit 4 or in STAIN scores across groups at any appointment, all P values were greater than 0.05. These results demonstrate that the intervention was equally effective in reducing staining scores across groups A, B, and C throughout the trial (Table 6).
Inter-Group Comparisons of Mean STAIN Score.

P-value by ANOVA with post-hoc Bonferroni's correction for Multiple group comparisons. P-value < 0.05 is considered to be statistically significant. NS – Statistically non-significant.
The mean STAIN score at visit 1, at visit 2, at visit 3, and visit 4 among the cases studied did not differ significantly between the three study groups (P-value > 0.05 for all). The mean % change in the STAIN score at visit 4 concerning STAIN score at visit 1 among the cases studied did not differ significantly between the three study groups (P-value > 0.05 for all).
The intra-group comparisons of mean Plaque Control Record (PCR) scores across four visits for Groups A, B, and C were as follows. Each group demonstrated a consistent reduction in PCR scores over time, with Visit 4 showing the lowest mean PCR score in all groups. Repeated measurements in statistical analysis PCR scores within each group decreased significantly between Visit 1 and subsequent visits, according to ANOVA (P < 0.05 for all comparisons). In particular, comparisons between Visit 1 and Visits 3 and 4 showed significantly significant declines (P < 0.001 for all groups). All three therapies were successful in enhancing plaque control within their respective groups over the research period, as seen by the notable intra-group decreases in PCR scores over time (Figure 1).
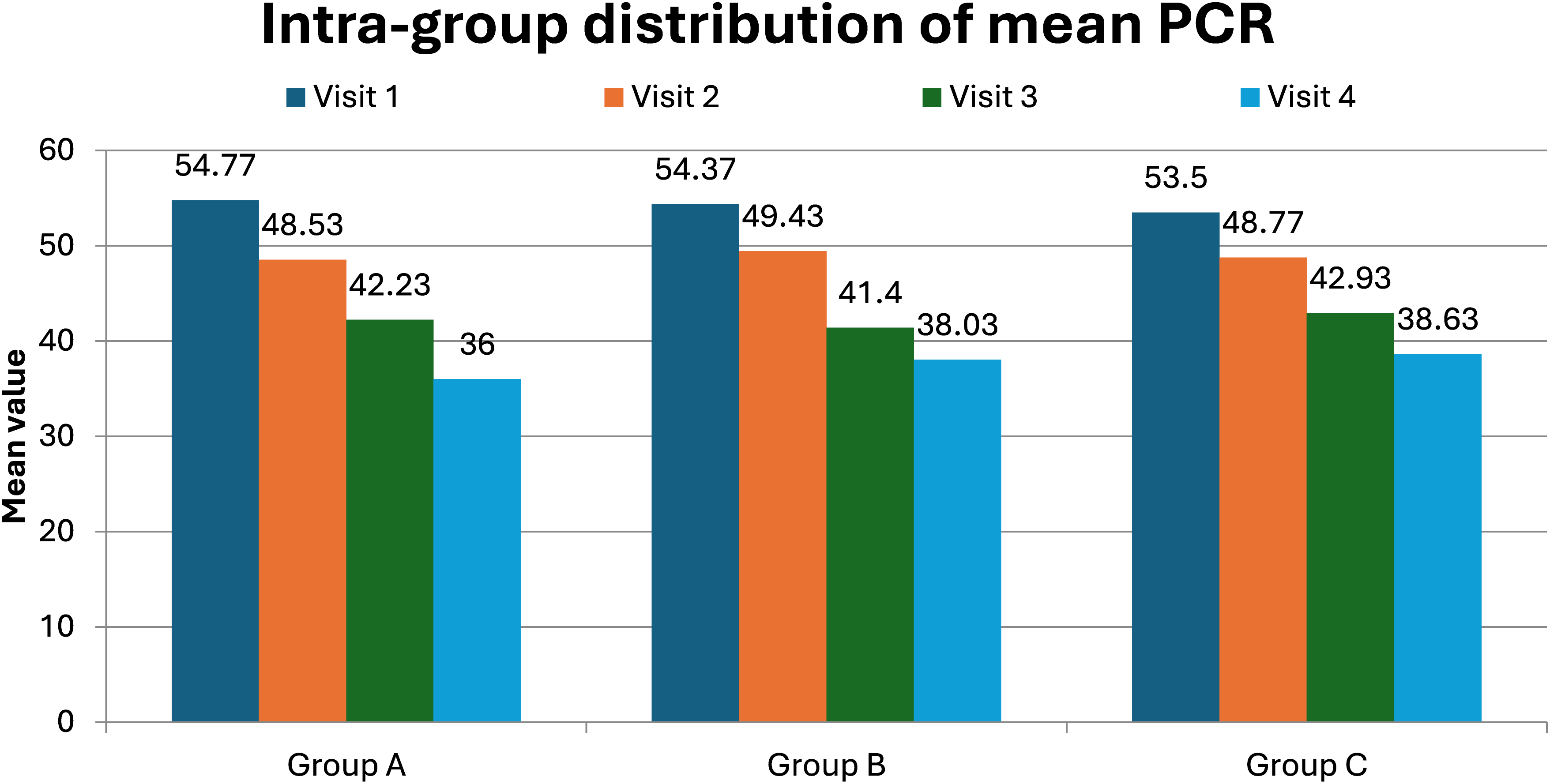
Intra-group distribution of mean PCR.
The intra-group comparisons of mean Gingival Bleeding Index (GBI) scores across four visits for Groups A, B, and C were as follows. Over time, GBI scores decreased across all groups, though the statistical significance varied. Significant decreases from Visit 1 to Visit 2 (P = 0.003) and extremely significant decreases from Visit 1 to Visits 3 and 4 (P < 0.001) were seen in Group A. Group B did not show a statistically significant reduction between Visit 1 and Visit 2 (P = 0.062), but significant reductions were observed from Visit 1 to Visits 3 and 4 (P < 0.001). Group C had no significant change between Visit 1 and Visit 2 (P = 0.408), but reductions from Visit 1 to Visits 3 and 4 were highly significant (P < 0.001) (Figure 2).

Intra-group distribution of mean GBI.
Groups A, B, and C's mean STAIN scores over the course of four visits were compared intra-group as follows. All comparisons between Visit 1 and subsequent visits revealed statistically significant findings (P < 0.001 or P < 0.01), and all groups showed substantial decreases in STAIN scores over time. In particular, STAIN scores for Groups A, B, and C decreased significantly from Visit 1 to Visits 2, 3, and 4, with very significant improvements noted at each visit (Figure 3).
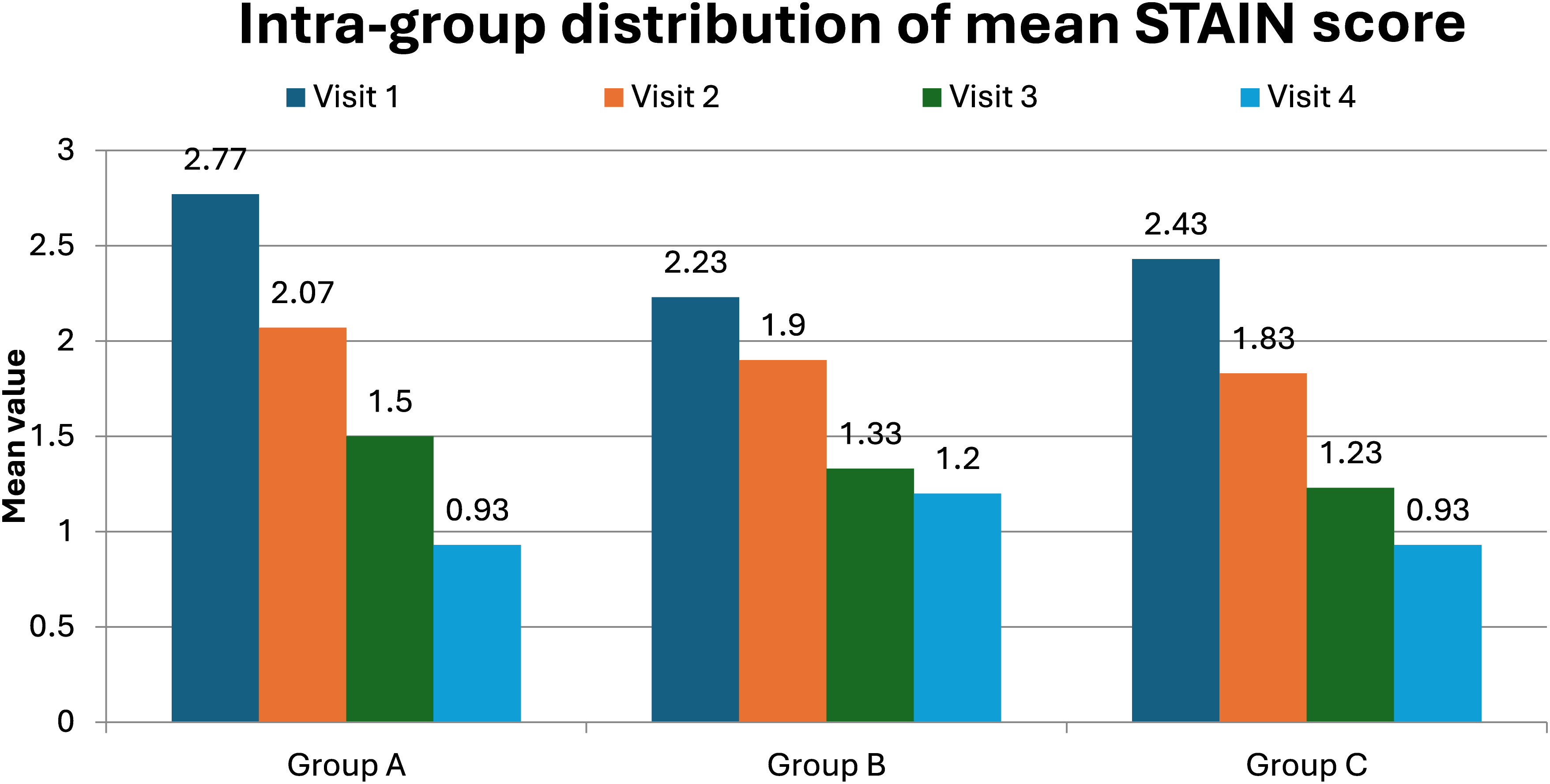
Intra-group distribution of mean STAIN score.
Discussion
Chlorhexidine is widely recognized as an effective antibacterial agent. It works by damaging bacterial cell membranes, leading to cell death. Chlorhexidine has broad-spectrum activity, effectively reducing bacterial load and preventing plaque buildup, a key cause of gingivitis. Chlorhexidine's excellent efficacy in suppressing oral bacteria makes it the gold standard for the treatment of gingivitis and periodontitis. However, its use is frequently associated with adverse consequences such as altered taste sensation, tooth discoloration, and oral mucosal irritation. 11
The amount of gingival bleeding (greatly decreased) with chlorhexidine (CHX) was much greater than the amount of gingival bleeding (decreased) with the natural oil based-interventions. No differences were found among groups in terms of plaque control record (PCR) or staining outcomes. This finding may reflect the broad-spectrum, strong anti-inflammatory and antimicrobial actions of CHX, which rapidly resolve gingival inflammation, even though there are no significant differences in gingival plaque accumulation between the two groups. PCR mostly measures the ability of a material to accumulate plaque and does not assess the degree of inflammation; staining depends on the presence of chromogenic compounds that are not necessarily produced by plaque formation. Therefore, although natural oils such as coconut and tea tree oil may limit plaque formation and are well tolerated, CHX's chemical action has a greater effect on reducing bleeding than do natural oils. The superiority of CHX's chemical mechanism of action should be considered when evaluating oral hygiene supplements. 12
Myrrh and olive oil have been reported to improve gum health through their antimicrobial properties and antioxidant effects, as well as through their anti-inflammatory effects. Bioactive components in myrrh (sesquiterpenes and furanosesquiterpenes) have been proven to inhibit the growth of bacteria responsible for periodontal disease and reduce inflammatory mediators in the gums. Extra virgin olive oil has the ability to regulate oxidative stress, suppress pro-inflammatory cytokines, and stimulate a beneficial immune response toward periodontal disease via the polyphenols contained in it; thus, both myrrh and olive oil appear as useful adjuncts to nonsurgical treatment of periodontal disease.13–15
In contrast, oil pulling uses natural oils, such as coconut oil, which contain antibacterial components, including lauric acid. The mechanical action of swishing oil helps remove dirt and microbes from the mouth cavity, and the oil itself has antibacterial properties. While oil pulling has grown in popularity because of its perceived safety and natural approach, scientific evidence is inadequate when compared to Chlorhexidine. 16
This study indicates that three different interventions, CHX, myrrh, and olive oil, can help improve oral health, such as raid control, gum bleeding, and decreased spots. The distribution of sample sizes across the three groups is uniform, resulting in a balanced experimental design that reduces displacement due to differential group sizes. The equilibrium and the uniform distribution of average age and gender across groups indicate that demographic factors probably did not affect the study outcomes, enhancing the reliability of the findings.
Regarding plaque management, as indicated by the PCR control, all groups exhibited a notable reduction over time, with no significant differences among groups. This shows that each strategy was equally successful in decreasing plaque development. Despite minor differences in the percentage change in PCR scores at Visit 4, the absence of statistical significance (P > 0.05 for all comparisons) suggests that no one intervention was superior for plaque control.
The Gingival Bleeding Index (GBI) revealed that Group A, which received CHX, had a higher reduction than the other groups. The significant difference between Group A and Group C (P = 0.006) suggests that CHX may be particularly effective in reducing gingival bleeding. Although the reduction in GBI was evident across all groups, statistical significance was limited to the comparison between Group A and Group C, underscoring the potential superiority of CHX over olive oil in this regard.
For stain reduction, as judged by the STAIN score, all three therapies resulted in significant reductions over time. Group A had the highest percentage reduction, but there was no significant difference between groups in mean STAIN scores or percentage change at visit 4 (P > 0.05). This suggests that all treatments were equally effective in removing stains and that none was superior to the others.
These findings are confirmed by within-group studies, which show significant reductions in PCR, GBI, and STAIN scores across all groups over time. These findings indicate that each intervention was effective in improving oral health outcomes in its target population. The considerable reductions in PCR, GBI, and STAIN levels observed at all visits demonstrate the medications’ efficacy throughout the research. While the reductions were significant, the lack of inter-group differences in several outcomes, such as PCR and STAIN scores, shows that the treatments may provide comparable benefits, with minor differences in specific outcomes such as GBI, where CHX outperformed olive oil.
Jong FJX et al (2024) conducted a comprehensive review to critically synthesise the evidence on oil pulling's effects on improving gingival health, plaque control, and bacterial counts compared with chlorhexidine and other mouthwash or oral hygiene practices. According to the study's findings, oil pulling may have a beneficial effect on gingival health. Compared with oil pulling, chlorhexidine was more effective at reducing plaque. However, the evidence was unclear, despite the clinically favourable benefits of oil-pulling interventions. 18
Shivakumar B et al (2023) did a study to assess the efficacy of oil pulling with sesame and coconut oils. The study found that oil-pulling treatment is as effective as chlorhexidine in reducing plaque and improving gingival health. More research is needed with a bigger sample size, altering the length and duration of oil drawing. 19
Griessl T, et al (2021) conducted a study to examine the oral microbiota at high resolution using oil pulling, compare it with saline pulling, and determine whether the procedure is capable of lowering the overall microbial burden of the mouth cavity. The study results allowed us to infer that oil pulling can be considered as an extension of regular oral hygiene treatments because it has the property of an oral massage, enveloping epithelial cells, transporting bacteria in oil vesicles, and reaching practically all unique habitats in the oral cavity. 20
Malik A et al (2022) conducted a study to compare the efficacy of virgin coconut oil pulling therapy and 0.2% CHX mouth rinse on clinical parameters and total microbial load in salivary samples from periodontally healthy individuals. Both study groups experienced decreases in Plaque Index (PI), Gingival Index (GI), and Gingival Bleeding Index (GBI) scores. Higher decreases were observed in the CHX group. It was shown that CHX and virgin coconut oil were efficient against microorganisms, resulting in a drop in CFU and so serving as a good alternative. 21
Bhalerao PV et al (2024) evaluated the effectiveness of coconut oil, sesame oil, and chlorhexidine mouthwash as adjuncts to SRP in individuals with plaque-induced gingivitis. Between baseline and three months, the chlorhexidine group had significantly lower plaque and gingival scores. The intragroup comparison demonstrated a statistically significant reduction in plaque and gingival index, suggesting that oil pulling may affect microorganisms and, in turn, treat plaque-induced gingivitis. 22
Over the last few years, increasing attention has been given to natural adjunct therapies to assist in the management of plaque-induced gingival inflammation. One such study was conducted by Zumbo et al, who evaluated the clinical efficacy of oil pulling with extra-virgin olive oil from the Itri region, high in polyphenols, in patients with gingivitis. The authors reported statistically significant reductions in gingival inflammation, attributed to the antioxidant, anti-inflammatory, and antimicrobial properties of olive oil polyphenols. The bioactive components of olive oil modulate oxidative stress, attenuate pro-inflammatory mediators, and inhibit the growth of pathogenic oral microorganisms. These results are consistent with those of the present study and indicate that there is promise in using natural oil-based adjunct therapies to assist with the management of plaque-induced gingivitis in young adults. 23
However, there is limited evidence supporting the effectiveness of natural oil-based adjunct therapies in more advanced periodontal disease states, such as periodontitis, or in populations that have systemic health concerns. Thus, while olive oil-based oil pulling may be beneficial as an adjunctive measure to support gingival health, it should not be viewed as an alternative to standard chemotherapeutic agents, such as chlorhexidine, or to antibiotic adjunctive therapy, especially among patients requiring comprehensive periodontal care.
Limitations
This study has many limitations. The study's short duration, absence of a validated experimental gingivitis model, and limited power for inter-group comparisons may restrict the generalizability of the findings. At start, the sample size was tiny, and the trial lasted only four weeks. To corroborate the results of this research, additional studies are essential for a larger sample size and a more in-depth examination. Second, this research did not examine prolonged exposure to oral health oil. Ultimately, this research was disregarded because of additional factors that might influence dental health, including diet and smoking habits.
Clinical Implications
The findings of this research carry significant clinical relevance. Oil mouthwash, a natural and non-invasive technique, can be recommended as an additional oral hygiene practice for young people. Nonetheless, due to its wide-ranging antibacterial properties, chlorhexidine mouthwash remains the benchmark for treating plaque and gingivitis.
Recommendations
Oil pulling may be suggested as a supplementary oral care practice for youth, offering an additional approach to preserving oral health. However, chlorhexidine mouthwash remains the gold standard for plaque and gingivitis control due to its established efficiency. While the current findings shed light on the benefits of oil pulling, larger sample sizes and longer durations are required to corroborate them. Furthermore, the long-term effects of oil pulling on dental health warrant further investigation to assess its viability and overall impact.
Conclusion
In conclusion, while all three therapies improved plaque control, gingival bleeding, and stain reduction, CHX may be especially advantageous for gingival health. The equivalent efficacy of the PCR across groups and the color point suggest that the three treatments can offer similar benefits for overall oral hygiene. Future studies with large sample sizes and extended observation durations will aid in elucidating long-term effects and possible therapies, compared with alternatives.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid university KSA for funding this research through a small research project with grant number RGP-1/159/46
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received a grant from the Deanship of Research and Graduate Studies at King Khalid University, KSA, through a small research project (grant number RGP1/159/46).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.