
Abstract
Previously, embryonic growth has been assumed to be uniform, but in recent years, it has become more clear that genetic and environmental factors may influence the intrauterine environment and therefore embryonic growth trajectories as well as pregnancy course and outcome. The objective of this study was to investigate associations between modifiable maternal nutrition and lifestyle factors during the periconception period and embryonic growth. We established a prospective cohort including 342 women less than 13 weeks pregnant. At enrollment, women filled out a questionnaire regarding demographic and medical data and a validated food frequency questionnaire. Participants received multiple 3-dimensional ultrasound examinations up until the 12th week of pregnancy, and crown–rump length (CRL) and embryonic volume (EV) were measured offline using V-Scope Virtual Reality software (version 1.0.0) in a Barco I-Space. Associations between maternal periconception vegetable and fruit intake, folic acid supplement use, smoking, and alcohol consumption and embryonic growth measurements were assessed by linear mixed models adjusted for potential confounders. No or postconception initiation of folic acid supplement use was significantly associated with a 0.76 mm (−7.8%) and 1.63 mm (−3.7%) smaller CRL and a 0.01 cm3 (−19.5%) and 0.86 cm3 (−12.2%) smaller EV at 7+0 and 11+0 weeks of gestation, respectively. Smoking, alcohol consumption, and inadequate fruit and vegetable intake showed weaker associations with embryonic growth parameters. These results emphasize the influence of periconceptional maternal folic acid supplement use on embryonic growth. Results regarding maternal nutrition and lifestyle factors also suggest an association with embryonic growth, but this has to be confirmed in a larger study.
Introduction
Early embryonic growth has traditionally been assumed to be uniform among humans, but in the past decade, subtle differences in embryonic growth trajectories have been shown. 1 –3 These differences not only concern embryonic development but are also suggested to predict a poor pregnancy course and outcome. 4 Embryonic development and growth is under the constant influence of the intrauterine environment, which is determined not only by genetic factors but also by parental environmental and lifestyle factors, of which most are modifiable. 5,6 In high-income countries, unhealthy lifestyle (including unhealthy nutrition) is an increasing problem. 7 A shift toward behavioral changes, resulting in high caloric intake, vitamin deficiencies, smoking, alcohol consumption, and physical inactivity, is causing an increasing prevalence of obesity and other noncommunicable diseases. 8,9
Unfortunately, the high frequency of unhealthy lifestyle is also present among women of reproductive age, even in those undergoing fertility treatment, despite the known negative effects on fetal growth and pregnancy outcome and the health of mother and child later in life. 10 For example, maternal smoking, alcohol consumption, and nutritional deficiencies are associated with fetal growth restriction and increased risks of miscarriage and fetal death. 11 –14 In the long term, unhealthy maternal lifestyle increases the risk of cardiovascular and metabolic disease in offspring. 15 –18
We hypothesize that increased fruit and vegetable intake and folic acid supplement use during the vulnerable periconception period (ie, the 14 weeks before and 10 weeks after conception) are positively associated with embryonic growth, whereas smoking and alcohol consumption are negatively associated. These 5 nutrition and lifestyle factors are not only known to affect fertility, they are also easy to address for a clinician and easy to (self-)report for a patient. Therefore, the aim of this study was to investigate associations between these 5 modifiable maternal periconception lifestyle risk factors and first trimester embryonic growth, making use of the novel state-of-the-art techniques of 3-dimensional ultrasound (3D-US) combined with the virtual reality technology of the Barco I-Space. 19 –21
Participants and Methods
Study Population
This study was part of the Rotterdam Periconception Cohort (PREDICT study), an ongoing prospective tertiary hospital-based study embedded in the outpatient clinic of the Department of Obstetrics and Gynecology of the Erasmus MC, University Medical Centre Rotterdam, Rotterdam, the Netherlands. A detailed cohort description has previously been published. 22 From November 2010 to December 2014, women of at least 18 years of age who were less than 13 weeks pregnant with a singleton pregnancy were eligible for participation.
Data Collection
All pregnancies that were conceived spontaneously or through intrauterine insemination, semen donation, and hormone therapy were considered to be spontaneous in comparison with pregnancies conceived through in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI). Pregnancies were dated as described previously. 22 In short, gestational age (GA) was either based on the last menstrual period in spontaneous pregnancies or on the conception date in IVF and ICSI pregnancies. To obtain information on demographic characteristics and 5 periconception lifestyle factors (ie, vegetable intake, fruit intake, folic acid supplement use, smoking, and alcohol consumption), participants completed a self-administered questionnaire at enrollment, together with a validated semi-quantitative food frequency questionnaire, which was verified for completeness and consistency by the researcher or research nurse at study entry. 22,23
Adequate daily fruit and vegetable intake was defined according to Dutch guidelines as 2 pieces of fruit (equivalent to 200 g) and 200 g of vegetables, respectively. Folic acid supplement use of 400 µg/d is recommended during the periconception period (ie, from 4 weeks prior to conception up to 8 weeks after conception). 24,25 Therefore, preconception initiation of folic acid supplement use was defined as adequate, whereas no or postconception initiation of folic acid supplement use was defined as inadequate. Total abstinence of smoking and alcohol consumption during the periconception period was considered adequate. Anthropometrics (ie, maternal blood pressure, weight, and height) were measured at study entry by a research nurse.
From November 2010 to December 2012, participants received weekly transvaginal 3D-US scans from enrollment up to week 12 of gestation (range: 6+0 to 12+6 weeks) by experienced sonographers. From the end of 2012 onwards, the number of scans was reduced to 3, performed in the 7th, 9th, and 11th week of gestation, as the pilot study showed that 3 scans are sufficient to accurately model embryonic growth curves. 2,26 Obtained 3D-US data sets were transferred to the Barco I-Space (a Cave Automatic Virtual Environment–like virtual reality system) to create an interactive virtual reality hologram. Trained researchers performed offline measurements using the I-Space and V-Scope software (version 1.0.0). Crown–rump length (CRL) was measured 3 times, and the mean of these measurements was used for analysis. Embryonic volume (EV) measurements were performed once using a semi-automatic method based on gray levels. 27
Statistical Analysis
General characteristics of the study sample and source population were compared using Mann-Whitney U tests (for continuous variables) or χ2 tests (for categorical variables). To take into account the correlation between measurements of the same pregnancy, linear mixed models were used to assess associations between adequate periconception maternal lifestyle and embryonic growth. A square root transformation of CRL and third root transformation of EV data led to linearity with GA and a constant variance independent of GA and were therefore used in the analysis.
In the first model, we adjusted for GA only to increase the precision of the measurements. In the second model, we additionally adjusted for maternal age, body mass index (BMI), ethnicity, educational level, parity, and mode of conception. In the final model, we also adjusted for folic acid supplement use, fruit intake, vegetable intake, alcohol consumption, and smoking (all dichotomous; adequate or inadequate) to investigate the independent effects of the lifestyle factors. In all models, embryonic growth rates for both CRL and EV were calculated by including an interaction term between the GA and the 5 risk factors of interest.
P values below .05 were considered statistically significant. All analyses were performed using IBM SPSS Statistics version 21.0 for Windows.
Ethical Approval
All data were anonymously processed. This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving patients were approved by the medical ethical and institutional review board of the Erasmus MC, University Medical Centre, Rotterdam, the Netherlands. Written informed consent was obtained from all participants at enrollment.
Results
From a total of 723 first trimester pregnancies enrolled in the PREDICT study between 2010 and 2014, CRL and EV measurements were available for 563 pregnancies. Of these pregnancies, 221 were excluded because of the following reasons: miscarriage, ectopic pregnancies, congenital anomalies, perinatal death, twin pregnancies, oocyte donation, pregnancy termination, irregular menstrual cycle, observed CRL discrepancy >6 days from expected CRL, missing questionnaires, and withdrawal (Figure 1). Thus, a total of 342 pregnancies were included in the analyses.
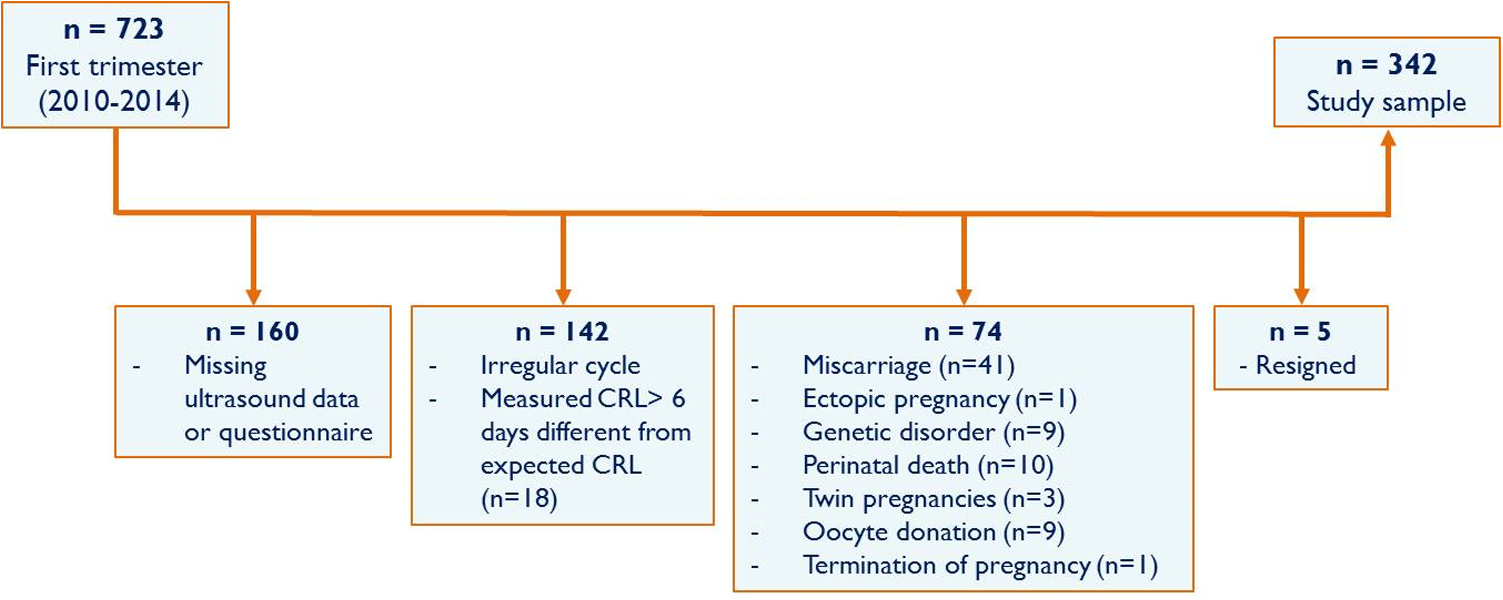
Flowchart of the study population. CRL indicates crown–rump length.
In these pregnancies, the median number of 3D-US examinations per pregnancy was 4 (range: 1-7), with a median GA at the first 3D-US examination of 7+3 weeks (range: 6+0-12+2). This yielded a total of 1443 ultrasounds, of which 1255 (87.0%) were of sufficient quality to perform CRL measurements and 1116 (77.3%) to perform EV measurements.
Women in our study sample more often conceived through IVF or ICSI compared with the source population of the PREDICT study (40.9% vs 26.5%, P < .001; Table 1). In the study sample, nearly all women used a folic acid supplement (n = 329, 98.2%) and 278 (83.0%) women started folic acid supplement use preconceptional. A total of 48 (14.2%) women smoked and 112 (33.2%) consumed alcohol during the periconception period. Fruits and vegetable intake was inadequate in 162 (52.9%) and 110 (35.9%) women, respectively.
Baseline characteristics of the source population and study sample.
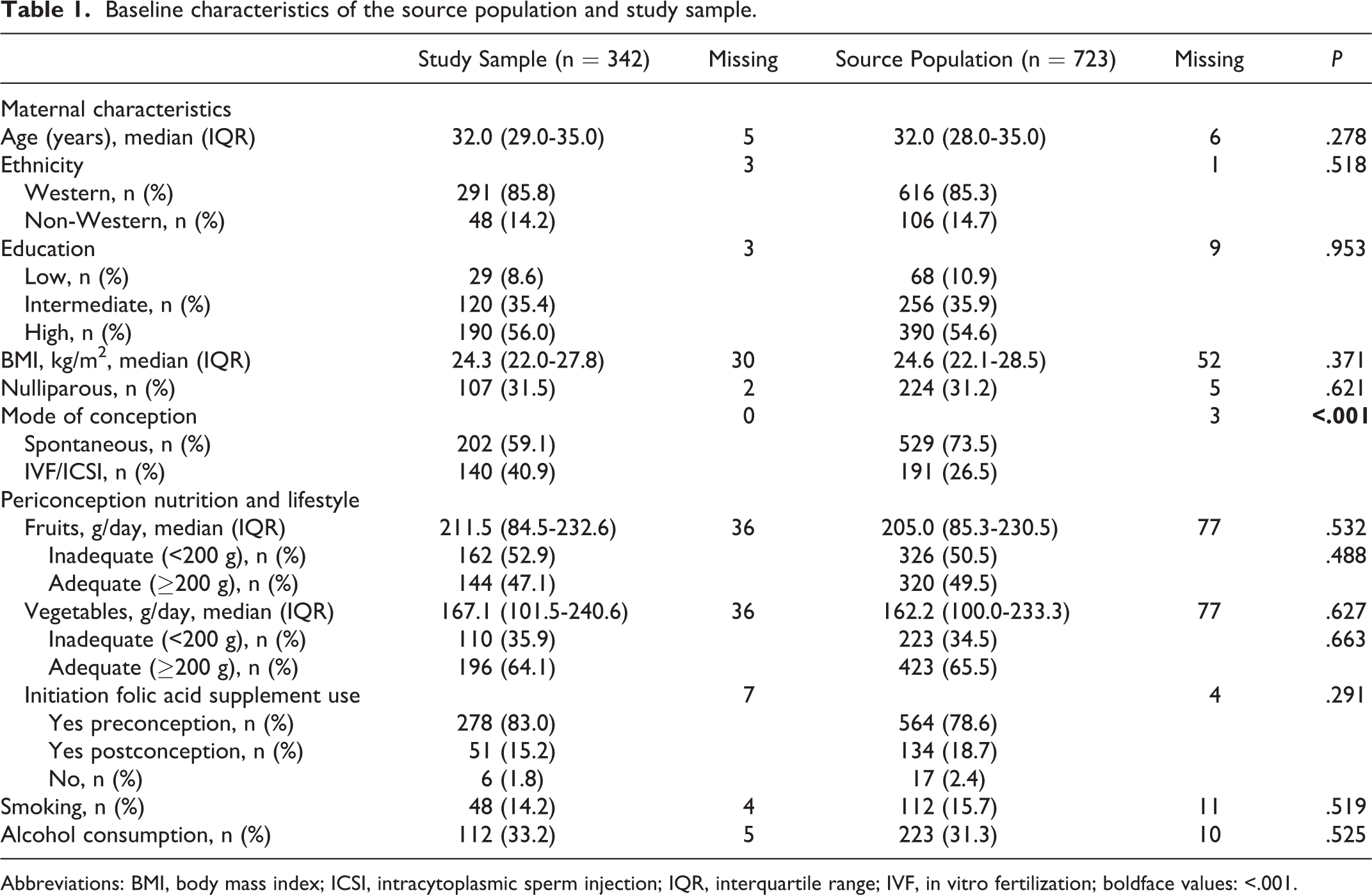
Abbreviations: BMI, body mass index; ICSI, intracytoplasmic sperm injection; IQR, interquartile range; IVF, in vitro fertilization; boldface values: <.001.
Inadequate folic acid supplement use was significantly negatively associated with CRL (−0.124, 95% confidence interval [CI]: −0.222 to −0.026) as well as EV (−0.059, 95% CI: −0.105 to −0.014; Table 2). Retransformation to the original scale showed that the CRL of an embryo of a woman with inadequate folic acid supplement use was on average 0.75 mm (reduction of 7.8%) and 1.63 mm (reduction of 3.7%) smaller at 7+0 and 11+0 weeks of gestation, respectively, compared to a woman with adequate folic acid supplement use (Figure 2A). In women with inadequate folic acid supplement use, the EV was on average 0.01 cm3 (reduction of 19.5%) and 0.86 cm3 (reduction of 12.2%) smaller at 7+0 and 11+0 weeks of gestation, respectively (Figure 2B). The interaction between GA and folic acid supplement use was statistically significant (P = .03) for EV, indicating that embryonic growth rates differed between both groups (ie, higher in women who adequately used folic acid supplements; Figure 2B). Smoking as well as inadequate fruit intake showed comparable negative associations with CRL and EV, though not statistically significant (Table 2).
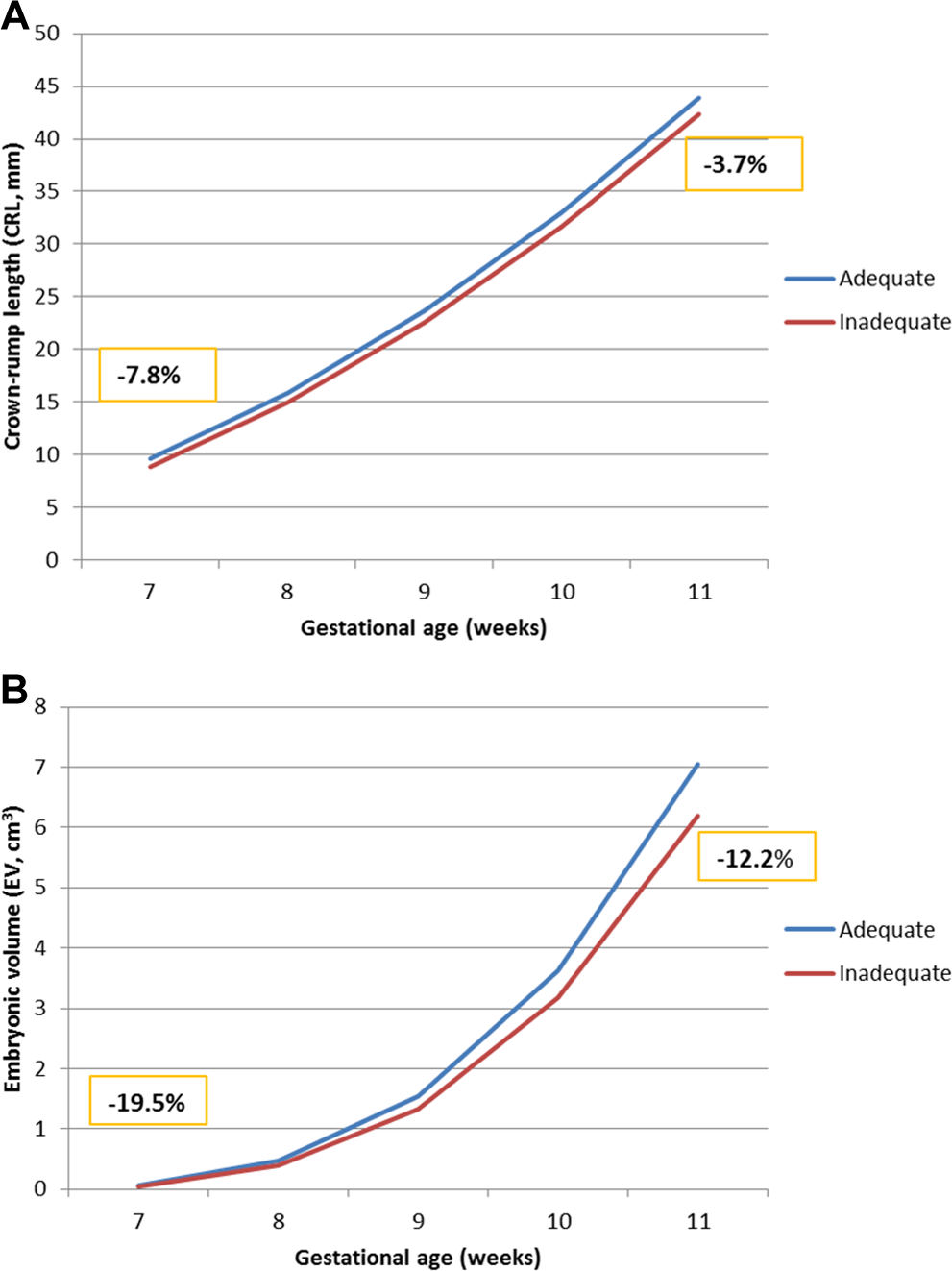
Embryonic growth trajectories for (A) crown–rump length (CRL) and (B) embryonic volume (EV). Adequate folic acid supplement use (preconception initiation, blue line) and inadequate folic acid supplement use (postconception initiation or no, red line), including the relative differences at 7 and 11 weeks of gestational age.
Associations between maternal periconception lifestyle and embryonic growth.
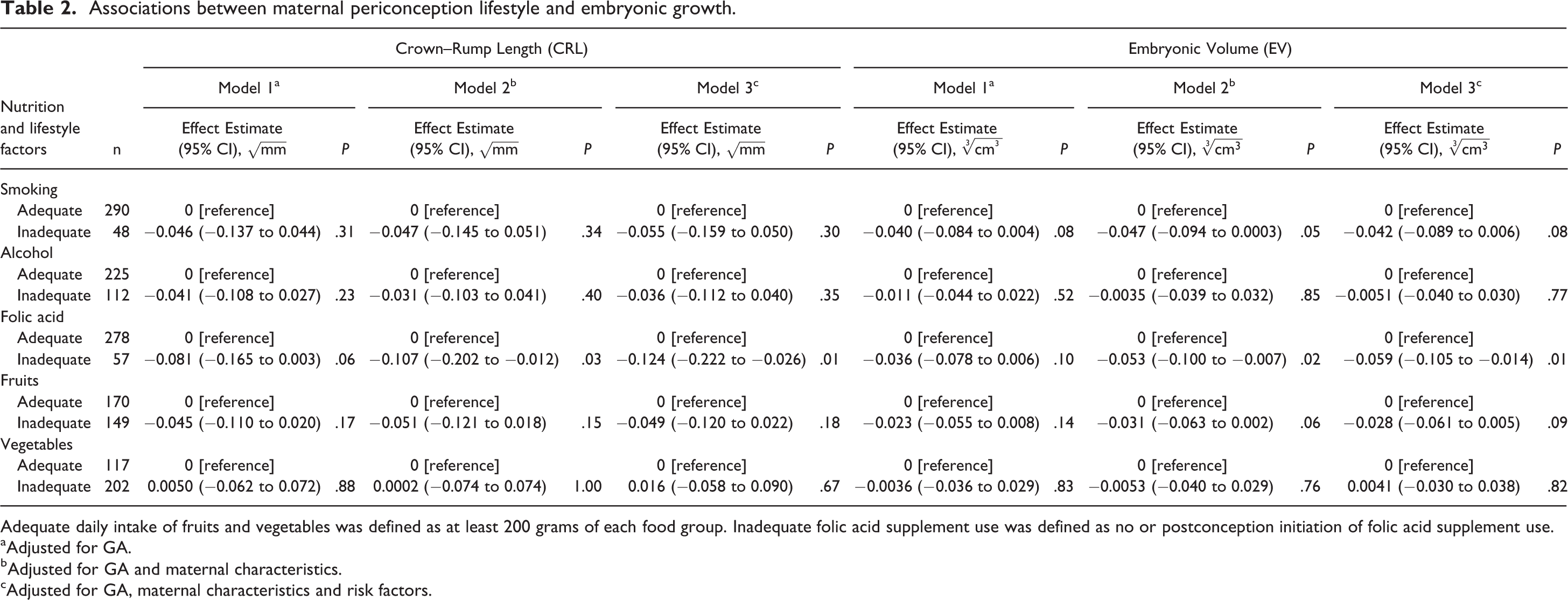
Adequate daily intake of fruits and vegetables was defined as at least 200 grams of each food group. Inadequate folic acid supplement use was defined as no or postconception initiation of folic acid supplement use. aAdjusted for GA. bAdjusted for GA and maternal characteristics. cAdjusted for GA, maternal characteristics and risk factors.
Discussion
In this study, we found a significant negative association between inadequate maternal folic acid supplement use and embryonic growth, measured as CRL and EV as well as growth rate during the first trimester. Maternal smoking and inadequate fruit intake showed comparable results, with nearly significant negative associations, but alcohol consumption and vegetable intake revealed no significant associations with embryonic growth in our study.
Folate is an important substrate used by the 1-carbon metabolism, in which 1-carbon groups are provided to critical processes, such as synthesis of DNA and proteins and epigenetic programming. This B vitamin is particularly known for its role in the prevention of neural tube defects. 17,28 As early pregnancy is a critical period with rapid cell division, growth, and proliferation as well as high responsiveness to external influences, optimal maternal folate concentrations are crucial. Optimal concentrations are frequently not achieved through regular dietary folate intake and deficiencies can lead to impaired epigenetic programming associated with long-term health consequences. 29 This may explain the reduced embryonic size and growth in women with inadequate folic acid supplement use in our study. However, our previous studies also showed that very high levels of maternal folate are associated with reduced embryonic and cerebellar growth, suggesting there is an optimum maternal folate status for embryonic growth. 30,31 Nutritional factors such as fruit and vegetable intake may also contribute to stable and reversible methylation abnormalities and impaired embryonic development, by means of insufficient supply or reduced uptake of cofactors of the 1-carbon metabolism. However, it is clear that this is only one of several metabolic pathways that are affected by maternal nutrition and as such influencing embryonic growth.
Longitudinal studies that focus on first trimester embryonic growth are scarce, but negative associations between maternal smoking and alcohol consumption and embryonic growth have been demonstrated. 4,26 This can be partly explained by their known deranging effects on the 1-carbon metabolism but also by the direct toxic effects of smoking on embryogenesis, placental development, and function and by the vasoconstrictive effects of alcohol consumption. 32 –34
One of the main strengths of this study is the longitudinally collected ultrasound data (with a median of 4 3D-US scans per pregnancy) combined with detailed and validated information regarding lifestyle. Also, offline virtual reality measurements of these 3D-US images show high reliability by their excellent inter- and intraobserver agreement. 20,27 Another strength of this study is the exclusion of pregnancies with an unreliable GA, whereas pregnancy dating is often a strong confounder in studies on embryonic growth, due to the variation in timing of ovulation and implantation in spontaneously conceived pregnancies. A limitation of this exclusion on the other hand is the smaller study sample and a relatively high percentage of pregnancies conceived through IVF/ICSI, although we did not observe any differences in association between nutrition and lifestyle and embryonic growth between both groups (data not shown).
In this study, we have included both high- and low-quality 3D-US images. Explanations for low-quality 3D-US images could be uterine position, movement of the embryo, and maternal BMI. Although 3D-US and virtual reality provide a more authentic and detailed view of the developing embryo, performing measurements on low-quality data can be difficult. In the future, results of separate analyses of high- and low-quality images could be compared to determine whether the quality actually influences the results.
Since diet is very complex and consists of a variety of foods and nutrients, focusing on a single food group, such as fruits or vegetables, may be less suitable to demonstrate associations between maternal nutrition and embryonic growth. Thus, it might be worth considering to study associations between dietary patterns and embryonic growth. However, it will be very time-consuming in routine clinical practice to determine a patient’s dietary pattern, while simple food groups, and consequently nutrient deficiencies, are much easier to query and to report. Our results emphasize the need to inform women who are contemplating pregnancy of the importance of preconception initiation of folic acid supplement use. Taking into account the high prevalence of inadequate nutrition and lifestyle in the reproductive population and the previously described associations between maternal lifestyle and fetal growth and pregnancy outcomes, preconception care should also focus on these inadequacies.
In conclusion, inadequate folic acid supplement use is negatively associated with embryonic growth and embryonic growth rate. We also show that there might be associations between periconception maternal smoking, alcohol consumption, inadequate fruit and vegetable intake, and impaired embryonic growth. Further research with larger study samples of different (general) populations should elucidate the association between periconception maternal lifestyle and embryonic growth, as the next step toward the early identification of pregnant women at risk of poor pregnancy course and outcome.
Footnotes
Authors’ Note
All authors revised the manuscript and gave approval to the final version. M.R.v.D. acquired, analyzed, and interpreted the data and drafted the final version of the manuscript. N.V.B. analyzed and interpreted data and cowrote the article. S.P.W. analyzed and interpreted the data. A.H.J.K. was responsible for (technical) support using the Barco iSpace. R.P.M.S.T. initiated and developed the Rotterdam Predict study and was responsible for all aspects of the study. M.P.H.K. contributed to data analysis and inference and critically reviewed all versions of the manuscript.
Acknowledgments
The authors would like to thank Dr Jeanne de Vries of the Wageningen University for her contribution in analyzing the data obtained from the food frequency questionnaires.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Department of Obstetrics and Gynecology, Erasmus MC, University Medical Centre, Rotterdam, the Netherlands, and a grant of the Erasmus MC Mrace program “Health Care Efficiency Research.”