
Abstract
Keywords
Rates of type 2 diabetes (T2D) are increasing, and many individuals with T2D do not meet glycemic targets. 1 For many patients with T2D, their primary care provider (PCP) is the only physician treating their diabetes. 2 In this retrospective, observational study, we used real-world data from 13 AMGA (American Medical Group Association) member health care organizations across the United Sates to assess whether real-time continuous glucose monitoring (RT-CGM) initiation was associated with improvements in glycemic metrics among individuals with T2D receiving primary care.
A retrospective analysis was performed using electronic health records and outbound administrative claims data, which were extracted, mapped, and normalized by Optum. Included individuals had a T2D diagnosis, were 18 to 85 years of age, had ≥1 outpatient PCP visit 18 months prior to RT-CGM use, initiated RT-CGM between August 1, 2015, and September 30, 2020, and had glycated hemoglobin (HbA1c) values ≤12 months prior to RT-CGM initiation (baseline) and three to nine months after RT-CGM initiation (follow-up). Exclusion criteria included diagnosis of T1D or gestational diabetes, evidence of palliative care or hospice, death within nine months of RT-CGM initiation, and evidence of prior CGM use. The primary outcome was change in HbA1c from baseline to follow-up. Individuals were stratified by baseline HbA1c (≤7.5% and >7.5%) and insulin regimen.
Participants (n = 458) were 61 [54-70] years of age (median [interquartile range]), 50% female, and 85% white, and the insured status was 50% commercial, 43% Medicare, and 2% Medicaid. The average number of PCP visits in the prior year was mean (SD) of 3.7 (2.9). Intensive insulin therapy (IIT, prandial ± basal insulin) was used by 75% (343/458) of participants, non-intensive insulin therapy (NIIT, basal insulin) was used by 11% (51/458), and non-insulin therapies (NITs) were used by 14% (64/458). Among individuals with baseline HbA1c >7.5%, HbA1c significantly decreased regardless of the insulin therapy regimen (Figure 1). Glycated hemoglobin did not significantly change in individuals with baseline HbA1c ≤7.5%.
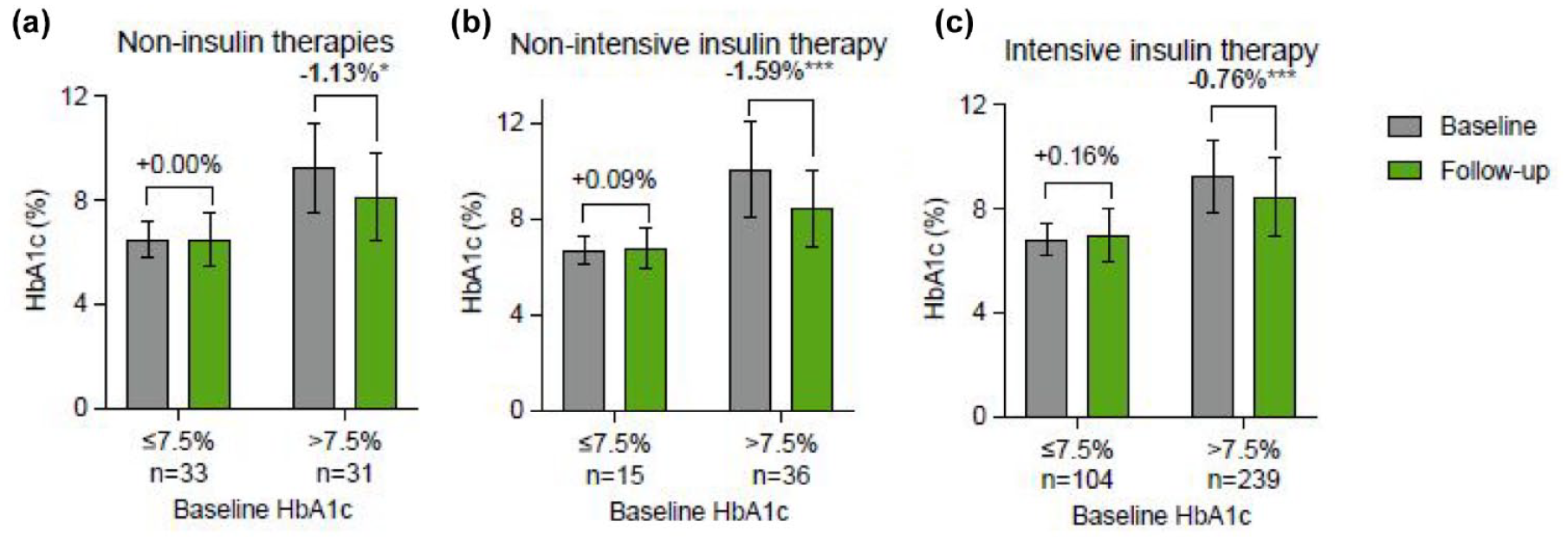
Change in HbA1c stratified by baseline HbA1c. Baseline and follow-up HbA1c stratified by baseline HbA1c in individuals on (a) non-insulin therapy, (b) non-intensive insulin therapy (bolus insulin), and (c) intensive insulin therapy (prandial ± basal insulin).
These results align with others in the literature. In Beck et al, initiation of RT-CGM by individuals with T2D on IIT experienced a significantly greater decrease in HbA1c (–1.0% with RT-CGM vs –0.6% for Controls). 3 In Grace et al, individuals with T2D on NIIT or NIT experienced a mean change in HbA1c of –3.0 percentage points after initiating RT-CGM. 4 Both studies required baseline HbA1c >7.5% for inclusion.3,4
Strengths of this study include the relatively large population and the diversity of insulin use and insurance coverage. Study limitations include the lack of a control group and the lack of CGM-based glycemic metrics. We do not know why participants initiated RT-CGM or the extent of their adherence to RT-CGM or their insulin regimens. We also do not know how insulin was delivered or whether any medications were changed between baseline and follow-up. Study generalizability is limited by the inclusion of only RT-CGM systems and the all-US population.
These findings suggest that RT-CGM initiation can improve HbA1c in primary care patients with poorly controlled T2D regardless of their insulin therapy reg. This real-world evidence supports further studies of RT-CGM’s benefits in the broader T2D population.
Footnotes
Acknowledgements
The authors thank Courtney Green for editorial assistance. Dexcom is a registered trademark of Dexcom, Inc. in the United States and other countries.
Abbreviations
AMGA, American Medical Group Association; CGM, continuous glucose monitoring; HbA1c, glycated hemoglobin; IIT, intensive insulin therapy; NIT, non-insulin therapies; NIIT, non-intensive insulin therapy; PCP, primary care provider; RT-CGM, real-time continuous glucose monitoring; T2D, type 2 diabetes.
Authors’ Note
This work was presented in part at the 82nd American Diabetes Association meeting in New Orleans, LA, on June 3-7, 2022.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SS and ELC are employees of American Medical Group Association (AMGA). GJN and RT are employees of Dexcom, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by Dexcom, Inc.