
Abstract
Continuous glucose monitors (CGMs) have increasingly been used in ambulatory and inpatient or hospital settings to improve glycemic outcomes for people with diabetes. Given their capacity to aid individuals in avoiding hypo- and hyperglycemia, they may also be useful when transitioning from hospital to home by reducing rates of hospital readmissions and emergency department visits. Several types of barriers presently exist that make the deployment of CGMs at the time of hospital discharge problematic, including (1) regulatory, (2) behavioral, (3) logistical, (4) technical, (5) staffing, and (6) systemic issues. In this commentary, we review the literature, discuss these barriers, and propose possible solutions to facilitate the use of CGMs in people with diabetes at the time of hospital discharge.
Introduction
Diabetes mellitus is becoming increasingly prevalent in the United States and represents a huge economic burden. 1 Readmission to the hospital within 30 days of discharge (30-day readmission) is a standard metric of quality of care. High 30-day readmission rates are associated with increased mortality 2 as well as financial penalties for hospitals under the Centers for Medicare and Medicaid Services’ Hospital Readmissions Reduction Program. 3 Therefore, it is of interest to all stakeholders involved to reduce 30-day readmission rates as much as possible.
In the United States, people with diabetes accounted for 30% of all hospital admissions in 2018. 4 Poor glycemic control in people with diabetes can lead to hospitalizations because of acute complications such as hypo- or hyperglycemia and diabetic ketoacidosis. 5 Furthermore, hyperglycemia can increase the risk of post-op complications. 6 People with diabetes also experience a disproportionate share of hospital readmissions, with a rate of 16.0% to 20.4%, 7 compared to 14% for people without diabetes. 8
Because checking fingerstick capillary blood glucose can be painful and cumbersome and often occurs with limited frequency, continuous glucose monitors (CGMs) have become widely used in ambulatory settings to identify glucose trends, reduce hypo- and hyperglycemia, and improve glycemic outcomes. 9 CGMs also allow for passive overnight monitoring of glucose levels 10 to detect nighttime hypo- and hyperglycemic events. Umpierrez et al 11 found that 29% of recently discharged people with diabetes experienced a hypoglycemic event within 12 weeks based on self-reported blood glucose levels. Moreover, up to 50% of hypoglycemic events can be asymptomatic.12,13 CGMs have emerged as a powerful technological tool for clinicians to identify trends and predict impending out-of-range glucose values to allow people with diabetes the opportunity to take action to prevent low and high glucose levels. Retrospective studies have shown that CGMs can be useful tools to prevent hospitalizations of people with diabetes irrespective of whether they were or were not recently discharged from a hospital.5,14,15
Given that CGMs can be effective tools to reduce acute diabetes complications, they have the potential to improve glycemic outcomes in recently discharged people with diabetes and reduce 30-day readmission rates in addition to preventing emergency department visits. Fructosamine concentrations as a marker of glycemic control have been linked to readmission following hip surgery. 16 It is logical that abnormal glycemia can be best assessed through the use of a CGM to predict and then take action to prevent hospital readmissions. However, to date, there has been very limited research reporting the impact of CGM deployment at the time of hospital discharge on 30-day readmission rates for people with diabetes.
Literature Review
We performed a literature search in PubMed for articles that discussed the impact of CGMs upon hospital discharge on readmission rates. Papers to be included must have met the following inclusion criteria:
Does the paper involve the use of a CGM?
Is the person with diabetes using a CGM upon being discharged from a hospital?
Are readmission rates measured?
We excluded articles that were not referenced in PubMed. Abstracts published without the full paper available were not considered unless they were published in the 2023 American Diabetes Association’s 83rd Scientific Session abstracts book.
We first searched PubMed using the search phrase “((continuous glucose monitor) OR (cgm)) AND (hospital) AND ((discharge) OR (readmission))” on July 26, 2023. We then screened the 92 resulting articles based on the inclusion criteria, yielding one relevant article. We additionally searched ADA 83rd Scientific Sessions Abstracts 17 using the same search term on July 26, 2023. The 26 search results did not yield any relevant abstracts.
The one relevant original article was an open-label study performed by Depczynski and Poynten, in which 2 of 19 enrolled people with diabetes, all of whom received a CGM upon hospital discharge, were readmitted within 30 days. 18 While their 30-day readmission rate of 10.5% is lower than the national average of 14%, 8 the study suffers from poor recruitment (19 enrolled out of 101 eligible participants) and a small sample size. 18 The enrolled participants had a median hemoglobin A1c of 10.9% at enrollment and 8.0% three months later. The article did not present the clinical characteristics of the 82 nonenrolled participants. Of these 82 nonenrolled participants, 31 stated that learning a new task at discharge was overwhelming or too stressful.
We further reviewed the 19 articles cited by Depczynski and Poynten and the one article listed in PubMed as citing Depczynski and Poynten. 18 We found none of these articles to be relevant. In addition, we found three results on Google Scholar that cited Depczynski and Poynten. 18 Of these three results, two were excluded for not being listed in PubMed, and the remaining one was a duplicate found via PubMed.
Based on our literature search of 138 articles and abstracts either in PubMed or published in the 83rd Scientific Sessions Abstracts, only one article was found to discuss the potential of lowering readmission rates based on providing a CGM to a person with diabetes upon hospital discharge. This lack of relevant articles indicates that more research is needed in this area to clearly demonstrate the efficacy of CGMs in reducing 30-day readmission rates in this setting. Figure 1 is a PRISMA diagram of the literature search that was performed. Based on the results of Depczynski’s study, 18 it is unclear how to extrapolate this data to other hospitals and health care systems about whether CGMs can be used to improve transition of care from the hospital to the individual’s home.
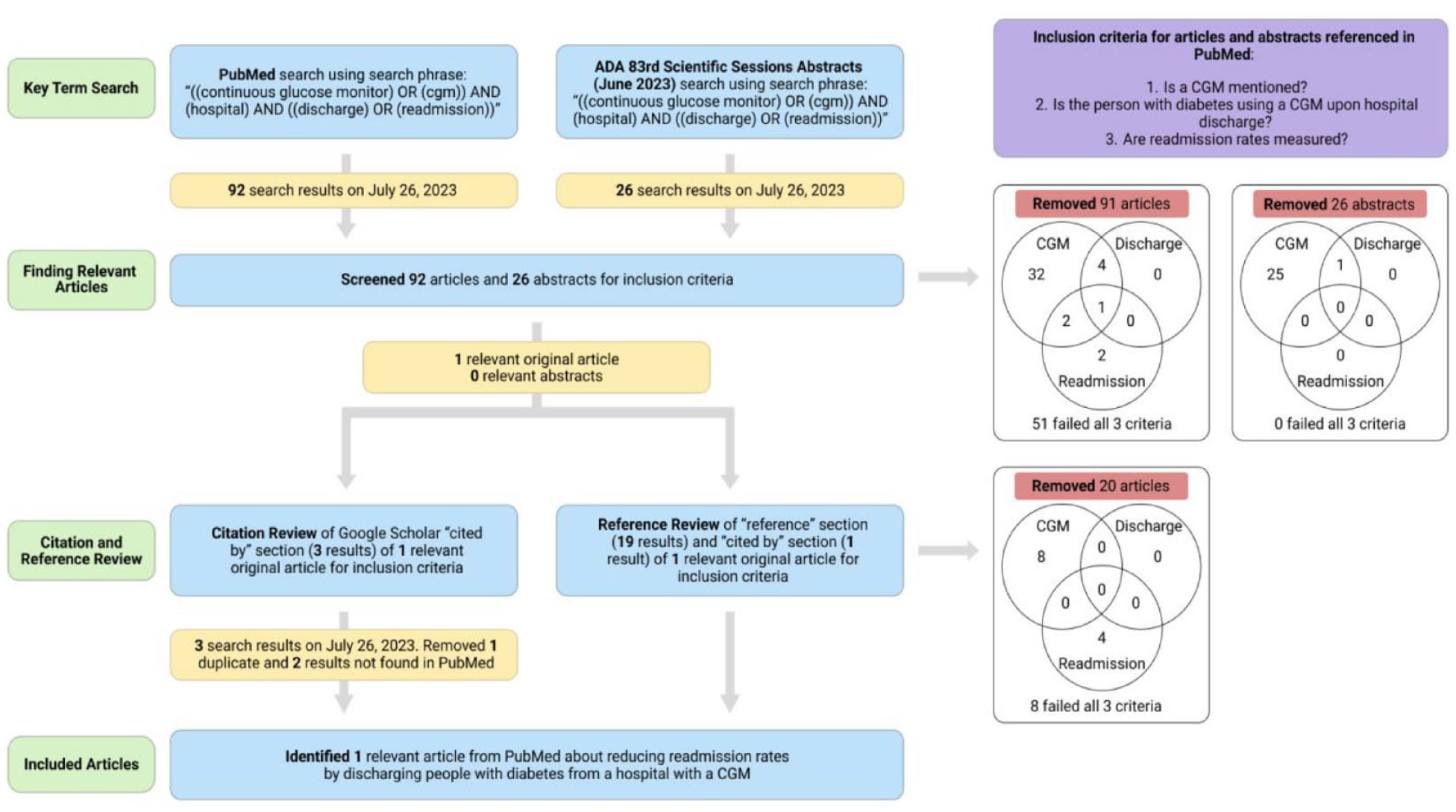
A PRISMA diagram describing the literature search that was performed. 19
Barriers
Many challenges for people with diabetes and health care professionals (HCPs) limit the implementation of CGMs upon hospital discharge. Several common barriers are outlined in Figure 2. These obstacles must be addressed if people with diabetes are to receive a CGM and be educated on its appropriate use before leaving the hospital, particularly if they have not used a CGM before.
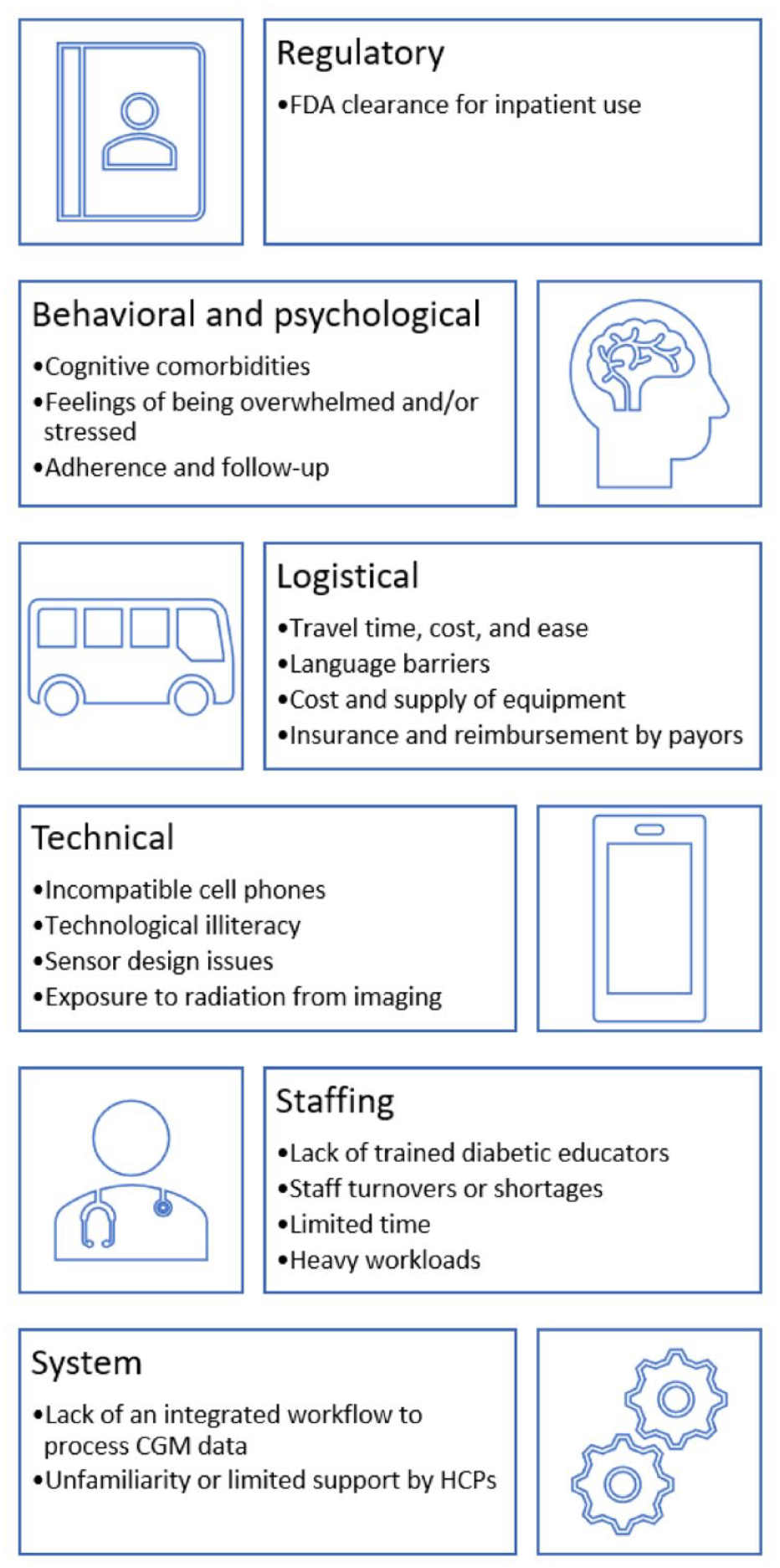
Barriers to CGM use for people with diabetes after hospital discharge.
Regulatory
A major barrier is that CGMs are currently not cleared by the U.S. Food and Drug Administration (FDA) for inpatient use. During the COVID-19 pandemic, the FDA announced an enforcement discretion to allow expanded use of some remote monitoring devices, 20 including CGMs, to monitor individuals while reducing HCP exposure. 21 During this time, the use of CGMs in hospital settings became more widespread. 9 This guidance remains in effect until November 7, 2023. 22 Meanwhile, the development of a hospital-dedicated product is ongoing. Dexcom was recently granted Breakthrough Device Designation by the FDA, which allows for expedited review. 23
Approval and adoption of this technology may influence the impact of CGM implementation upon discharge. If CGMs cannot be used in the hospital to assess for hypo- and hyperglycemia and to dose insulin, then it is less likely that HCPs will be accustomed to implementation and use of this technology. Additionally, because CGMs are not cleared by the FDA for inpatient use, a hospitalized person with diabetes who has never used a CGM prior to admission misses an opportunity to learn how to interpret CGM data while hospitalized. Knowledge from inpatient education can empower the individual to successfully use CGM data for self-management upon discharge.
Behavioral
People with diabetes recently discharged from a hospital may encounter difficulties in learning to use CGMs, particularly if they are unfamiliar with the technology. Although CGMs can be relatively easy for many outpatients to use, this might not be the case for people who were recently acutely ill or recently discharged from a hospital. When burdened by concerns such as new diagnoses, medications, and recovery, they may find CGMs challenging to use.
People with diabetes may also be facing cognitive 18 and behavioral health 24 comorbidities or be stressed and overwhelmed by their hospital stay. 18 These factors, combined with skepticism, distrust, or unfamiliarity toward the new technology, can lead to CGMs being unwelcomed.
Furthermore, the discharge process in a hospital can be complicated, with many instructions for new treatments. Any education about CGMs and diabetes management can be difficult for people with diabetes to master and remember. This is further complicated by any pain and medications that may cause forgetfulness, sleepiness, or irritation. As a result, people with diabetes may not follow the recommended self-care behaviors for CGMs and could use them ineffectively.
Logistical
People with diabetes face a variety of barriers in accessing care and medical equipment that prevent them from receiving and wearing CGMs. The number of hospitals in their area, the cost of travel to appointments in terms of direct costs, lost time, and lost wages, and language barriers between the individual and their HCP may make access to care and diabetes education challenging.
The supply and cost of CGM equipment can also be a barrier to access. In 2017, the Centers for Medicare & Medicaid Services issued a ruling, expanded in 2021, allowing CGMs to be classified as Durable Medical Equipment. 25 However, applying for coverage of CGMs with insurance can still be difficult. Hospital HCPs often do not have the administrative resources to determine a preferred brand, assess coverage requirements, and submit necessary paperwork for prior authorization. Additionally, some payors require an outpatient visit for documentation of CGM needs. 26 Furthermore, CGMs may not be approved by hospital pharmacy and therapeutics committees or available in hospital pharmacies.
Technical
There are also issues with the CGMs themselves that can make them difficult to use for recently discharged people with diabetes. Many of them require smartphone applications; however, individuals may encounter difficulties downloading these applications or have incompatible phones. The different components of CGMs also may be challenging for individuals who are less technologically or numerically literate.
Problems with the sensor design itself can also lead to discontinued use. Skin irritation and allergic reactions as well as poor adhesion to the skin have been reported because of CGM use. If the CGM sensor falls off, then it will need to be replaced, further increasing the burden for people with diabetes. People with diabetes who are on anticoagulant therapy, commonly used in the acute care setting, or who have thrombocytopenia may experience bleeding at the site. 27 Fear of bleeding and other side effects as a result of using a CGM may discourage use among people with diabetes. An additional technical barrier is potential CGM exposure to radiation from X-rays, computed tomography scans, and magnetic resonance imaging. If such imaging is needed after discharge, then the person with diabetes will have to remove their CGM and might elect to not replace it. CGM data can also be difficult to learn to interpret. While these are concerns for all CGM users, they are particularly pertinent for individuals who are recovering from acute illness and require ongoing support and follow-up with HCPs experienced with CGM use.
Staffing
Implementing CGMs prior to hospital discharge requires trained diabetes care and education specialists (DCES) to teach people with diabetes how to use their CGMs and assuage any worries or skepticism. However, there are only about 20 000 DCES in the United States, 28 which means they are often scarce in hospital settings, and many hospitals do not have a dedicated staff member for diabetes education. According to the Centers for Disease Control and Prevention, in 2020, 2158 sites were delivering diabetes education and support services across the United States. 29 In these cases, most training is done by nurses, dieticians, and pharmacists who may not be highly familiar with CGM technology. In a multicenter study by Madhun et al, 30 only 28% of surveyed respondents including inpatient hospitalists, advanced practice providers, and primary care physicians in the United States were familiar with institutional CGM policies, and only 43.8% were reviewing CGM data to guide insulin dosing. Furthermore, DCES face limited time and already heavy workloads, which limits their time to initiate CGMs in addition to other responsibilities.
System
Finally, there is a lack of an integrated system or workflow to handle and process CGM data. A comprehensive review of glucose data is important in order to take advantage of the large influx of data that a CGM can provide. CGM data needs to be transferred from the individual’s smartphone or CGM receiver/reader and made available to the HCP, typically via upload to cloud-based software systems. For the CGM data to be useful within the 30-day readmission period, an HCP needs to review the data usually at 14-day intervals after discharge and adjust treatments as needed. The HCP, whether they are an endocrine specialty HCP or a primary care provider (PCP), may not be trained to interpret and make treatment recommendations utilizing CGM data. Many HCPs are also not aware that they are eligible to receive reimbursement for their time spent reviewing CGM data. In the case of an individual who has recently been acutely ill, however, adjusting medications quickly is extremely important, especially in preventing readmission.
Strategies for Overcoming Barriers
Behavioral
Different inpatient education techniques may help promote CGM use among recently discharged people with diabetes. Transitional care programs for postdischarge individuals combined with scheduled follow-up appointments may improve the performance of self-care. Additionally, offering virtual visits and remote support, involving family and caretakers, or incorporating CGMs into general diabetes education could better familiarize people with diabetes with this technology. Empowering individuals to self-manage diabetes via data-driven shared decision-making will also serve to motivate individuals to try CGMs and foster long-term adoption of this valuable tool.
Logistical
Many of the logistical barriers that were discussed relate to the social determinants of health and are therefore challenging to overcome. However, language barriers can more easily be addressed by providing accessible, high-quality educational materials in many different languages. These materials, describing the use of the CGM, downloading and interpreting CGM data, and troubleshooting methods, could be of great use both to people with diabetes as well as their family members and caregivers. Care navigators and transition coaches may also be used to address logistical barriers by providing additional support in the transition between hospital and home. 31
Technical
Legislation would make it possible for CGM sensors and readers to be readily available and at low or no cost. While most Americans do own a smartphone, only 61% of the elderly and 76% of adults with household income less than $30 000 own a smartphone, as opposed to 96% of adults ages 18 to 29 and 97% of adults with household income $100 000 or more.32,33 As smartphones become more widely used, it will become easier for the entire population to use CGMs.
Staffing
Staff training programs such as Diabetes Champion Programs can be implemented to educate nurses, dieticians, and pharmacists to become service-line based diabetes specialists. 34 Additionally, some degree of diabetes education should be provided by these diabetes specialists when people with diabetes receive their prescribed CGM in the hospital at the time of or soon after discharge. The development of online curriculums, availability of patient training resources, and remote training also has the potential to rapidly increase the number of trained DCES.
System
More training will be needed for nonspecialist HCPs and PCPs to download, review, and interpret CGM data, as endocrinology clinics are not able to take on this burden alone. Projects like the Integration of Continuous Glucose Monitoring Data into the Electronic Health Record (iCoDE) Standard Project 35 will help to ensure that CGM data is presented in a useful way to people with diabetes and their HCPs for treatment decisions to be based on.
Future Directions
To expand the current state of CGM deployment for people with diabetes at hospital discharge, we present the following calls to action:
Additional research needs to be conducted to describe the outcomes and readmission rates as well as a cost benefit analysis for hospitalized people with diabetes who are issued a CGM at the time of discharge.
Once inpatient CGM use is cleared by the FDA, it will need to be used more in the hospital setting. At this time, additional technical barriers will need to be addressed, including CGM exposure to radiation from X-rays, computed tomography scans, and magnetic resonance imaging. However, if people with diabetes start using a CGM while in the hospital and see the added value to their care, then they may be more inclined to continue its use after discharge at home for self-management.
Education regarding CGM use should be started during hospitalization, rather than waiting until an outpatient visit. When individuals use a CGM in the hospital, they will be better equipped to continue use after discharge. This type of expanded use depends not only on FDA clearance but on coverage by payors, which needs to be established for inpatient deployment and use.
Hospitals should develop highly structured programs to integrate inpatient and outpatient care to keep people with diabetes from being readmitted after discharge, irrespective of their hospital discharge diagnosis. Use of a CGM by a recently discharged person, particularly those at high risk for readmission, along with specific criteria to determine which individuals may derive the most benefit, may be incorporated into these programs. Existing remote patient monitoring programs using blood glucose monitoring can provide examples of the costs and benefits of implementing similar programs with CGMs. 36
CGM manufacturers will need to create multi-media educational programs for recently discharged people with diabetes so that those using a CGM for the first time will have readily available resources including resources for individuals with low literacy for education and support.
New CGM metrics will need to be adopted to help clinicians identify people with diabetes who are not meeting glycemic goals while using a CGM during the transition of care from hospital to home. The Glycemia Risk Index 37 is one such potential new metric that could be used for monitoring recently discharged individuals.
Hospital systems must begin to implement the integration of CGM data into the electronic health record (EHR). 35 EHR connectivity and access will allow CGM data to be easily accessed by clinicians and guide insulin dosing decisions.
Continuous glucose monitors have the potential to be a powerful tool for people with diabetes to improve glycemic outcomes and reduce risk of diabetes complications and hospital readmissions. Although there are barriers to providing a CGM at hospital discharge, possible solutions should be tested to potentially improve the quality of diabetes care and prevent readmission in people with diabetes.
Footnotes
Abbreviations
CGM, continuous glucose monitor; DCES, diabetes care and education specialists; EHR, electronic health record; FDA, U.S. Food and Drug Administration; HCP, health care professional; PCP, primary care provider.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JJS is a consultant for Lifescan Diabetes Institute. CJL has received research support by the NIDDK and Helmsley Foundation and industry support paid to the Icahn School of Medicine at Mount Sinai from Abbott Diabetes, Dexcom, Insulet, Novo Nordisk, Senseonics, and Tandem. CJL has received consulting fees from Eli-Lilly, and Dexcom outside of this work. GEU is partly supported by research grants from National Institutes of Health (NIH/NATS UL 3UL1TR002378-05S2) from the Clinical and Translational Science Award program, and from National Institutes of Health and National Center for Research Resources (NIH/NIDDK 2P30DK111024-06). GEU has received research support (to Emory University) from Abbott, Bayer, Dexcom and Sanofi. DCK is a consultant for Better Therapeutics, EOFlow, Integrity, Lifecare, Nevro, Novo, Rockley Photonics, and Thirdwayv. TT, REA, RL, and IN have nothing relevant to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.