
Abstract
Oral ailments, for instance, oral mucositis, periodontitis, gingivitis, xerostomia, Sjögren's syndrome, oral leukoplakia, oral ulcer, oral lichen planus, and oral cancer, distinctly influence the state of health on account of their unfavorable impacts on the patient's digestion, vocal function, mastication, and aesthetic needs. Past research has displayed that herbal medicine could constrain the development of several oral ailments via modulating metabolism, the participation of signaling axes, and regulating cell motility. Herbal medicines exerted favorable functions mainly by means of various signaling axes like IL-17, TNF-α, ROS, p21, NF-κB, p38, ERK, mTOR, Src, TLR4, JNK1/2, PI3K, AKT, MAPK, and MMP-2/9, the occurrence of cell cycle arrest, and osteoblastic differentiation. Besides, they inhibited inflammation and had a significant influence on the growth, migration, invasion, and apoptosis of oral cancer cells. This review summed up the preclinical and clinical studies of herbal medicine in treating oral diseases, presented the curative effect and action mechanism of herbal medicine, and pointed out a direction for pharmaceutical exploitation and the following research fields.
Introduction
Oral disorders usually affect the oral mucosa and carry a risk of cancer. The buccal cavity is the starting part of the alimentary system, the second channel of breath, and a pivotal organ for chewing, pronunciation, and aesthetic requirements. Bad oral circumstances might result in body pain, malaise, and even disfigurement. 1 Oral ailments impact numerous people, causing burdens on global citizenship, particularly those in an inferior economic position. 2
Based on the authoritative classification systems of the American Academy of Oral and Maxillofacial Pathology, AAP/EFP, and WHO, oral diseases can be systematically categorized into the following major groups: Inflammatory and immune-mediated diseases, including oral mucositis (OM), gingivitis, oral lichen planus (OLP), and Sjögren's syndrome; Infectious diseases, represented by periodontitis; Potentially malignant disorders, encompassing oral leukoplakia (OLK) and proliferative verrucous leukoplakia; Malignant diseases, primarily oral cancer; Glandular dysfunction disorders, typically manifested as xerostomia; Ulcerative diseases, such as oral ulcer; and Developmental disorders, for instance, cleft lip and palate, dental developmental abnormalities, and genetic oral syndromes. 3 The nine oral diseases on which this review focuses—OM, periodontitis, gingivitis, xerostomia, Sjögren's syndrome, OLK, oral ulcer, OLP, and oral cancer—comprehensively cover most of the aforementioned core disease categories. These conditions not only have high incidence rates and significant clinical impacts globally, but also face limitations with current therapeutic approaches, while herbal interventions have demonstrated potential therapeutic advantages. Other oral disorders, such as pulp diseases, certain genetic disorders, and dental caries, were not included in this review due to their well-defined etiologies, established treatment protocols, and limited research evidence for herbal interventions.1,4
Herbal medicines, as an old scientific cultural inheritance, are a natural gift. They have assisted humans in confronting disorders, keeping healthy, prolonging life, and maintaining reproduction for thousands of years. 5 So far, herbal medicine has been used to cure multiple diseases and has fewer untoward reactions. It is still ubiquitous and satisfies the needs of numerous populations worldwide. 6 The worldwide herbal medicine market is presently worth about 700 billion RMB. Their usage is dramatically increasing. People feel healthier when they take herbal medicine. 7
The effectiveness of herbal agents depends on the functions of their active constituents, which work together to produce a synergistic effect and enhance the treatment's efficacy. 8 Past research has displayed that herb medicine could constrain the development of malignant oral diseases via modulating metabolism, the participation of signaling axes, and regulating cell motility. In vitro study, Shuanghuangbu-scaffold extract could upregulate the proliferation motivation of periodontal ligament cells. 9 In randomized clinical experiments, phytochemicals and medicinal plants were efficacious and secure remedies for the treatment of recurrent aphthous stomatitis. 10 Moreover, phytomedicines had fewer side effects and more satisfaction compared with disinfectants or antifungals. 11 The use of chewing gums with Pycnogenol could lower plaque attachment and gingival bleeding. 12
Studies in the past few years have concentrated on the investigation of herbal therapies for various oral diseases (Figure 1). There is a continuous effort to know the specific action mechanism of the process of herbal therapy. In this literature, we presented the recent research progress of herbal medicines, showing the clinical benefits of aiming at the diseases-related signaling axes and using herbal medicines or single active product to cure oral diseases. Confirming the mechanism of action is extremely crucial for offering proof of their therapeutic effect, which might result in pharmaceutical exploitation, and provide a vision for the following research fields.

Herbal agents against various oral diseases.
OM
In an OM model of rat, [6]-gingerol and [6]-shogaol (from Zingiber officinale Roscoe), two active components of hangeshashinto (HST, a traditional Japanese Kampo medicine containing Pinellia ternate (Thunb.) Breit., Scutellaria baicalensis Georgi, Zingiber officinale Roscoe, Panax ginseng C.A. Meyer, Glycyrrhiza uralensis Fisch., Ziziphus jujuba Mill., and Coptis japonica Makino), played essential roles in alleviating the pain of OM by blocking the Na+ channel. 13 Another literature form Miyano et al exhibited that HST increased the migration of oral keratinocytes based on MAPK and CXCR4 mobilization, accelerating tissue healing of cancer-related oral ulcerative mucositis. 14 They conducted an in-depth mechanism study in 2022, revealing that HST promotes oral keratinocyte migration and healing of chemotherapy-induced oral mucositis ulcers by activating the ERK signaling pathway to upregulate CXCL12 expression, thereby activating the CXCR4 receptor. 15 In OM modeling rats, Shuanghua Baihe Tablet (SBT, containing Lonicera japonica Thunb., Scutellaria baicalensis Georgi, and Lilium brownii F.E.Br. ex Miellez) modulated the metabolism of linoleic acid, glycerophospholipid, and amino acid, and inhibited IL-17/TNF signal pathways to maintain Th17 and Treg cell homeostasis, thus decreasing chemotherapy-caused OM. 16 By the analysis of GO and KEGG enrichment, Liu et al uncovered that Sancao Yuyang Decoction (SCYYD, containing Trifolium pratense L., Glycyrrhiza uralensis Fisch., and Sophora flavescens Aiton) yielded beneficial results for OM therapy through related pathways, for example, Ras and HIF-1 axes. Then, molecular docking exhibited that primary constituents (sitosterol, naringenin, kaempferol, quercetin, and luteolin) in SCYYD had the best-combining competence with the core targets like STAT3, Src, HIF-1α, and HSP90AA1. Furthermore, the in vivo experiment revealed that SCYYD not only suppressed inflammation responses and facilitated wound repair of oral mucosa in OM rats, but also decreased the expressions of HSP90AA1, Src, HIF-1α, STAT3, TLR4, mTOR, MMP-9, and augmented the expression of ESR1. Taken together, these results provide a mechanistic basis for the clinical use of SCYYD in the management of oral mucositis. 17 An experiment of 54 golden hamsters uncovered that the topical use of Carum carvi L. (caraway) hydroalcoholic extract might be linked to depressed severity of cheek pouch scratching and 5-FU-caused OM, which was attributed to suitable antibacterial dynamism and γ-Terpinene (main component of essential oil) concentration. 18 Plantago ovata Forssk. (blond psyllium) hydrocolloid obviously diminished the mucositis grade, the pain level, and the xerostomia degree. 19
In randomized clinical studies of treating or preventing OM among cancer patients, the utilization of topical chamomile (Matricaria chamomilla L.) was valid, accompanied by a concentration distribution varied from 1% to 2.5% and a duration of time varied from 1 to 4 times every day. 20 Another study also showed that sufferers using 3% topical chamomile oral gel appeared to have weakened mucositis severity and low pain sensation. 21 A mucoadhesive formulation including curcuminoids (from Curcuma longa L.) and Bidens pilosa Linn (hairy beggarticks) extract was secure and applicable in two suitable doses against OM. 22 Rhodiola algida (stonecrop) improved chemotherapy-generated OM in patients with breast cancer by promoting the generation of lymphocytes, without liver and renal damage. In addition, the levels of granulocyte-macrophage colony-stimulating factor (GM-CSF) and IL-2/4 of lymphocytes were increased 23 (Table 1).
The Action Mechanism of Herbal Agents in Treating OM.

Periodontitis
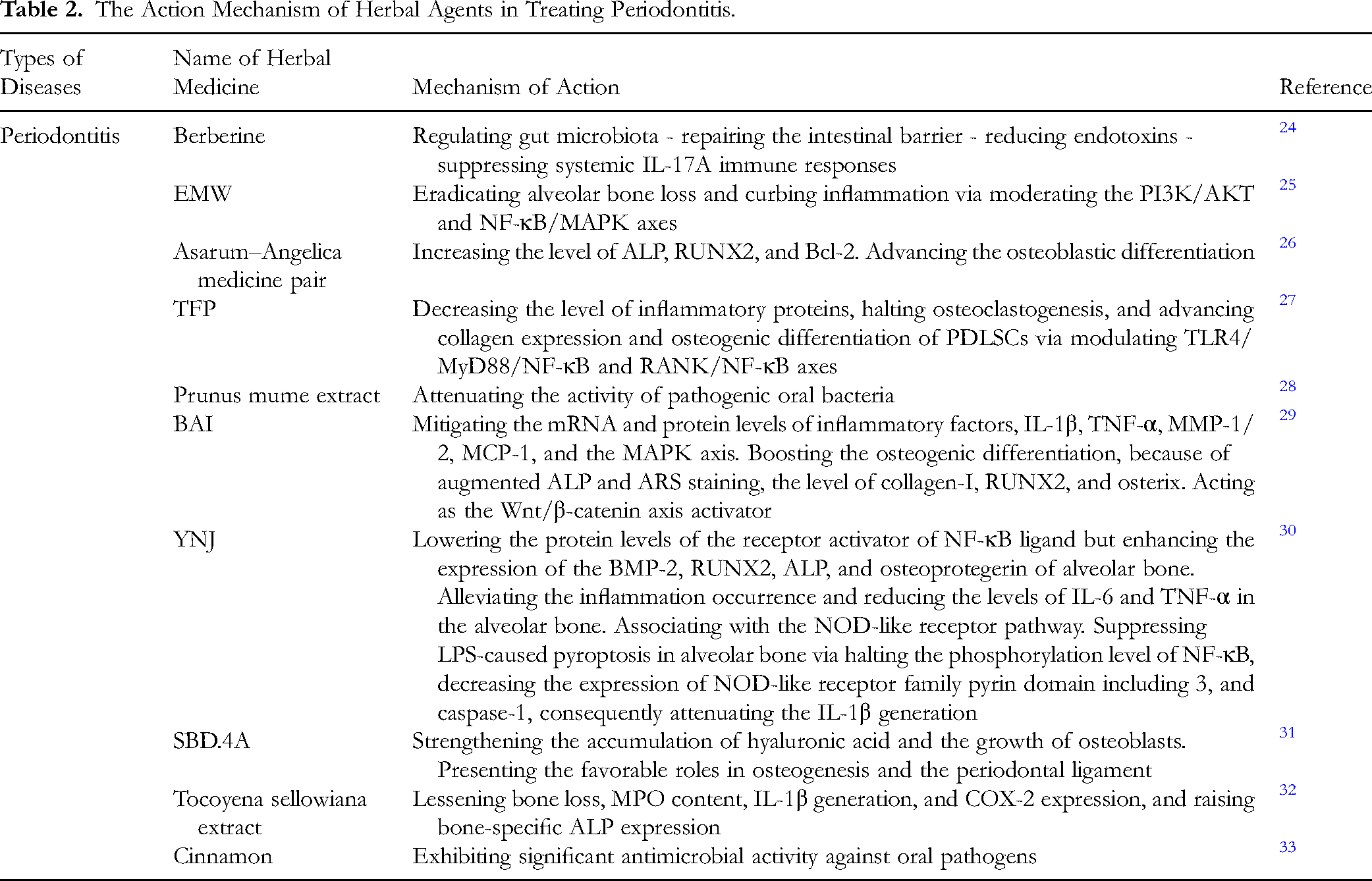
In an established rat periodontitis model, Jia et al exhibited that berberine alleviates local inflammation and bone destruction in periodontal tissues through a cascade of effects: regulating gut microbiota - repairing the intestinal barrier - reducing endotoxins - suppressing systemic IL-17A immune responses. This reveals the critical role of gut microbiota in estrogen-deficient aggravated periodontal bone loss, providing theoretical support for berberine as an adjunctive therapy for periodontitis, particularly in cases of systemic compromise such as estrogen deficiency. 24 Xia et al recognized that Ermiao Wan (EMW) could eradicate alveolar bone loss and curb inflammation via modulating the PI3K/AKT and NF-κB/MAPK axes, consequently holding back the occurrence of periodontitis. 25 Network pharmacology analysis was employed by Chen et al to predict the effect of the Asarum-Angelica medicine pair in promoting osteogenic differentiation. This effect was hypothesized to be associated with targeting the PI3K/AKT axis, a key regulatory axis in osteoblast differentiation and survival. Subsequent in vitro experiments confirmed that this compound significantly increased phosphorylated AKT levels in human periodontal ligament cells. Furthermore, the expression of both osteogenic markers alkaline phosphatase (ALP) and Runt-related Transcription Factor 2 (RUNX2), as well as Bcl-2, was found to be enhanced, while the apoptotic protein Bax was suppressed. This elucidates its causal mechanism for promoting osteogenic differentiation: by activating the PI3K/AKT signaling pathway, it enhances osteoblast activity and inhibits apoptosis. 26 Tang et al found that total flavonoid extract from propolis (TFP) could decrease the level of inflammatory proteins, halt osteoclastogenesis, and advance collagen expression and osteogenic differentiation of periodontal ligament stem cells (PDLSCs) through regulating TLR4/MyD88/NF-κB and RANK/NF-κB axes. 27 Prunus mume extract attenuated the activity of pathogenic oral bacteria. 28 In LPS-stimulated PDLSCs, baicalein (BAI) manifestly mitigated the mRNA and protein levels of inflammatory factors, containing interleukin-1β (IL-1β), TNF-α, MMP-1/2, monocyte chemoattractant protein 1 (MCP-1), and the MAPK axis. In addition, BAI also boosted the osteogenic differentiation, because of increased ALP and ARS staining, expression of collagen-I, RUNX2, and osterix. Above all, it could function as the Wnt/β-catenin axis activator. 29 In the orthodontic ligation and LPS-stimulated periodontitis rat model, yunvjian decoction (YNJ) lowered the protein levels of the receptor activator of NF-κB ligand but enhanced the expression of the BMP-2, RUNX2, ALP, and osteoprotegerin of alveolar bone. In addition, YNJ alleviated the occurrence of inflammation and reduced IL-6 and TNF-α expression in the alveolar bone. The analysis of network pharmacology exhibited that the nucleotide-binding oligomerization domain (NOD)-like receptor pathway was the key axis associated with treatment for YNJ. The study finally proved that YNJ suppressed LPS-caused pyroptosis in alveolar bone via halting the phosphorylation level of NF-κB, decreasing the expression of NOD-like receptor family pyrin domain including 3, and caspase-1, consequently attenuating the IL-1β generation. 30 In models of periodontal regeneration, SBD.4A (a confirmed preparation of Angelica sinensis) in vitro notably strengthened the accumulation of hyaluronic acid and the growth of osteoblasts. It presented the favorable roles in osteogenesis and periodontal ligament. 31 The extract of Tocoyena sellowiana as Brazilian plant, lessened bone loss, myeloperoxidase (MPO) content, IL-1β generation, and cyclooxygenase-2 (COX-2) expression, and raised bone-specific ALP expression, without alteration of body weight and organs in Wistar rats. 32 Cinnamon essential oil, extracts, and their main pure compounds, such as cinnamaldehyde and eugenol, exhibit significant antimicrobial activity against oral pathogens 33 (Table 2).
The Action Mechanism of Herbal Agents in Treating Periodontitis.
Gingivitis
Cheng et al proved that toothpaste containing pudilan extract (containing Corydalis bungeana Turcz., Scutellaria baicalensis Georgi, Isatis indigotica Fortune, and Taraxacum mongolicum Hand.-Mazz.) possessed a beneficial impact on alleviating chronic gingivitis through suppressing plaque formation, decreasing inflammatory occurrence, and downregulating the degree and rate of bleeding. 34 The application of chewing gums, including C. incanus (Cistus incanus L.) extracts and S. lateriflora (Scutellaria lateriflora L.), caused obvious amelioration of the gingival condition after subjects enrolled for 3 months. 35 Mouthwash with triphala (a traditional Ayurvedic formulation containing Terminalia chebula Retz., Terminalia bellirica (Gaertn.) Roxb., and Phyllanthus emblica L.) diminished the inflammatory index in patients with gingivitis. 36 Topical utilization of the transmucosal herbal periodontal patch (containing Centella asiatica (L.) Urb., Echinacea purpurea (L.) Moench, and Sambucus nigra L.) might be valid and secure in diminishing inflammation occurrence 37 (Table 3).
The Action Mechanism of Herbal Agents in Treating Gingivitis.

Xerostomia
Kagami et al discovered that Bakumondo-to (containing Ophiopogon japonicus (Thunb.) Ker Gawl.) displayed increased roles in cell growth in vitro cultured salivary gland cells, and indicated that Bakumondo-to enhanced the average size of secretory granules in parotid gland cells. 38 Yukmijihwang-tang (YMJ, containing Rehmannia glutinosa (Gaertn.) DC., Cornus officinalis Siebold & Zucc., Dioscorea opposita Thunb., Alisma orientale (Sam.) Juz., Poria cocos (Schw.) Wolf, and Paeonia suffruticosa Andrews) polished up the moisture condition and dryness status in older subjects 39 (Table 4).
The Action Mechanism of Herbal Agents in Treating Xerostomia.

Sjögren's Syndrome
In a six-week clinical study, the application of ShengJinRunZaoYangXue granules (containing Rehmannia glutinosa (Gaertn.) DC., Ophiopogon japonicus (Thunb.) Ker Gawl., Scrophularia ningpoensis Hemsl., and Angelica sinensis (Oliv.) Diels) for primary Sjögren's syndrome improved the phenomenon of dry eyes, dry mouth, and inferior tear flow frequency with smaller adverse roles. 40 Herbal SS-1, including the powder form of “Gan-Lu-Yin”, “Sang-Ju-Yin”, and “Xue-Fu-Zhu-Yu decoction”, obviously curbed maturation antigen of B-cell to ameliorate ocular eye signs 41 (Table 5).
The Action Mechanism of Herbal Agents in Treating Sjögren's Syndrome.

OLK
OLK is the most common malignant oral lesion. Hou et al have proved Scutellaria baicalensis Georgi (SBG) might potentially cure patients with OLK. In particular, BAI, as a main active component of SBG, could obviously inhibit the proliferation and migration of dysplastic oral keratinocyte (DOK), trigger apoptosis, hold back the cell cycle, and restrain the mRNA expression of the hub genes via suppressing the PI3K/AKT signal transduction 42 (Table 6).
The Action Mechanism of Herbal Agents in Treating OLK.

Oral Ulcer
In the oral ulcer rat model, Chen et al verified that Kouyanqing Granule (KYQG) evidently halted the serum expression levels of COX-2, MMP-9, and TNF-α. KYQG also showed advantageous efficacy on oral ulcer, possibly by preventing inflammation occurrence, modulating immunological feedback, and restraining oxidative stress. Network pharmacology analysis suggested that the HIF-1 and TNF pathways may play pivotal roles in KYQG's protective mechanism against oral ulcer 43 (Table 7).
The Action Mechanism of Herbal Agents in Treating Oral Ulcer.

OLP
Natural remedies could be of service to control the OLP. Curcuminoids (from Curcuma longa L.) had fine tolerance and might be significant in restraining signs of OLP, with 3 divided concentrations of 6000 mg/day. 44 The joint of topical glucocorticoids (TGCs) and Tripterygium glycosides (TGs, from Tripterygium wilfordii Hook.f.) ameliorated clinical effectiveness and declined relapse without adding the danger of side roles. 45 Purslane (Portulaca oleracea L.) was beneficial in the clinical therapy of OLP 46 (Table 8).
The Action Mechanism of Herbal Agents in Treating OLP.

Oral Cancer
Yang et al concluded that Duchesnea indica extract (DIE) has shown anti-metastatic properties against oral cancer. DIE suppressed the motility, migration, and invasion of oral squamous cell carcinoma (OSCC) cells through inhibiting the MMP-2 expression. This was achieved by mechanistically restraining the MEK/ERK axes. 47 In the study of the vincristine-resistant tumor cell line, celastrol induced cell apoptosis via lowering the Bcl-2 level. What's more, c-Jun N-terminal kinase (JNK)1/2 was the main axis of celastrol-mediated apoptosis. Celastrol exerted pro-apoptotic effects on drug-resistant oral malignancy cells by simultaneously activating intrinsic and extrinsic apoptotic machinery, reflected in the accumulation of cleaved forms of caspase-3/8/9 and Poly (ADP-ribose) Polymerase. 48 Yun et al found that verticinone could cause apoptosis via a caspase axis regulated by mitochondrial damage (increased cytochrome c levels, caspase-3 activation) and G0/G1 cell cycle arrest in oral cancer cells and immortalized keratinocytes. 49 Reports about Hsiao et al showed that curcumin (CUR), dimethoxy curcumin (DMC), and bisdemethoxycurcumin (BDMC) initiated apoptotic cell death via reactive oxygen species (ROS), a mitochondria-dependent way, and generation of cell autophagy in human oral cancer cells. 50 The investigation from Chiu et al has shown chloroform extract of Solanum lyratum (SLEC) irritated G0/G1 arrest through the p21/p16 signaling pathway and mediated apoptosis through ROS, caspases, and mitochondrial approaches in human oral cancer cell lines. 51 Rhein remarkably curbed oral cancer cell proliferation via triggering apoptosis and arresting the cell cycle at the S-phase. Furthermore, it restricted the migration and invasion of oral cancer cells via moderating epithelial-mesenchymal transition. In addition, it gave play to the antitumor role in vivo and in vitro by producing oral cancer cell apoptosis and ROS generation through the AKT/mTOR axis in oral cancer. 52 The findings of V. Bharath Kumar et al showed that sodium danshensu definitely decreased the migration and invasion activity of oral cancer cells by lessening p38 MAPK phosphorylation. 53 Chen et al proved that magnolol reduced cell growth via activating the sub-G1 cell cycle and apoptosis of SCC-9 and HSC-3 cells. The apoptosis in oral cancer cell lines was mediated by the JNK1/2- and p38 pathways-leaded caspase activation. 54 Yeh et al suggested geraniin in vitro manifestly inhibited the migration of SCC-9 and SCC-14 cells via a mechanism that included the reduction of MMP-2 expression level and activity caused by down-regulated FAK/Src and ERK1/2 axes. 55 The investigation of Uen et al showed that aqueous extracts of S. nigrum (AESN) significantly augmented ROS generation. Besides, it also activated the caspase-3 and caspase-9 pathway, as well as following excitation of the mitochondrial fission approach. 56 Wang et al revealed that Polygonum cuspidatum extract (PCE) markedly enhanced caspase-3 and −9 activities. Moreover, it obviously boosted the protein expression of Atg5/7/12, LC3, Bax, Beclin-1, and cleaved caspase-3 in cisplatin-resistant human oral cancer CAR cells. After treating with PCE, autophagy and apoptotic cell death appeared. 57 Based on the analysis of network pharmacology and the techniques of molecular docking, Dong et al identified six potential key target spots of oral cancer therapy with quercetin. These target spots included PIK3R1, AKT1, MYC, HSP90AA1, Src, and HIF-1α, suggesting quercetin might impact oral cancer via these core targets. 58 Ruan et al concluded that the roles of Shikonin in restricting cell growth and mediating apoptosis, the latter achieved partly by restricting the NF-κB signaling pathway and subsequently activating the caspase family in Tca-8113 cell lines. 59 Treating with aloe-emodin made the cell cycle cease at the G2/M stage and increased ALP expression in the human oral cancer cell line KB cells. 60 Wang et al found that antitumor B, a mixture of six Chinese herbal medicines (Polygonum bistorta, Sonchus arvensis L., Dioscorea bulbifera, Dictamnus dasycarpus, Sophora tonkinensis, and Prunella vulgaris), restricted cell proliferation and lowered the levels of phosphorylated epidermal growth factor receptor (EGFR) and EGFR. 61 Selaginella tamariscina prevented oral cancer cell motility via restricting MMP-2/9 activities and decreasing the activity of DNA combination with promoter elements. In addition, the anti-metastatic roles were also related to devitalized AKT. 62 Chen et al reported honokiol (HNK) inhibited the growth of OSCC cells because of apoptotic occurrence. 63 Han et al uncovered that the methanol extract of K. scoparia, mature fruit (MEKS) generated the apoptosis of OSCC cells via elevating caspase-3 and −9 activities mediated by the p38 MAPK axis. 64 In oral cancer cells, Tang et al thought that treatments of ethyl acetate extract of Nepenthes adrianii×clipeata (EANA) brought about DNA damage and oxidative stress on account of ROS generation, mitochondrial membrane electric potential destruction, γH2AX, and mitochondrial superoxide. Subsequently, EANA incurred prior killability, DNA damage, and apoptosis by means of oxidative stress. 65 Lee et al observed that after treating with Juniperus communis extract (JCo), the G0/G1 stage cell cycle arrest appeared because of the regulation of Rb and p53/p21 axes. Additionally, JCo also led to an upregulation in the sub-G1 cell cycle and cell apoptosis. 66 Guan et al certified that partial utilization of Zengshengping (ZSP) manifestly inhibited the number of BrdU-positive buccal pouch cancer cells and restricted the production of MAPK. Additionally, ZSP accelerated tumor cell apoptosis via augmenting caspase-3 level but reducing Bcl-2 protein generation. 67 An examination revealed that the Eclipta prostrata extracts (EPE) alleviated oral cancer cell migration and invasion through downregulating the enzyme activities of MMP-2. What's more, EPE evidently decreased the level of ERK1/2. 68 Rheum palmatum L. extract (RLEs) displayed an antimetastatic role in oral cancer cells via repressing transcription expression of MMP-2 by means of the ERK1/2 axis. 69 Wang et al observed that ZSP-2 had a chemoprophylactic impact on oral cancer via repressing inflammation, growth of tumor cells, microvessel generation, and boosting cancer cell apoptosis. 70 In oral mucoepidermoid carcinoma (MEC), methanol extract of Smilax china L. (MESC) diminished cell viability and triggered apoptosis in MEC cells, increasing DR5 due to enhanced protein stability, which produced Bim and t-Bid. Additionally, MESC blocked the ERK axis, causing apoptotic death of cells. 71 Zhang et al deemed magnolia extract (ME) curbed mitochondrial complex I-induced respiration process, oxidized peroxiredoxins, stimulated AMP-activated protein kinase (AMPK), and reduced STAT3 phosphorylation, causing the containment of the proliferation and growth of oral cancer cells 72 (Table 9).
The Action Mechanism of Herbal Agents in Treating Oral Cancer.

Conclusion
Herbal medicines are presently widespread and identified in various countries as vital supplementary and replaceable agents. They have received more focus in the area of various oral disorders. 5 Herbal medicines serve beneficial functions in attenuating the development of oral ailments, for example, OM, periodontitis, gingivitis, xerostomia, Sjögren's syndrome, OLK, oral ulcer, OLP, and oral cancer, which is ascribed to the smaller adverse reactions, broad practicality, desirable therapy outcomes compared with traditional drugs, and attractive price. 73
Based on the above analysis, the various herbal preparations covered in this review can be categorized into the following types of action: (1) Single-herb extracts, such as DIE, with clearly identified active components and relatively single mechanisms of action; (2) Herbal pair combinations, such as the Asarum-Angelica medicine pair, where the two herbs synergistically exert enhanced effects; (3) Classic formulas, such as HST, SBT, and SCYYD, which adhere to Traditional Chinese medicine (TCM) formula theory, where multiple herbs and components exert synergistic effects through multi-target and multi-pathway mechanisms; (4) Active single compounds, such as berberine, BAI, CUR, and celastrol, which originate from herbs and, after separation and purification, can be used for mechanism research and drug development. Each type of herbal preparation possesses distinct characteristics and application value. Single compounds and drug pairs are suitable for mechanism studies, while compound preparations better reflect the therapeutic advantages of TCM's holistic perspective.
Herbal medicines generally include multiple medically active constituents, but traditional medicines generally involve only one. 74 Having knowledge of the action mechanism of herbal medicines can create a favorable sight for following clinical studies. Based on the critical evaluation of included studies in this review, the roles of herbal medicine in treating oral diseases can be summarized under the following core themes: (1) Anti-inflammatory roles: Restricting pro-inflammatory cytokines by moderating inflammatory signal transduction including NF-κB, MAPK, and Th17/Treg; (2) Antioxidant effects: Mediating cell protection/apoptosis by modulating ROS; (3) Immunomodulation: Restoring immune homeostasis by regulating Th17/Treg balance and B-Cell; (4) Tissue regeneration promotion: Promoting tissue regeneration via modulating Wnt/β-catenin and BMP axes; (5) Antitumor effects: Inhibiting tumor cell proliferation, migration, and invasion by mediating cell cycle arrest and apoptosis; (6) Antibacterial effects (Figure 2). The clinical significance of these mechanisms lies in their provision of a theoretical foundation for developing multi-target therapeutic strategies, while also guiding personalized medicine and combination drug design. These roles are modulated via multiple signaling axes, including IL-17, TNF-α, NF-κB, PI3K, AKT, and mTOR. These findings can guide mechanism-based combination therapy development and identify novel drug targets for oral disease treatment. Additionally, identifying these effects helps to understand rational biomarkers and design outcome measures for clinical trials.

Integrated mechanistic framework of herbal medicines in treating oral diseases.
Although a growing tendency for herbal medicine usage in patients between the East and the West manifests, the scientific proof of efficacy and safety is gradually questioned by scholars. 75 It is worth noting that research standards and typical methodologies exhibit shortcomings, quality control of TCM remains uncertain, and there is a lack of extensive clinical evidence supporting its application in clinical practice.76–78
Multiple factors contribute to this uncertainty, including: raw material variability; lack of standardized extraction and preparation methods; absence of universally accepted biomarkers for quality assessment; inconsistencies in chemical fingerprints across batches and manufacturers; and the complexity of synergistic effects among multiple components. These factors result in differences in chemical fingerprint profiles between batches.79,80
We propose the following recommendations to address the aforementioned issues: (1) The establishment of herbal fingerprinting technology using high-performance liquid chromatography (HPLC) or liquid chromatography-mass spectrometry (LC-MS) is recommended to create standardized chemical fingerprints, thereby ensuring batch-to-batch consistency81,82; (2) Researchers should develop bioactivity-based quality control methods that utilize cellular or molecular targets to evaluate extract bioactivity83,84; (3) Manufacturers are encouraged to implement GAP and GMP to control raw material quality at the source ; (4) The scientific community should establish comprehensive herbal ingredient databases encompassing chemical structures, physicochemical properties, bioactivity, and pharmacokinetic parameters for each component83,84; (5) International organizations such as the International Organization for Standardization (ISO) and national pharmacopoeias are urged to promote the development of unified herbal quality standards. 85 These measures are expected to enhance the quality consistency of herbal products, thereby ensuring the reproducibility of clinical research and the predictability of therapeutic outcomes.
Although this review details promising preclinical evidence for specific compounds such as berberine, BAI, and Shikonin, a significant translational gap remains. 86 Currently, extensive studies fail to report the Release Profile Index (RPI), which severely limits the prediction of in vivo efficacy. Similarly, only a few studies have reported pharmacokinetic data for herbal active ingredients, while many herbal components (such as BAI) have poor water solubility and inferior oral bioavailability, restricting their clinical application. The first-pass effect further exacerbates this complexity. Future research should systematically determine and report RPI data based on cumulative release profiles and kinetic models, and investigators should correlate these parameters with in vitro activity and in vivo efficacy. 87 Concurrently, researchers should measure pharmacokinetic parameters using advanced techniques such as LC-MS/MS, and they should develop delivery strategies, including nanoformulations and phospholipid complexes, to augment oral bioavailability. 88
In the treatment of oral cancer, utilizing the Enhanced Permeability and Retention (EPR) effect to achieve targeted delivery of nanomedicines is crucial. 89 The report by Wang et al highlighted the passive targeting properties of nanoparticle delivery systems within tumor tissues, which aligns with the fundamental principles of the EPR effect. 57 However, these researchers did not directly measure the parameters of the EPR effect. Furthermore, a comprehensive safety evaluation of herbal medicines, including acute and chronic toxicity and genotoxicity, is a prerequisite for clinical translation, yet systematic toxicological research remains insufficient. Future safety studies should adhere to OECD or FDA guidelines, and investigators should systematically elucidate target-organ toxicity and carcinogenic risks through acute and chronic toxicity tests, as well as reproductive and genetic toxicity assessments. 90 In the aspect of oral cancer treatment, the following investigations should concentrate on exploring the influence of physicochemical properties, such as particle size and charge, of herbal nanoformulations on their distribution in tumor tissues, and researchers should focus on augmenting the EPR effect by combining these formulations with microenvironment modulators. Furthermore, as most studies lack systematic adverse reaction assessments, future research should follow ICH and FDA guidelines, and investigators should establish monitoring databases to comprehensively collect and grade adverse events. 91
Interactions between herbal medicines and conventional drugs represent a critical safety concern that may lead to adverse clinical outcomes. These risks include the following: (1) Pharmacokinetic interactions occur through modulation of cytochrome P450 enzymes and drug transporters, resulting in altered drug concentrations; (2) Pharmacodynamic interactions produce additive, synergistic, or antagonistic effects; (3) Combining antiplatelet or anticoagulant drugs with herbs affecting coagulation increases bleeding risk 92 ; (4) Hepatotoxicity may be induced by herbs containing pyrrolizidine alkaloids; (5) Nephrotoxicity is associated with herbs containing aristolochic acid.90,93 This underscores the importance of thorough medication reconciliation and patient education in clinical practice.
In addition, researchers must urgently consider herbal agent preparation forms and therapy measures because of bad absorption, poor activity in experiments in vivo, and incompatibility with other compositions of herbal ingredients, which usually depend on the remedy properties and clinical demand. The upgradation of traditional preparation forms and the detection of active plant components can yield novel therapeutic methods in the treatment of patients. 94
Based on the above discussion, future research should further drive the clinical translation of herbal medicines through systematic, multi-dimensional approaches. This strategy includes employing systems biology and network pharmacology to map multi-target mechanisms and establish spectrum-effect relationships.95,96 At the clinical level, investigators need to conduct rigorous double-blind trials and extend these studies to special populations, alongside the development of core outcome sets that integrate biomarkers and patient-reported outcomes with long-term follow-up. 97 Ultimately, integrating traditional theory with modern pharmacogenomics will help address key scientific questions, facilitating the evolution of herbal medicine from empirical practice to evidence-based medicine. 95
In conclusion, further investigations are required to design fine and in-depth fundamental research to study the pathogenesis of oral disorders, determine the action mechanism of more herbal medicines, screen for the most effective therapeutic drugs, explore more clinical trials, and strengthen the joint use between herbs and traditional drugs.98,99 The clinical study of herbal medicine is hopeful to accelerate the knowledge of herbal medicine effectiveness, explore new therapies, and enhance the adoption of these therapies, making herbal medicines applicable to clinical therapy and hastening clinical success.97,100
Footnotes
Abbreviations
Acknowledgements
No Apply.
Ethics Approval and Consent to Participate
No Apply.
Consent for Publication
All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Authors’ Contributions
All authors contributed to the study conception and design. Article collection and writing of the first draft were performed by LY.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Young Talent Fund of Association for Science and Technology in Shaanxi,China.
Shaanxi Provincial Association for Science and Technology's Young Talent Support Program.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
All cited articles in the current study are available in the public database.