
Abstract
Background
Menopausal vasomotor symptoms like hot flashes and night sweats negatively impact quality of life.
Objectives
This study aimed to determine the effects of primrose oil versus lavender oil on menopausal symptoms.
Methods
A double-blind, randomized, controlled trial was conducted on 150 menopausal women aged 40–60, who had experienced amenorrhea for over 6 months, and had no herbal allergies or serious illnesses. The women were consecutively recruited and, using a sealed, opaque envelope method, randomly allocated to receive either primrose oil, lavender oil, or a placebo for 8 weeks. All women applied oil twice daily to specific body areas. Prior to, four weeks and eight weeks after the intervention, the women completed the Daily Hot Flashes/Night Sweats Diary, Hot-Flash/Night Sweats Problem Rating, and Hot Flashes Related Daily Interference Scale. The data were analyzed using the Mann-Whitney U test, Chi-square, analysis of variance, and post hoc tests. The level of significance was set at ≤0.05
Results
At baseline, the three groups did not significantly differ regarding the mean daily interference (P = .22), frequency of hot flashes/night sweats (P = .61), and hot flashes severity index (P = .84). The mean daily interference (P < .001), frequency of hot flashes/night sweats per week (P < .001), and hot flashes intensity index (P < .001) in women receiving primrose oil or lavender oil exhibited a significant decline at the end of the fourth and eighth weeks after the intervention. The decreases in the frequency and severity of hot flashes were notably greater in the lavender oil group (P = .001).
Conclusion
Primrose and lavender oils are both effective in reducing the frequency and severity of hot flashes and night sweats, but the lavender oil was more effective in reducing the frequency and severity of hot flashes and night sweats in postmenopausal women.
Introduction
Menopause is the absence of menstruation for more than 6 to12 months following the previous menstrual cycle. 1 It typically occurs between the ages of 45 and 55, although women may exhibit symptoms as early as age 40. 2 Symptoms of menopause can range in severity from mild to severe. These symptoms include vasomotor symptoms (VMS) like hot flashes and night sweats, and genital symptoms like vaginal dryness, joint pain, loss of sexual desire, anxiety, depressed mood, and irritability. 1
Hot flashes and night sweats can occur several times a day. Most of the time, they last a few minutes, although sometimes they last for an hour or longer. As the ovaries stop producing hormones during menopause, estrogen levels in the body significantly drop, and hot flashes are thought to be a result of this. 3 Hot flashes affect a woman's life, such as her work, recreational pursuits, sleep, and overall well-being.4–6
The primary treatment for hot flashes and night sweats is menopause hormone therapy (MHT). However, this treatment has some negative consequences. 7 Thus, numerous studies have supported the use of complementary and alternative therapies such as herbal medicines to promote health and relieve menopausal symptoms.8,9
Primrose and lavender oils are among the herbal medicines that can be used to treat menopausal symptoms. Primrose, also known as Oenothera biennis, belongs to the Onagraceae family. It contains fixed oils such as linoleic acid, gamma-linolenic acid, and palmitic and oleic acids. Linoleic acid and its other metabolites help reduce inflammation and support healthy skin function.10–13
Lavender, known as Lavendula angustifolia L., or L. officinalis, also contains volatile oils such as linalool and linalyl acetate. 14 It is usually used in perfumes, cosmetics, and household chemicals and has antibacterial, antifungal, antioxidant, 15 anti-spasmodic, anti-inflammatory, diuretic, and pain-relieving effects. It has also been used for its relaxing and sleep-inducing properties. 16 Lavender has been extensively used in the fields of psychosomatic obstetrics and gynecology to treat dysmenorrhea, ease labor and post-cesarean pain, lessen postpartum depression and anxiety, and reduce symptoms like arthralgia, hot flashes, melancholia, and myalgia. 17
The existing literature is conflicting regarding the effects of primrose and lavender oils on menopausal VMS. A study reported that lavender aromatherapy reduced menopausal hot flashes. 18 Some studies also concluded that the anxiolytic and relaxing properties of lavender oil may contribute to the reduction of VMS in menopausal women. 19 Similarly, a study reported that the use of evening primrose oil can decrease postmenopausal hot flashes. 20 On the other hand, a study examining the effects of primrose oil and black cohosh on menopausal hot flashes showed that both herbs effectively reduced the severity of hot flashes, although black cohosh was superior. 18 Contrarily, another study found that primrose oil capsules did not significantly reduce the duration, frequency, and severity of hot flashes. 21 Such inconsistencies can lead to hesitancy among healthcare providers and patients alike. Furthermore, no studies have compared the effects of primrose oil and lavender oil on menopausal hot flashes and night sweats. Therefore, the question arises, among lavender oil and primrose oil, which one is more effective in treating hot flashes/night sweats in menopausal women?
Research Hypotheses
H1: Menopausal women who receive primrose oil or lavender oil versus control group may have lower total mean scores regarding hot flashes frequency and severity index
H2: Menopausal women who receive primrose oil or lavender oil versus control group may have lower total mean scores regarding interference of hot flashes with daily life activities.
H3: Menopausal women who receive primrose oil or lavender oil versus control group may have lower total mean scores regarding hot-flashes/ night sweats problem-rating scale.
H4: There is a difference between menopausal women who receive primrose oil versus lavender oil in relation to frequency and severity of hot flashes and night sweats.
Outcome Measures
-
Objectives
Therefore, this study aimed to determine the effects of primrose oil versus lavender oil on hot flashes and night sweats among menopausal women.
Methods
Study Design and Participants
A double-blind, randomized, controlled trial was conducted with a total of 150 menopausal women. The study was conducted from October 2022 to April 2023.
The sample size was meticulously performed using a power analysis through G*Power software version 3.1.1; and the sample size calculated based on the primary outcome of the study which is the effectiveness of using primrose oil, lavender oil or a placebo on the frequency and severity of hot flashes and night sweats among menopausal women. To compare three independent groups, a one-way ANOVA test was chosen, the medium effect size (f = 0.25), the significance level (0.05), and the desired statistical power (80%) were assumed. 22 The total sample size needed was calculated to be 150; 50 for each group. Consequently, menopausal women were randomly distributed into three groups to receive either primrose oil, lavender oil, or a placebo.
The women were consecutively pooled from the women's care clinic at the Obstetrics and Gynecological Department of Kasr ElAiny University Hospital affiliated with Cairo University from October 2022 to April 2023. This unit provides free obstetrics and gynecological health services for low-risk and high-risk pregnant and non-pregnant women and counseling for family planning. The meeting with the menopausal women was held on the second floor, where the community health and women's health nurses provide their services. The unit serves about 10,000 women with gynecological problems annually.
Two parts of the selection process were employed to guarantee randomization: recruitment and sample randomization. First, computer-generated random numbers table were used to conduct a random allocation recruitment of the women. We assessed 250 menopausal women to recruit 150 of them randomly with the inclusion criteria. Allocation concealment was carried out using sealed, sequentially numbered and opaque envelopes in this study. Another person who wasn’t involved in the data collection and interaction with the sample prepared the contents of the envelopes. Moreover, to preserve the blinding, the interventions, such as primrose oil, lavender oil, and placebo, were presented in the identical package in regard to appearance and labeling, and scent-masking procedures. Group assignments were also coded (Group A, B, C) and the treatment to receive was not revealed so that participants and the research personnel could be unaware of the type of intervention being applied. (Figure 1). Following the necessary training, two nurses at the women's care clinic performed the group allocation procedure, with the principal investigator remaining uninvolved.

The Study Flow Diagram.
Inclusion criteria included women aged between 40 to 60 years, able to read and write, experienced amenorrhea for > 6 months, complaining of mild or moderate-to-severe hot flashes and night sweats at least twice a day during a routine gynecologic consultation, no abnormal vaginal bleeding, normal blood pressure, no known kidney or liver disorders, no history of convulsion, and no allergy to herbal remedies. Exclusion criteria included incomplete completion of questionnaires or incomplete use of oils, getting a serious disease during the study, an explanation for hot flashes other than natural menopause, and the use of hormonal medications or herbal treatments in the preceding two months to treat hot flashes or night sweats. I specify those exclusion criteria to maintain data integrity, internal validity of the findings and overcome any extraneous factor that may affect the outcome. This study was reported in accordance with the CONSORT 2025 guidelines for randomized controlled trials. 23
Data Collection Instruments
Four instruments were used to collect data. The first was a structured interviewing questionnaire schedule designed by the researcher to assess the participant's age, education level, place of residence, occupation, age at menarche, the interval between menses, duration of menstruation, age at menopause, regularity of menstruation, hysterectomy, or oophorectomy. The content validity and face validity of this instrument were confirmed by three experts in the field of maternity and community nursing.
The second to fourth instruments were Sloan's daily hot flashes/night sweats diary, the Hot Flash/Night Sweat Problem Rating (HFNSPR), and the Hot Flash Related Daily Interference Scale (HFRDIS). 24
Sloan's HFNS diary is a self-report diary where women document how many hot flashes they experience each day and the severity of each on a scale from “1 = mild” to “3 = severe”. A weekly hot flash frequency score is created by averaging the number of hot flashes over 7 days. The daily severity score is calculated by summing the number of hot flashes reported at each severity level, and a hot flash severity index is calculated using the sum of daily severity scores over seven days. The total number of hot flashes per day is added to determine the hot flash severity score for each day. 25 this is the formula of Mean Hot Flashes Severity Index; severity score = (number of mild hot flashes/ day ×1) + (number of moderate hot flashes/ day ×2) +(number of sever hot flashes/ day ×3)/ total number of hot flashed/ day. Higher scores indicate worse symptom as there is no maximum score science the score is patient dependant for both number and severity. The tool is formally validated and is acceptable for use clinical trial 26
The HFNSPR is a self-report measure developed by Hunter and Liao to assess the impact of HFNS and how problematic they feel. It consists of three items, each rated on a 10-point Likert scale to determine how bothersome, distressing, and disruptive HFNS are to daily life. The three questions are averaged to determine the problem rating, with higher scores indicating more troublesome situations. The internal consistency (alpha = 0.87) and test-retest reliability (r = 0.8) of the HFRSPR are good. 25 Also, the problem rating scale is significantly correlated with the HFRDIS (Carpenter), r = 0.74, P 0 < 0.001 27
The 10-item HFRDIS was developed by Carpenter (2001) to examine how hot flashes disrupt a woman's daily life. The first nine items examine how well people can perform their daily activities, including their work, social connections, leisure pursuits, sleep, mood, concentration, interpersonal relationships, sexuality, and general happiness in life. The overall QOL is assessed in the last item. All items are rated on a scale from “0 = do not interfere” to “10 = totally interfere”, with women rating the extent to which hot flashes had disrupted their activities in the past week. The sum of the individual items yields a score between 0 and 100, with higher scores indicating a greater impact on activities of daily living. Scores from 0 to 33, 34 to 67, and 68 to 100 are interpreted as mild, moderate, and severe interference, respectively. 25 The HFRDIS was internally consistent, where its alphas reached an alfa value of 0.96 at times 1 and 2. The validity was addressed by (1) correlations with other hot flash variables, (2) correlations with affect and mood measures (3) significant differences between women with and without hot flashes, and (4) sensitivity to changes over time. The HFRDIS is a valid psychometric instrument to evaluate the effect of hot flash on everyday task performance and quality of life when used in clinical or research studies. 28
Cultural Adaptation and Content Validity
The second to fourth instruments was validated nationally as mentioned before in the description of each instrument but there is no regional validation has been reported so the instruments went through multiple process to ensure cultural adaptation; firstly, conducting translation by an expert to ensure linguistic appropriateness relevance to Egypt. Then The content validity of the tools was reviewed by a panel of 5 expert from Faculty of Nursing/ Cairo University, maternal and newborn health nursing and Community Health Nursing. They reviewed length, overall appearance, format, wording, content, item sequence, clarity, and coverage of the tools. The researchers made the necessary adjustments after the experts evaluated the study tool. After that a pilot study was conducted on 10% of the sample (15 postmenopausal women) who were excluded from the study. The primary objective of a pilot study was to find out the understandability and applicability of the study tool. Based on this stage it was possible to get feedback on the tool itself, more concretely, on the level of its understandability. And thus, there was no need for more extensive changes. The reliability of tools was tested using Cronbach's alpha test, and the result was highly reliable (0.74 &0.82 & 0.78) for tools (2, 3 & 4).
Preparation of the Oils
We purchased the primrose oil and lavender oil from AYURVEDA (natural care product). We also used a carrier oil as a placebo that did not contain the active substances. The placebo oil was prepared in bottles of a similar shape and color to those used for primrose and lavender oils.
The analysis of the fatty acid profile of primrose oil received from the market is crucial for verifying the validity of the oil and the assurance of the consistency of the results. The analysis was carried out using gas chromatography coupled to mass spectrometry (GC/MS) following a standard protocol. The chemical composition of the lavender oil sample was performed using a Trace GC-TSQ mass spectrometer (Thermo Scientific, Austin, TX, USA) with a direct capillary column TG–5MS (30 m×0.25 mm × 0.25 µm film thickness). The column oven temperature was initially held at 50 °C and then increased by 5 °C /min to 250 °C, held for 2 min. increased to the final temperature 300 °C by 30 °C /min and hold for 2 min. The injector and MS transfer line temperatures were kept at 270, and 260 °C, respectively; Helium was used as a carrier gas at a constant flow rate of 1 mL/min. The solvent delay was 4 min, and diluted samples of 1 µL were injected automatically using Autosampler AS1300 coupled with GC in the split mode. EI mass spectra were collected at 70 eV ionization voltages over the range of m/z 50-650 in full scan mode. The ion source temperature was set at 200 °C. The components were identified by comparison of their mass spectra with those of WILEY 09 and NIST 14 mass spectral databases. 29 (Table 1).
GC/MS Analysis of Lavender Oil.

Abbreviation: Rt, retention time.
The GC-MS results of lavender oil revealed the detection of 12 identified peaks comprising 85% of the total peak areas. Linalool and linalyl acetate were the major components of the oil with relative percentages of 20.19% and 22.68%, respectively. In addition, eucalyptol, camphor, borneol, and bornyl acetate were detected in 6.20, 2.65, 1.80, and 1.80%, respectively. The overall GCMS profile of the oil is by the published data regarding lavender oil from different localities.30,31
Preparation of Primrose oil for GC-MS Analysis
To 10 mg of the oil, H2SO4 -methanol 2% (v/v) was added into a glass vial. The vial was heated at 80 °C, then 0.25 mL of 1 M sodium hydroxide was added. The mixture was cooled to room temperature, and 1 mL KCl (0.8 M) was added with vigorous shaking. 1 mL of hexane was added to the previous mixture and vigorously shaken, and the upper organic layer was used for GC/MS analysis. 32 Regarding the GC/MS analysis of the saponifiable part of primrose oil, linoleic acid was found to be the major constituent, comprising 45.67% of the total fatty acid methyl esters (FAME). Oleic acid was the second major identified unsaturated fatty acid (32.62%). In addition, stearic acid and palmitic acid were the major saturated fatty acids, comprising 11.90% and 3.24%, respectively. Finally, a significant amount of Vitamin E (5.41%) was identified. The fatty acid profile of primrose oil is in accordance with the previous literature.11,33 (Table 2).
Fatty Acid Methyl Ester (FAME) Profile of the Saponifiable Part of Primrose oil.

Regarding the placebo oil was a mineral oil that was free of any odor and similar in texture and color to the active oils in that it had no documented therapeutic value. to reduce any bias, all the oils were prepared in the same opaque containers with only the pharmacist knowing the codes written on the containers. The oils appeared similar and whereas lavender oil was less aromatic, participants, interventionists and assessors were blinded regarding group assignment. Although, the research team made efforts to reduce smell-related stimuli for lavender and advice the users not to smell the oil intentionally, the distinctive scent of the lavender oil may be source of bias.
Intervention
Data collection was started after receiving permission from the administrative authorities of the aforementioned women's care clinic. Data was collected four days per week, over a seven-month period, beginning in October 2022 and ending in April 2023. Each group underwent four stages, including baseline assessment, intervention, follow-up, and final evaluation.
The baseline assessment included structured individual interviews to collect participants’ demographic characteristics and menstrual- and menopausal-related information. This interview was conducted in the waiting room of the women's care clinic. Then, the women were provided with Sloan's HFNS diary, the HFNSPR, and the HFRDIS to be completed as self-reports. The trained nurses who worked as research assistants were available to help the women in completing the questionnaires and respond to their questions, if any. The baseline assessment took about 35 min for each woman.
In the intervention phase, women in all groups were trained to apply one teaspoon of the given oil on the abdomen near the umbilicus, the bottoms of the feet, and the neck areas twice daily (every 12 h) for 15 min for 8 weeks. Women were advised to shake the oil bottle well before using it and store it in a cool and dark place. The researcher educated the women on how to use the oil by using pictures, booklets, and demonstrations. The treatment period was set at eight weeks, as this is the minimum duration required to demonstrate the long-term efficacy of a non-hormonal compound.7,34
The follow-up and final evaluation were carried out by telephone calls at the fourth and eighth weeks post-treatment. The Sloan's HFNS diary, the HFNSPR, and the HFRDIS were again completed through these telephone calls. Each telephone call lasted about 20 min. The telephone calls were conducted by trained personnel to ensure consistency all over the calls. The women were asked to record the frequency and severity of their hot flashes daily within seven days of consecutively. Then the researched obtained the women response through the call at the end of the day and recorded them then saved the responses into secure data base.
Ethical Considerations
Permission was obtained from the Research Ethics Committee of the Faculty of Nursing, Cairo University, Egypt (Code: 2022) with the final approval number RHDIRB2019041701 on 26 April 2023 and recorded in the Cairo University Registry of Clinical Trials with the registration number: NCT05988242. Moreover, oral explanations of the trial's significance and goal were given to each participant. Informed written consent was obtained from all participants, and all of them were informed that the study was voluntary and open to withdrawal at any moment. Additionally, the anonymity, secrecy, and privacy were all upheld.
Data Analysis
In this study, we conducted an intention-to-treat (ITT) approach. This approach involves analyzing participants’ data, regardless of whether they completed the intervention or not. But in our study we didn’t have any excluded cases. Statistical analyses were conducted using SPSS version 28 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including frequencies, percentages, means, and standard deviations, were calculated to summarize the participants’ characteristics and their menstrual and menopausal data. To assess the normality of the study variables, the Kolmogorov-Smirnov test was utilized. When comparing two or more independent samples with the same or different sample sizes Kruskal-Wallis test was utilized
The chi-square test was used to compare the groups for their categorical data. Analysis of variance (ANOVA) and Tukey post-hoc test were used to compare the means of quantitative variables between the three groups. The significance level was set at ≤ 0.05.
Results
The Demographic Characteristics and Menstrual History of the Women in the Three Groups.
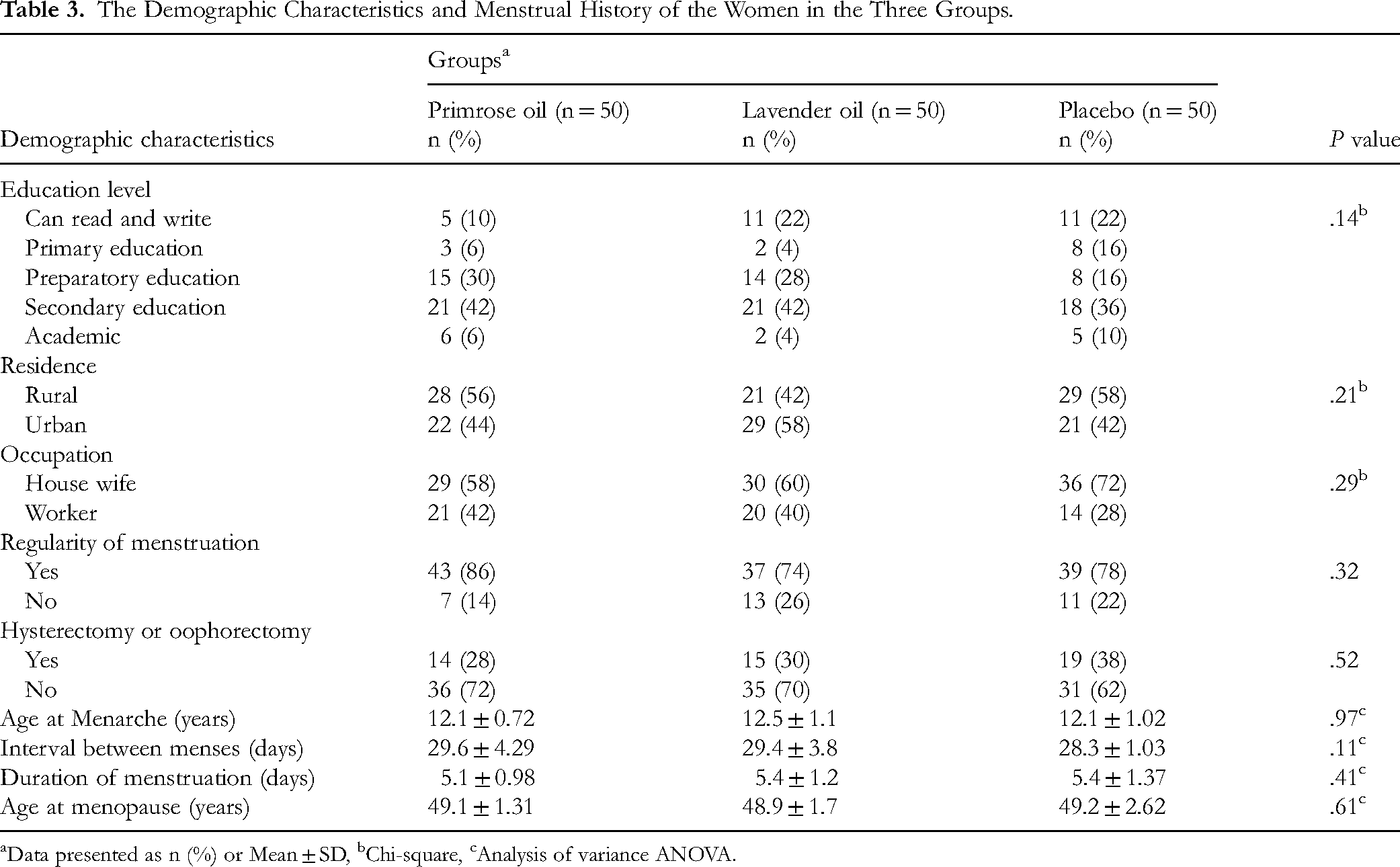
Data presented as n (%) or Mean ± SD, bChi-square, cAnalysis of variance ANOVA.
Comparison of the Mean Total Daily Interference of hot Flashes and Night Sweats, the Mean Frequency of hot Flashes, and the Mean hot Flashes Severity index among Women in the Three Groups.
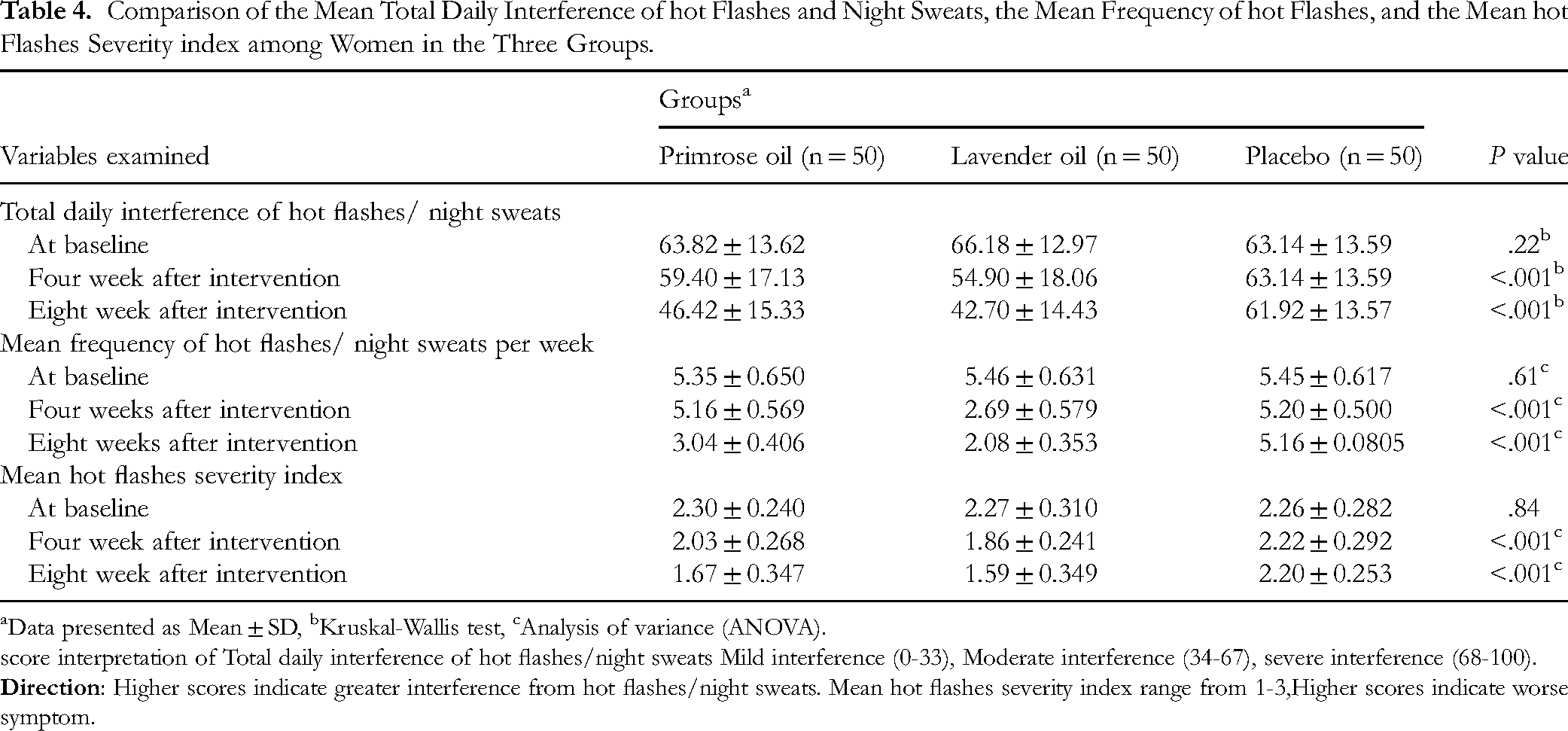
Data presented as Mean ± SD, bKruskal-Wallis test, cAnalysis of variance (ANOVA).
score interpretation of Total daily interference of hot flashes/night sweats Mild interference (0-33), Moderate interference (34-67), severe interference (68-100).
Effect Size and Confidence Intervals 95% Between Lavender oil VS Primrose oil Group at Four Week After Intervention.

Table 6 shows lavender group had a significant improvement in hot flash severity showing a much lower rate of severity than placebo group (mean difference = –0.61; 95% confidence interval = –0.73 to −0.49; mean = –1.96), which is indicative of a clinically significant change. As illustrated in Table 6, the decreases in the frequency and severity of hot flashes were notably greater in the lavender oil group. The Tukey post-hoc test showed that the superiority of the lavender oil in reducing the mean frequency of hot flashes was statistically significant at both the end of the fourth (P < .001) and eighth weeks (P = .003). However, the superiority of lavender oil in reducing the mean severity of hot flashes was statistically significant only at the end of the fourth week (P < .01) (Table 7).
Effect Size and Confidence Intervals 95% at Eight Week After Intervention.

Post-hoc Pairwise Comparison of the Mean Frequency and Total Severity of hot Flashes Between the Study Groups at the Three Measurement Times.a

Data presented as P value\ Post-hoc pairwise comparison using Tukey post-hoc test.
At baseline, all participants had moderate or severe hot flashes. However, in the fourth week, 8% of women in the primrose oil group and 16% in the lavender oil group experienced mild hot flashes. Moreover, the proportion of women experiencing mild hot flashes in the primrose oil group and the lavender oil group increased by 22% and 32%, respectively, in the eighth week (Table 8).
Distribution of Women According to the Severity of hot Flashes and Night Sweats Before and After the Intervention.a
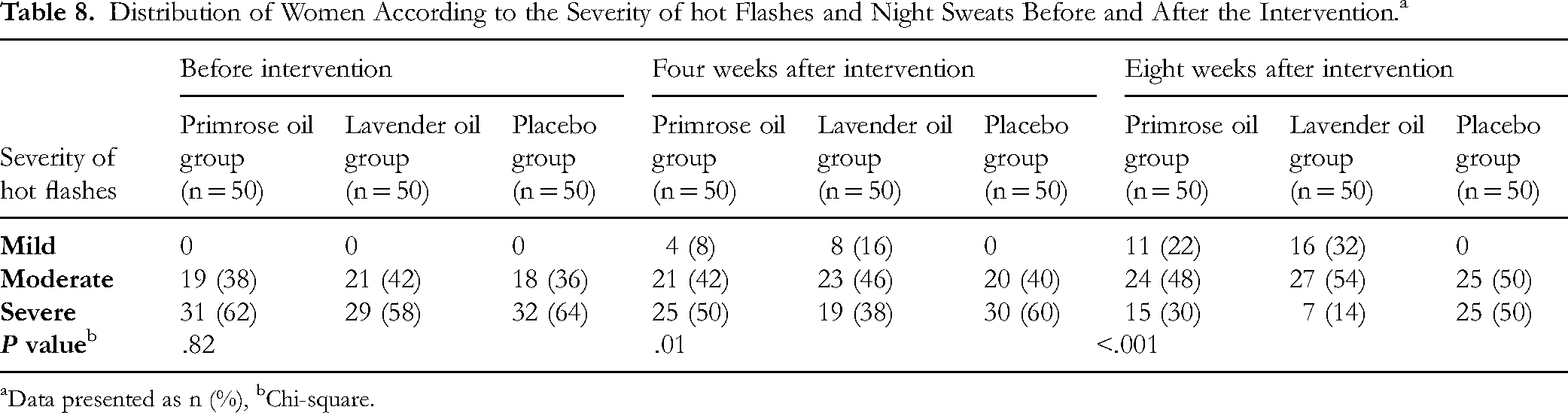
Data presented as n (%), bChi-square.
Discussion
The present study demonstrated that the use of lavender or primrose oils for eight weeks significantly reduced the interference of hot flashes/night sweats on the daily activities of postmenopausal women. Although lavender oil demonstrated superior efficacy to primrose oil in reducing the interference of hot flashes/night sweats on the daily activities of menopausal women. As the mean interference did not change notably in the placebo group during the study, the reduction in the treatment groups can be confidently attributed to the effects of the oils. No previous studies have compared the effects of lavender oil and primrose oil on the interference of hot flashes in the daily activities of postmenopausal women. However, our findings are consistent with those of a previous study that demonstrated the effectiveness of oral primrose oil on the improvement of menopausal hot flash frequency, severity, and duration. 20 This study suggests that primrose oil has a positive effect on a key menopausal symptom. In the same line another study give evidence on the positive health effects of evening primrose oil on the mental health of postmenopausal women. 35
In harmony with our findings, a study also found that lavender oil aromatherapy could effectively improve sleep quality and QOL in postmenopausal women. 36 The latter study suggests that despite differences in methodology, lavender oil may have a broader spectrum of benefits in menopausal women that may potentially make it a more holistic treatment option in menopausal women.
In the present study, both the lavender and primrose groups experienced a substantial decrease in the mean frequency and severity of hot flashes in both the fourth and eighth weeks after the intervention. A systematic review also concluded that several herbs, including evening primrose oil, can help reduce both the intensity and frequency of menopausal hot flashes and their side effects. 37 Another study also showed the advantages of evening primrose oil on menopausal vasomotor symptoms. 10 These findings are somewhat incongruous with a study that examined the effects of evening primrose oil capsules on hot flashes and night sweats in postmenopausal women and found that the intervention did not significantly reduce the mean duration, frequency, and severity of hot flashes, although it could decrease the frequency and intensity of night sweats. 38 Some other studies also reported that lavender aromatherapy could improve the QOL and reduce the severity of physical and psychological symptoms in postmenopausal women.18,39 Our findings, along with other studies, support the effectiveness of both lavender and primrose in the alleviation of menopausal symptoms. However, some differences in outcomes may be attributed to the distinct intervention modalities. For instance, our study used primrose oil and lavender oil ointments, while some studies used it in capsule 38 or aroma18,39 forms. Nevertheless, further research is needed to support the evidence that alternative medications can alleviate menopausal symptoms.
The mechanisms by which lavender and primrose oils alleviate menopausal symptoms such as hot flashes and night sweats are not fully known, yet some theories exist. Lavender oil, with compounds like linalool and linalyl acetate, may calm the nervous system 40 and help regulate body temperature. 41 Primrose oil contains gamma-linolenic acid, which could reduce inflammation and influence hormone balance, lessening menopausal symptoms. 42 Essential oils might also have estrogen-like effects, but more research is needed to understand this. 43 Both oils can be locally applied for absorption and possible relief, but their detailed mechanisms and effects require further study.
This study has some limitations. Firstly, a lack of national and international research comparing the impact of primrose and lavender oil on menopausal symptoms as it limits the capacity to justify the findings in a large body of literature. Second, this study had a limited sample size and no long-term follow-up. Also limited inclusion criteria in the diagnosis of menopause like analysis of gonadotropin releasing hormone as increasing GNRH levels may classify a woman with amenorrhea as experiencing menopause or other medical issues. Moreover, another limitation is associated with the intention-to-treat (ITT) principle. Although the generally accepted rules of ITT analysis apply to all the participants as originally randomized, some exclusions were made under this study, as mentioned in the sample part. Such exclusions were made to avoid confounding and maintain the internal validity of the research, but it could have brought about biasness and diverted the research to be other than ITT. It is recommended to use per-protocol analysis and modified ITT analysis in the future to ensure the exploration of such factors and maintain strict methodology. Future studies should be conducted with a bigger sample size and long-term follow-up to generalize the result. Also, the frequency of VMS in this sample of women was very low (5 per week, which reduced to an average of 2-3 in the treated groups). Similarly, Mean hot flashes severity index at base line was 2.30 and reduce after intervention to 1.6 which would be considered not to be much of a problem at all, which may limit the generalizability of the findings.
Conclusions
Both primrose and lavender oils reduce hot flashes and night sweats in postmenopausal women, but lavender oil is more beneficial. Menopausal women can use one of these herbal products, based on their personal preferences, to reduce their symptoms. It is recommended that counseling programs be developed for women at primary health care centers about the effective use of herbal remedies like lavender or primrose oil to manage menopausal symptoms. It is also recommended to replicate the study on a larger probability sample to achieve more generalizability.
Footnotes
Acknowledgment
We would prefer to express our gratitude to all women who participate in this study.
Ethical Considerations
Permission was obtained from the Research Ethics Committee of the Faculty of Nursing, Cairo University, Egypt (Code: 2022) with the final approval number RHDIRB2019041701 on 26 April 2023 and recorded in the Cairo University Registry of Clinical Trials with the registration number: NCT05988242.
Statement of Informed Consent
Written informed consent was obtained from the women for their anonymized information to be published in this article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the research Ethics Committee of the Faculty of Nursing, Cairo University, Egypt (Code: 2022), with the final approval number RHDIRB2019041701 on 26 April 2023 and recorded in the Cairo University Registry of Clinical Trials with the registration number: NCT05988242, URL: ![]()
Authors’ Contributions
F. Zaghloul & L. Saad: Conceptualization, Methodology, Supervision, Writing – original draft.
W. Alanazy& D. Mohamed: Data curation, Formal analysis, Visualization.
W. Mahmoud & E. Alshawish & A Abd El-azeem: Writing – review & editing, Project administration.
Ali M. El Halawany: Investigation, Resources.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data used in this study are available from the corresponding author on request.