
Abstract
Background:
Accurate and painless glucose monitoring remains a major challenge in diabetes management. To address this need, we developed a compact, portable, and non-invasive continuous glucose monitoring (CGM) device based on transdermal band-pass Raman (BPR) spectroscopy intended for benchtop point-of-care use.
Methods:
The BPR-CGM optically probes the molecular vibrations of glucose in the interstitial fluid targeting only three ultra-narrow Raman bands to extract glucose concentration trends while compensating for background variations through intra-spectrum referencing. By refraining from collecting redundant full-spectrum information as in standard Raman spectroscopy, our technology overcomes the need for bulky and expensive components while maintaining high sensitivity, making point-of-care non-invasive CGM a reality.
Results:
A six-participant clinical study compared the non-invasive BPR-CGM with a standard blood glucometer and two commercial needle-based CGMs during a standard oral glucose tolerance test, inducing dynamic postprandial glucose variations. Glucose trends inferred by the BPR-CGM closely matched reference blood glucose values without algorithmic lag compensation. Across participants, the device achieved a mean absolute relative difference of 11.34 ± 1.96%, statistically indistinguishable from needle-based CGM sensors performance (10.42 ± 2.46% and 12.93 ± 4.69%). All BPR-CGM readings fell within clinically acceptable zones A and B of the Parkes (consensus) error grid. No adverse skin reactions were observed following the trial.
Conclusions:
These results demonstrate that the BPR-CGM technology can achieve clinical-grade accuracy comparable to invasive systems, paving the way for wearable, needle-free, and miniaturized glucose monitoring solutions.
Keywords
Introduction
There is currently no cure for diabetes. The number of adults living with the disease is projected to reach 700 million by 2045, placing a growing burden on health care systems. 1 Management strategies primarily focus on controlling blood glucose (BG) through monitoring2,3 and insulin therapy, aiming to prevent both acute episodes and long-term complications such as atherosclerotic cardiovascular disease, nephropathy, retinopathy, cognitive decline, and functional disability. 4 Conventional glucose monitors include self-monitoring BG meters, which require finger pricks, and more recent continuous glucose monitoring (CGM) systems, 5 based on needles or subcutaneous implants. Both remain invasive to varying degrees, often leading to pain and reduced user engagement. 6 In particular, needle-based minimally invasive CGMs require adhesive patches that often cause severe skin irritation, require sensor replacement every one to two weeks and come with an operative cost of $2000 to $6000 per year.3,7-10 On the contrary, DePasquale et al 11 recently demonstrated that CGM users show increased time in range and lower hemoglobin A1c (HbA1c) levels compared with BG users. Fully reagent-free non-invasive CGMs with a long lifetime performing with accuracy comparable to blood-based measurements would therefore represent a major advance in diabetes management and care.12,13 Although none are yet commercially available, several optical, electrical, and biochemical approaches have been explored. Direct optical methods target the intrinsic vibrational features of glucose molecules using full-spectrum Raman, 14 near-infrared, 15 mid-infrared, 16 photothermal, 17 and photoacoustic18,19 optical spectroscopy. Other modalities, such as terahertz, 20 microwave, 21 radiofrequency, 22 ultrasound-assisted, 23 and bioimpedance 12 spectroscopy, probe overall optical, electrical, or thermal changes of the tissue. Purely indirect approaches, including photoplethysmography, 24 breath analysis, 25 and alternative fluid sampling 26 such as sweat and saliva, infer glucose from correlated physiological or chemical markers. However, most non-invasive prototypes rely on bulky, expensive instrumentation, limiting portability and point-of-care adoption. Moreover, their accuracy still lags behind invasive CGMs, often compensated by complex artificial intelligence-based corrections that raise concerns about generalizability, interpretability, and trustworthiness.27,28
In this work, we validate the transdermal performance of a compact, portable, non-invasive CGM device based on band-pass Raman (BPR) spectroscopy intended for benchtop point-of-care use. In a cohort of healthy subjects, glucose metrics derived from our BPR-CGM achieved accuracy comparable to that of commercial needle-based CGMs. Unlike conventional Raman systems, our design eliminates the need for bulky and expensive instrumentation, finally opening a path toward truly non-invasive CGM devices with long lifetime and minimal operating cost.
Methods
Band-Pass Raman Technology
We developed a compact, portable BPR-CGM device equipped with a forearm holder interface for transdermal glucose measurements in humans. The instrument, described in detail elsewhere, 29 is intended for benchtop point-of-care use. It measures 31 × 27 × 21 cm and weighs approximately 10 kg (excluding power supplies), primarily due to its aluminum casing (Supplemental Figure 1). The device detects the Raman vibrational signature of glucose molecules diffusing within the interstitial fluid (ISF), characterized by a dominant peak at 1125 cm-1. Unlike conventional full-spectrum Raman systems for transdermal CGM, our patented design eliminates bulky and costly components such as charge-coupled devices and free-space gratings, enabling a compact and cost-effective configuration that maintains sensitivity across the physiological and diabetic glucose concentration ranges. Instead of collecting broadband Raman spectra, the BPR-CGM measures three selected Raman bands through custom ultra-narrow optical band-pass filters (Alluxa): 1120.12/50.11 cm–1 for the glucose peak, and 948.03/24.62 and 1175.32/20.08 cm–1 for the sidebands used as intra-spectrum references to correct for background variations. An 830.35-nm infrared laser illuminates the skin at a 60° incidence angle with 110 mW of power, producing an elliptical 0.5 × 1 mm spot through a quartz window on the device top interface. This illumination delivers a light dose comparable to or lower than previously reported transdermal Raman studies.14,30,31 Each glucose reading lasts approximately 36 seconds, comprising three ten-second acquisitions per Raman band and two three-second pauses for automated filter switching. The Raman signals are detected by an amplified silicon photodiode (Femto, model: FWPR-20-SI), while a silicon-based amplified photodetector (Thorlabs, model: PDA40) simultaneously records the laser intensity back-reflected from the optical window. This secondary channel provides reference data to correct laser power fluctuations and changes in skin refractive properties.
Clinical Study
We conducted a clinical validation of our BPR-CGM technology in a cohort of six healthy adult volunteers. Participants were between 18 and 80 years old and had HbA1c levels below 5.7%. Exclusion criteria included diabetes, pregnancy, anemia, bleeding disorders (eg, hemophilia and Von Willebrand), anticoagulant use (eg, Warfarin or Eliquis), bilateral wrist tattoos, known infectious disease, or inability to fast for 8 hours. All procedures were approved by the Massachusetts Institute of Technology Committee on the Use of Humans as Experimental Subjects (COUHES #2312001174A001). The cohort comprised three males and three females, with one Fitzpatrick type II and two type III participants in each group (Figure 1a). Each participant completed two study visits lasting 1.5 and 5 hours, respectively. During the first visit, blood samples were collected for HbA1c assessment, and two commercial needle-based CGMs (Abbott FreeStyle Libre 3 and Dexcom G7) were applied to the same upper arm. Both devices rely on electrochemical sensing of ISF glucose. To ensure optimal performance of such needle-based sensors, known to improve after 48 hours of wear, 32 the second visit took place after at least two full days of CGM use. Participants fasted for 8 hours prior to the second visit. During this session, glucose levels were simultaneously monitored using four devices (Figure 1b): (1) the non-invasive BPR-CGM, acquiring transdermal ISF glucose readings every five minutes from the other forearm than the one wearing commercial sensors (Figure 1c); (2) a Nova Biomedical glucometer, providing capillary BG readings every ten minutes via finger-prick by clinical staff; (3) the Abbott FreeStyle Libre 3, recording ISF glucose every minute; and (4) the Dexcom G7, recording ISF glucose every five minutes. To induce dynamic glucose variations, participants ingested two 75-g GlucoCrush™ drinks at two different time points, following a standard oral glucose tolerance test (OGTT) protocol.
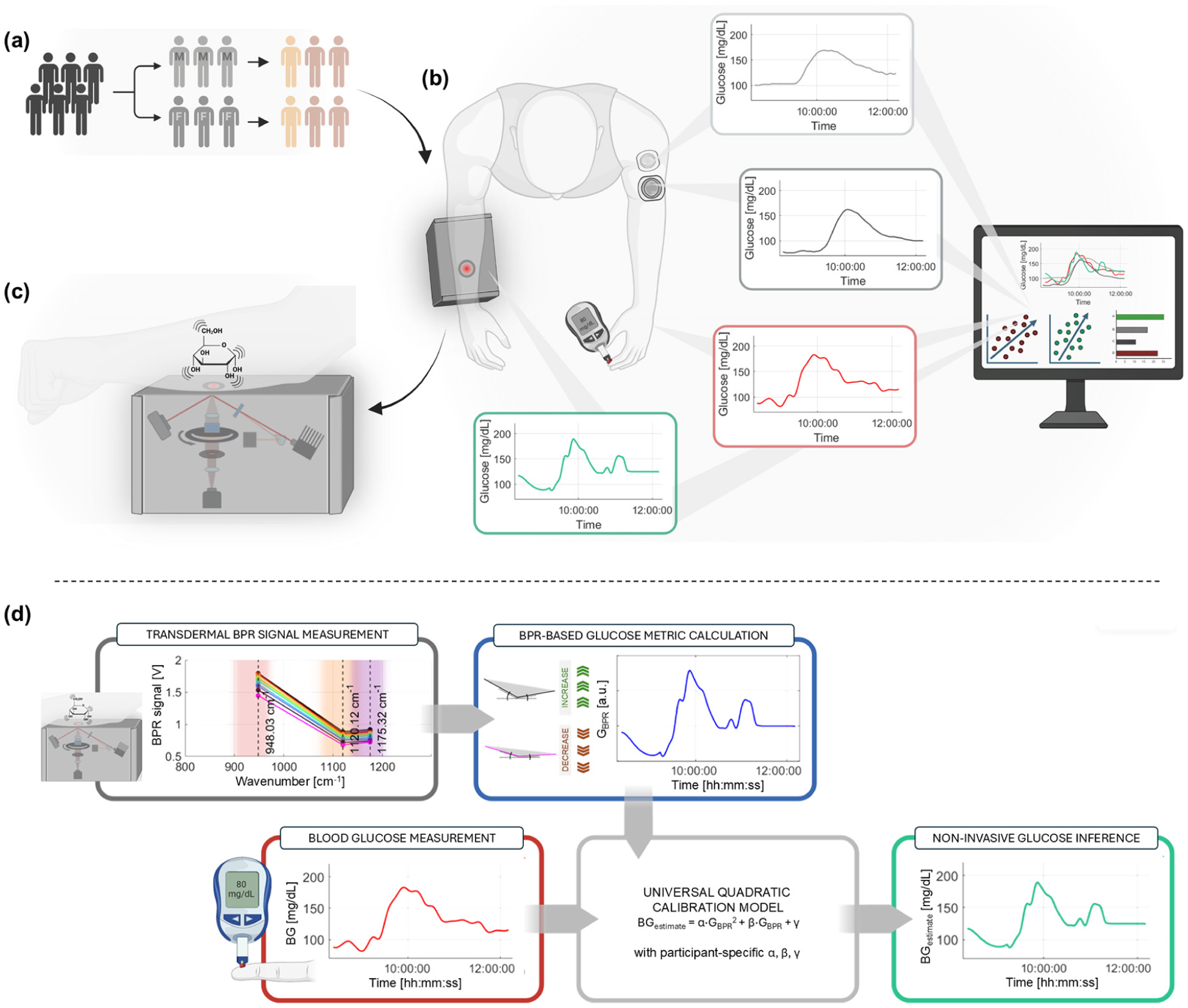
Schematic of the study. (a) Gender (i.e., male [M] and female [F]) and Fitzpatrick skin type level distribution of the six-participant cohort of healthy human subjects. (b) Study rationale: glucose readings are simultaneously recorded via our non-invasive BPR-CGM device and commercial, needle-based, Abbott FreeStyle Libre 3 and Dexcom G7 CGMs. The medical team produces reference BG values via a standard glucometer upon finger-pricking. (c) Technology principle of our BPR-CGM device, which records Raman vibrational signatures of glucose molecules diffusing in the ISF, triggered via an off-axis 830.35-nm laser illumination of the skin. (d) Calibration rationale of the BPR-based metric against reference BG values for non-invasive inference of glucose levels in mg/dL. Created with BioRender.com.
Data Collection and Processing
To ensure temporal alignment across devices, all glucose readings were spline-interpolated at one-minute intervals and trimmed for synchronization. For the BPR-CGM, such interpolation was applied onto the glucose metric value. The BPR glucose metric quantifies the prominence of the glucose Raman peak relative to its sidebands (scaling as the triangular area encompassed by the three-bands signal) and is defined as:
Previous tissue phantom experiments demonstrated a mild quadratic dependence of the BPR metric on glucose concentration, with R2 = 0.895 for a linear fit and R2= 0.995 for a quadratic fit. 29 Based on these findings, we adopted a single, global quadratic calibration model to map the Raman-derived BPR metric GBPR to BG concentration as measured from capillary finger-stick measurements using a commercial glucometer by Nova Biomedical (model: StatStrip). For each participant, calibration coefficients were obtained by least-squares regression between the BPR metric (Supplemental Figure 3) and temporally matched reference BG values, according to BGestimate = α·GBPR2 + β·GBPR + γ, where α, β, and γ are participant-specific calibration coefficients (Figure 1d). Such a universal calibration model with participant-specific parameter tuning is not only valid, but necessary for a proof-of-concept study on a small-scale cohort with limited longitudinal duration per participant: a universal parameter set is unrealistic for early-stage clinical validation. The resulting calibration function was then applied to the full non-invasive BPR-CGM time series to infer glucose concentration in units of mg/dL. As this work aims at validating the effectiveness of non-invasively measured transdermal BPR signal trends as indicators of BG trends, a broader exploration of calibration strategies aimed at maximizing predictive accuracy is left for future work.
Uncertainty in the BPR-derived glucose levels was estimated by propagating the standard deviation of the raw photodetector voltages through the entire processing pipeline. Details on the signal-to-noise ratio of the BPR-CGM device can be found in Supplemental Figure 4. Uncertainty propagation and the derived confidence intervals for BPR-based glucose readings are provided in Supplemental Figure 5.
Results and Discussion
Interstitial fluid glucose levels are known to lag behind BG by approximately 5 to 15 minutes, a delay previously documented for both Raman-based systems33,34 and commercial CGMs.35-37 In this study, no lag-compensation or temporal alignment algorithm was applied; all optical readouts are presented in a temporally unaltered form to allow a more direct assessment of the BPR-CGM performance. To capture multiple glucose excursions and maintain adequate coverage across the normoglycemic range, participants received the first glucose drink within the first 50 minutes of the session and a second at 100 minutes. This protocol reliably induced repeated postprandial peaks, enabling a more comprehensive validation of device performance under dynamic conditions and minimizing the risk for spurious correlation from a relatively simple glucose profile given by a single OGTT drink. The mean ± standard deviation of the pairwise Pearson correlation coefficient of BG curves is R = 0.498 ± 0.3. This broad distribution indicates partial shared structure, as expected for OGTT physiology, but substantial inter-participant variability in temporal dynamics (Supplemental Figure 6).
We report representative data from a 4.5-hour trial (Figure 2). Non-invasive BPR-based glucose readings (green) closely tracked the temporal trends observed with the reference glucometer (red) and with the Abbott FreeStyle Libre 3 (dark gray) and Dexcom G7 (light gray) commercial CGMs (Figure 2a). In this example, the BPR-CGM achieved a mean absolute relative difference (MARD) of 9.06%, demonstrating strong agreement with BG levels.

Single-participant non-invasive BPR-CGM performance referenced to BG readings and compared to needle-based Abbott and Dexcom CGMs. (a) Glucose levels over clinical trial time obtained via BPR-CGM after metric calibration (in green), shown with Abbott FreeStyle Libre 3 predictions (in dark gray), Dexcom G7 predictions (in light gray), and glucometer-based BG values (in red). (b) MARD (%) and Parkes (consensus) error grid analysis of the non-invasive BPR-CGM device. (c) Picture of the participant’s skin after laser irradiation through the 4.5-hour-long trial. No sign of irritation is shown. (d) MARD (%) and Parkes (consensus) error grid analysis of the Abbott FreeStyle Libre 3 sensor. (e) MARD (%) and Parkes (consensus) error grid analysis of the Dexcom G7 sensor.
When paired with reference BG values on the Parkes (consensus) error grid (Figure 2b), all BPR-based glucose readings fell within the clinically acceptable A and B zones: 91.84% of points in zone A and 8.16% in zone B, with no observations in zones C through E. This distribution indicates that all BPR-derived readings would lead to clinically correct or benign treatment decisions. Comparable accuracy was observed for commercial needle-based devices. The Abbott FreeStyle Libre 3 (Figure 2e) and Dexcom G7 (Figure 2d) showed slightly higher MARD values (i.e., 11.06% and 13.03%, respectively) and smaller proportions of zone A readings (i.e., 86.96 and 85.11%, respectively). Figure 2c shows the illumination site on a participant’s forearm after measurement. No erythema, itching, or skin irritation was observed, and no adverse events were reported within 12 months following the study.
Figure 3 summarizes the statistical validation of BPR-CGM performance across the six-subject cohort, which included Fitzpatrick skin types II (fair skin that burns easily and tans minimally) and III (light-to-medium skin that may burn mildly and gradually tans to a light brown). Compared with the Food and Drug Administration (FDA)-cleared CGMs by Abbott and Dexcom, the BPR-CGM exhibited no statistically significant differences in MARD, as determined by the Mann-Whitney U non-parametric test. The BPR-CGM achieved a cohort-average MARD of 11.34 ± 1.96% (mean ± SD), compared with 10.42 ± 2.46% for the Abbott FreeStyle Libre 3 and 12.93 ± 4.69% for the Dexcom G7 (Figure 3a). No significant correlation was found between BPR-CGM MARD values and Fitzpatrick skin type (Pearson’s R = 0.14), supporting robustness across pigmentation levels. Additional correlation analyses between the BPR sensor accuracy and participant-specific variables (i.e., gender, HbA1c, signal decay time constant) are provided in Supplemental Figure 7. It is important to note that the BPR-CGM results were obtained without algorithmic lag compensation or proprietary data-correction procedures. Such processing steps, implemented in commercial CGMs to refine temporal alignment and suppress noise, 38 can alter signal dynamics and influence MARD values. 39 Here, no lag correction was applied, and the original BPR-based time series are reported as part of the feasibility study, while avoiding additional model assumptions or time-domain manipulations. As established in prior work on Raman-based glucose sensing, 33 glucose transport from blood to ISF introduces participant-specific, direction-dependent time shifts. During rapid glucose increases, BG rises first and ISF glucose follows with a delay, whereas during glucose downstroke the compartments can exhibit different clearance rates, which can produce apparent relative temporal shifts between compartments that are not fully captured by a simple uniform time delay, as illustrated in Figure 2. These considerations motivate the need for physics-informed lag correction in future studies, since blood-to-interstitial glucose dynamics are not adequately described by a simple uniform time shift and are better represented by compartmental diffusion and clearance modeling. 40 At the same time, we emphasize that the reported BPR-CGM MARD values arise from participant-specific post-processing and calibration, which inherently limits strict quantitative comparability with factory-calibrated commercial CGMs. In commercial systems, factory calibration is derived from large population data sets and embedded into proprietary algorithms. 41 Developing an equivalent population-level calibration framework is beyond the scope of this study but represents a necessary outlook for translation.

Multi-participant non-invasive BPR-CGM performance referenced to BG readings and compared with needle-based Abbott and Dexcom CGMs. (a) Six-participant MARD (%) values (mean ± SD) of our BPR sensor (in green), and of the commercial needle-based CGMs by Abbott (in dark gray) and Dexcom (in light gray). No significant differences (ns) across devices as per the Mann-Whitney U test for non-normal populations. (b) AR 20/20 (%) and AR 15/15 (%) performance metrics of our BPR sensor (in green), and of the Abbott (in dark gray) and Dexcom (in light gray) needle-based commercial CGMs. Differences in AR across devices are not statistically significant (ns), as per the Mann-Whitney U test for non-normal populations, corroborating the comparable performance of our solution to commercial needle-based sensors. Multi-participant Parkes (consensus) error grid analysis results of the Raman-based CGM (c), of the Abbott FreeStyle Libre 3 (d), and of the Dexcom G7 (e) are reported for comparison of BG levels prediction accuracy. Bland-Altman test, including bias and limit of agreement (LoA) values for our Raman-based sensor (f), for the Abbott FreeStyle Libre 3 (g), and for the Dexcom G7 (h). Rate-of-change (RoC) analysis, with slope and the Pearson correlation coefficient (R) for our BPR-based sensor (i), for the Abbott FreeStyle Libre 3 (j), and for the Dexcom G7 (k).
Agreement rate (AR) metrics further support the system performance (Figure 3b). Using the Mann-Whitney U test, no significant differences were found between the BPR-CGM and commercial CGMs. The AR 20/20 (i.e., the percentage of readings within 20% of the reference value for concentrations higher than 100 mg/dL or within 20 mg/dL of the reference value for concentrations equal to or lower than 100 mg/dL) reached 87.35 ± 8.66% for the BPR-CGM, compared with 89.63 ± 7.24% for the Abbott FreeStyle Libre 3 and 81.07 ± 19.84% for the Dexcom G7. Under the more stringent AR 15/15 criterion (i.e., the percentage of readings within 15% of the reference value for concentrations higher than 100 mg/dL or within 15 mg/dL of the reference value for concentrations equal to or lower than 100 mg/dL), the BPR-CGM achieved 74.44 ± 6.23%, while the Abbott and Dexcom sensors yielded 80.22 ± 12.19% and 62.73 ± 16.18%, respectively. Notably, the BPR device showed greater reproducibility than the commercial comparators, with lower standard deviations in both MARD and AR 15/15 metrics. To assess the performance of our BPR-CGM sensor with greater granularity, we computed ARs within glucose ranges. Interestingly, while the Raman-based sensor shows lower AR 20/10 and AR 15/15 mean values within 70 to 100 mg/dL BG levels compared with needle-based CGMs, it achieves greater on average ARs at all higher BG brackets (i.e., 100-120, 120-140, and 140-200 mg/dL), as reported in Supplemental Figure 8. Such a behavior can be explained by the BPR-CGM sensor approaching its limit of detection of 37.53 ± 15.05 mg/dL at lower BG levels, with a predominantly quadratic scaling of signal and glucose concentration in the illuminated volume. 29
For reference, commercial CGMs typically report AR 20/20 values of about 85% to 95% and AR 15/15 values of 80% to 90%. 42 As per FDA CGM criteria, more than 87% of values must be within ±20% of the reference standard across the measuring range. 43
Multi-participant Parkes (consensus) error grid analysis (Figure 3c) provides a comprehensive view of the device performance across the study cohort. All Raman-derived glucose estimates fell within clinically acceptable zones A and B, confirming the robustness of the BPR-CGM across subjects. Specifically, 86.21% of readings were in zone A, compared with 88.62% and 78.34% for the Abbott (Figure 3d) and Dexcom (Figure 3e) devices, respectively. The remaining 13.79% of BPR-CGM readings were in zone B (Figure 3c), consistent with 11.38% for Abbott (Figure 3d) and 21.66% for Dexcom (Figure 3e).
Bland-Altman test results quantify systematic bias and limit of agreement (LoA) between the CGM sensors and BG. The BPR-CGM shows an almost null measurement bias of 0.29 mg/dL (Figure 3f), while Abbott and Dexcom showed mean biases of −7.31 mg/dL (Figure 3g) and 6.57 mg/dL (Figure 3h), respectively. The LoA width is comparable to Abbott and lower than Dexcom. Most concurrent pairs fall inside the LoA for all sensors. For the BPR-CGM, a subtle trend was observed at BG levels below 100 mg/dL BG, consistent with the reduced AR 20/20 and AR 15/15 values in the 70 to 100 mg/dL range (see Supplemental Figure 8).
Beyond static accuracy metrics, we performed a rate-of-change (RoC) analysis that enables the evaluation of the BPR-CGM dynamic fidelity and quantifies the impact of the time lag between ISF- and blood-based glucose monitors. The slope of the RoC relationship reflects the extent to which glucose dynamics are attenuated by each sensing modality and its associated processing pipeline: our BPR strategy features a RoC slope of 0.31 (Figure 3i), lower than the 0.44 RoC slope of Abbott and Dexcom (Figure 3j and k). The Pearson correlation coefficient (R) between device RoC and reference BG RoC is lower for Raman-based readings (i.e., R = 0.33 vs R = 0.55 for Abbott FreeStyle Libre 3 and R = 0.49 for Dexcom G7; Figure 3i-k). This denotes a weaker temporal coupling of the BPR-BG dynamics and directly reflects the lack of time lag compensation in our data processing pipeline, which is likely implemented in the proprietary algorithms of the commercial needle-based devices. These results indicate that future lag-compensation strategies may further improve BPR-CGM performance.
Together, these results indicate that the measured inference accuracy and reproducibility provide a technological basis for future miniaturized and potentially wearable Raman-based CGMs. This study demonstrates this capability using a proof-of-concept, fully non-invasive, compact, tabletop BPR spectroscopy platform currently already suitable for point-of-care deployment.
Conclusions
This study demonstrates that BPR spectroscopy enables accurate and reproducible non-invasive transdermal glucose sensing through compact optical instrumentation. By replacing broadband spectrometers with narrow-band detection of glucose-specific Raman features, the BPR-CGM achieves accuracy comparable to FDA-approved needle-based sensors while maintaining a lightweight, portable, and compact design. The present clinical validation, conducted on a small cohort of participants without diabetes and over a restricted glucose dynamic range, establishes the feasibility, stability, and robustness of the BPR approach at a proof-of-concept stage.
Future work will refine calibration strategies to transition the system from inference-based to predictive operation, enabling subject-independent glucose estimation. Engineering advances in miniaturization, integrated low-power laser sources, and on-chip photodetection will further enhance portability and cost-efficiency. Broader validation on cohorts with diabetes, across wider glucose excursions, and including darker Fitzpatrick skin types will be critical to confirm generalizability and guide translation toward wearable, needle-free BPR-CGMs.
Supplemental Material
sj-docx-1-dst-10.1177_19322968261445056 – Supplemental material for Clinical Validation on Healthy Humans of a Portable Non-invasive Continuous Glucose Monitor Based on Transdermal Band-Pass Raman Spectroscopy
Supplemental material, sj-docx-1-dst-10.1177_19322968261445056 for Clinical Validation on Healthy Humans of a Portable Non-invasive Continuous Glucose Monitor Based on Transdermal Band-Pass Raman Spectroscopy by Arianna Bresci, Youngkyu Kim, Miyeon Jue, Lorenza Pia Foglia, Elyse Moores, Peter T. C. So and Jeon Woong Kang in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
AR, agreement rate; BG, blood glucose; BPR, band-pass Raman; CGM, continuous glucose monitoring; FDA, Food and Drug Administration; ISF, interstitial fluid; MARD, mean absolute relative difference.
Author Contributions
JWK was responsible for conceptualization. AB contributed to optical system development, software, formal analysis, and visualization. AB was also responsible for sample preparation. AB and YK were responsible for data acquisition. AB, LPF, and EM contributed to data curation. AB, YK, and JWK were responsible for clinical trials. MJ, PTCS, and JWK supervised the project and funding acquisition. AB wrote the original draft of the manuscript. MJ, LPF, and JWK were responsible for manuscript revision. All authors have given approval to the final version of the manuscript. The authors are grateful to Tatiana Urman, MSN, RN, Libby Schultz, BSN, RN, and Catherine Ricciardi, DNP, ANP-BC, for their help with the human subject experiment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health (P41EB015871, UH3CA275687, R01DC021326), National Cancer Center, Korea (NCC-24H1170), Korea Technology and Information Promotion Agency for SMEs (TIPA) (RS-2025-25458481) and Apollon Inc. The clinical study was conducted at the Center for Clinical and Translational Research (CCTR) at the Massachusetts Institute of Technology, supported by the National Center for Advancing Translational Sciences, National Institutes of Health, Award Number UL1TR002544. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YK and MJ are employees of Apollon, a company developing needle-free Raman-based non-invasive CGM devices.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.