
Abstract
Reducing the environmental footprint of medical devices used by people with diabetes remains a challenge within the constraints of current regulatory frameworks. These frameworks, which rightly prioritize patient safety, sterility, and traceability, introduce substantial scientific, operational, and legal barriers to sustainable innovation. Efforts to integrate recycled or biodegradable materials, minimize packaging, or redesign products are often impeded by the complexity of revalidation processes, extensive documentation requirements, and a general lack of regulatory precedent. This commentary examines how such structural constraints hinder progress toward sustainable device design, despite mounting evidence of the environmental toll of single-use technologies. It advocates for a strategic shift toward “Design for Sustainability.” Coordinated systemic incentives and regulatory evolution are essential to align sustainability objectives with prevailing safety and quality imperatives.
Introduction
There is growing recognition that the usage of medical devices for the treatment of patients with diabetes (PwD) generates a lot of waste.1 -4 However, reducing waste in the medical device industry is a complex and challenging task, particularly when operating under the stringent requirements of ISO 13485 and the European Union Medical Device Regulation (MDR) 2017/745. 5 Below is a detailed scientific and regulatory description explaining why this is the case and why we believe that an “Eco Design” of medical devices is the only practical way ahead.
Regulatory Requirements Prioritize Patient Safety Over Environmental Considerations
The International Organization for Standardization (ISO) 13485 is an international standard that outlines the requirements for a quality management system (QMS) specific to the medical device industry. 6 Similarly, the MDR is a regulation that enforces stringent controls over medical devices entering the European market, with a strong emphasis on traceability, risk management, and clinical evidence. The manufacturer of medical products has to follow these regulatory frameworks; otherwise, they neither get a CE mark nor Food and Drug Administration (FDA) approval for their products.
As long as patient safety is at all times the highest standard, all other aspects have to follow. If we want to mitigate any risk of harm to PwD, the problem is that this might lead to the use of materials and processes that may be less environmentally friendly but more reliable and sterile. This prioritization on patient safety and product performance comes at the expense of environmental or sustainability concerns, as we will outline below. For example, with recycled materials, this consistent quality cannot be guaranteed. Medical-grade plastic has significantly higher costs compared to commercial materials, due to the strict maintenance of material quality and purity! When these regulations were initiated, the focus/interest was not so much on environmental aspects as they are today; 7 however, to adjust “outdated” regulations to up-to-date requirements is a challenging task. Nevertheless, there is a strong political will to do so, at least in Europe.
Sterility and Single-Use Mandates Generate Significant Waste
Many medical devices are single-use by design, especially those that are invasive or come into contact with body fluids. The MDR and ISO 13485 enforce rigorous sterility requirements that make reprocessing and reuse either highly regulated or impractical:
ISO 13485 Clause 7.5.5 emphasizes the need to validate sterile barrier systems and maintain sterility throughout product life.
MDR Annex I, Chapter II outlines general safety and performance requirements (GSPRs), mandating sterility assurance for devices where applicable.
These standards effectively mandate the disposal of large volumes of materials, including plastics, packaging, and electronics, after a single use. 8 The manufacturer has to perform a biocompatibility test for all materials used. In case any of the materials used for the product or its packaging are changed, they have to do it again. A prerequisite is that the product material is absolutely homogeneous, and this is not possible with recycled materials.
The manufacturer also must do a sterility validation and afterwards a transport validation. With every production step and different production batches, they have to ensure that the performance and sterility of the device are not negatively influenced. So changing a given material in a medical device into a probably more biocompatible one is a highly complex undertaking that takes years and is associated with high costs. 9
Traceability and Documentation Requirements Add Complexity
The MDR imposes extensive traceability requirements, especially through the introduction of the UDI (Unique Device Identification) system. Each device component must be traceable through its entire lifecycle, necessitating robust labeling, documentation, and tracking systems. This requirement introduces additional packaging and labeling waste, often in materials that cannot be easily recycled due to their inclusion of printed electronics, adhesives, or biocidal coatings. Furthermore, efforts to reduce material use or modify packaging must go through design change control, including:
Design validation (ISO 13485 Clause 7.3.6).
Risk management (ISO 14971,10,11 integrated by reference in ISO 13485 and MDR).
Regulatory submissions for significant changes (MDR Annex II and III).
For example, a medical device manufacturer must be able to tell from which bag/batch the plastic product came before injection molding of this plastic piece. In other words, the whole supply chain must be 100% under control at all times. These efforts are one explanation why medical devices are so expensive.
Design Control and Change Management Barriers
In such a regulatory environment, implementing environmentally friendly design changes (eg, using biodegradable plastics or reducing material volume) is not straightforward. Under ISO 13485 and MDR, any design change—especially one affecting materials, manufacturing processes, or packaging—must be:
Fully documented and justified.
Assessed for risk (via ISO 14971).
Validated through clinical or performance testing.
Notified to Notified Bodies if classified as a significant change under MDR.
It is obvious that to change existing products, with established production lines and regulatory approval, is quite demanding. Changing, eg, the design or material of a disposable insulin pen, with an up-and-running production line with a capacity of 100 million pens per year, would require doing the whole validation and verification again. Such products are manufactured in a clean room environment. So, any changes to a product are time-consuming, expensive, and high-risk, making manufacturers reluctant to pursue sustainability-driven changes unless mandated by regulation or incentivized by market demand. Nevertheless, to our understanding, the manufacturer sees the need for such activities. They are considering environmental aspects when designing new products. However, some elements can be changed relatively easily and fast, eg, getting rid of “Instructions for use” (IFUs) in x languages and allowing the users of the devices to download them with a barcode would be an easy step. 12 Also, to acknowledge that political structures can react to a changing situation, there is a clear interest in electronic IFUs in the European Union (EU). 13
Limited Availability of Approved Sustainable Materials
Medical device manufacturers are limited in the materials they can use. All materials must demonstrate biocompatibility (ISO 10993 series), stability (also toward sterilization), and compatibility with sterilization methods (eg, gamma, Ethylene oxide, and steam). 14 Biodegradable or recyclable materials often lack sufficient data or precedent in the medical domain, making regulatory approval difficult. Even if such materials exist, they may not perform reliably under clinical conditions or may degrade during the required shelf life. This results in a continued reliance on virgin polymers, engineered composites, and synthetic materials that are robust but not environmentally sustainable.
To our knowledge, at the moment, there is no medical-grade plastic material available for Class II medical devices that came out of the recycling process. However, the hope is that the manufacturer of such materials will react to the demand for “better” materials from an environmental point of view. In the longer run, materials might come to the market that fulfill more recent requirements.
Liability and Risk Aversion
The MDR has substantially increased the legal liability of medical device manufacturers. This includes tighter scrutiny over post-market surveillance, incident reporting, and clinical performance. Manufacturers are increasingly risk-averse, focusing more on regulatory compliance than on environmental innovation. Any failure attributed to a change intended to reduce waste, no matter how minor, can have severe business and legal consequences. This creates a strong disincentive to prioritize sustainability unless clear, risk-free pathways are available. The only way we see ahead is to change the view of the regulatory agencies in, eg, Europe, on this topic. In addition, manufacturers that are willing to invest in the development and production of products that use recycled materials should receive some kind of incentive.
Economic and Operational Constraints
While environmental sustainability may be a long-term cost-saving strategy, in the short term, it often introduces higher costs for:
Redesign and revalidation of products.
Supply chain adaptations.
New vendor qualification.
Regulatory submission and review.
In a highly competitive and regulated industry with tight margins, especially for lower-risk medical devices (Class I/IIa), these economic burdens—at least currently—often outweigh the perceived benefit of waste reduction initiatives. As indicated, there is a need for support by payers/regulatory agencies to manufacturers that are willing to go the extra mile and invest in the future/reduce the environmental burden. To be clear, this would require exclusivity or higher sales prices to compensate for the significant extra effort. The question is, who is willing to accept this?
Potential Ways Ahead: Toward More Sustainable Diabetes Devices
Despite the structural and regulatory barriers outlined above, meaningful opportunities exist to reduce the environmental impact of diabetes medical devices—if sustainability is considered from the very beginning of the design process. While ISO 13485 and the MDR impose strict controls around safety, traceability, and validation, they do not preclude innovation. Rather, they demand that environmental strategies be systematically planned and robustly justified.
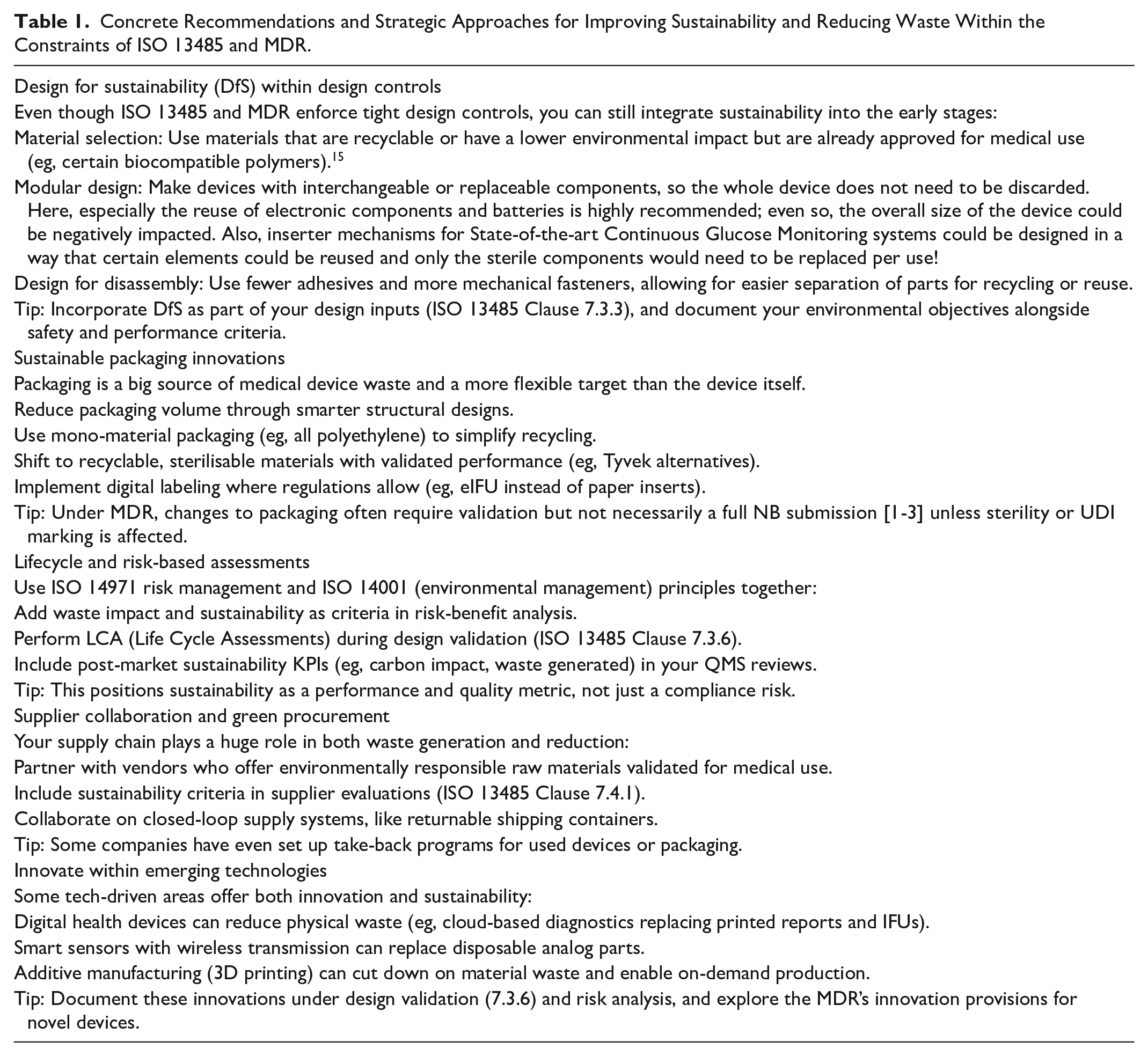
One such strategy is to embed Design for Sustainability (DfS) principles directly into the product lifecycle. Choosing materials that are both recyclable and already approved for medical use—such as certain biocompatible polymers—can help avoid revalidation hurdles while lowering environmental impact. Modular product architectures present another promising avenue. Instead of fully disposable devices, future systems could be composed of replaceable and reusable components. For instance, separating sterile, single-use elements from electronics, batteries, and mechanical parts would allow high-impact components to be retained and reused across multiple cycles. This is particularly relevant for patch pumps or inserters for continuous glucose monitoring (CGM) systems, where reusable applicator mechanisms could significantly reduce overall waste. Similarly, designing for disassembly—using mechanical fasteners rather than adhesives—can simplify the separation of materials for recycling or refurbishment, making end-of-life management more feasible.
Packaging, although often overlooked, represents another critical target. Many current device systems rely on multilayered, non-recyclable packaging to ensure sterility and traceability. However, switching to mono-material packaging, optimizing structural design to reduce bulk, and using sterilisable but recyclable alternatives can meaningfully reduce waste. Digital innovations also play a role: eg, the use of electronic Instructions for Use (eIFUs), where permitted, could eliminate the need for bulky multilingual paper inserts. While any change to packaging must be validated, not all will trigger full Notified Body submissions under the MDR—particularly if sterility and UDI markings remain unaffected.
To institutionalize these changes, environmental considerations should be integrated into risk and quality frameworks. By aligning ISO 14971 risk management with ISO 14001 environmental principles, manufacturers can elevate sustainability to a measurable performance metric. This may involve incorporating waste generation and carbon impact into risk-benefit analyses, conducting life cycle assessments (LCAs) during design validation, and setting environmental key performance indicators (KPIs) for post-market surveillance and QMS reviews. Such integration shifts sustainability from a peripheral concern to a central quality objective.
Sustainability must also extend into the supply chain. By partnering with vendors who provide environmentally responsible, validated materials—and by embedding sustainability criteria into supplier evaluations—manufacturers can drive systemic improvements beyond their own operations. Collaborative programs, such as returnable shipping containers or device take-back schemes, are already in place at some organizations and could be scaled across the industry.
Finally, technological innovation offers pathways to leapfrog current constraints. Digital health technologies, for instance, can replace physical components with cloud-based tools, reducing both material use and waste. Smart sensors with wireless data transmission eliminate the need for disposable analog accessories, while additive manufacturing (3D printing) enables low-waste, on-demand production of customized components. As these technologies evolve, they should be thoroughly documented within the design validation and risk assessment processes. The MDR’s provisions for novel technologies may provide regulatory flexibility for forward-thinking solutions that are both safe and environmentally sound.
Together, these strategies present a roadmap for reconciling sustainability with safety and regulatory compliance in diabetes device design (Table 1). While implementation will require concerted effort across engineering, manufacturing, regulatory affairs, and patient engagement, the potential for positive environmental impact is both real and urgently needed.
Concrete Recommendations and Strategic Approaches for Improving Sustainability and Reducing Waste Within the Constraints of ISO 13485 and MDR.
In addition to product design changes, behavioral and systemic shifts will be needed. Encouraging PwD to adopt reusable alternatives where appropriate, and providing sufficient education and support for their use, can create meaningful demand for environmentally conscious solutions. Although sustainability is not yet a primary factor in product selection for most PwD, there is a growing awareness of the environmental burden posed by disposable technologies. 3
Conclusion
The current regulatory landscape governing diabetes medical devices, anchored by ISO 13485 and the MDR, rightfully so, prioritizes patient safety, product sterility, and traceability. These are essential pillars of quality and clinical reliability, but they inadvertently limit flexibility for innovation in sustainability. The complex requirements around biocompatibility testing, sterility validation, and supply chain traceability create high entry barriers for the use of recycled or biodegradable materials. Likewise, any modification to approved designs is subject to extensive revalidation, which deters even well-intentioned efforts to reduce waste.
Nevertheless, growing environmental awareness, technological advancement, and political momentum, particularly in Europe, are beginning to shift the conversation. As this paper outlines, the path forward is not to relax safety standards but to expand the design framework to include environmental performance as a co-equal design objective. By embedding sustainability into design controls, material selection, risk management, and supplier collaboration, manufacturers can begin to make incremental but meaningful improvements. Approaches such as modular design, digital IFUs, recyclable packaging, and closed-loop supply systems are already feasible within existing regulatory structures.
Ultimately, advancing sustainability in diabetes technology will require coordinated action. Regulatory bodies must evolve to explicitly recognize environmental impact as part of product evaluation. Manufacturers need incentives to innovate responsibly while still meeting safety and performance benchmarks. Patients and health care systems also play a role, as greater awareness and preference for sustainable options can help shift market demand.
If pursued with urgency and collaboration, the integration of sustainability into the regulated development of diabetes devices is not only possible—it is essential. Only by addressing environmental responsibility with the same rigor as clinical safety can the medical device industry fully respond to the pressing challenges of our time.
Footnotes
Abbreviations
DfS, design for sustainability; GSPRs, general safety and performance requirements; IFUs, instructions for use; MDR, medical device regulation (EU); PwD, patients with diabetes; QMS, quality management system; UDI, unique device identification.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SH is an employee of Diabetes Center Berne. DB is an employee of Diabetes Center Berne and a Member of the Investment Committee of the Diabetes Venture Fund at Serpentine Ventures. LH is a shareholder of the Profil Institut für Stoffwechselforschung GmbH, Neuss, Germany; Science Consulting in Diabetes GmbH, Düsseldorf, Germany; and diateam GmbH, Bad Mergentheim, Germany. LH is a consultant for several companies that are developing novel diagnostic and therapeutic options for diabetes treatment.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.