
Abstract
Background:
Diabetes mellitus (DM) and its complications have wide-ranging effects on numerous aspects of health, particularly as they affect individual’s static and dynamic balance. Balance assessments and interventions have emerged as key components of rehabilitation strategies for individuals with DM. As part of the growing incorporation of virtual reality (VR) technology into rehabilitative, this systematic review aims to synthesize the current evidence on VR-based assessment and interventions for balance in individuals with DM.
Methods:
A comprehensive search of electronic database including PubMed, Embase, CINAHL, Cochrane, and PEDro was conducted from the inception through April 2024. Studies applying VR technology either as balance assessments or interventions among individuals with DM were made potentially eligible for inclusion.
Results:
A total of 12 studies were included according to the inclusion criteria, which included 345 individuals with DM. Four studies utilized VR for balance assessment, revealing that individuals with DM exhibited impaired balance compared with healthy controls. Eight studies applied VR tools for balance training. Despite variations in statistical significance, all studies reported enhanced balance after VR interventions.
Conclusion:
This systematic review summarizes VR as an innovative and interactive approach, demonstrating its applicability and usefulness in both balance assessment and intervention among individuals with DM.
Introduction
Diabetes mellitus (DM), a chronic metabolic disorder characterized by increased blood glucose levels, is increasingly prevalent in many high- and middle-income countries. 1 The World Health Organization predicts that by 2030, DM will be the seventh leading cause of death worldwide. 2 As of 2023, approximately 39 million individuals in the United States had been diagnosed with DM. This disease commonly leads to complications such as nephropathy, retinopathy, and diabetic peripheral neuropathy (DPN), all of which negatively affect sensory perception, cognitive functions, and motor control—key elements for maintaining balance.3-5 Individuals with DM often experience balance impairments due to somatosensory or vestibular dysfunctions,6,7 cognitive decline, and increased postural sway. These deficits are associated with postural instability and a heightened risk of falls,8,9 ultimately contributing to a lower quality of life.10,11
Balance including both static and dynamic components is essential for effective patient management in individuals with DM. 12 Static balance is a measure of one’s ability to maintain an erect posture while managing body sway, 13 while dynamic balance is the maintenance of stability through movement of the body.14,15 Clinical tools such as the Functional Reach Test and the Berg Balance Scale (BBS) are used to assess static balance in adults with DM,16-19 while dynamic balance is assessed through the Timed-Up-and-Go (TUG) and Dynamic Gait Index (DGI) tests and is often administered in conjunction with obstacle or cognitive tasks.16,17,20 Given the multifactorial character of balance impairments in DM, there is no single assessment tool that has been globally recommended. To address and improve balance, conventional measures such as resistance training and gait exercises have been widely used. Empirical evidence shows that the addition of ankle strengthening exercises to gait training is common, with evidence supporting the effectiveness of ankle strengthening plus progressive gait challenges to improve both static and dynamic balance in the DM population.21,22 However, optimal intervention strategies for this population remain unclear.
Virtual reality (VR) technology holds tremendous promise in improving the rehabilitation in the form of secure, reliable, and standardized assessment and intervention measures.23-25 Virtual reality offers objective, computerized assessments in a variety of metrics and enables the development of innovative procedures that extend beyond conventional measures. 26 By providing a complicated sensory experience with multiple sensory modalities stimulated, including visual, auditory, and proprioceptive modalities, VR encourages multisensory processing and simultaneously activates motor and cognitive function.27-29 In addition, VR supports simultaneous motor and cognitive engagement, promotes physical recovery, and stimulates neural activity (eg, cortical remapping). 30 As an affordable technology with low adverse events, VR is especially efficient for application in a clinic-based setting and can potentially optimize patient motivation for participation in rehabilitation efforts.9,31,32
Recent studies have explored the use of VR in clinical balance assessment, showing its potential to enhance its evaluation accuracy. 23 Virtual reality–based intervention has also demonstrated efficacy in improving balance in patients with Alzheimer’s disease, multiple sclerosis and Parkinson’s disease.33-35 Several systematic reviews and meta-analyses have explored the use of VR in individuals with DM.36-38 One review reported significant improvements in static balance following VR-based interventions, 37 while another demonstrated positive effects on both static and dynamic balance in individuals with DPN, favoring VR-based rehabilitation over conventional interventions. 36 Given the varied complications of DM, it is uncertain whether VR-based balance interventions can provide consistent benefits across the broader DM population. While VR has shown promise for improving balance, its utility as an assessment tool has been less explored. 38 As VR offers innovative clinical assessment capabilities, a focused review of its application in both assessment and intervention is warranted to support its integration into rehabilitation for DM. 26 This systematic review aims to summarize current applications of VR balance assessment and intervention in individuals with DM, with the goal of informing clinical practice and supporting the integration of VR into routine balance management.
Methods
Study Design and Registration
The protocol for this systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42024552013). This review was conducted in accordance to with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 39 and the detailed search strategy is provided in the Supplementary Material.
Selection Criteria and Outcomes
This systematic review included English-language studies involving adults (≥18 years) with Type 1 or Type 2 DM, with or without complications such as retinopathy or peripheral neuropathy. Eligible studies used VR for balance assessment or intervention and included randomized controlled trials, quasi-experimental designs, observational studies, and single-arm pre-post studies. Virtual reality–supported rehabilitation was defined as any intervention or assessment using tools that deliver augmented, real-time performance feedback and engage participants with a simulated environment through multiple sensory inputs channels. 40 Virtual reality environments can be classified as immersive, semi-immersive, non-immersive, or augmented. Immersive VR fully engages multiple senses (eg, sight, sound, touch) to create a strong sense of presence within the virtual environment. Semi-immersive VR allows partial interaction without fully enclosing the user, while non-immersive VR enables interaction with a computer-generated environment without sensory immersion. 41 Included studies examined VR-based static or dynamic balance interventions compared with conventional care, as well as standalone VR applications without comparison.
The primary outcome of this review was balance performance, reported via postural sway (eg, center of pressure), gait metrics (eg, step length), and clinical measures. Intervention studies included both objective tests such as BBS, Mini Balance Evaluation Systems Test (Mini-BESTest), and TUG, while subjective scales such as the Falls Efficacy Scale-International (FES-I) and Activity-specific Balance Confidence (ABC). Fall incidence was considered as a secondary outcome.
Extraction of Data and Identification of Studies
References identified through database searching were then entered into Covidence (Melbourne, Australia), where duplicate entries were removed systematically. Two reviewers (KC and FA) then made independent title and abstract screens for exclusion of studies considered irrelevant, with subsequent full text evaluation for final eligibility. Reasons for exclusion were noted. Any disagreements were resolved through discussion with a third reviewer (CH).
Assessment of Risk of Bias and Methodological Quality
Two reviewers (KC and FA) independently assessed risk of bias and study quality, with a third reviewer (CH) resolving discrepancies. Randomized controlled trials (RCTs) were evaluated using the Cochrane Risk of Bias tool (RoB 2), covering five domains and rated as “low risk,” “some concerns,” or “high risk,” along with an overall judgment. 42 For non-RCTs, the LEGEND (Let Evidence Guide Every New Decision) appraisal tools were used to assess reliability, validity, and applicability, with studies rated as “good,” “lesser,” or “not valid, reliable, or applicable.”
Results
A total of 874 studies were identified and 12 studies met the inclusion criteria for this systematic review.43-54 Figure 1 represents the PRISMA flow diagram with exclusion reasons. Among the included studies, four focused on assessment46,49,53,54 and eight on intervention.43-45,47,48,50-52 Collectively, they involved 345 participants with DM with ages ranged between 45 and 79. One study included a comparison group of younger healthy adults (mean age 26.1 ± 5.0 years).53,54 Six studies included people with DPN specifically. 44 ,46-50 The HbA1c level ranged from 7% to 8.9% and study durations varied from a single session to 12 months. Table 1 presents the study design and characteristics.
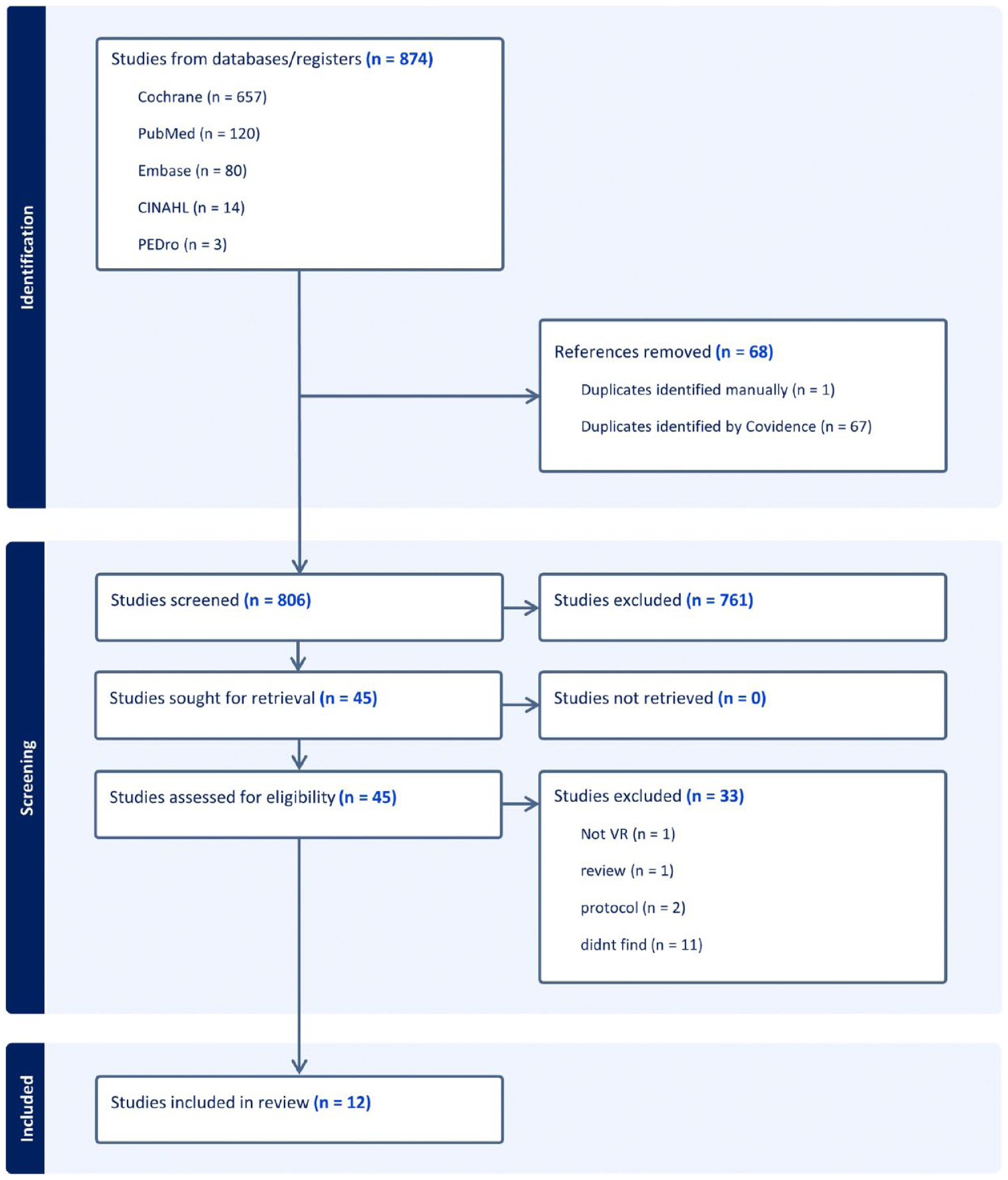
PRISMA flow chart of the study selection.
Characteristics of Included Studies.
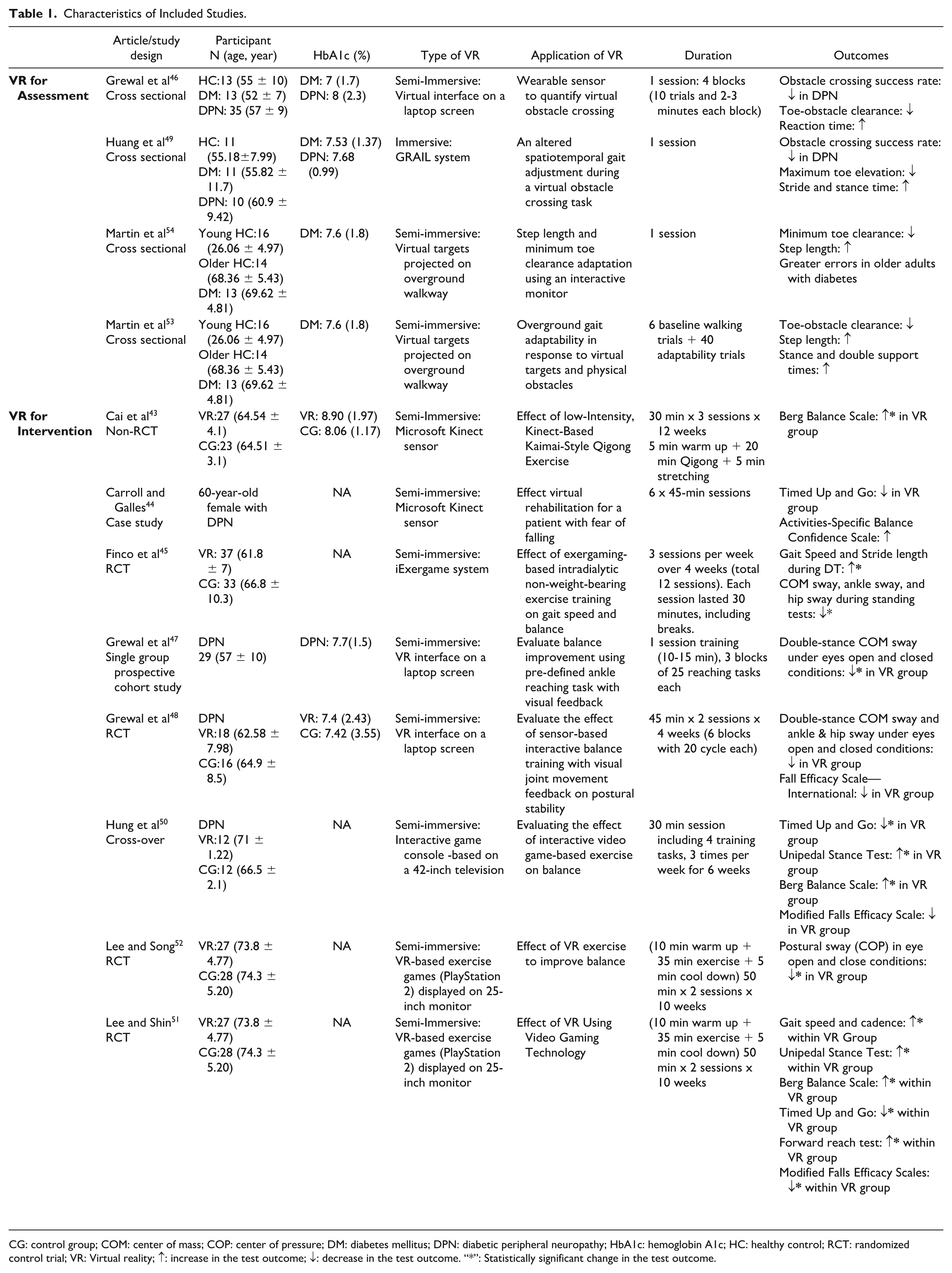
CG: control group; COM: center of mass; COP: center of pressure; DM: diabetes mellitus; DPN: diabetic peripheral neuropathy; HbA1c: hemoglobin A1c; HC: healthy control; RCT: randomized control trial; VR: Virtual reality; ↑: increase in the test outcome; ↓: decrease in the test outcome. “*”: Statistically significant change in the test outcome.
Risk of Bias and Methodological Quality
Among the 12 selected studies, there were four cross-sectional studies, four RCTs, one non-RCT, one prospective cohort study, one case study, and one cross-over study. Risk of bias assessment of the four RCTs (Figures 2 and 3) classified one as low risk 51 and three as moderate risk.45,48,52 Assessors were not blinded in those three studies, which led to some concerns about bias from outcome measurement. Grewal et al 48 applied a self-developed VR setting, leading to some concern about bias from tool standardization. Lee et al and Finco et al 45 failed to report adverse events, which might cause bias due to missing outcome data. The studies with a design other than RCT were rated as moderate to good quality using the LEGEND appraisal tool (Table 2). Validity concerns were noted in Cai et al 43 due to the non-randomized design and unblinded participants, and Grewal et al 47 due to lacking control group. Overall, all studies demonstrated moderate to high methodological quality, with some concerns related to measurement and data reporting.
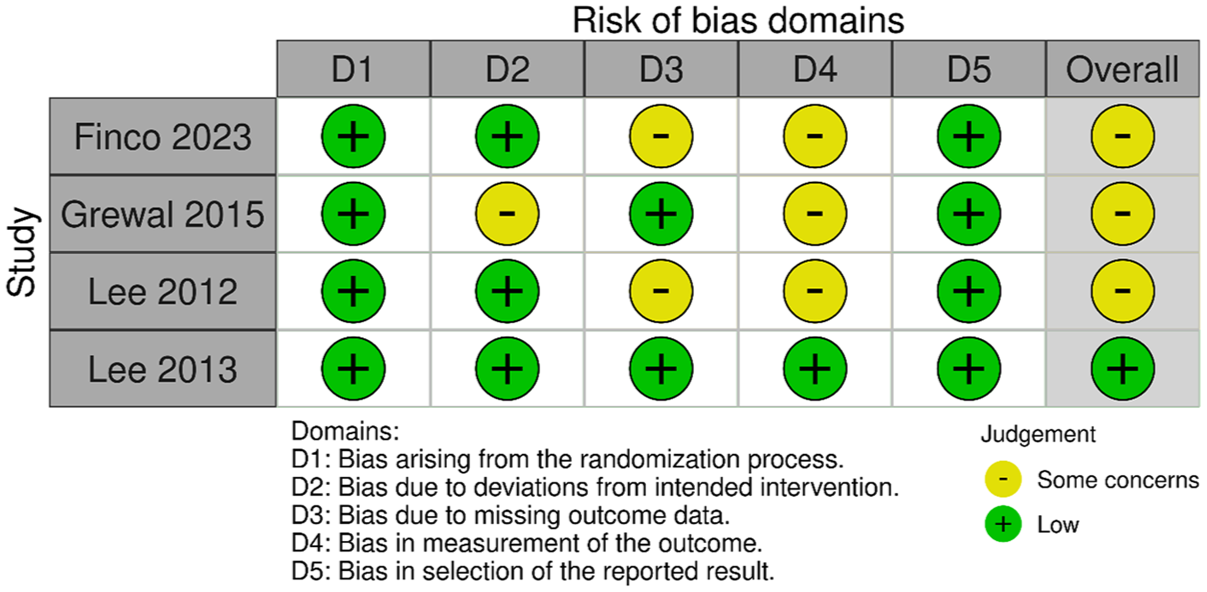
Risk of bias for selected RCT studies.
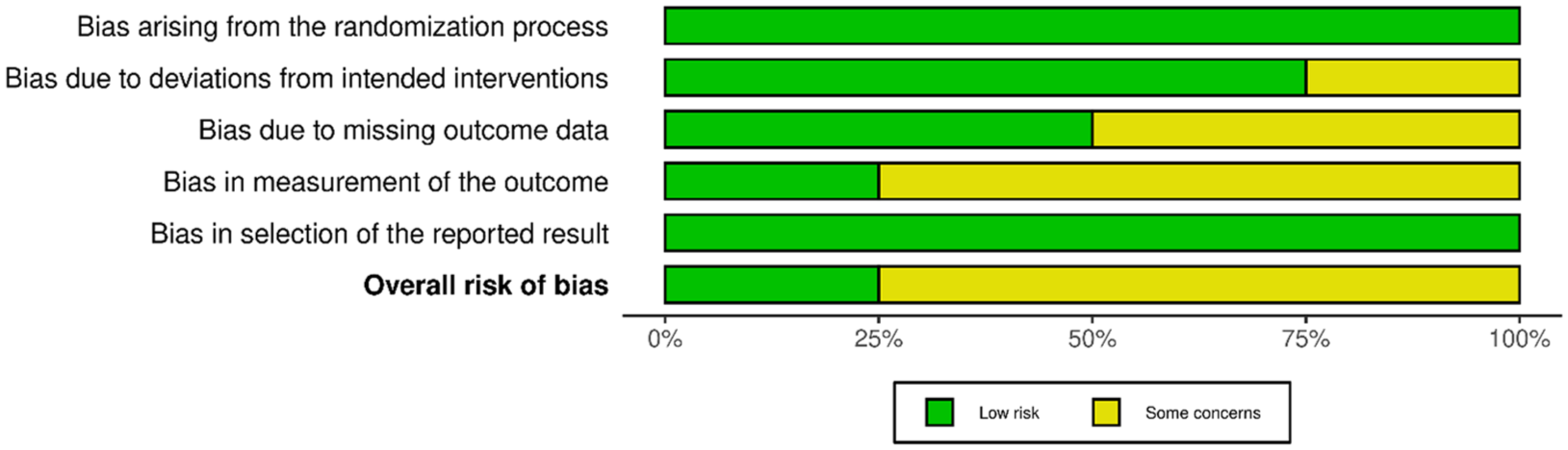
Overall risk of bias for RCT studies presented in percentage.
Quality Assessment Using the LEGEND Appraisal Tools. 55
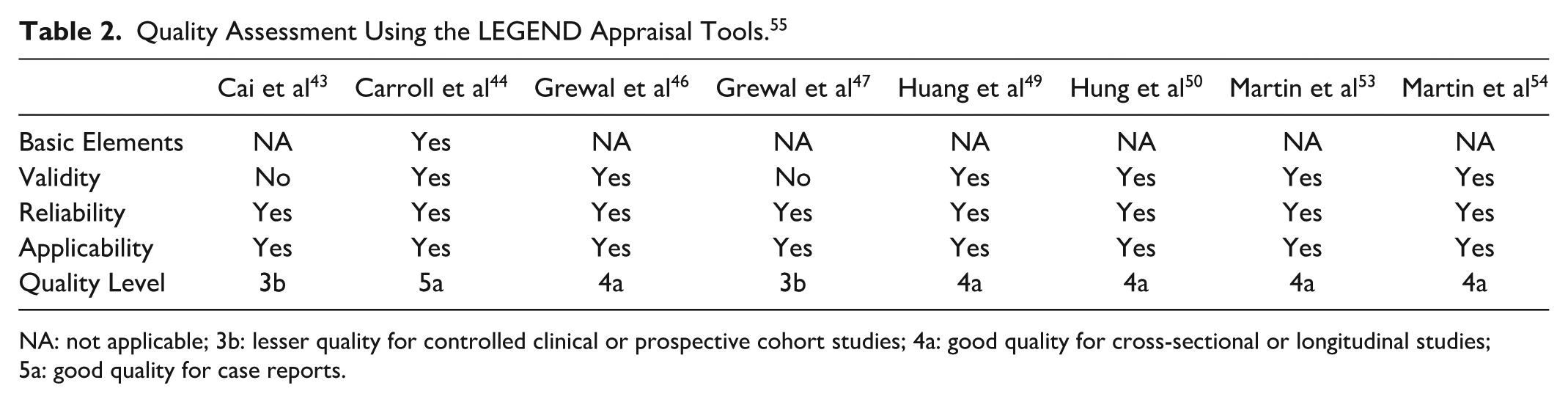
NA: not applicable; 3b: lesser quality for controlled clinical or prospective cohort studies; 4a: good quality for cross-sectional or longitudinal studies; 5a: good quality for case reports.
Experimental Settings
Virtual reality tools with different levels of immersion (eg, immersive and semi-immersive) were applied for training or assessing balance (Table 1). One study 49 applied immersive VR protocol (GRAIL system) while 11 studies43-48,50-54 applied semi-immersive protocols (eg, interactive software and exergaming). In four assessment studies, all focused on assessing the dynamic balance (eg, gait during obstacle crossing).46,49,53,54 In eight interventional studies,43-45,47,48,50-52 four focused on improving static balance,43,47,48,52 one targeted dynamic balance 44 and three investigated both static and dynamic balance improvement.45,50,51 The duration of the training session ranged from 10 to 50 minutes, including breaks between tasks.
In assessment studies, Grewal et al 46 applied a virtual obstacle crossing paradigm to assess crossing performance, where participants interacted with virtual obstacles on a laptop screen. Martin et al examined the gait performance through an interactive system. Virtual step length targets were projected, along with a physical (5 cm) obstacle.53,54 Participants were asked to walk on the treadmill to match targets of step length while avoiding the obstacle. Huang et al 49 applied GRAIL treadmill system with a virtual environment projected onto a cylindrical screen based on the three-dimensional motion capture system. Participants were asked to step over virtual obstacles while walking on the treadmill, and dynamic balance performance was evaluated.
Among intervention studies, Cai et al 43 proposed Kaimai-style Qigong intervention program based on the Kinect system, which enabled incorporating body tracking to guide participants to perform Qigong exercise. Participants were engaged in 30-minute sessions three times a week for 12 weeks. Grewal et al 47 introduced point-to-point ankle-reaching training using a sensor-based interactive approach. Building on these methods, in 2015, both sensor-based ankle-reaching training and interactive-interface-based obstacle crossing training were employed to improve balance. 48 Based on the Kinect sensor, Carroll and Galles 44 built custom VR games for balance training. Participants were asked to play games such as guiding a car along a track or navigating a boat, while performing balance and movement exercises. They were also supported by a weight-bearing harness in the initial session and the reliance on harness was decreased in later sessions. Six 45-minute training sessions were completed. Finco et al 45 applied exergaming-based intradialytic exercise system combined with wearable sensors to track real-time foot movements. Participants were asked to perform non-weight-bearing ankle exercises during hemodialysis, with 30-minute sessions three times a week for four weeks. Hung et al 50 proposed training by employing an Interactive Video-Based (IVGB) system. Participants were asked to perform exercises on a stepping mat while interacting with virtual characters of games. Lee and Shin 51 and Lee and Song 52 applied VR-based exercise system including tasks such as window cleaning and bowling, aiming at static and dynamic balance improvement.
Outcome Measures
Synthesis of results is shown in Table 1. Four studies applied immersive and semi-immersive VR tools for dynamic balance assessment in one session.46,49,53,54 Older healthy and DM adults (defined as individuals over 60 years of age) were compared in these four studies, while two of them also compared findings with healthy younger adults.53,54 All four studies used virtual obstacle paradigm to evaluate dynamic balance parameters, and three evaluated spatiotemporal gait variables. No study applied VR for static balance assessment. All four studies applied VR tools to evaluate balance were able to record the deterioration in dynamic balance for individuals with DM when compared with healthy controls.
Eight studies applied semi-immersive VR tools for balance training purposes for older adults with DM.43-45,47,48,50-52 The duration of total training programs was inconsistent between studies with a range from 4 to 12 weeks. Grewal et al 47 applied semi-immersive VR training for one session only. The most used outcome to assess static balance before and after VR intervention is postural sway during double and single leg stance with eyes open or closed. Besides, TUG was the most used measure to assess dynamic balance improvement after VR intervention. While the statistically significant level was varied within included studies, all of them revealed enhancement in both static and dynamic balance performance after VR rehabilitation program. Regarding the safety, no significant adverse event was reported in all included studies.
Discussion
This systematic review summarized current applications of VR-based assessments and interventions for balance in individuals with DM. Four assessment studies (n=82) demonstrated that VR tools can effectively detect balance impairments. Eight intervention studies (n=263) consistently reported balance improvements following VR-based training. These findings highlight VR as a promising tool for both evaluating and enhancing balance in people with DM. Its interactive and engaging nature may improve rehabilitation outcomes and address key challenges.
Impact of VR on Balance Rehabilitation
To assess balance in individuals with DM, two studies applied VR technology to emulate virtual obstacles to perform obstacle crossing task (OCT).46,49 Obstacle crossing task is a widely adopted method to assess gait and balance by requiring participants to step over obstacles.56-58 In DM population, reduced toe-obstacle clearance in both legs has been observed during actual OCT, increasing the risk of tripping.59,60 Hsu et al 60 reported tripping incidents in three participants who contacted physical obstacle. In contrast, virtual OCT revealed similar impairment such as decreased toe-obstacle clearance and crossing success rate. In addition, individuals with DM showed increased reaction time, stride time, and stance time during virtual OCT. This highlights the advantage of virtual OCT in safely assessing dynamic balance. Another study used VR to project step targets during overground walking, finding increased step length, stance time, and double support time in participants with DM. 53 Martin et al 53 used an interactive system displaying virtual targets on a monitor, showing individuals’ peak step length and toe clearance, and asked participants to match these peaks accordingly. The study identified gait impairments in DM, including decreased toe clearance, increased step length, and greater response errors. These deficits are linked to central nervous system impairments in DM, which hinder processing and integration of sensory information for voluntary postural adjustments. 5 This leads to delayed evoked potentials during walking and reduced peripheral nerve conduction velocity, causing slower or inappropriate responses and impaired postural control. 61 In summary, VR technology provides an interactive method for balance assessment, delivering valuable insights into motor and cognitive responses to external stimuli during balance control.
In intervention studies, combining VR with exercise training (eg, exergaming) is a common approach for balance rehabilitation in people with DM. Exergaming delivered via screens, controllers, and specialized software is recognized as a valid and safe therapeutic tool. 62 It is widely used in clinical practice due to its motivational benefits over repetitive traditional tasks, 62 and enables autonomous at-home rehabilitation, enhancing convenience and efficiency. 63 Selected intervention studies reported balance improvements measured by clinical tools such as the BBS, TUG, FES-I, unipedal stance test, forward reach test, activity-specific balance confidence scale, and modified falls efficacy scales.
VR Settings in Balance Rehabilitation
Both immersive and semi-immersive VR systems showed effectiveness in assessing and improving balance. Most included studies utilized semi-immersive VR systems, which typically use screens, projections, and controllers to balance virtual engagement and with real-world interaction. Due to their lower cost, simpler setup, and ease of use, semi-immersive VR may be more practical for broader clinical implementation while still offering meaningful benefits.64-66 One study applied a fully immersive gait analysis system to assess dynamic balance, but its high cost and specialized equipment limit accessibility in clinical settings. 49 To enhance the feasibility of fully immersive VR in rehabilitation, head-mounted displays (HMD) offer a promising alternative. Head-mounted displays are lightweight, portable, and cost-effective, allowing users to be fully immersed in customizable virtual environments with real-time feedback. 67 They can also safely and effectively emulate challenging real-world scenarios such as obstacle crossing. 68 Such characteristic allows assessment or intervention to take place in a safe and non-threatening yet realistic environment. 69 Full immersion enhances embodiment, which can improve neurofeedback performance and offer additional advantages in rehabilitation. 70 Advances in HMDs such as wider field of view, higher resolution, and reduced motion sickness have made fully immersive VR more accessible and practical in rehabilitation benefits compared with non-immersion or semi-immersion setups. 71 These improvements position immersive VR as a promising tool in rehabilitation, with growing research interest. However, further investigation is warranted in the diabetes population.
Multimodal Technological Approaches in VR Balance Training
Rather than solely assessing postural sway, four studies utilized inertial measurement units (IMUs) to create interactive VR environments by providing real-time feedback on body movements.45-48 This setup allowed participants to adjust their posture dynamically, enhancing postural control and potentially reducing fall risk in individuals with diabetes. Inertial measurement units are wearable devices track changes of position, acceleration, and orientation, showing potential as user-friendly motion analysis tools in clinical settings. 72 Compared with traditional motion capture systems, IMUs offer advantages in portability, cost, and clinical usability. 73 Future studies combining IMU technology with semi-immersive VR may offer a practical and efficient approach for balance training and long-term progress monitoring.
Limitations and Future Directions
Despite promising findings, several limitations should be acknowledged. First, research in VR-based balance assessment in DM remains limited, with current findings are primarily on dynamic balance. Future research might consider exploring VR applications for standing balance, such as the VR-based Sensory Organization Test (SOT), which offers a cost-effective, space-saving alternative to conventional SOT systems that have revealed sensory-related balance impairments in DM.25,74 Second, key baseline data—such as diabetes duration, HbA1c levels, and medication use—were inconsistently reported. Third, heterogeneity in study duration, sample size, and VR protocols hinders cross-study comparisons. While these variations still lead to similar improvements in balance and suggest consistent balance performance in individuals with DM across all studies, the impact of these differences makes it challenging to establish optimal VR rehabilitation protocols for the DM population, despite the overall robust effect of VR rehabilitation on balance. Larger, more diverse cohorts and standardized methodologies are needed to validate VR’s utility in DM population.
Further research is needed to explore the long-term effects of VR interventions on balance in individuals with DM. Investigations into the optimal frequency, duration, and type of VR interventions will help in developing evidence-based guidelines for clinical practice. More balance assessment studies using VR are limited and more research are warranted. Integrating VR with portable sensor technologies may further enhance the accuracy and accessibility of balance assessments.
Conclusion
In conclusion, VR-based assessments and interventions show promise as effective tools for evaluating and improving balance in individuals with DM. With its interactive and engaging nature, VR offers precise, innovative solutions for rehabilitation. Ongoing research will be essential to further validate its benefits and support its integration into routine clinical practice.
Supplemental Material
sj-docx-1-dst-10.1177_19322968251375370 – Supplemental material for Virtual Reality for Balance in Individuals With Diabetes: A Systematic Review of Assessment and Intervention Strategies
Supplemental material, sj-docx-1-dst-10.1177_19322968251375370 for Virtual Reality for Balance in Individuals With Diabetes: A Systematic Review of Assessment and Intervention Strategies by Kai Cheng, Fatimah Alkhameys, Hannes Devos, Patricia Kluding, John Miles and Chun-Kai Huang in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
CG, control group; COM, center of mass; COP, center of pressure; DM, diabetes mellitus; DPN, diabetic peripheral neuropathy; HbA1c, hemoglobin A1c; HC, healthy control; HMD, head-mounted display; IG, intervention group; RCT, randomized control trial; VR, virtual reality.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the KUMC School of Health Professions PhD Student Research Award (Cheng).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.