
Abstract

The care of people with type 1 diabetes (T1D) has been revolutionized by technological advances, including the automated insulin delivery (AID) system, which uses data from a continuous glucose monitor (CGM) to automatically adjust insulin delivered via a continuous subcutaneous insulin infusion (CSII). 1 A growing number of commercial AID systems are approved by the US Food and Drug Administration, but none have approval for use in pregnancy, due to the absence of rigorous data. With few adjustable variables, these commercial AID systems do not allow for customization of insulin delivery parameters, which is particularly limiting for pregnant individuals who have tighter glycemic targets and greater glycemic variability than nonpregnant individuals. These limitations can be circumvented with open-source AID systems (“hacked” or “do-it-yourself” [DIY] loops),2,3 which link commercially available CGM to CSII via unregulated but customizable software. This software was created by a community of volunteers, is freely available online, and has been adopted by a growing population. 4 Although there are data supporting the clinical benefits of open-source AID systems in the nonpregnant population, 5 available literature for the pregnant population remains scant.
We identified five cases of successful pregnancies in individuals who used open-source AID systems at a single institution between 2021 and 2022 (Table 1). All patients had ≥2 years of experience with open-source AID systems and A1c ≤ 6.5% prior to conception. There were no episodes of severe hypoglycemia or AID system failure. Only one patient had a preterm delivery. None of the infants required intravenous dextrose for treatment of hypoglycemia or neonatal intensive care unit admission secondary to maternal T1D. There were no cases of major congenital malformations or macrosomia in any of the infants.
Demographics, Glycemic Details, and Perinatal Outcomes for Patients With T1D Using Open-Source AID Systems During Pregnancy.
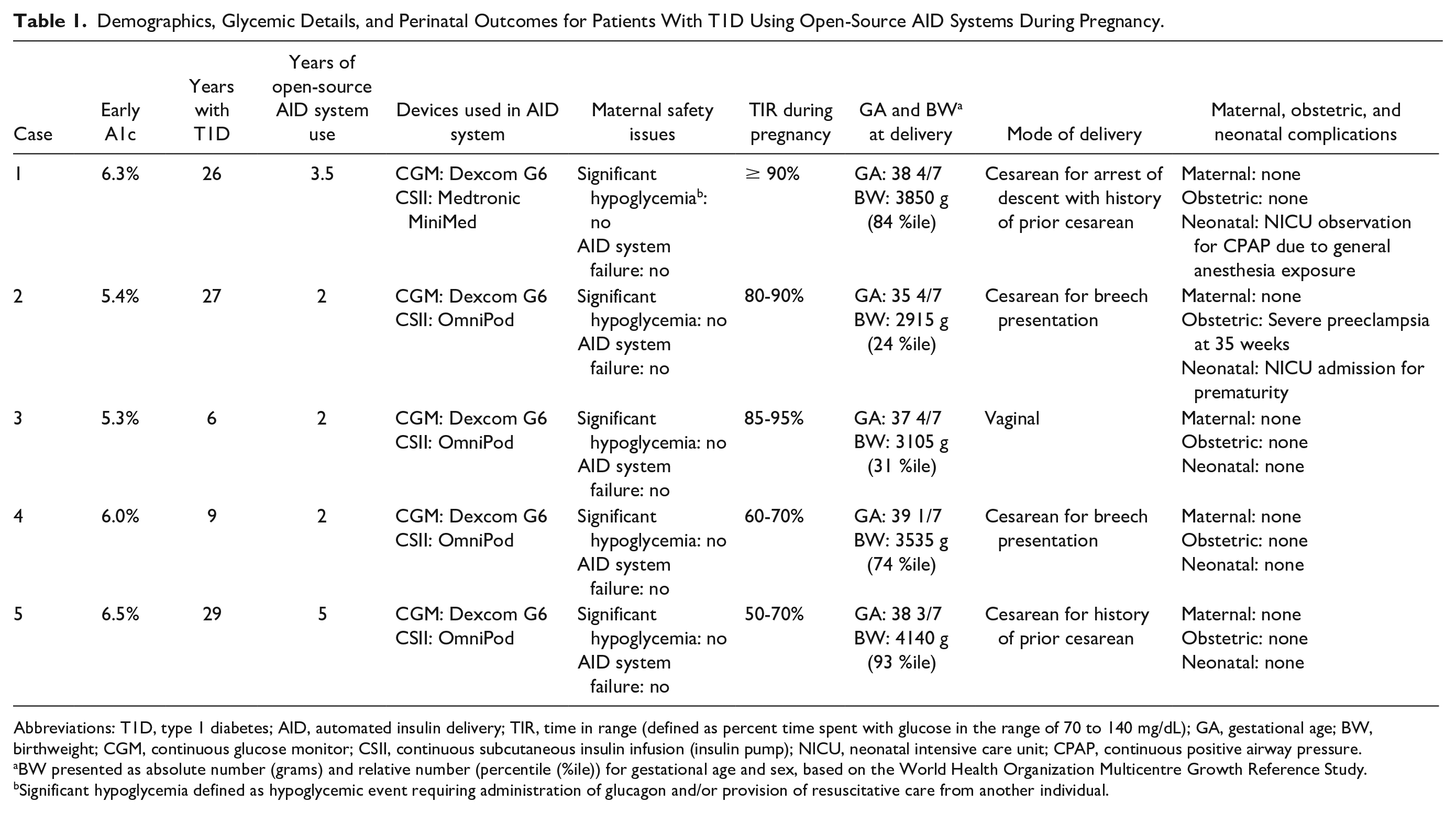
Abbreviations: T1D, type 1 diabetes; AID, automated insulin delivery; TIR, time in range (defined as percent time spent with glucose in the range of 70 to 140 mg/dL); GA, gestational age; BW, birthweight; CGM, continuous glucose monitor; CSII, continuous subcutaneous insulin infusion (insulin pump); NICU, neonatal intensive care unit; CPAP, continuous positive airway pressure.
BW presented as absolute number (grams) and relative number (percentile (%ile)) for gestational age and sex, based on the World Health Organization Multicentre Growth Reference Study.
Significant hypoglycemia defined as hypoglycemic event requiring administration of glucagon and/or provision of resuscitative care from another individual.
This case series provides promising information regarding open-source AID system use in pregnancy. T1D-related risk of maternal and neonatal morbidity is directly related to degree of hyperglycemia, making management of glycemia critical in pregnancy. 6 The physiological changes of pregnancy contribute to frequent and often unpredictable changes in glycemia, making pregnancy an ideal state for open-source AID systems that allow for greater flexibility and customization than commercially available AID systems. Two unique aspects of the described population limit the generalizability of these findings. First, these patients represent a unique subpopulation that achieves euglycemia prior to conception, is technologically savvy, and has advanced diabetes self-agency. Open-source AID systems require considerable motivation, time, and effort, and individuals who use these systems are distinct from the general T1D population. Second, these patients were cared for by a multidisciplinary team of experts in Maternal-Fetal Medicine, Endocrinology, Nursing, and Nutrition, all of whom have experience in and comfort with management of complicated diabetes technology.
We encourage clinicians to become familiar with the detailed workings of both commercial and open-source AID systems. As more nonpregnant individuals utilize these technologies, more patients will conceive while using these technologies, and many will prefer to continue their use in pregnancy. Clinicians should be equipped to counsel patients regarding the absence of data supporting use of open-source AID systems in pregnancy and to use shared decision-making to support patient preferences. We also recommend ongoing efforts to systematically study these systems in pregnancy. Safety and efficacy data should be collected for both glycemic outcomes and clinically relevant obstetric outcomes. Efforts should be made to understand patient-reported measures of time spent on diabetes management and the emotional burden of diabetes care in pregnancy. Because the number of gravidas using open-source AID systems at single institutions is likely to be small, consideration should be given to the development of a national registry that prospectively collects data from multiple sites.
Footnotes
Acknowledgements
The authors thank the individuals described herein for their enthusiastic willingness to provide their data for publication and to share their experience with open-source automated insulin delivery systems in pregnancy.
Abbreviations
AID, automated insulin delivery; CGM, continuous glucose monitor; CSII, continuous subcutaneous insulin infusion; DIY, do-it-yourself; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.