
Abstract
Accumulating evidence indicates that adolescent endometriosis is common and often severe. Here we explore the possibility that seeding of naive endometrial progenitor cells into the pelvic cavity early in life, that is, at the time of neonatal uterine bleeding or soon after the menarche, results in more florid and progressive disease, characterized by highly angiogenic implants, recurrent ectopic bleeding, and endometrioma formation. We discuss the potential intergenerational risk factors associated with early-onset endometriosis and explore the molecular drivers of disease progression. Taken together, the available data suggest that an increased focus on early-life events may help to identify young women at risk of severe, progressive endometriosis.
Introduction
Effective management of endometriosis should be informed by the likelihood of disease progression, especially in younger women who have yet to achieve pregnancy. But what are the conditions or risk factors associated with endometriosis progression? A recent study analyzed the laparoscopic findings in 500 adult women in an attempt to shed light on this issue. 1 Unexpectedly, no correlation between the stage of endometriosis and the age of the patient was observed. The authors concluded that the revised American society for reproductive medicine (rASRM) classification stage I or II endometriosis is “equally likely to be present in women of all ages.” They also concluded that stage III and IV disease is “not age dependent.” Unfortunately, the study did not include a significant number of adolescents with endometriosis. Nevertheless, the findings illustrate that there is no obvious way to stratify patients with endometriosis on the basis of whether the disease is likely to progress, remain static, or regress.
This unsatisfactory state of affairs is not surprising as there is no agreed definition of “progression” or even an understanding of the natural history of endometriosis. In fact, the conclusion reached by Savaris et al 1 rests on the critical assumption that the rASRM staging system can be employed to measure disease progression. This conjecture is highly contentious. In a 3-year long prospective study of 643 consecutive laparoscopies, Koninckx et al 2 evaluated the area, depth, and volume of endometriotic lesions. The authors observed that the incidence, area, and volume of subtle lesions decreased with age. For typical lesions, however, these parameters increased with age. More recently, the same group proposed a simple classification system, which scores separately the severity of superficial, cystic, deep, and other lesions. 3 If implemented, such a scoring system would yield quantitative data that could be used to predict the risk of progression for each type of lesion, thus potentially resolving many of the uncertainties that currently hamper more effective management of endometriosis.
Notwithstanding the dearth of evidence, it is not unreasonable to consider that the time of onset of endometriosis in the life cycle could be an important determinant of the risk of disease progression. 4 In this position paper, we explore the possibility that early-onset or adolescent endometriosis is distinct from, and more progressive than, adult endometriosis. We wish to stress that our hypothesis is largely based on biological plausibility, rather than conclusive clinical evidence. Our aim is to pique interest into neglected early-life events that may shape the course of endometriosis during the reproductive years.
Origins of Early-Onset Endometriosis
Over the last few years, we have reinterpreted and summarized the largely historical literature on neonatal uterine bleeding (NUB) and concluded that endometrial breakdown and bleeding soon after birth likely represent an important risk factor for early-onset endometriosis. 5 –10 This hypothesis is based on a series of intriguing observations. Like menstruation, NUB is triggered by the rapid fall in circulating progesterone levels in the first few days after birth. However, unlike menstruation, NUB affects only 5% of newborn girls. 11 –14 The reason for this discrepancy lies in the ontogeny of steroid hormone responses in the fetal endometrium. Rosa 15 studied fetal sexual development in a series of 31 female fetuses, aged between 4½ months gestation to term. Although formation of the fetal endometrium is completed by 4½ months, both the stromal and glandular compartments were found to be inactive. Evidence of an estrogenic response was observed between 5 to 7½ months of gestation. By the second half of the eighth month, progesterone-dependent changes in the glandular compartment became apparent, exemplified by coiled glands, apocrine secretions, and glycogen enclaves. In fact, these observations led to the concept that the fetal endometrium, over a period of 4 months (from the fifth month till term), mimics the changes observed in a normal 28-day “menstrual” cycle. There are, however, significant differences between the sequential estrogen and progesterone actions in the fetal endometrium and those of the menstrual cycle, including the poorly developed glands in fetal endometrium and the absence of the decidual changes in stroma. On the other hand, the pioneering yet largely ignored postmortem study of Ober and Bernstein 16 documented a broader spectrum of progesterone responses in uteri from neonates who had died soon after birth. This study demonstrated that decidual transformation and endometrial shedding do occur in the neonatal uterus, but the incidence is low, approximately 5%. However, occult bleeding, detectable using different laboratory techniques, is more common and affects approximately 25% of babies. 12,13
Neonatal uterine bleeding is today viewed as a clinically irrelevant event. This was not always the case. Several large clinical studies carried out in the 1960s and 1970s identified potential risk factors for NUB. 11 –14 As these studies preceded ultrasound dating of pregnancy, the findings should be interpreted with caution. Nevertheless, the collective evidence indicates that postmaturity is a major risk factor for NUB. 14 More surprisingly, NUB was also found to be strongly associated with preeclampsia and low birth weight. There was also a suggestion of an association between NUB and Rhesus or ABO incompatibility, although this is contentious. 10,11 Nevertheless, a recent epidemiological study found that Rh-negative women are twice as likely to develop endometriosis. 17 Chromosome 1p, which contains the genes coding for the Rh factor, also harbors an endometriosis susceptibility region near the WNT4 gene. 18 In this respect, a recent metanalysis by Rahmioglu et al 18 evaluated 8 genome-wide association studies (GWAS) in an attempt to identify common genetic variants in endometriosis. The investigators concluded that there is a remarkable consistency in endometriosis GWAS results across studies, with little evidence of population-based heterogeneity. They also stressed the importance for future studies to include detailed sub-phenotype information. We believe that this recommendation is particularly appropriate for GWAS studies. Functional studies in relevant tissues are needed to understand the effect of the variants on downstream biological pathways.
At present, Sampson theory developed in the 1920s remains the most widely accepted theory on the origins of endometriosis. 19 His hypothesis is based on the tacit assumption that menstrual effluent contains viable cells from the superficial endometrium. It is now well established that menstrual blood indeed comprises a mix of endometrial mesenchymal stem cells (eMSCs) and stromal fibroblasts, although epithelial and epithelial progenitor cells may have been overlooked. 20,21 These cells presumably first attach and then breach the peritoneum, a notion increasingly supported by experimental data. 22,23 Interestingly, Arcellana et al 24 provided evidence of the initial stages of endometriosis formation in a female infant with menstruation-like bleeding. The baby had McKusick-Kaufman syndrome and died approximately 8 hours after birth. Postmortem examination revealed an intact transverse vaginal septum with hydrocolpos containing 200 mL of cloudy fluid. Examination of the peritoneal cavity revealed hemorrhagic endometrial reflux and implantation of epithelial fragments on the bowel serosa as well as adhesions around the ovaries and upper uterus. These findings are consistent with the implantation model of endometriosis. It seems not unreasonable to assume that eMSCs and epithelial progenitor cells have the ability to quickly implant in the pelvis during the early neonatal period. The relatively long cervix and thick cervical secretions in the neonate may even facilitate retrograde seeding of endometrial progenitor cells. 6,7 Inherent to endometrial stem/progenitor cells is their ability to remain dormant for many years. 25 Hence, it is not inconceivable that endometrial progenitor cells seeded in the pelvis soon after birth remain quiescent until rising estrogen production that precedes the menarche stimulates angiogenesis and promotes the formation of hemorrhagic endometriotic lesions. 7,26 By extension, it can be argued that the earlier the menarche takes place in the life cycle, the higher the risk may be of inimical endometriotic disease because of seeding of less committed and more multipotent endometrial stem/progenitor cells. Whether or not NUB in turn is associated with early menarche, possibly reflecting increased steroid hormone responsiveness of the endometrium, is not known.
Intergenerational Risk Factors
There is increasing awareness that reproductive disorders prior to conception may increase the risk of obstetrical complications in pregnancy. 27 However, if and how pregnancy disorders impact on the reproductive function of the offspring remains unknown. Arguably, the reportedly strong association between maternal preeclampsia and NUB 10,11 warrants further investigation as it raises the possibility that in utero stress in pregnancy accelerates the process of hormonal responsiveness of the fetal endometrium and thus the risk of NUB. Furthermore, it is not inconceivable that maternal preeclampsia also facilitates subsequent ectopic implantation of endometrial tissue in the newborn. This conjecture is based on the emerging role of platelets in the pathogenesis of endometriotic lesions. 28 In a mouse model of endometriosis, aggregation of platelets at ectopic implants coincides with heightened vascular endothelial growth factor (VEGF) expression and increased microvessel formation. Furthermore, coculturing of endometriotic stromal cells with platelets increases proliferation and stimulates the expression of key factors, including estrogen receptor-β, VEGF, cyclooxygenase 2, and gelatinase (Matrix-Metallo-Peptidase-9). 28 It is well established that preeclampsia influences the expression of surface glycoproteins on not only maternal but also neonatal platelets. 29,30 Klein et al 31 demonstrated that platelets from newborn of preeclamptic mothers exhibit increased reactivity, even in response to weak activators such as adenosine diphosphate. Hence, it would be informative to examine the responses of endometriotic stromal cells to cord blood platelets isolated from preeclamptic versus control pregnancies. In addition, in view of a possible association between exposure to certain environmental toxic agents and endometriosis, 32 it is also conceivable that in utero or postnatal exposure to endocrine disruptors or xeno-estrogens, like bisphenol A and S, may be permissive for early-onset endometriosis.
Adolescent Endometriosis: Hemorrhagic Lesions and Endometrioma Formation
It has been suggested that endometriosis is a physiological process, unless recurrent bleeding in ectopic implants causes disease progression by inducing adhesions, fibrosis, and the formation of endometriotic cysts. 33 Adolescent endometriosis is typically characterized by red hemorrhagic peritoneal lesions and, in severe cases, by large ovarian endometriomas (Figure 1). Gogacz et al 34 described a case of ovarian endometrioma in a prepubertal girl showing typical features of endometrial tissue with hemosiderin-loaded macrophages lining the ovarian cortex. Tong et al 35 described a series of 94 young girls with Herlyn-Werner-Wünderlich syndrome (HWWS), defined by the presence of a uterus didelphus with an obstructed hemivagina and ipsilateral renal agenesis or dysplasia. Endometriosis was found at laparoscopy or laparotomy in 18/94 (19%) patients; and all had cystic ovarian endometriosis. The median time between menarche and onset of cyclic pelvic pain was 1 year (range 0-16 years), while the median time between menarche and the diagnosis of pelvic endometriosis was 3 years (range 1-16 years). The age of onset of endometriosis (18 ± 5.4 years) was much earlier than the age of diagnosis of HWWS. The presence of typical endometriomas in these girls supports the notion that adolescent endometriosis is indeed caused by retrograde shedding of eMSCs. Notably, MSCs isolated from ectopic lesions show greater invasiveness and migration ability as well as the capacity to stimulate neoangiogenesis compared to those in eutopic endometrium. 26 These cellular differences may relate to the distinct niche environment in ectopic sites 36 or, alternatively, reflect the early-life origins of ectopic eMSCs. 7
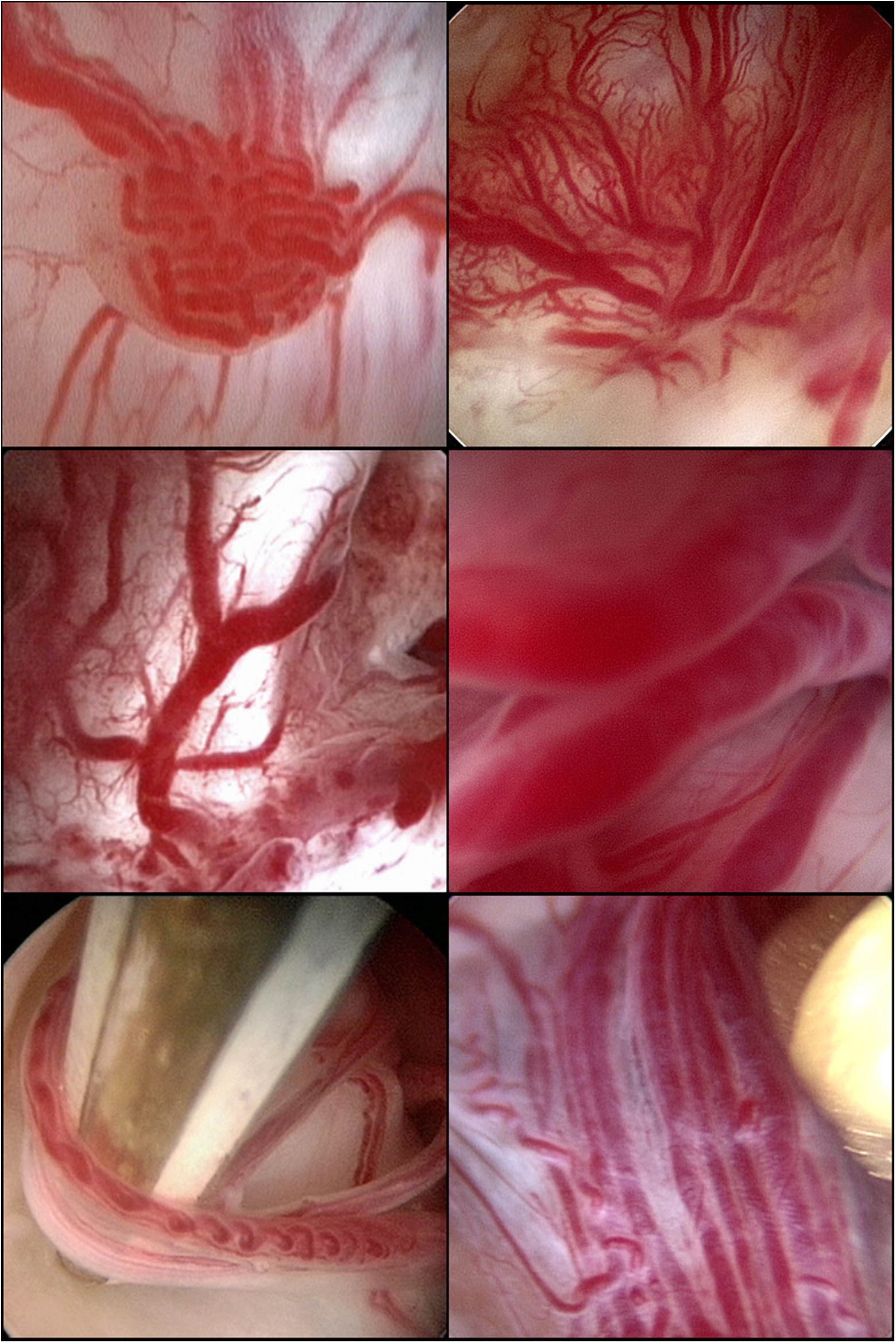
Vascularity of endometriotic lesions assessed by transvaginal hydrolaparoscopy. More than 65% of underwater close-ups of so called “atypical” or “subtle” peritoneal implants (top row), active endometriotic implants within the opened endometrioma (middle row), or connecting and nonconnecting endometriotic adhesions (bottom row) show a complex vascular tangle of newly formed capillaries, illustrating the extensive neovascularization that accompanies the development of endometriosis. This information is lost at conventional laparoscopy due to the increased intra-abdominal pressure induced by the pneumoperitoneum. Moreover, this hypervascularization offers a second target, beside the implants themselves, for electro- or laser coagulation, thus interrupting hormonal exposure and oxygen supply to the lesions.
Until recently, the presence of an endometrioma in adolescents was considered the exception. Wright and Laufer 37 reported on a 19-year-old woman with bilateral endometriomas and concluded: “Endometriomas are rare in adolescents. There are no case reports in the literature to date” and “most endometriosis in adolescence is of an early stage.” Yet, a literature review of recent studies shows that a substantial proportion of girls with early-onset endometriosis have a severe (rASRM stage III or IV) disease at laparoscopy and that the severity is largely caused by the presence of ovarian endometriomas (Table 1). 35,38 –42 A recent study of 86 adolescents and young women (aged ≤ 22 y) attending a tertiary referral center for surgery showed that 66 (77%) had stage I or II disease and 20 (23%) had stage III or IV, of whom 14 (70%) had endometriomas. 41 Rectovaginal endometriosis was found in 1 case and diaphragmatic and pulmonary disease in another case. The authors concluded that the main reason for advanced stage endometriosis in this age-group was the presence of ovarian endometriomas, rather than extensive adhesive disease. Finally, another study of 55 adolescents with endometriosis, aged between 12 and 19 years, reported stage III/IV disease in 24 (44%) girls, including 18 (33%) patients with endometriomas and 6 (11%) with deep infiltrating endometriosis. 42 Taken together, these studies show that adolescent endometriosis is neither rare nor mild. Instead, early-onset endometriosis is often characterized by florid hemorrhagic lesions and endometrioma formation, an observation that further supports the conjecture that the implants must have been established prior or soon after to the onset of the menarche.
Incidence of Ovarian Endometrioma and Deep or Rectovaginal Endometriosis in Adolescents or Young Women With Advanced Stage Pelvic Endometriosis.
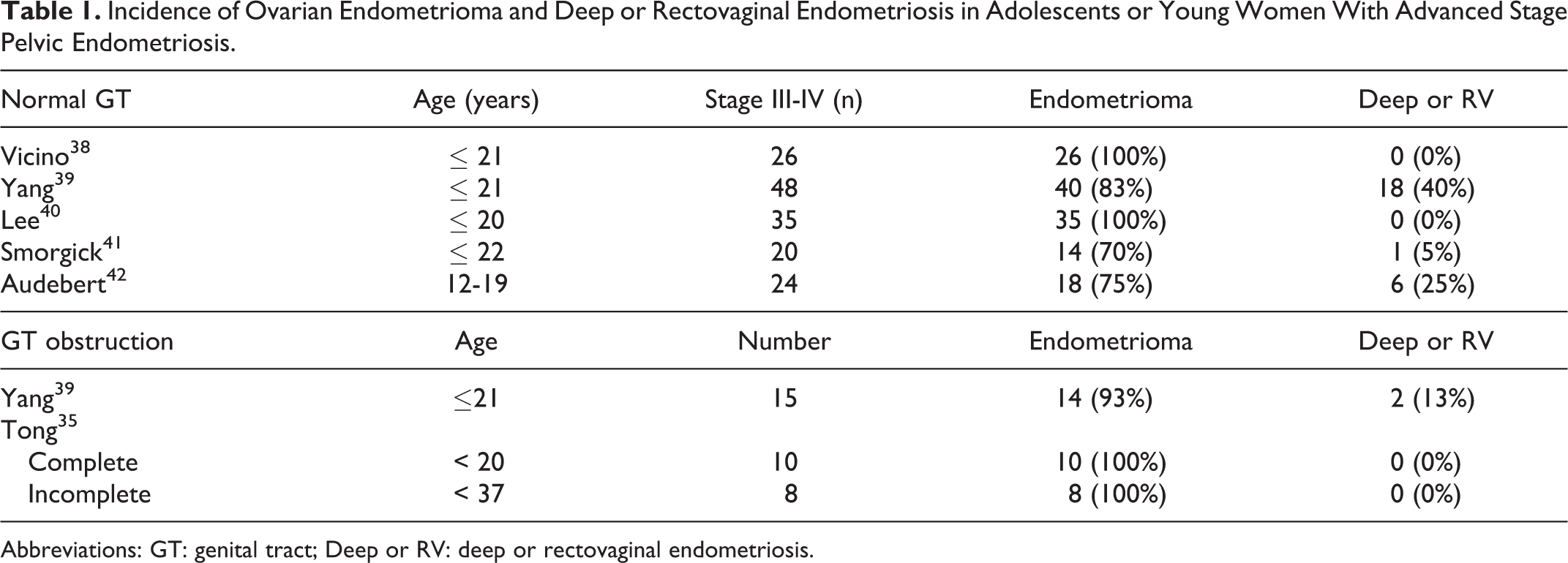
Abbreviations: GT: genital tract; Deep or RV: deep or rectovaginal endometriosis.
The Progressive Phenotype of Ovarian Endometriomas
In a seminal study of ovaries with endometriomas in situ obtained at the time of hysterectomy, Hughesdon 43 described degenerative changes in the cortex lining the cyst and the underlying interstitial tissue. In most cases, the ovarian cortex was no longer recognizable and seems to have been replaced by a darkly stained connective tissue. However, the occasional presence of follicles and continuity with unaltered cortex confirmed that the ovarian surface of the endometrioma was in fact cortex partly or completely transformed into fibromuscular tissue. According to Hughesdon, 43 the presence of an inner cortex implies that ectopic endometrium does not erode its way into the ovary, rather the cortex becomes invaginated. In agreement, ovarioscopy, that is, endoscopic inspection of an ovarian cyst, often reveals a marble-white or pigmented invaginated cortex lined by endometrial-like tissue in recently formed endometriomas, which is gradually replaced by dark pigmented fibrotic tissue in older patients (Figure 2). In support of these findings, transvaginal color Doppler sonography demonstrated decreased interstitial flow and significantly higher resistance indices in patients with ovarian endometriomas when compared to controls presenting with a benign ovarian tumor. 44
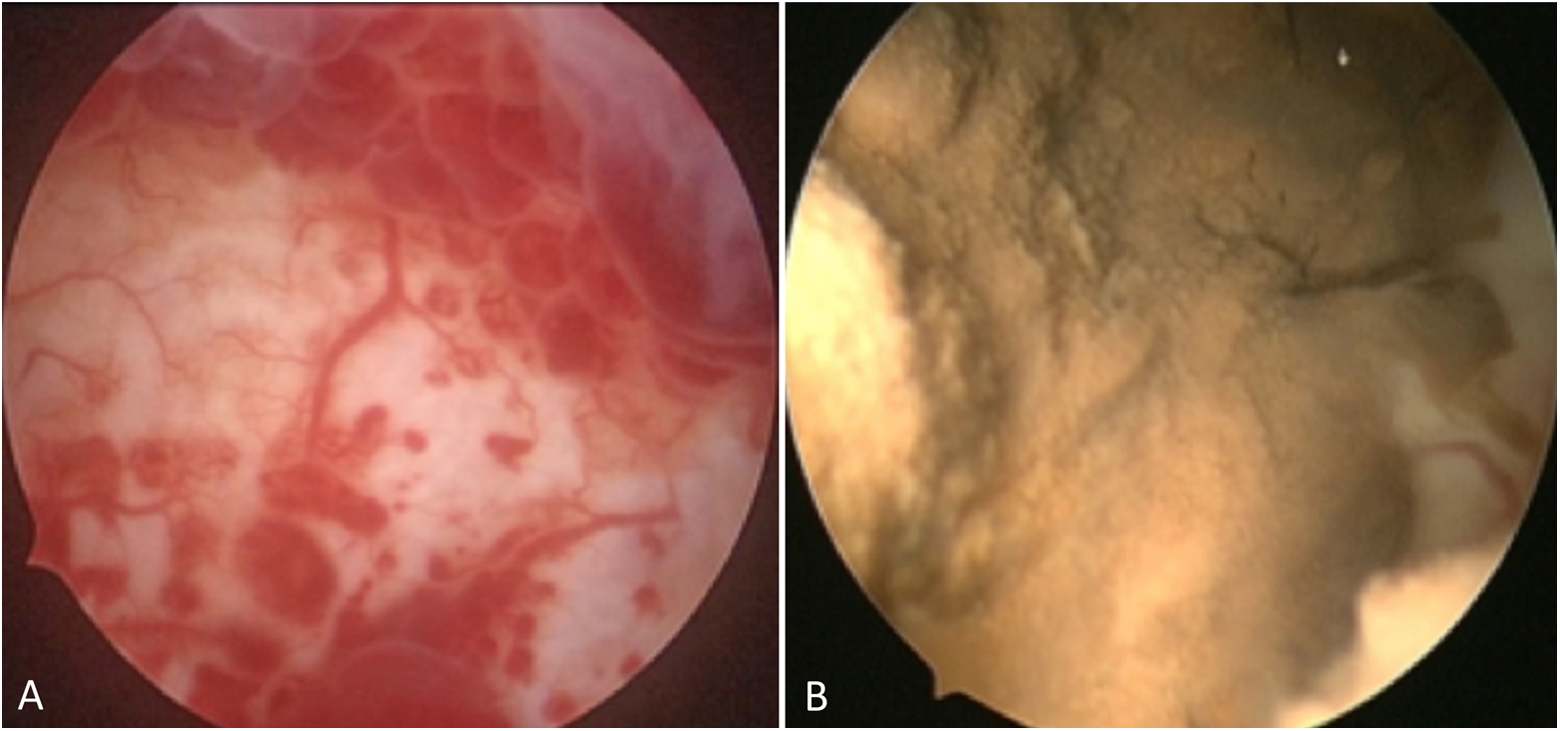
Assessment of ovarian endometriomas by ovarioscopy. A, In younger women, the wall of the endometriotic cyst has the same marble-white or yellowish appearance as the outer cortex and is lined by a thin highly vascularized mucosa. B, By contrast, the lining of older cysts typically appears darker, fibrotic, and devascularized.
Smooth muscle metaplasia (SMM), detectable by positive staining for alpha-smooth muscle actin, is a common feature of ovarian endometriomas. 45 As is the case in other tissues, SMM and tissue fibrosis are the consequence of repetitive tissue injury, bleeding, and repair. Platelets aggregate in ovarian cysts and promote epithelial-mesenchymal transition, characterized by acquisition of specialized smooth muscle cell markers, such as desmin, oxytocin receptor, and smooth muscle myosin heavy chain. 28 Guo et al 46 found that fluid from endometriomas from older patients also contains significantly higher concentration of total bilirubin, ferritin, and free iron when compared to younger women. In addition, older lesions have significantly more collagen content, higher adhesion scores, and contain more viscous fluid. Taken together, these data support the notion that the changing nature of endometriomas with age reflects the impact of repeated injuries and repair, resulting in largely fibrotic, nonprogressive lesions that are resistant to hormonal treatment. 46 Similar observations can also be seen in adenomyosis, a closely related disorder. 47
A recent review charted the potential cellular and molecular mechanisms by which endometriomas could damage the ovary. 48 Endometriomas contain free iron, reactive oxygen species, proteolytic enzymes, and inflammatory molecules in concentrations that are 10 to 100 times higher than those in peripheral blood. The noxious cyst content triggers a chronic stress response in endometrial cells lining the endometrioma, thereby altering gene expression and potentially damaging DNA. The physical barrier between the cyst contents and the interstitial ovarian tissue is a thin wall composed of the overstretched ovarian cortex or fibro-reactive tissue. Reactive oxygen species can permeate to the surrounding tissues and activation of proteolytic enzymes promotes remodeling of the normal ovarian cortex and contributes to the generation of fibrous tissue. The lower follicular density observed in the endometrioma bed may be primarily the result of vascular sclerosis. Finally, iron and ferritin concentrations are also significantly higher in the peritoneal fluid of patients with endometriosis. 49 In a mouse model, iron overload did not affect the establishment of ectopic lesions but promoted cell proliferation and thus contributed to the further growth of endometriotic lesions. 50
Perspectives
While both NUB and cyclic menstruation share the core concept that endometrial tissue breakdown following progesterone-dependent decidualization enables implantation of endometrial cells at ectopic sites, a number of putatively distinguishing features should be considered. First, it is not unreasonable to assume that neonatal eMSCs and endometrial epithelial progenitor cells are longer lived, less committed, and more multipotent than their adult counterparts. Conversely, the potential of more differentiated or aging endometrial progenitor cells seeded later in life to form hemorraghic endometriotic lesions may be greatly diminished. Second, increased platelet activation, especially in the context of preeclamptic pregnancies, and a more naive immune system may further increase the implantation density of endometrial stem/progenitor cells at NUB compared to cyclic menstruation. Furthermore, prolonged enforced dormancy of these implants, from birth until the menarche, may lead to selection of more aggressive lesions. Bone marrow-derived cells may also be recruited to the developing lesions, promoting their progression and rapid development soon after the menarche. 51 As illustrated by the changing nature of endometriomas, the angiogenic potential of the ectopic implants is likely the primary driver of disease progression with recurrent tissue injury, bleeding, and repair ultimately resulting in largely fibrotic lesions.
Our 2-pronged origins of endometriosis hypothesis should focus and advance the search for discriminatory cellular or molecular markers that identify patients at risk of progressive disease. This is an obligatory step to make precision medicine in endometriosis a reality. Systematic recording of the presence or absence of NUB in neonatal records has the potential to significantly change our understanding of the origins of endometriosis. Unfortunately, even if this simple measure is put in place, it will take decades for prospective studies to prove or disprove a link between NUB and endometriosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study by C.I.G. was funded by a Senior Research Fellowship (CEG) from the National Health and Medical Research Council of Australia (1042298, CEG) and Victorian Infrastructure Support Program.