
Abstract
Background:
The use of fructosamine to assess the glycemic control represents a new step in diagnostics, and it has been accompanied by the active scientific discussion in recent years. That is why the purpose of this work is to study the average level of fructosamine in apparently healthy individuals and individuals with diabetes mellitus (DM), as well as the possibility to use it when evaluating the effectiveness of inpatient treatment of patients with hyperglycemia on the seven to ten days of hospitalization.
Methods:
This research work was carried out in Alma-Ata, Republic of Kazakhstan, based on the endocrinology department in the period from 2020 to 2022. The work consists of a retrospective analysis of previously examined patients and a prospective stage. The statistical evaluation was carried out with the calculation of reliability coefficient, confidence interval, and criteria for testing for normality. The level of fructosamine in healthy individuals in the corresponding region was analyzed in this article for the first time, and the correlation between this indicator and the level of glycated hemoglobin was found.
Results:
The effectiveness of treatment of the Type 2 DM (according to the treatment protocol) has also been studied in stationary conditions for the seven to ten days, which makes it possible to judge the effectiveness of the prescribed therapy.
Conclusions:
These results will allow identifying the irrationality of the prescribed therapy at an early stage, which is especially important for the correct management of patients with this pathology, and minimizing the possible complications.
Keywords
Introduction
Diabetes mellitus (DM) is a complex, chronic disease that is a serious medical problem throughout the world, and it has a significant impact on life quality and expectancy, but at the same time, it significantly increases health care costs. Diabetes affects the person’s functionality, increases cardiovascular risk and premature mortality. Amiel et al 1 raise concerns in their work regarding the fact that more than one-third of diabetes-related deaths occur in young people (under 60). The authors also emphasize that rapid economic development and urbanization of countries have led to an increase in the burden of diabetes, and the factors, such as unhealthy diets and sedentary lifestyles, are the main factors in a tendency to gain weight and increase in fasting plasma glucose levels. At the same time, the economic aspect of the disease has been noted: the cost of treating a patient with DM is at least three times higher than the average health care costs, but in the presence of disease complications, it generally increases up to 9.4 times.
If to speak about the prevalence, then according to the authors’ assessments of the publication “Epidemiology of type 2 diabetes—global burden of disease and forecasted trends,” 2 around 465 million people worldwide suffer from the Type 2 DM, which corresponds to 6.28% of the world population. More than 1 million deaths were associated with this disease in 2017, and this fact put DM in ninth place among the leading causes of death. In this article, these numbers were compared in dynamics (eg, compared with 1990), and it was found an alarming increase, because DM was ranked eighteenth at that time among mortality. It is also noted that DM epidemiology has a tendency among the countries in the socioeconomic paradigm: Western Europe has significantly higher prevalence rates that continue to rise despite the public health measures, and the growth rate does not seem to be slowing down. Thus, the average rate around the world amounted to 6059 cases per 100 000, while the highest rates were recorded in the Netherlands and Sweden (11 344 and 10448/100 000, respectively). However, the lowest rates were established in Asian countries (India—4770/100 000). Despite the great interest in research of this disease, an increase in the DM prevalence indicates insufficient primary prevention and the effectiveness of treatment schemes.
In the Republic of Kazakhstan (RK), enough attention is also paid to this chronic disease. According to the data of the Ministry of Health of the Republic of Kazakhstan, the number of patients with diabetes has increased by 3.5 times over 15 years. At the beginning of 2021, there were 382 000 people at the dispensary, and among them: 30 000 with Type 1 DM, and another 352 000 patients with Type 2 DM. At the same time, more than 2.5 million cases of diseases have been identified with the help of screening procedures among the adult population, where about 60 000 cases have turned out to be the DM. The increase in the number of such patients, including the above-mentioned factors, also indicates an improvement in the early detection and diagnosis of disease. 3 Currently, the DM diagnosis and its management are based on two historical tests: plasma (or capillary) glucose, and determination of glycated hemoglobin (HbA1c). However, these studies are not reliable in all cases. Blood glucose levels are very sensitive to a number of conditions, including recent food intake, acute stress, and daily fluctuations, medications that affect glucose metabolism (corticosteroids, fibrates, cyclosporins, beta-blockers, diuretics, and others). With regard to HbA1c, the generally recognized disadvantages include lower diagnostic rates in pregnant women, the elderly, and patients with iron deficiency anemia. 4
In recent publications, particular attention has been paid to the use of serum fructosamine. Thus, it may be applicable for assessing glycemic control. The latest standards of medical care in diabetes published by the American Diabetes Association (ADA) emphasize that early diagnosis and monitoring are critical to prevent or delay the onset of acute complications and reduce the risk of long-term complications of diabetes. While HbA1c reflects the glycemic control over the previous 6 to 12 weeks, fructosamine reflects the glycemic control over the previous one to three weeks. 5 However, at the same time, it should be noted that there are no scientific works on the study of fructosamine as a marker of control in diabetes treatment. In addition, the correlation between its level and the level of HbA1c has not been fully studied, and this is especially important in those clinical situations when it is necessary to analyze the result after a short course of treatment or a change in regimen. Considering the data described above, the study of fructosamine may be useful for detecting impaired blood glucose control before any surgical intervention, as well as for monitoring people with diabetes with a poorly controlled course of the disease.
That is why the purpose of this work has become the investigation of the average level of fructosamine in apparently healthy individuals and individuals with DM, as well as the possibility of its use in assessing the effectiveness of inpatient treatment of patients with hyperglycemia on the seven to ten days of hospitalization.
Materials and Methods
This randomized controlled research was carried out in 2020 to 2022 based on the secondary health care institutions in Almaty, Kazakhstan (endocrinology department of the city clinics), which was conducted in two stages. At the first retrospective stage, it was analyzed the data of the patient’s medical documentation, and two groups were formed: Group I consisted of 80 practically healthy people without chronic and acute diseases at the time of study (including DM) and Group II consisted of 95 participants with the Type 2 DM, moderate severity, stage of decompensation. The level of serum glucose, fructosamine, and HbA1c were determined in both groups.
Diabetes Mellitus was diagnosed according to the criteria of the updated recommendations (2020) of the ADA, namely, the “Standards of Medical Care for Diabetes”: a fasting blood glucose level of more than 7.0 mmol/L (the absence of food intake is defined in fasting state for at least eight hours), or the 2-hour glucose higher than 11.1 mmol/L during a glucose tolerance test (while using a load of 75 g glucose), or the HbA1c level higher than 6.5% (48 mmol/mol), or the classic symptoms of hyperglycemia or hyperglycemic coma, with an occasional measurement of plasma glucose higher than 11.1 mmol/l. 6 Type 2 DM refers to the progressive loss of adequate insulin secretion by pancreatic B cells, often in the presence of insulin resistance. Exclusion criteria are as follow:
Chronic kidney disease (glomerular filtration rate less than 60 ml/min);
Uncontrolled arterial hypertension;
Acute complications from the cardiovascular system at the time of the study;
Proliferative retinopathy;
Hypoalbuminuria;
Severe anemia (hemoglobin below 70 g/L).
At the second prospective stage of scientific work, it was analyzed the indicators of 34 patients after the seven to ten days of inpatient treatment, such as fasting blood glucose, HbA1c, and fructosamine. Treatment was carried out in accordance with the protocol adopted in the RK. 7 In a hospital setting, patients usually received a combination therapy, which included insulin, metformin, drugs from the group of receptors SGLT2 inhibitors. Before being included in the study, all patients were explained in detail about the goals and objectives of scientific work, and written voluntary consent to participate was obtained. The design of work and its safety corresponded to the Declaration of Helsinki 8 of the World Medical Association. Laboratory testing: determination of fructosamine was carried out in the INVITRO laboratory. For its determination in the blood serum, it was used a colorimetric method (nitroblue tetrazolium). Thirty minutes before the blood test, it is necessary to exclude smoking, physical activity and emotional stress. The range of 170 to 285 µmol/L was chosen for the test reference values.
To determine the level of HbA1c, the whole blood (with ethylenediaminetetraacetic acid—EDTA) was examined by means of capillary electrophoresis (NGSP [National Glycohemoglobin Standardization Program] certified method). A blood test was also conducted on the empty stomach. At the same time, the authors considered that pathologies, such as sickle cell anemia, pregnancy (second and third trimesters, and the postpartum period), glucose-6-phosphate dehydrogenase deficiency, HIV (human immunodeficiency viruses) infection, hemodialysis, recent blood loss or blood transfusion, erythropoietin therapy, affect the erroneous indicator value, therefore, cannot be used in such patients. Statistical data analysis was conducted using the SPSS 13.0 statistical software package for Windows and MS Excel analysis package. To assess the statistical significance of the difference between comparable groups, the Student’s t-test was used, in which the critical significance was considered to be < 0.05. Descriptive statistics and normality test criteria will be used. In addition, to determine the hypothesis, it was carried out the calculation of odds ratio (OR), their confidence intervals (CIs) at a level of at least 95% and the reliability criterion P < .05.
In Group I, the average age of patients was 31 ± 7.5 years. There were the following differences in the gender ratio: men made up 36% (29 people) and women—64% (51 participants), which is a statistically significant difference (P < .05). At the same time, the fructosamine index for men was 225 ± 12.6 µmol/L, and for women—221 kkmol/L, without a significant difference between them (P > .05). According to the age range, patients were divided into the group according to the WHO (World Health Organization) classification: under ten years old—27.5% (22 people), from 10 to 18 years old—3.8% (three people), young age—the largest number (40%, 32 people), average age—15% (12 people), elderly—12.5% (ten people), and senile age—only one person. Along with this, the authors analyzed the level of fructosamine in these groups, which is shown in Figure 1. As it can be seen, the highest rate was observed in minors over ten years old (226 ± 17.5 µmol/L), slightly lower rate was observed in patients aged 45 to 59 years—212 ± 16.9 µmol/L, and the lowest rate was observed in patients aged 60 to 74 years—212 ± 13.6 µmol/L. Nevertheless, at the same time, there is no significant difference between these indicators.
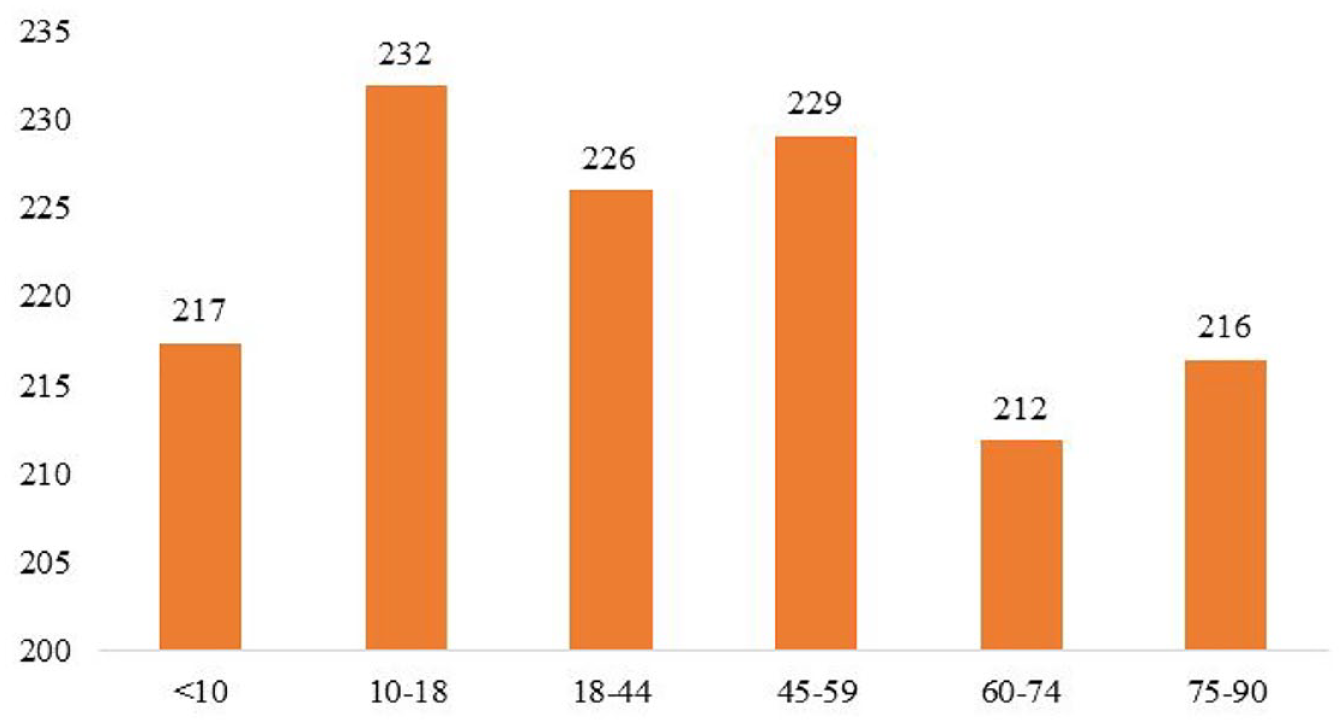
Average fructosamine in patients of Group I according to the age.
Results
The authors calculated indicators of glycemic control, namely, the average indicator of fructosamine in the sample amounted to 222.4 µmol/L (95% CI = 217-227.8), the average level of HbA1C—5.45% (95% CI = 5.17%-5.74%) and the average level of serum glucose—5.30 mmol/L (95% CI = 5.00-5.59 mmol/L). When analyzing correlations, it has been found that there is no statistically significant correlation between the level of fructosamine and HbA1C (r = −0.16 with P-value for F-test at the level of .52) and any correlation between fructosamine and glucose (r = 0.001), which is shown in Figures 2 and 3.
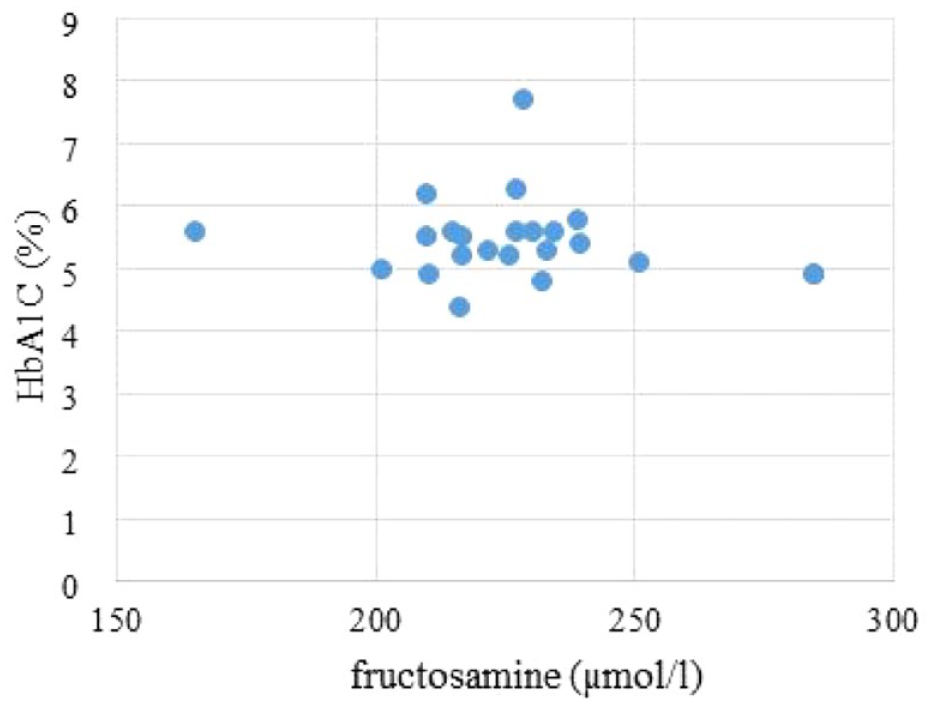
Correlation between the levels of fructosamine and glycated hemoglobin in patients of group I.
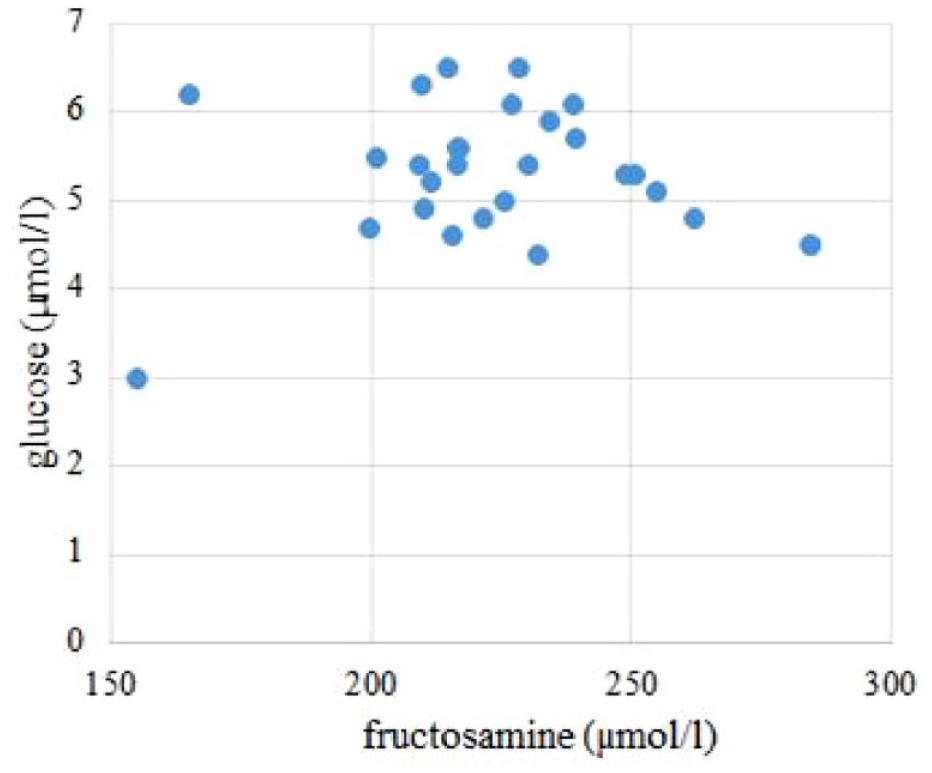
Correlation between the levels of fructosamine and serum glucose in patients of Group I.
Based on these results, it can be concluded that the level of fructosamine in apparently healthy individuals in the study region corresponds to the accepted reference values that are used in the INVITRO laboratory. When analyzing patients of Group II (with DM), it has been found that gender distribution in the sample was approximately equal: 49.4% for men (47 people) and 50.6% for women (48 people). At the same time, there was no statistically significant difference in fructosamine indicators (391 ± 13.5 µmol/L in men and 399 ± 14.3 µmol/L in women, P > .05). In this group, the average rate of fructosamine (before treatment) amounted to 395 µmol/L (95% CI = 383-407 µmol/L).
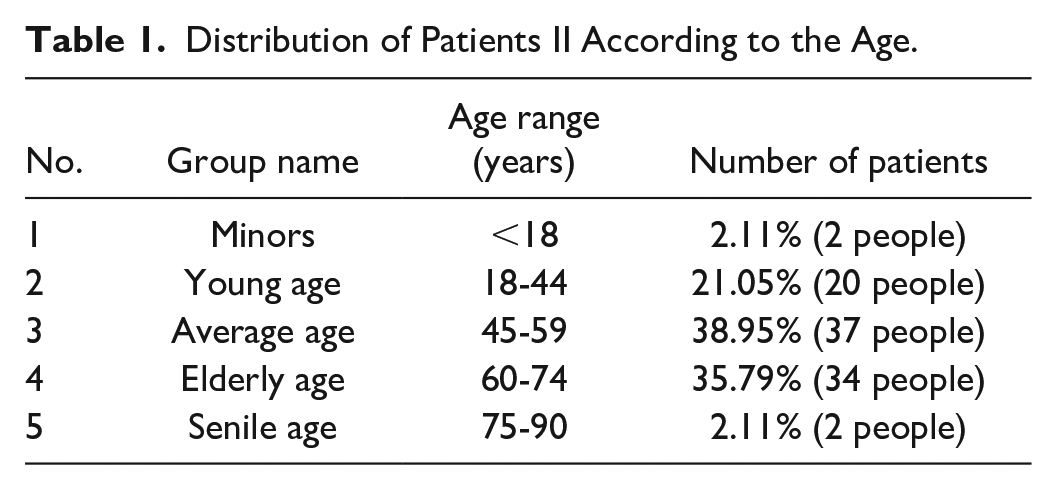
The average age in the sample is 52 ± 9.5 years, with the following age distribution according to the WHO classification (Table 1). As can be seen from the table, the overwhelming majority were middle-aged patients (38.9%) and elderly patients (35.79%), which is typical for Type 2 DM. It is noteworthy that a fairly high rate among young people (under 44 years old)—21%, may indicate an early onset of metabolic disorders and the formation of insulin resistance. At the same time, there are very few patients under 18 years of age and over 75 years of age (2.11% in each group).
Distribution of Patients II According to the Age.
Along with this, the authors analyzed the average level of fructosamine in these age groups (Figure 4). It has been revealed that the highest rate is typical for the participants under 18 years (633 ± 19.5 µmol/L), almost identical results have been observed for participants under 44 years and 45 to 59 years—(403 ± 16.1 and 397 ± 16.8 µmol/L, respectively, P > .05), and the lowest rate—for the senile people (298 ± 14.7 µmol/L).
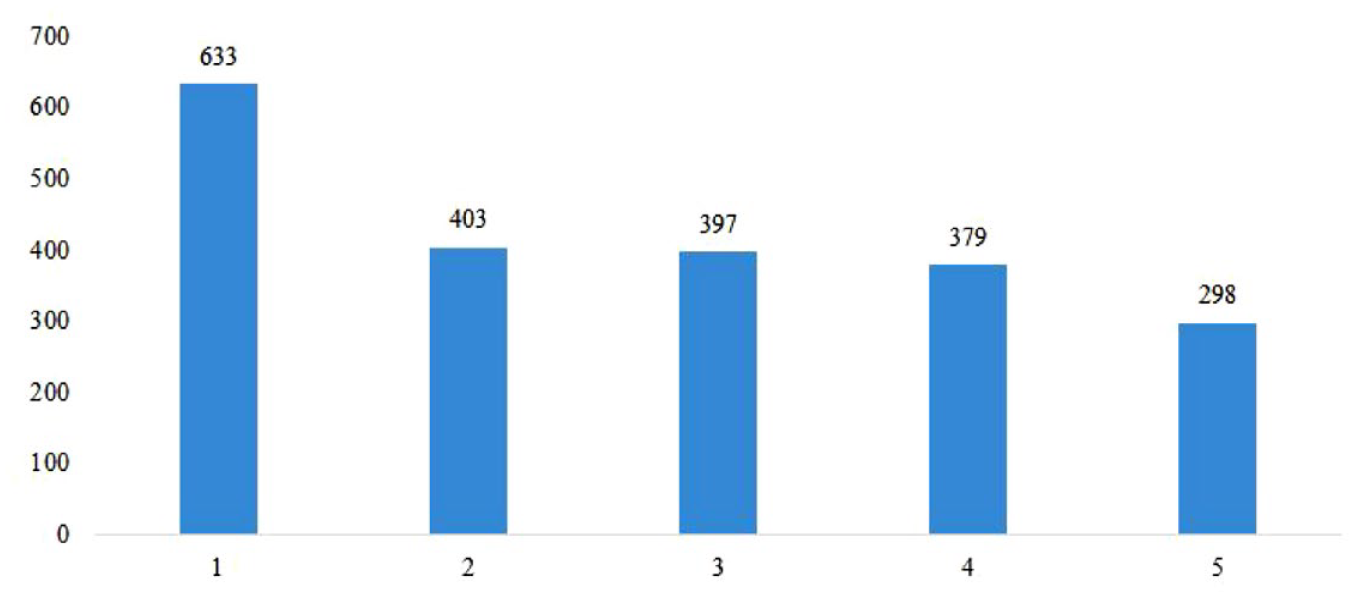
Average indicators of fructosamine in patients with DM according to age. 1—minors, 2—young age, 3—middle age, 4—elderly age, 5—senile age.
For an expanded sample of 78 people, a study was conducted for the presence of a correlation between fructosamine and HbA1c. The study also showed a statistically significant positive correlation between fructosamine and HbA1c (correlation coefficient = 0.73, P value close to zero for F-test of the hypothesis of non-linear relationship). The main discrepancies found in this study and the scatter diagram on the graph are related to the difference between HbAlc and fructosamine, since they integrate glycemia between HbAlc and fructosamine at certain time periods. Since the latter reflects complex glycemia within two weeks, the authors in their study showed that the determination of its level can be effective in detecting changes in glycemic control over a shorter period of time. In addition, statistical analysis showed the absence of a statistically significant correlation between fructosamine (correlation coefficient = −0.28, with a P value of F-test equal to .24).
Next, the results of the study of the second prospective stage are presented (in patients with DM for monitoring the effectiveness of inpatient treatment); HbA1c measurement has become the standard test for assessing glycemic control in patients with DM. All participants had an indicator above the target values. When analyzing the level of fructosamine, DM decompensation was also found (170-285 µmol/L is considered as the reference value). After inpatient treatment, fasting blood samples were taken and fructosamine was determined. The study was conducted with 34 patients who went to inpatient treatment in the endocrinological profile of the clinic. These patients taken fasting blood samples and they were measured the glucose, HbA1c, and fructosamine.
The average age of patients was 56 ± 7.5 years, and the disease duration averaged 11 ± 1.5 years. All patients had normal blood hemoglobin values, as well as normal values of serum creatinine and albumin. The average indicator of fructosamine before treatment was 396.18 mmol/L, standard deviation = 92.56 µmol/L (95% CI = 364.86-427.50 µmol/L), with a minimum value of 211.5 µmol/L and a maximum of one—618.7 µmol/L. After treatment, the average indicator of fructosamine decreased to 359.07 mmol/L, and the standard deviation amounted to 78.89 mmol/L (95% CI = 332.38-385.76 µmol/L), which is statistically significant (P < .05). Along with this, the minimum value is without significant dynamics (214.6 µmol/L), but the maximum value is significantly lower (528.2 µmol/L, P < .05). At the same time, the tests by Kolmagorov-Smirnov and Shapiro-Wilk confirm the normal distribution of fructosamine indicator in the sample both before and after treatment (Table 2). by
Distribution of the Normality of the Fructosamine Level Before and After Treatment in patients With Diabetes Mellitus.

According to the results obtained, it can be argued that a decrease in fructosamine level was observed in the vast majority of cases (ie, a positive trend was observed) and a desire to compensate for DM. To analyze the statistical significance of the results obtained, the authors conducted a paired Student’s t-test for the average difference between the fructosamine indicators before and after therapy. Thus, the average decrease in fructosamine in the sample under consideration amounted to 37.11 mmol/L, with a standard error of 6.62 mmol/L. The final Student’s t-test was 5.61, which corresponds to a P value close to zero for the hypothesis of a zero difference in the decrease of fructosamine after therapy. Accordingly, this suggests that there is a statistically significant decrease in the level of fructosamine levels in the sample after treatment (P < .05). This conclusion is maintained even at very high levels of statistical significance (1% or less), which is presented in Table 3.
Statistical Analysis of Fructosamine Level Before and After Treatment in Patients with Diabetes Mellitus.

The authors also analyzed the correlation between the level of fructosamine before and after treatment in the age groups with the disease duration. Its results are shown in Figure 5. Thus, young patients had the shortest disease duration (6.1 ± 1.3 years), while fructosamine decreased from 428 to 395 µmol/L. Patients of the average age range had DM for an average of 7.2 ± 1.8 years, and it was them who showed the most significant decrease in the indicator by 14.4% (409 vs 350 µmol/L, P < .05). Patients aged 60 to 74 years (11.9 ± 2.4 years) suffered from DM the longest, while fructosamine decreased by 27 µmol/L. Patients of senile age showed the lowest levels both before (295 µmol/L) and after (263 µmol/L) treatment, while the disease duration was only 10 ± 2.2 years.
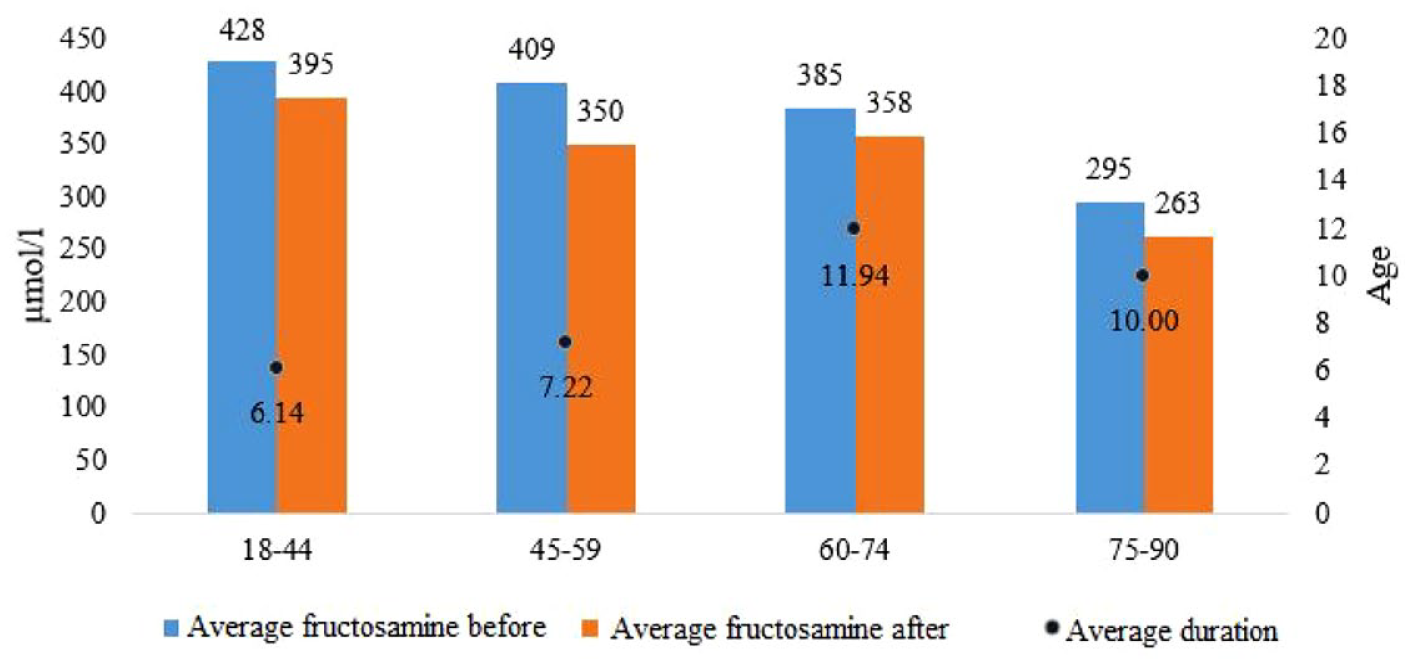
Distribution of fructosamine indicators before and after treatment in different age groups and its association with the disease duration.
After the inpatient treatment in this sample of patients, the following positive changes were found: 21% of patients achieved the compensation (fructosamine indicator less than 285 mmol/L) and another 15% of patients achieved the sub-compensation (fructosamine indicator less than 336 mmol/L). The average age of patients who achieved compensation was 62 ± 12.5 years, and the average age of patients who achieved sub-compensation was 61 ± 13.3 years, without statistical difference between them (P > .05). It is important to note that inpatient treatment had a positive dynamic, while the average decrease in fructosamine was 36.6 ± 6.96 µmol/L, which is a highly significant positive result (P < .001). At the same time, the authors have analyzed once again the correlation between fructosamine and glycated hemoglobin in patients with diabetes before and after inpatient treatment, which is shown in Figure 6. Thus, there is a clear tendency to combine these indicators, with the highest correlation at HbA1c level of 8.5% to 10.8%, which corresponds to the stage of sub-compensation of the underlying disease. That is why fructosamine can be used not only in apparently healthy people, but especially in patients with DM during the selection of a treatment regimen.
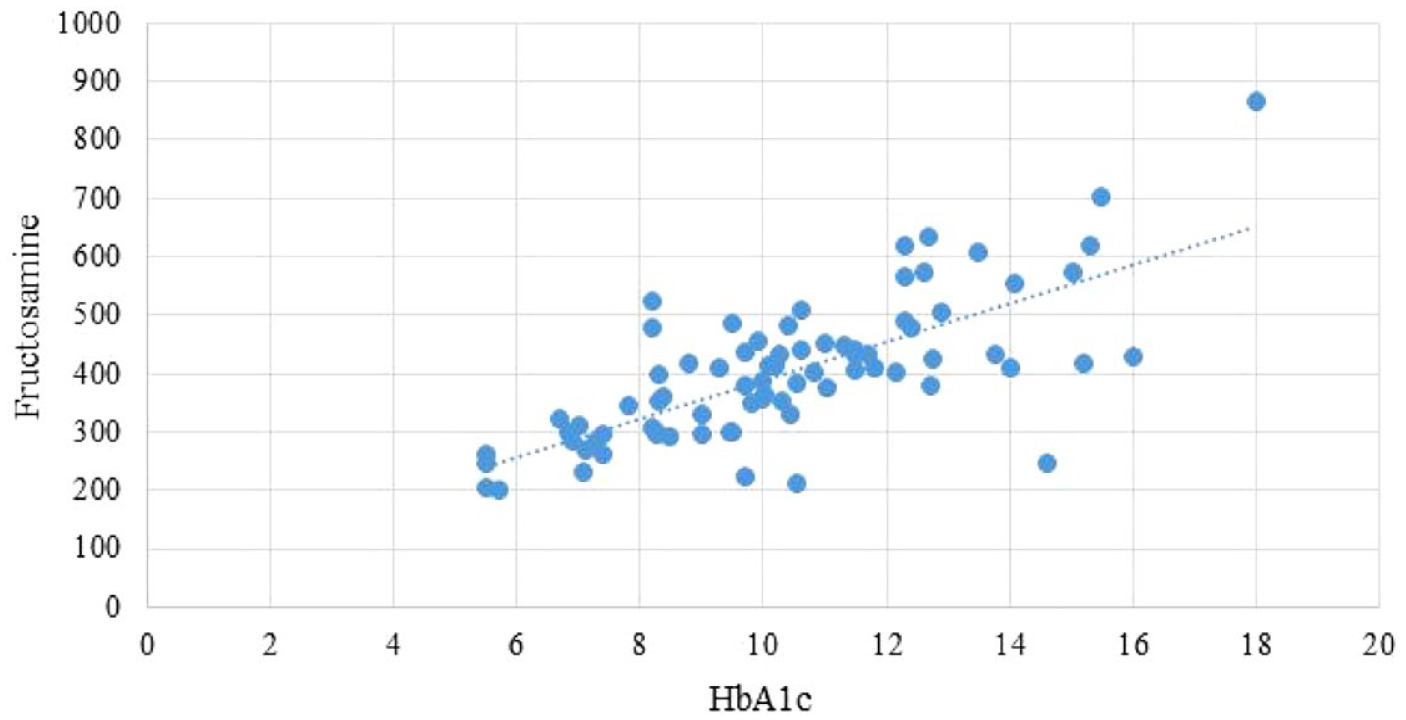
Correlation between the levels of fructosamine and glycated hemoglobin in patients with diabetes mellitus.
Discussion
Diabetes Mellitus is characterized by chronic metabolic disorders and persistent hyperglycemia. This may be due to a violation of insulin secretion, resistance to peripheral receptors, or due to certain pathologies or conditions (pregnancy, chronic pancreatitis, or pancreatic necrosis). Approximately, 90% of all cases of diabetes are Type 2 disease. In this case, the consumption of insulin by the body cells is reduced, and this leads to the emergence of insulin resistance. Earlier, this disease was more common in people over the age of 60, but now, it is increasingly being diagnosed in young people and even adolescents.9 -11 Thus, this trend was also found in this study. In the group of patients with DM, young patients (from 18 to 44 years) accounted for as much as 21%, another third of patients—the middle-aged people, and only 35%—the elderly patients (over 60 years old). At the same time, the average age for the entire sample was quite young (52±9.5 years). This is most likely due to the rising levels of obesity, lack of physical activity and a high-calorie diet, and it may lead to an early onset of metabolic disorders and the formation of strong insulin resistance. Currently, more than 410 million people worldwide live with DM, however, over the past decades, the number of cases in almost all regions of the world has increased significantly, and by 2040, this figure is able to increase by another 200 million. This fact is a matter of concern, since an increase in the prevalence of DM will lead to an increase in chronic and some acute diseases, which significantly affects the quality of life, and increases the demand for medical services and the corresponding economic costs.12,13
For example, the authors in their work analyzed the duration of diabetes in different age groups. It is expected that young patients (6.1 ± 1.3 years) had the shortest duration of disease, the patients of middle age (7.2 ± 1.8 years) had a slightly higher duration of disease, and paradoxically, the lowest rate was observed in people of senile age (10 ± 2.2 years). This tendency may lead to more frequent DM complications, which in turn complicates their control and increases the burden on the health care system. Chronic hyperglycemia in synergy with other metabolic disorders in people with diabetes can cause the defeat of various systems of organs, by leading to the development of disabling and life-threatening complications. 14 Macrovascular complications of DM, including coronary heart disease, blood stroke and peripheral vascular disease, as well as microvascular complications (such as end-stage of the chronic kidney disease, retinopathy, and lower limb amputations) bear the bulk of the burden associated with diabetes. Therefore, the factors, such as timely diagnosis, correct treatment, and monitoring of patients are the main challenges of the modern health care system. 15
Determination of HbA1c makes it possible to judge the level of glucose in the blood over the past 120 days. It is generally accepted that it is a convenient, fast, and standardized test not only for establishing a diagnosis, but also for monitoring treatment. However, at the same time, this is a rather expensive study, and it can sometimes have a lower sensitivity. In addition, the effectiveness of HbA1c may depend on the calculation method, so that, the use of the certified method of the NGSP and the Diabetes Control and Complications Trial (DCCT) is considered as the gold standard. 16 Today, the issue of the advisability of using HbA1c for screening the hyperglycemia and sensitivity of this method is being especially actively discussed. Thus, N.C. do Vale Moreira et al 17 examined in their work about 800 people to identify the elevated glycemic indicators. It has been found that HbA1c sensitivity and specificity in DM are quite high (69.2% and 92.1%, respectively), but these indicators are significantly lower for pre-diabetes (sensitivity = 57.3%, specificity = 52.0%, P < .05). This may indicate some limitations in using this diagnostic method, as well as the need to use new alternative methods.
In this study, the glycemic indicators in both people with diabetes and apparently healthy people were also examined. At the same time, the average level of HbA1C amounted to 5.45% (95% CI = 5.17%-5.74%), and the average level of serum glucose—was 5.30 mmol/L (95% CI = 5.00-5.59 mmol/L). When calculating correlations, it was not found a statistically significant correlation between the level of fructosamine and HbA1C (r = −0.16 with P value for F-test at the level of .52) and fructosamine and glucose (r = 0.001). These discrepancies may be explained by the difference between HbAlc and fructosamine, since they determine the changes at different periods of the disease. In another large study, the correlation between HbA1c indicators, gender and age was studied. It involved 18 265 people, and it was found a significantly higher level of HbA1c in men than in women (P < .0001). At the same time, the indicator gradually increased with age up to 79 years, and then it reached a plateau, but the difference in HbA1c values in people of different genders only at the age of 30 to 59 years was statistically significant among themselves (P < .05). 18 This tendency may be due to the factors such as higher blood pressure and higher blood lipid level in men of this age group, but in women, these factors can easily fluctuate from the endocrine profile. Along with this, it should be noted that when choosing HbA1c as a screening criterion for diabetes, more attention should be paid to the patient’s gender and age.
Since HbA1c has its disadvantages when used as a marker for diabetes control, other possible markers are being actively studied. Fructosamine is an indicator of the total glycated protein of blood serum that does not require an overnight fast before donation, and it is much cheaper and easier to perform than HbA1c tests, and it may have an advantage in patients with certain conditions. It was first used about 40 years ago, but in recent decades, this issue has been studied in more detail, especially for preoperative screening. 19 This biomarker has a half-life of 14 to 21 days, and thus it measures glucose control over two to three weeks. This is what makes it a valuable marker for both screening and monitoring the therapeutic purposes. In patients with inadequate glycemic control during the treatment, a return to better glycemic control can be confirmed within two weeks of using fructosamine, rather than three months, such as when using HbA1c. 20 The possibility of using fructosamine as a marker for glycemic control has been studied in various types of research. Since erythrocytes survival does not influence on fructosamine, this indicator may be more appropriate for glycemic control, than HbA1c in patients with chronic kidney disease. 21 In addition, the level of fructosamine is useful for rapid assessment of recent therapeutic effectiveness after the change in therapeutic tactics. This is also useful for determining the initial treatment for children and adolescents with DM and for lightning-fast diabetes. 22
For example, in this study, the average level of fructosamine in Group I amounted to 223.5 µmol/L, while it was not found significant difference in men and women (P > .05). Based on this, it can be argued that its level in apparently healthy individuals in the study region corresponds to the accepted reference values that are used in the INVITRO laboratory. At the same time, the average indicators in patients with diabetes before treatment amounted to 395 µmol/L (95% CI = 383-407 µmol/L), but it is noteworthy that the highest rate is typical for participants under 18 years (633 ± 19.5 µmol/L), and the lowest rate is observed in people of senile age (298 ± 14.7 µmol/L). It can be assumed that the duration of disease anamnesis, adherence to the prescribed therapy and the severity of DM influence this.
In this study, the authors evaluated the correlation between fructosamine and HbA1c in patients with DM. A statistically significant positive correlation was found between fructosamine and HbA1c (correlation coefficient = 0.73, P value is close to zero for F-test of the hypothesis of non-linear relationship). Knowing that fructosamine reflects the complex glycemia only during the last 14 days, the authors showed in their work that determination of its level can be effective in the targeted detection of changes in glycemia over a shorter period of time, than other markers. For now, there are works by other authors in confirmation of this. For example, in the study by Skinner et al, 23 it was compared the ratios between HbA1c, serum glucose, and fructosamine in 102 people with diabetes. According to the results, a correlation was found between HbA1c and fructosamine, fructosamine and DM (r = 0.71, P < .0001 and r = 0.61, P < .0001, respectively). Chi-square analysis showed that the number of patients classified as people with diabetes was significantly 15.6% higher with fructosamine compared with HbA1c (P = .016). This may indicate that the use of fructosamine is a more sensitive method, but at the same time, it does not exclude the possibility of overdiagnosis.
At the same time, fructosamine can be used not only as a marker for glycemic control but also for predicting adverse outcomes after surgical interventions. For example, 1212 patients took part in a recent large prospective multicenter study (for 2021), the observation period was one year. It was found that with a level of fructosamine more than 293 µmol/L, the probability of developing postoperative complications was 6.7 times higher compared with the indicator below 293 µmol/L (P = .002). In addition, patients with elevated levels were significantly more likely to be rehospitalized (16.7% vs 4.4%, P < .007) and they had a higher mortality rate (3.7% vs 0.6%, P = .057). 24 This testifies to the fact that fructosamine is a good predictor of adverse outcomes in patients undergoing endoprosthesis, and it is necessary to consider its routine use to reduce the risk of complications and mortality. Also in this study, it was found an early positive tendency toward stabilization of the glycemic levels after inpatient treatment based on its level. After treatment, the average indicator of fructosamine decreased to 359.07 mmol/L (95% CI = 332.38-385.76 µmol/L), which is statistically significant (P < .05). It is interesting that besides this, the value of the minimum indicator did not have significant dynamics (214.6 µmol/L), but the maximum value significantly decreased (P < .05). After inpatient treatment, 21% of patients achieved DM compensation with a fructosamine indicator of less than 285 mmol/L, and another 15% achieved sub-compensation with a fructosamine indicator less than 336 mmol/L. It can be summarized that this treatment had positive dynamic, while the average decrease in fructosamine amounted to 36.6 ± 6.96 µmol/L, which is a highly significant positive result (P < .001) that can be considered for use in practice. Although the estimate of glucose concentration required for the correlation of fructosamine and HbA1 is somewhat arbitrary, it serves to provide a numerical expression to a purely subjective judgment made in clinic when the diabetic diaries are reviewed, and is thus a pertinent exercise. Estimates of fructosamine and HbA1 obtained during a clinic visit are helpful tools for deciphering the diabetic diary data. 25
Conclusions
This scientific study of the average level of fructosamine in apparently healthy individuals and individuals with DM, as well as the possibility of its use in evaluating the effectiveness of inpatient treatment of people with hyperglycemia on the seven to ten days of hospitalization, led to such conclusions. The level of fructosamine in healthy individuals in this region corresponds to the reference values proposed by the INVITRO laboratory, and it amounted to 222 µmol/L (95% CI = 216-227). The authors did not find a statistically significant correlation between the level of fructosamine and HbA1C (r = −0.16 with P value for F-test at the level of .52), while no significant correlation was found between the indicators of fructosamine and glucose. In patients with DM during the disease decompensation, it was found both an increased level of HbA1C and an increased level of fructosamine. At the same time, a statistically significant positive correlation between fructosamine and HbA1c was determined (correlation coefficient = 0.73, P value is close to zero for the F-test of the hypothesis of the absence of a linear relationship), which was earlier confirmed in other studies.
In this study, during hospitalization in the endocrinology department (seven to ten days) and proper therapy, was achieved DM compensation only in 21% of patients with a fructosamine indicator of less than 285 mmol/L, and sub-compensation in 15% of patients with a fructosamine indicator of less than 336 mmol/L. It was noted that inpatient treatment had a positive dynamic, while the average decrease in fructosamine indicator amounted to 36.6 ± 6.96 µmol/L, which is a highly significant positive result (P < .001). Based on the obtained results, it is possible to argue that fructosamine can be a reliable indicator for determining the effectiveness of DM treatment in a short period. The main significance of the work performed lies in the fact that its results serve as a basis for understanding and further in-depth study of using fructosamine for the diagnosis and monitoring of diabetes, which will allow the evaluation and implementation of new cost-effective medical technologies. The results obtained can be useful for practicing doctors not only in secondary health care, but also for district endocrinologists and therapists in the outpatient management of patients, as well as for health care organizers. Further studies are needed to examine fructosamine level in a larger sample and long-term monitoring period.
Footnotes
Abbreviations
ADA, American Diabetes Association; CI, confidence intervals; DCCT, Diabetes Control and Complications Trial; Df, degree of freedom; DM, diabetes mellitus; NGSP, National Glycohemoglobin Standardization Program; RK, Republic of Kazakhstan; WHO, World Health Organization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.