
Abstract
Purpose:
Uterine activity plays a key role in reproduction, and altered patterns of uterine contractility have been associated with important physiopathological conditions, such as subfertility, dysmenorrhea, and endometriosis. However, there is currently no method to objectively quantify uterine contractility outside pregnancy without interfering with the spontaneous contraction pattern. Transabdominal electrohysterography has great potential as a clinical tool to characterize noninvasively uterine activity, but results of this technique in nonpregnant women are poorly documented. The purpose of this study is to investigate the feasibility of transabdominal electrohysterography in nonpregnant women.
Methods:
Longitudinal measurements were performed on 22 healthy women in 4 representative phases of the menstrual cycle. Twelve electrohysterogram-based indicators previously validated in pregnancy have been estimated and compared in the 4 phases of the cycle. Using the Tukey honest significance test, significant differences were defined for P values below .05.
Results:
Half of the selected electrohysterogram-based indicators showed significant differences between menses and at least 1 of the other 3 phases, that is the luteal phase.
Conclusion:
Our results suggest transabdominal electrohysterography to be feasible for analysis of uterine activity in nonpregnant women. Due to the lack of a golden standard, this feasibility study is indirectly validated based on physiological observations. However, these promising results motivate further research aiming at evaluating electrohysterography as a method to improve understanding and management of dysfunctions (possibly) related to altered uterine contractility, such as infertility, endometriosis, and dysmenorrhea.
Introduction
Uterine activity is most evident during pregnancy when it culminates in the expulsion of the fetus at the end of the delivery. However, uterine activity plays a key role in different, possibly related, aspects of reproduction outside pregnancy as well.
Uterine activity is known to affect embryo implantation in animals. 1 –3 In healthy, nonpregnant, human uteri, previous research consistently reported specific contractile patterns that evolve during the menstrual cycle. 4 –6 These evolving patterns are in line with the hypothesis of a functional role of uterine motion in normal menstrual cycles to promote fertilization. 1,5,7,8 Furthermore, there is evidence that disruption of these natural properties is the cause of a number of dysfunctions, including subfertility, dysmenorrhea, endometriosis, and adenomyosis. 9 –11
An increasing percentage of couples, currently 20%, have difficulties conceiving. 12,13 Approximately half of these subfertile couples seek medical care services and eventually recur to assisted reproduction. 14,15 In spite of major efforts to improve assisted reproductive technology over the past 20 years, the overall effectiveness remains below 30% per treatment cycle, even for in vitro fertilization (IVF). 16
Embryo implantation is the factor with the greatest limitation on IVF. 17 Successful establishment of a pregnancy after embryo transfer is governed by complex mechanisms, 18 which depend on the quality of the embryo as well as uterine receptivity. 19,20 While classically, uterine receptivity has been identified with the histological and biochemical readiness of the endometrium to accept an embryo, uterine quiescence has been recently suggested as an additional determinant for the successful establishment of pregnancy after embryo transfer. 4,17,21 –24
Dysmenorrhea occurs in up to 50% of menstruating females. Dysmenorrhea is characterized by fluctuating, spasmodic pelvic cramps that begin shortly before or at the onset of menses and last 1 to 3 days. 25 This debilitating pain can lead to a woman’s failure to function normally during menstruation, making them unable to perform regular daily activities. Dysmenorrhea is associated to abnormalities in uterine activity, including elevated basal tone and active pressure, increased contraction frequency, and lack of rhythm and coordination. 26 Yet, the link between the contraction pattern, the degree of dysfunction, and the effectiveness of treatment has never been defined.
Endometriosis is a chronic disease characterized by development of endometrial tissue outside its normal location in the uterus. Its prevalence approaches 10% to 15% of the general female population and is associated with pain, dysmenorrhea, and, in 30% of the women, with infertility. 27 Unfortunately, the links among these diseases, particularly between endometriosis and infertility, are unclear, even though the association is clinically recognized. 28 In line with the theory that links retrograde menstruation to migration of viable endometrial cells that attach and implant in the pelvic cavity, altered uterine contractility is hypothesized to play a key role in endometriosis. 29 Unfortunately, etiology and pathogenesis of this disorder remain uncertain, hampering any progress for new treatment for disease associated with pain and infertility. 30
In fact, the lack of an objective and noninvasive tool for quantifying contractility in nonpregnant women has limited the possibility of investigating the complex and largely unknown mechanisms underlying uterine contractility and to quantify their impact on reproduction and in dysfunctions, such as subfertility, dysmenorrhea, and endometriosis. 4,9
In nonpregnant humans, uterine activity has been first explored by using invasive intrauterine pressure catheters, 7,10,31 magnetic resonance imaging, 5,32,33 and hysterosalpingoscintigraphy. 5 Unfortunately, these methods are unfeasible for routine use during IVF procedures and checkups because they are invasive, expensive, or employing ionizing radiations. 4,34 Visualization of uterine contractility by transvaginal ultrasonography has been recently more extensively used due to the availability and noninvasiveness of ultrasound (US). 10 However, this visual approach, based on either unprocessed image sequences 5,9,11,35 –44 or derived anatomical motion-mode images, 17 is operator dependent and thus difficult to reproduce for follow-up and comparative studies. 45,46
As an alternative to current diagnostics, transabdominal electrohysterography has been successfully proposed to characterize uterine contractions during pregnancy. 47 –52 The electrohysterogram (EHG) measures the electrical activity that triggers and drives the mechanical contraction of the uterus. The EHG signals can be recorded noninvasively by electrodes placed on the abdominal skin. 53,54 Being related to the root cause of the uterine muscle contraction, the EHG can potentially allow for a complete characterization of uterine activity also in the nonpregnant uterus. However, descriptions of EHG measurements on nonpregnant humans mainly focus on recordings performed directly on the uterus or on the cervix. 55,56
In this article, we evaluate for the first time (to our knowledge) the feasibility of transabdominal electrohysterography for the analysis of uterine contractions in healthy nonpregnant women, aimed at understanding the electrophysiology of uterine contractions during the menstrual cycle by a noninvasive approach.
Material and Methods
Patients and Study Protocol
All measurements were performed at the Gynecology Department of the Catharina Hospital in Eindhoven (NL) after approval by the relevant medical ethical committee (protocol NL52466.100.15). After signing an informed consent, 22 women were enrolled in the study. The inclusion criteria were an age between 18 and 40 years and a regular, natural menstrual cycle. Exclusion criteria were ongoing pregnancy, mental disability, significant language barrier, and cesarean delivery in the past. Uterine anomalies (congenital or noncongenital), uterine pathologies (leiomyomas, adenomyosis, and endometriosis), and infertility were additional exclusion criteria.
Women were recorded longitudinally at 4 predefined moments of the menstrual cycle, namely, during menses, which coincides with the early follicular (EF) phase, 57 in the late follicular (LF) phase, in the early luteal (EL) phase, and in the late luteal (LL) phase. All phases were in the same cycle. Menses dates were based on the last menstrual period. The LF phase, expected between day 11 and day 13 of the cycle, was established based on estimates of the follicle size measured on US images. The EHG measurements for the LF phase were performed only when one of the follicles had a diameter larger than 16 mm. The EL and LL phases were set at 3 and 7 days after ovulation, respectively. Blood tests were performed in order to measure hormone levels and exclude any hormonal unbalance that might contribute to dysfunctional uterine activity. 7 More specifically, concentrations of Luteinizing hormone (LH), Follicle-stimulating hormone (FSH), Estrogen and Progesterone were measured.
During each measurement session, 4-minute data were acquired. Based on the literature, depending on the phase of the cycle, at least 2 contractions can be expected to occur in this time range. 7
Eectrohysterogram Recording
After skin preparation for contact impedance reduction, the EHG was recorded by a flexible electrode grid placed on the abdomen immediately above the pubic bone (Figure 1). The correct placement of the abdominal grid was guided by US in order to maximize alignment with the uterus.
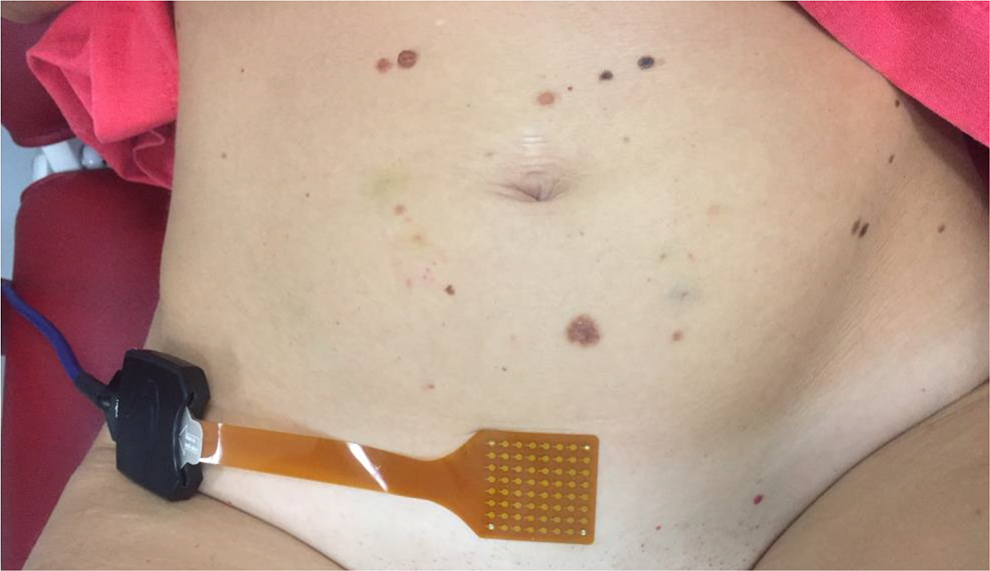
Electrode grid on the abdomen. The authors confirm permission from the woman to use this picture.
The adopted electrode grid (Figure 2) comprises an 8 × 8 array of electrodes (2 mm diameter, 4 mm distance). Such high-density electrode grids provide the augmented spatial resolution that might be necessary for analysis of EHG propagation properties in future work. 58,59 In this feasibility study, however, we focus on single-channel analysis for a qualitative evaluation of contraction timing and strength. 60 For this purpose, which does not require high-spatial resolution, the signal quality is improved by averaging neighboring electrodes and simulating larger sensing surfaces. 53,61 Furthermore, larger interelectrode distances are more suited than a high-density grid to investigate electrophysiological signals originated deeper as in the case on the nonpregnant uterus. 53,61 Furthermore, vertical derivations, aligned to the middle line of the muscle, are expected to be closer to the uterus and, therefore, provide a better signal to noise ratio. Two larger sensing areas, A and B in Figure 2, were, therefore, obtained by averaging the corresponding electrodes. Since bipolar derivations improve the signal quality by reduction of the common mode noise, a single bipolar signal was derived by subtracting the 2 sensing areas A and B. 62,63
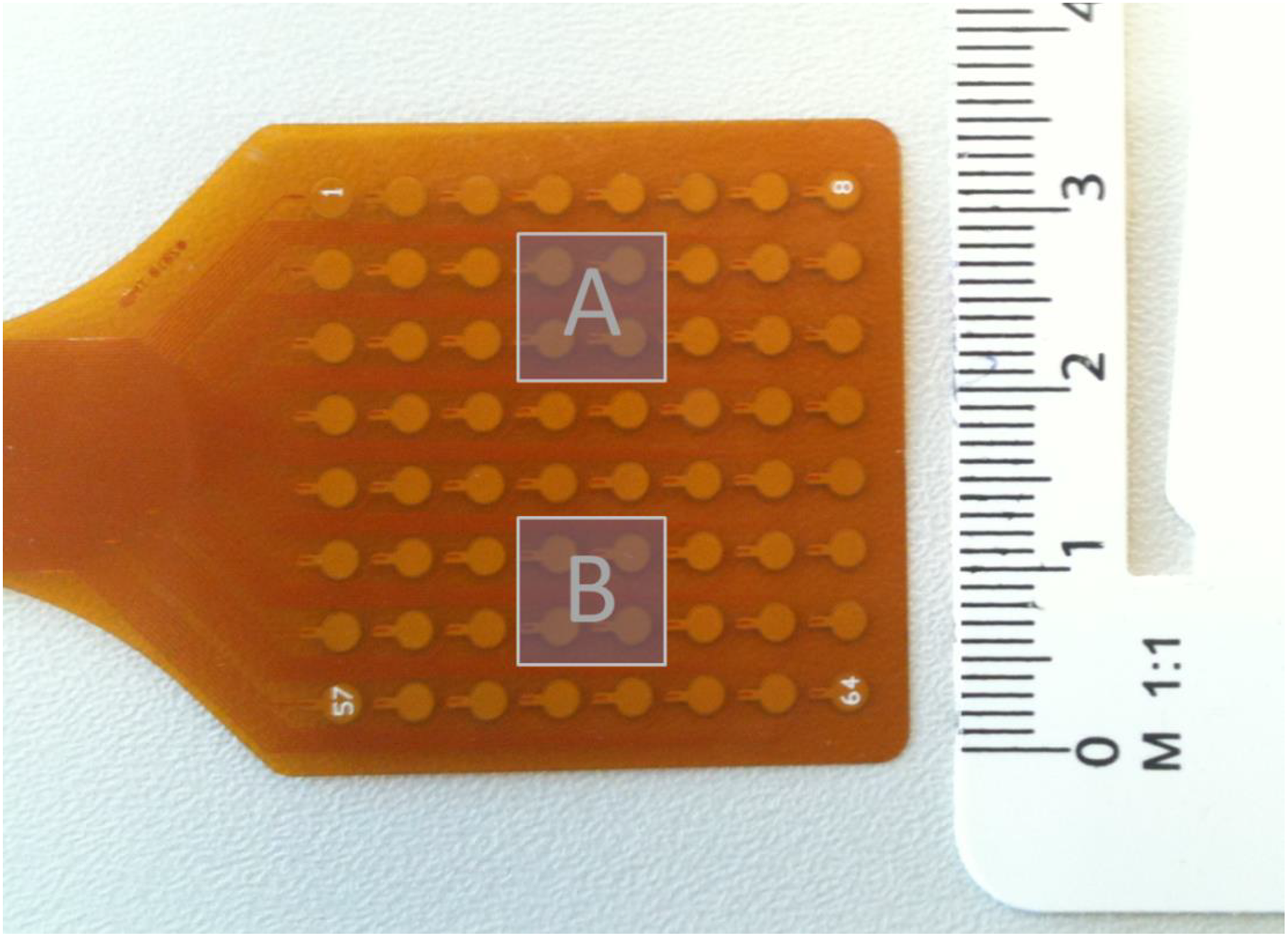
High-density electrode grid and schematic of the sensing surfaces A and B.
The EHG was then recorded and digitized, after the required antialiasing low-pass filtering, at a sampling frequency of 1024 Hz using a Refa system (TMS International, Enschede, the Netherlands), a multichannel amplifier for electrophysiological signals.
Feature Extraction
For each recording session, a set of features is extracted from the single-channel EHG signal. Depending on the chosen feature, the acquired signal is first preprocessed by dedicated prefiltering. 64,65 Features are then extracted following a 2-step approach: the preprocessed EHG is analyzed in step 1 in order to enhance specific properties of the EHG signal related to the contraction strength. Four different approaches, based on previous research on EHG analysis during pregnancy and implemented both in the time and in the frequency domain, are used in step 1 to provide a set of signals, referred to as (time-varying) features. From these features, the (global) indicators are extracted in step 2 and compared among the representative phases of the menstrual cycle for validation. The proposed approach for feature extraction is schematically described in Figure 3 using a recorded EHG signal as an example.
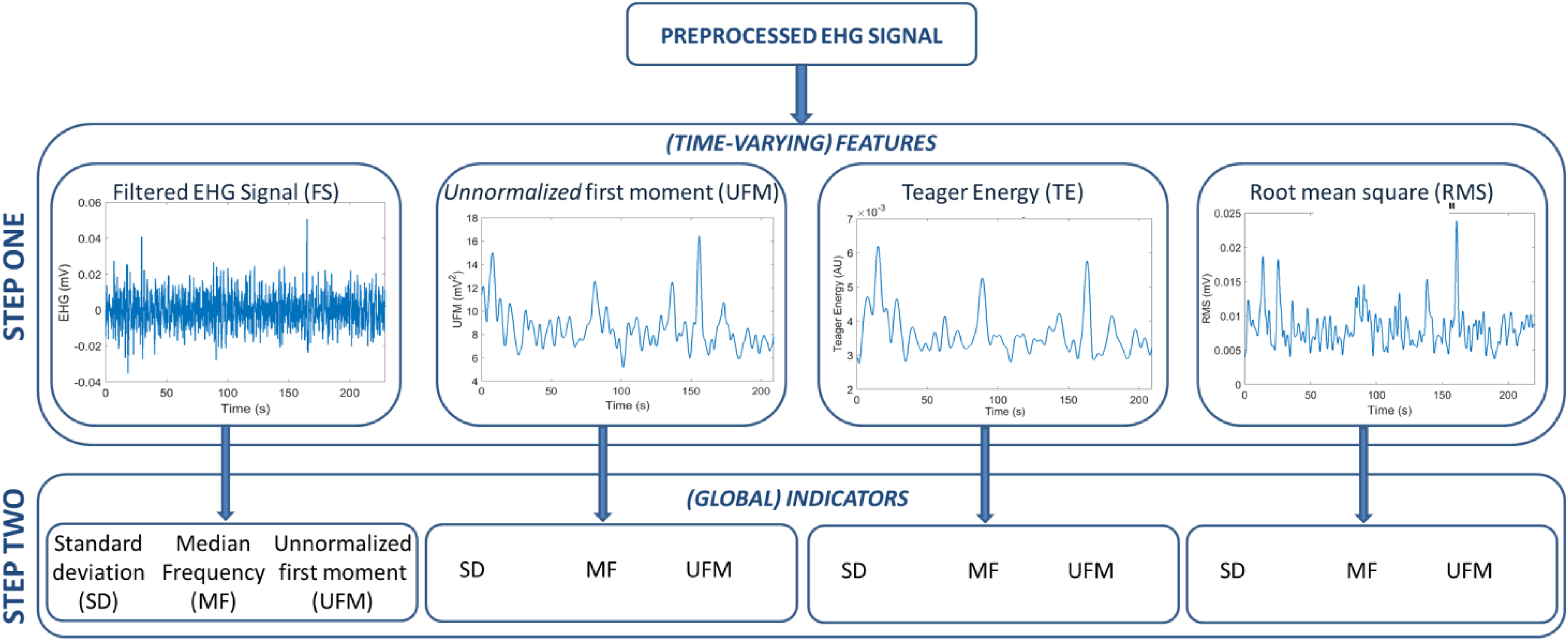
Scheme of the proposed approach for feature extraction. The same EHG signal recorded during the LF phase from one of the included women is shown as an example. EHG indicates electrohysterogram; LF, late follicular phase.
In clinical practice, timing and strength of uterine activity during pregnancy and delivery are assessed by direct or indirect measurement of the intrauterine pressure variations induced by contractions. 66 On pregnant women, previous research demonstrated an accurate measure of the intrauterine pressure variations related to uterine contractions by estimating the EHG signal energy. 60 The unnormalized first statistical moment (UFM) and its low-complexity alternative, the Teager energy (TE) operator, have been proposed in the previous literature for intrauterine pressure estimation. 67,68 The UFM is obtained as the product between the average signal frequency and the signal energy, both estimated in the time-frequency domain. 60 The TE operator is calculated in the discrete-time domain using a multiband solution for energy tracking. 68,69 In pregnancy, these frequency-weighted estimates of the signal energy seem, in fact, to provide a good representation of the hypothesized physiology of uterine muscle force development in response to electrical activity. 60 In this article, both the TE and the UFM are investigated as features and calculated in sliding windows similarly. 60,68 Signal amplitude estimations obtained by the root mean squared (RMS) and the band-filtered EHG signal (FS) are considered as 2 additional features (see Figure 3). 63,70,71 Further details of the feature extraction steps are provided in the subsequent section.
Prefiltering
The electrical signals originating from the activity of smooth muscles like the uterus are characterized by a low-frequency content. 72 For the uterus, frequencies below 5 Hz are expected, while the frequency band below 0.3 Hz can be seriously affected by movement artifacts related, for example, to respiration. 64,65 To estimate the intrauterine pressure increase by EHG analysis in pregnancy, frequency bands below 1 Hz have been previously adopted. 60,68,71,73 In fact, a better correlation with the invasively recorded intrauterine pressure was found in this frequency band while rejecting the maternal electrocardiogram. Nevertheless, during pregnancy, the EHG signal energy distribution extends beyond the upper frequency limit of 1 Hz. 70,74 –76 Analysis of our data suggests the EHG signal energy to show similar frequency distribution also outside pregnancy.
Due to the current lack of a reference golden standard, in this feasibility study, all features are derived in the 0.3 and 5 Hz frequency band, where an improved signal quality is expected. Preliminary tests confirmed that the interference due to the electrocardiographic signal, expected at frequencies as low as 1 Hz, 77 could be neglected due to the small interelectrode distance on the abdomen. For the TE, RMS, and BF, a fourth-order Butterworth filter with cutoff frequencies at 0.3 and 5 Hz is employed prior to calculation of the features. The definition of the UFM in the frequency domain allows estimation in the desired frequency band without prefiltering. 60
Time-Varying Features
The time-varying features have been calculated in 6-second sliding Han windows. The choice of the window type is in line with the previous literature, 68 while the window length is experimentally optimized in agreement with the frequency band of interest. In fact, this band allows to resolve the lowest frequency of interest (0.3 Hz) at a sufficient temporal resolution to enhance possible contractile events.
Indicators
Comparison of the considered phases of the menstrual cycle is then based on indicators subsequently extracted from the 4 chosen features. To this end, the standard deviation (SD), median frequency (MF), and UFM are estimated from each feature to form the set of indicators evaluated in the representative phases. These specific indicators, extracted from each of the above features (see Figure 3), were chosen in order to assess whether their frequency (represented by the MF), amplitude (as SD), or a combination of both frequency and amplitude (UFM) could be representative of the uterine activity in the considered phase. 70
Statistics
The indicators extracted in the 4 selected phases of the menstrual cycle, 12 in total, are compared using 1-way analysis of variance with repeated measures. Post hoc analysis is performed using the Tukey honest significance test (Tukey-Kramer method) and a significance level P = .05. 78
Results
Of the 22 women enrolled in the study, only 11 were eventually retained for the data analysis. Of the 11 women, 6 were excluded due to subfertility issues that emerged during or immediately after the study, 2 withdrew their consent after inclusion, and 3 could not attend the recording sessions, which resulted in an incomplete data set.
Of the 11 retained participants, 9 had a natural pregnancy shortly before or after the measurement, while 2 of them had no child wish at the moment of recording. At the time of measurement, women had an age between 25 and 39 years (31 years on average) and a cycle length between 24 and 40 days (29 days on average). Tests on the hormone levels did not show any unbalance, and figures were all within the expected ranges for healthy women in the presumed phase of the menstrual cycle. The average values of hormone test results are reported in Table 1.
Hormone Test Results.

Abbreviations: FSH-Follicle-stimulating hormone; LH-Luteinizing hormone.
As shown in Table 2, significance emerged only when the SD and the UFM were used as indicators. Instead, the use of the RMS as feature did not produce any significance difference among phases, independently from the adopted indicator.
Significance of feature Differences for Each Combination of Indicator Feature.
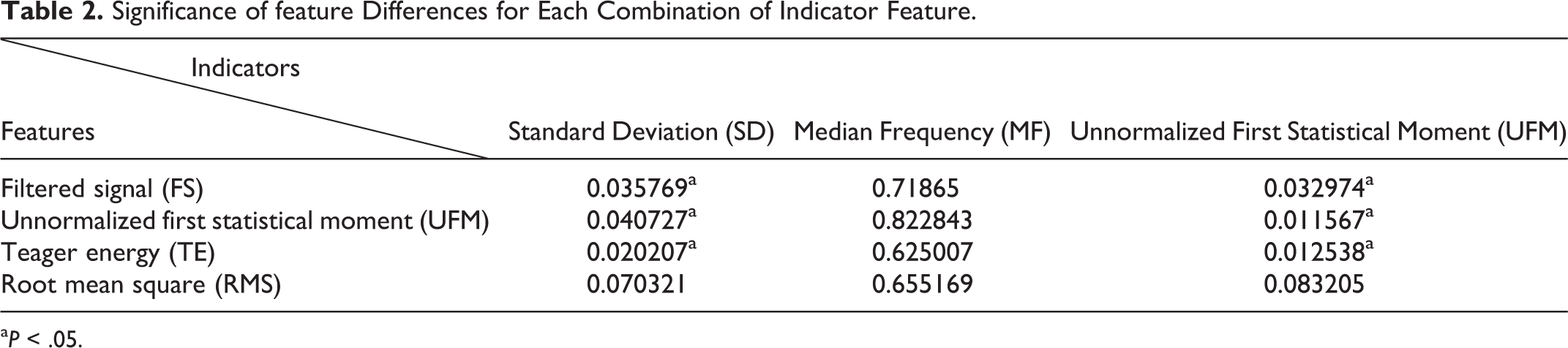
aP < .05.
The values of the derived indicators are plotted in Figures 4 to 6, in terms of average and SD. Normalized values are used to mitigate the impact of interpatient variability for improved visualization. Normalization was performed patient-wise, relatively to the LL phase. When SD and UFM are used as indicators, a decreasing trend along the cycle can be observed, which is absent in the results obtained by the MF indicator.
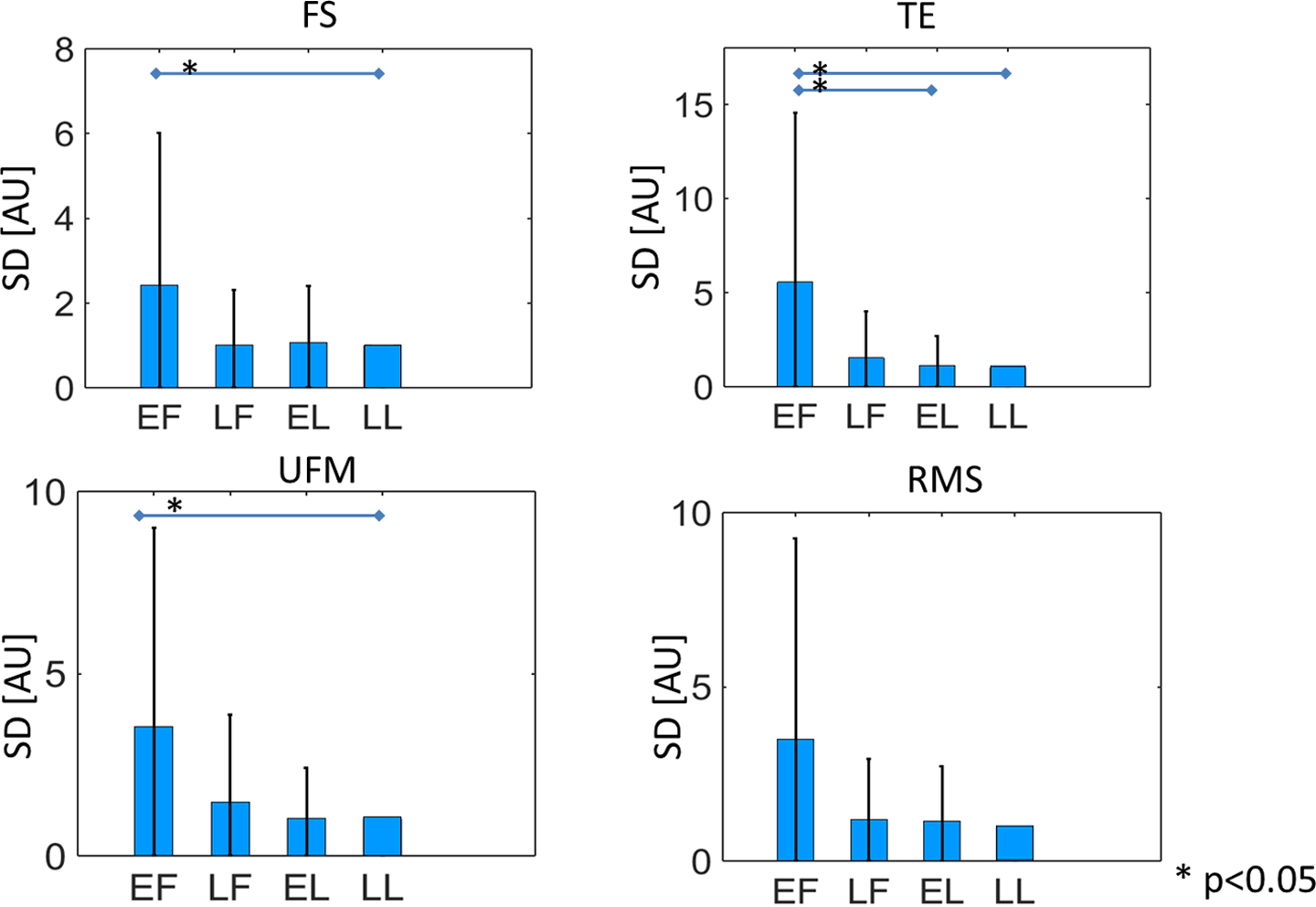
Value of the SD indicator (average and standard deviation [SD]) for different features in each of the evaluated cycle phases. Normalized values are used to mitigate the impact of interpatient variability for improved visualization.
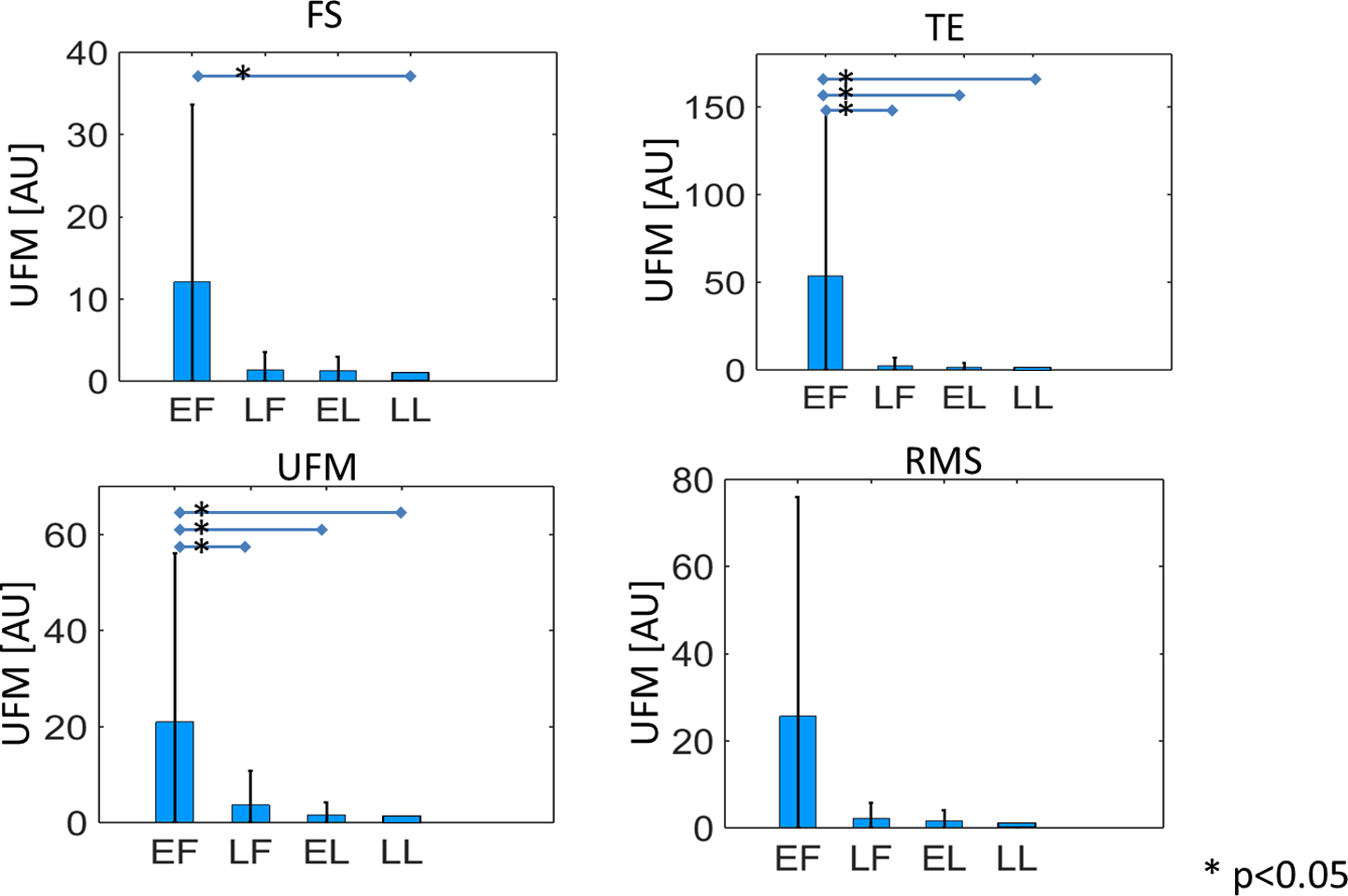
Value of the UFM indicator (average and standard deviation) for different features in each of the evaluated cycle phases. Normalized values are used to mitigate the impact of interpatient variability for improved visualization. UFM indicates unnormalized first statistical moment.
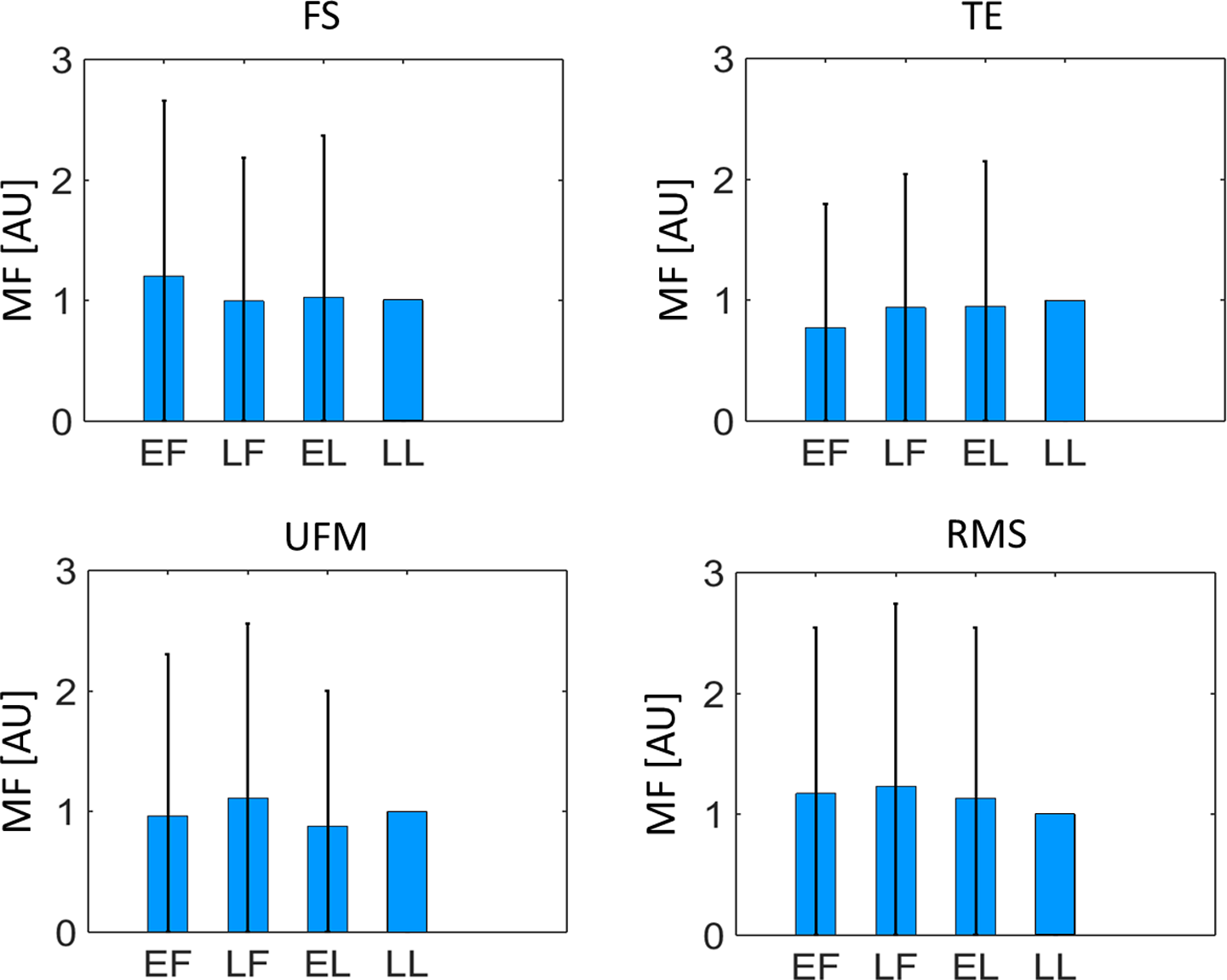
Value of the MF indicator (average and standard deviation) for different features in each of the evaluated cycle phases. Normalized values are used to mitigate the impact of interpatient variability for improved visualization. MF indicates median frequency.
Discussion
Uterine activity plays a key role in natural as well as in assisted reproduction. Furthermore, dysfunctional uterine activity is recognized among the main causes of important medical issues, including subfertility, dysmenorrhea, and endometriosis. 9 –11
Unfortunately, the lack of an objective method for uterine activity quantification hampers progress in understanding and treatment of these dysfunctions. This article studies for the first time the feasibility of transabdominal electrohysterography in the nonpregnant uterus. Electrohysterography measures the biopotential underlying the physiological process of uterine muscle contractions. Due to the lack of a golden standard for uterine contraction assessment outside pregnancy, an indirect validation approach is proposed in this study, which relies on the different motility patterns reported for the uterus at different stages of a physiological menstrual cycle. To this end, nonpregnant healthy women are measured longitudinally, at 4 selected representative phases of the menstrual cycle, namely, the EF, LF, EL, and LL phases.
During the cycle, the ovaries and the uterus undergo hormone-dominated physiological changes that, in healthy women, are functional to the establishment of a pregnancy. More specifically, the ovaries undergo changes aiming at egg production, while the uterus evolves synergistically to a progressively more receptive status toward fertilized embryos. During the follicular phase, the preparatory phase for egg release, the progressive increase in uterine contraction frequency is thought to facilitate sperm ascension toward the distal end of the fallopian tubes, where fertilization takes place. 4,5 After ovulation, the uterus undergoes progressive relaxation that culminates during the mid-luteal phase. This relaxation phase, which usually occurs approximately 7 days after ovulation, may assist proper embryo positioning in the uterine cavity and, thus, facilitate embryo implantation. 7,41 During menses, if no egg has been fertilized to start a pregnancy, labor-like contractions promote shedding the uterine lining and a new cycle begins. 7,44,55,79 –81
Based on validated approaches previously developed for EHG analysis in pregnancy, in this study, a number of selected features is extracted from the recorded EHG signal at each of the representative phases of the menstrual cycle. Half of the 12 indicators here extracted from the recorded EHG show some significant differences among phases. Consistent, significant differences have been found between the EF phase and the LL phase. Especially with the UFM indicator, the EF phase shows consistent significant difference from all other phases. This phase, which coincides with menses, 57 also shows the highest variability. Both these aspects, namely, its significant difference from the other phases and the indicator variability, can be related to intermittent and cramping-like contractions typical of menses. Previous studies on nonpregnant uteri have in fact reported a wavelike, peristaltic activity of the uterus during most of the menstrual cycle as opposed to menses and parturition, when cramping-like contractions are alternated to quiescent periods of inactivity. 7,44,55,79-8181 Qualitative comparison of the recordings of this study with signals recorded during pregnancy with a similar protocol also indicates a more continuous, peristaltic activity, rather than alternation of contracting and quiescent periods of electrical activity (burst), which are typical of pregnancy and observed more frequently during menses. Noteworthy, as an initial step toward the use of EHG outside pregnancy, our approach is based on previous EHG studies in pregnancy.
Due to the size increase and hormonal changes that the uterus undergoes in pregnancy, some additional challenges should be accounted for when using EHG measurements outside pregnancy. Yet, similarly to pregnancy, pressure increases have also been measured during contractions outside pregnancy, 26,55 and spontaneous electrical activity has been observed and recorded. 55,82
Furthermore, the significance of the features extracted during menses supports the employment of the proposed methods for the investigation of dysfunctions related to menses, such as dysmenorrhea. Future studies, aiming at developing tailored methods for the analysis of the EHG outside pregnancy, may also reveal significance differences between the LF and the luteal phases as well as between different moments within the luteal phase.
All features show decreasing trend in their value along the cycle. This decrease is mostly not significant but may reflect a progressively more quiet state along the cycle that is in line with the uterine function of promoting embryo implantation by increased receptivity. In contrast, previous US and intrauterine pregnancy measurements during the menstrual cycle evidenced a progressive increase in contraction frequency and strength in the follicular phase followed by a decrease in the luteal phase, 34,40,55 suggesting a role of estrogens as stimulator and progesterone as inhibitor of uterine contractions. 8,83,84 In general, a direct comparison between the EHG features evaluated in this work and the uterine contraction properties evidenced by intrauterine pressure catheters and US should be cautiously evaluated; the fundamental different nature of the measurement approaches used in this study and in the previous literature (electrical vs mechanical) and the specific signal analysis employed in this study should first be jointly evaluated in relation to the underlying physiological mechanisms, which are still largely unknown.
We record the EHG signal transabdominally, using an electrode patch containing 64 channels. Our choice for testing the feasibility of transabdominal recording of the EHG, rather than more invasive methods to evaluate uterine electrical activity, is motivated by the urgent need for a cost-effective, noninvasive, and easy-to-use method for deriving uterine activity in everyday clinical practice. This abdominal approach does not take into consideration the possible role of other organs, such as the bladder or the intestine, that also produce biopotential. Based on our results, we may conclude that the main organ activity extracted by our measurements is from the uterus. Additional evidence that our signals are representative of uterine biopotential alone is being researched. As for the electrodes chosen in this study, in pregnancy, it has been demonstrated that the EHG can potentially quantify amplitude, frequency, and, when arrays of electrode are used, direction and velocity of contractions. The use of a multichannel grid for the signal acquisition is here meant to demonstrate the feasibility of multichannel EHG recording and possibly open the way to future studies aiming at assessing contraction direction and velocity. Eventually, the optimal interelectrode distance should be carefully evaluated in relation to the increased depth at which the uterus lies into the pelvic cavity as compared to pregnancy.
Conclusion
In conclusion, this study confirms that transabdominal EHG measurements are a feasible option to investigate noninvasively and objectively the activity of the nonpregnant uterus. The standard analysis methods used in this study are, in fact, already capable to single-out menses contractions from the other representative cycle phases.
These promising results motivate future work aiming at optimizing the use of this technology. Dedicated approaches should be researched to enable full characterization of uterine contractions outside pregnancy and detect the different patterns of physiological and pathological uterine activity. Supported by dedicated ex-vivo and invasive electrophysiological studies, our future efforts will focus on consolidating this feasibility study, which paves the way to a full exploitation of the potential of electrohysterography to quantify the activity of the nonpregnant uterus and improve management of dysfunctions (possibly) related to altered uterine contractility, such as subfertility, endometriosis, and dysmenorrhea.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an unconditional Veni grant from the