
Abstract
Background:
The American Diabetes Association (ADA) recommends measuring A1c in all inpatients with diabetes if not performed in the prior three months. Our objective was to determine the impact of utilizing Lean Six Sigma to increase the frequency of A1c measurements in hospitalized patients.
Methods:
We evaluated inpatients with diabetes mellitus consecutively admitted in a community hospital between January 2016 and June 2021, excluding those who had an A1c in the electronic health record (EHR) in the previous three months. Lean Six Sigma was utilized to define the extent of the problem and devise solutions. The intervention bundle delivered between November 2017 and February 2018 included (1) provider education on the utility of A1c, (2) more rapid turnaround of A1c results, and (3) an EHR glucose-management tab and insulin order set that included A1c. Hospital encounter and patient-level data were extracted from the EHR via bulk query. Frequency of A1c measurement was compared before (January 2016-November 2017) and after the intervention (March 2018-June 2021) using χ2 analysis.
Results:
Demographics did not differ preintervention versus postintervention (mean age [range]: 70.9 [18-104] years, sex: 52.2% male, race: 57.0% white). A1c measurements significantly increased following implementation of the intervention bundle (61.2% vs 74.5%, P < .001). This level was sustained for more than two years following the initial intervention. Patients seen by the diabetes consult service (40.4% vs 51.7%, P < 0.001) and length of stay (mean: 135 hours vs 149 hours, P < 0.001) both increased postintervention.
Conclusions:
We demonstrate a novel approach in improving A1c in hospitalized patients. Lean Six Sigma may represent a valuable methodology for community hospitals to improve inpatient diabetes care.
Background
One in four patients admitted to a hospital carries a diagnosis of diabetes mellitus, and about 30% of these patients require two or more hospitalizations in any given year. 1 Hospitalization remains a unique opportunity to assess glycemic control in patients who are otherwise not routinely followed up by outpatient providers and those who may not even know they have diabetes. The advantage of using the hemoglobin A1c (A1c) in assessing glycemic control is that it does not require patients to be fasting and reflects glycemic control over the preceding three months. Studies have shown it can predict inpatient glycemic control and assist with discharge planning.2 -7 It has become a standardized, reliable test used extensively in outpatient and inpatient settings. 8 The American Diabetes Association Standards of Care recommend A1c measurement for all patients with a known history of diabetes or hyperglycemia admitted to the hospital, if not performed in the previous three months. 9 However, data are lacking examining how frequently this recommendation is being followed and what could be done to improve compliance.
The Six Sigma methodology was first implemented by the Motorola company in the mid-1980s as a management system to improve efficiency. Since then, it has been adopted by other industries including the healthcare sector. A recent systematic review 10 found it has been utilized across various specialties to not only increase cost-effectiveness but also improve time-utilization and reduce medical errors. Of all the articles analyzed, 26.5% used a synergistic combination of Lean and Six Sigma management processes. Lean is a management philosophy that focuses on producing goods optimally by eliminating waste, and by incorporating Six Sigma, it aims at reducing variation.
Six Sigma projects have typically utilized the DMAIC (define, measure, analyze, improve, and control) framework to improve existing practices. The five phases of DMAIC are (1) define the problem and obtain team alignment; (2) measure the baseline to determine the gaps; (3) analyze the process and data to determine the root cause of the defects and opportunities for improvement; (4) improve the process by implementing solutions that address the root causes; and (5) control the improvements by instituting mechanisms to sustain them.
In this study, we describe the use of Lean Six Sigma to increase the frequency of A1c measurement in inpatients with a history of diabetes in a community hospital setting.
Methods
Patients
Data from all adult patients (age ≥18 years) with diabetes mellitus hospitalized at a community hospital in Maryland, between January 1, 2016, and June 31, 2021, were collected retrospectively using the electronic health record (EHR). The diagnosis of diabetes mellitus was indicated by an International Classification of Diseases, Tenth Revision (ICD-10) diagnosis code of E08 (diabetes due to underlying condition), E09 (drug- or chemical-induced diabetes mellitus), E10 (type 1 diabetes), E11 (type 2 diabetes mellitus), E12 (malnutrition-related diabetes), or E13 (other specified diabetes) recorded in the primary diagnosis code, secondary diagnosis code, problem list, or consultation order.
We excluded patients who had an A1c result within the three months prior to admission in the Johns Hopkins Healthcare System EHR. We also excluded patients under observation status as most were only in the hospital for less than 48 hours. In cases where the same patient had multiple admissions, each admission was counted individually. Those admitted under the care of the Kaiser Permanente Medical Group, Inc, were excluded as their care providers did not wish to be included in the planned intervention.
All personal identifiers of patient data were stripped to protect patient privacy. This quality-improvement study has been acknowledged by the Johns Hopkins Medicine Institutional Review Board.
Intervention
A multidisciplinary committee was formed, composed of an endocrine hospitalist, 11 pharmacist, information technology nurse, hospitalist, hospitalist practice administrator, and a Six Sigma Master Black Belt Coach (an individual who is proficient in the Six Sigma methods and tools). They designed interventions, educational materials, and monitoring. Results were reported quarterly to the hospital’s glucose steering committee. 12
Define
During the define phase of the Six Sigma methodology, the problem was defined from both the hospital’s and the provider’s perspective. A high-level process map was developed to track steps involved in the admission of patients, for example, documentation of past medical history, review of recent labs, and outpatient medication reconciliation. These maps charted the suppliers, inputs, process, outputs, and customers (SIPOC) of each stage that influenced the A1c measurement (Table 1). A communication strategy was developed to identify audiences for planned interventions. This depended on the willingness of care providers and laboratory technicians to share their potential biases concerning the importance of A1c measurements and the hurdles to completing laboratory analysis efficiently. Potential areas of improvement were identified after the development of this process map.
The SIPOC (Suppliers, Inputs, Process, Outputs, Customers) Flowchart.
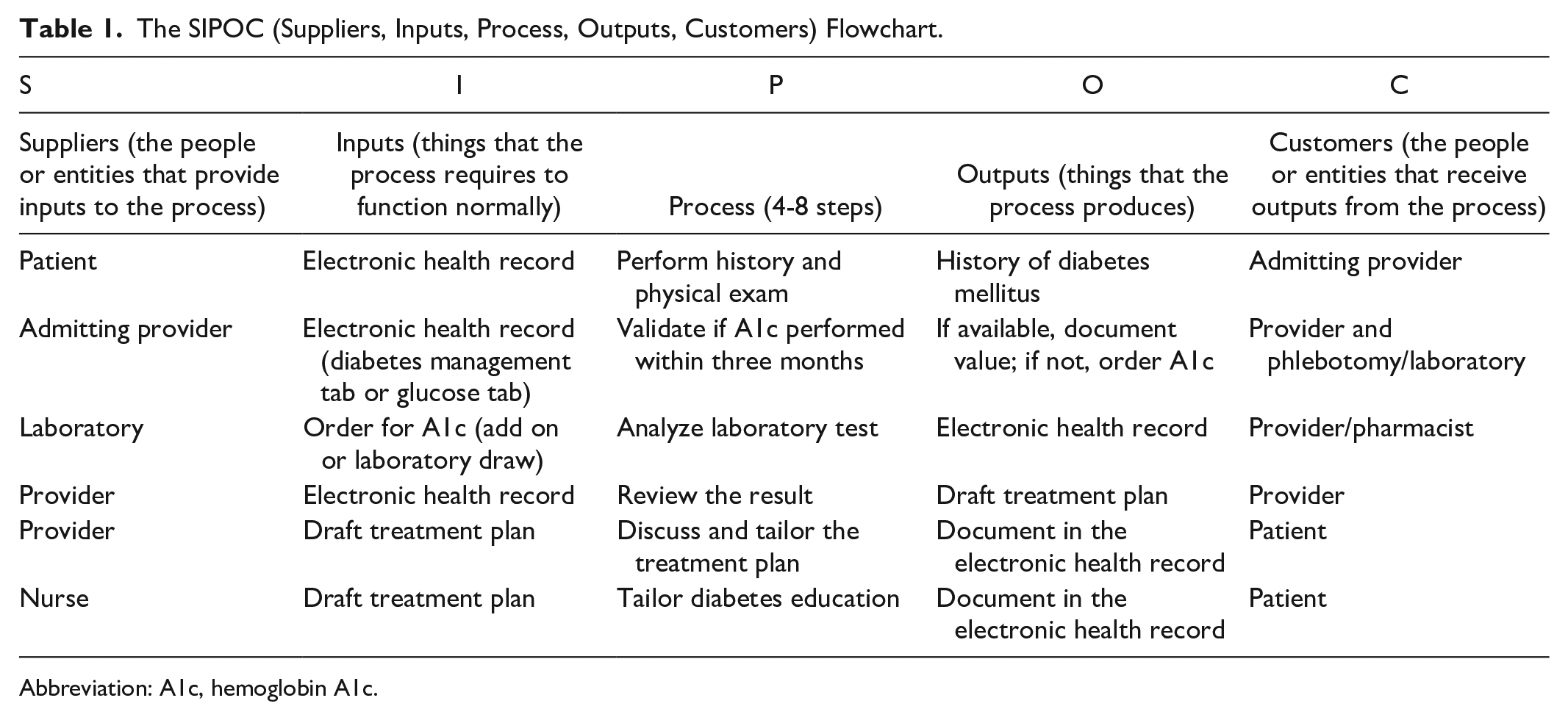
Abbreviation: A1c, hemoglobin A1c.
Measure
The performance at baseline (percentage of A1c laboratory results for patients admitted with a past medical history of diabetes and no A1c checked within three months of admission) was ascertained to validate that a problem existed. We found that at baseline, in the year 2016, only 58.67% of qualifying patients had an A1c measured during their admission.
Analyze
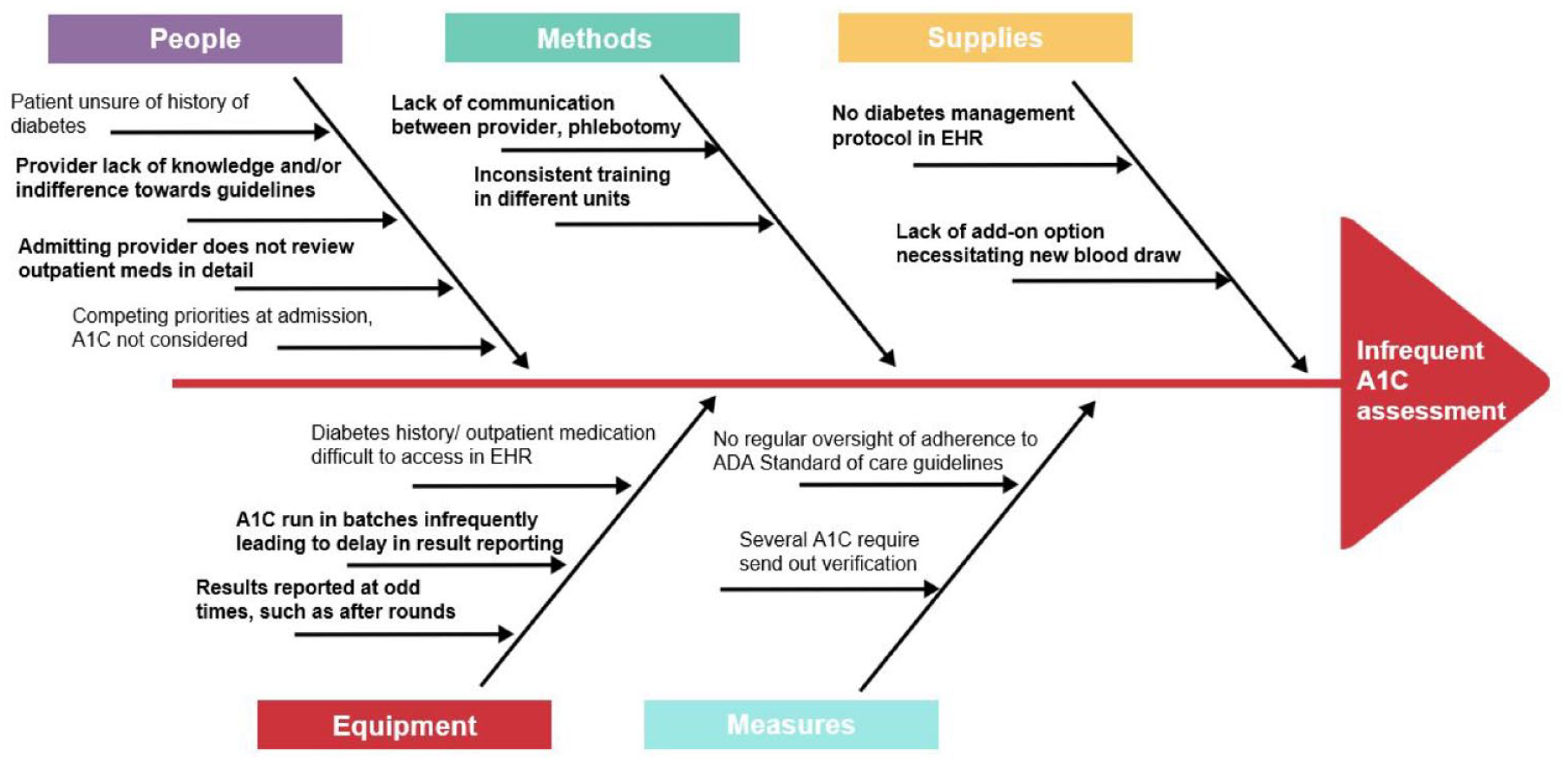
The team identified the main hurdles that impacted performance and determined the cause of each based on the analysis of process maps, interviews with staff (eg, admitting providers, phlebotomy, laboratory, pharmacists), and development of an Ishikawa fishbone diagram (Figure 1). Based on this, the primary/root causes to focus our interventions on were selected.
For example, admitting providers were surveyed about their understanding of American Diabetes Association guidelines regarding A1c and the potential reasons for deviation from these (Table 2). Many providers were unsure of the benefits of measuring A1c in the inpatient setting, considering that most patients with diabetes were hospitalized for reasons other than glucose management. In general, glycemic control was a secondary thought, to be taken care of by another care provider later during the admission. Inconsistency in training and inadequate communication in this chain of care providers would eventually result in no order being placed.
Provider Survey Response for Why A1c Is Not Ordered in Patients With a History of Diabetes.
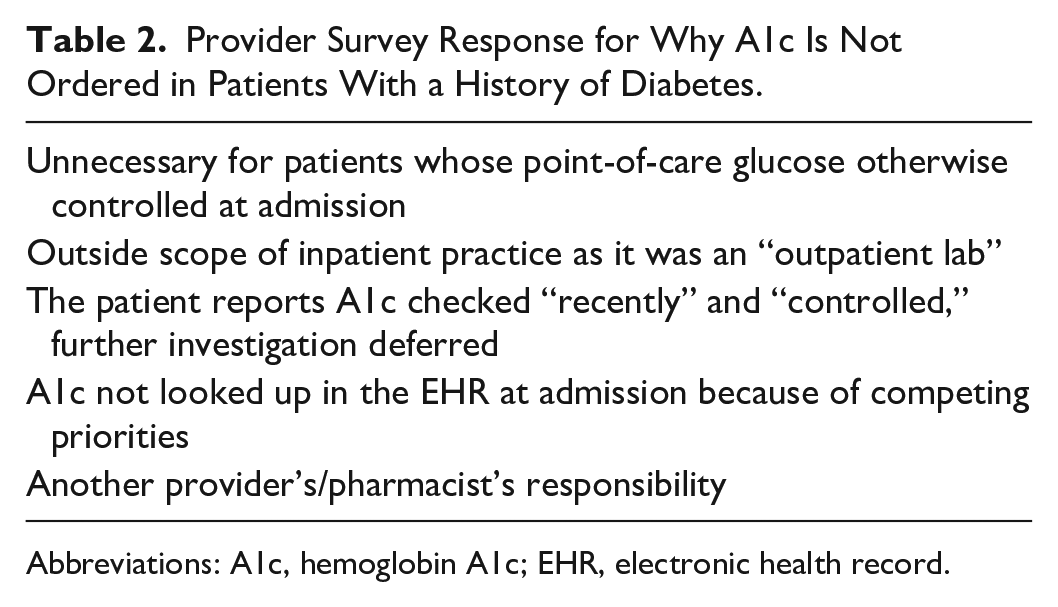
Abbreviations: A1c, hemoglobin A1c; EHR, electronic health record.
After meeting with the hospital’s laboratory leadership, it was realized that A1c samples were batched and analyzed only a few times per week, leading to delays in results. The rationale behind this was that A1c was not being ordered frequently by inpatient providers and was still largely considered an “outpatient test” whose results were not required immediately. The inpatient providers, in turn, assumed they would not have the results back for review in a timely fashion and were, thus, less likely to request this test. Also, several A1c results, for example, unusually high values, were sent out for verification, resulting in further delays.
Improve
The intervention bundle was rolled out between November 2017 and February 2018. This included the following specific actions:
Control
Various mechanisms were proposed to sustain the improvements in the system. Pamphlets were disseminated across the hospital as a refresher for care providers after initial training. Partnership with nursing to provide feedback to hospitalists was also vital in ensuring these changes were sustained. The outcomes of these interventions were presented at follow-up meetings of the glucose steering committee.
Statistics
The primary outcome of the study was the change in frequency of A1c testing preintervention (January 2016-November 2017) versus postintervention (March 2018-June 2021). Student’s t-test and χ2 test were used to assess differences in means and frequencies between groups, respectively. Changes in slope were assessed using linear regression. Data were transformed as necessary to maintain assumptions of normality.
Results
A total of 13 867 patients were included (5227 preintervention and 8640 postintervention). The characteristics of the study population are shown in Table 3. Demographics did not differ between the preintervention and postintervention groups. Overall, the patient cohort had a slightly higher proportion of men than women (52.2% vs 47.8%) and consisted of older adults (mean age: 70.9 years, range: 18-104 years). Most patients had a diagnosis of diabetes listed in their secondary diagnoses (99.6%), with only 5.6% having it listed as a primary diagnosis at admission.
Demographics of Full Patient Cohort.
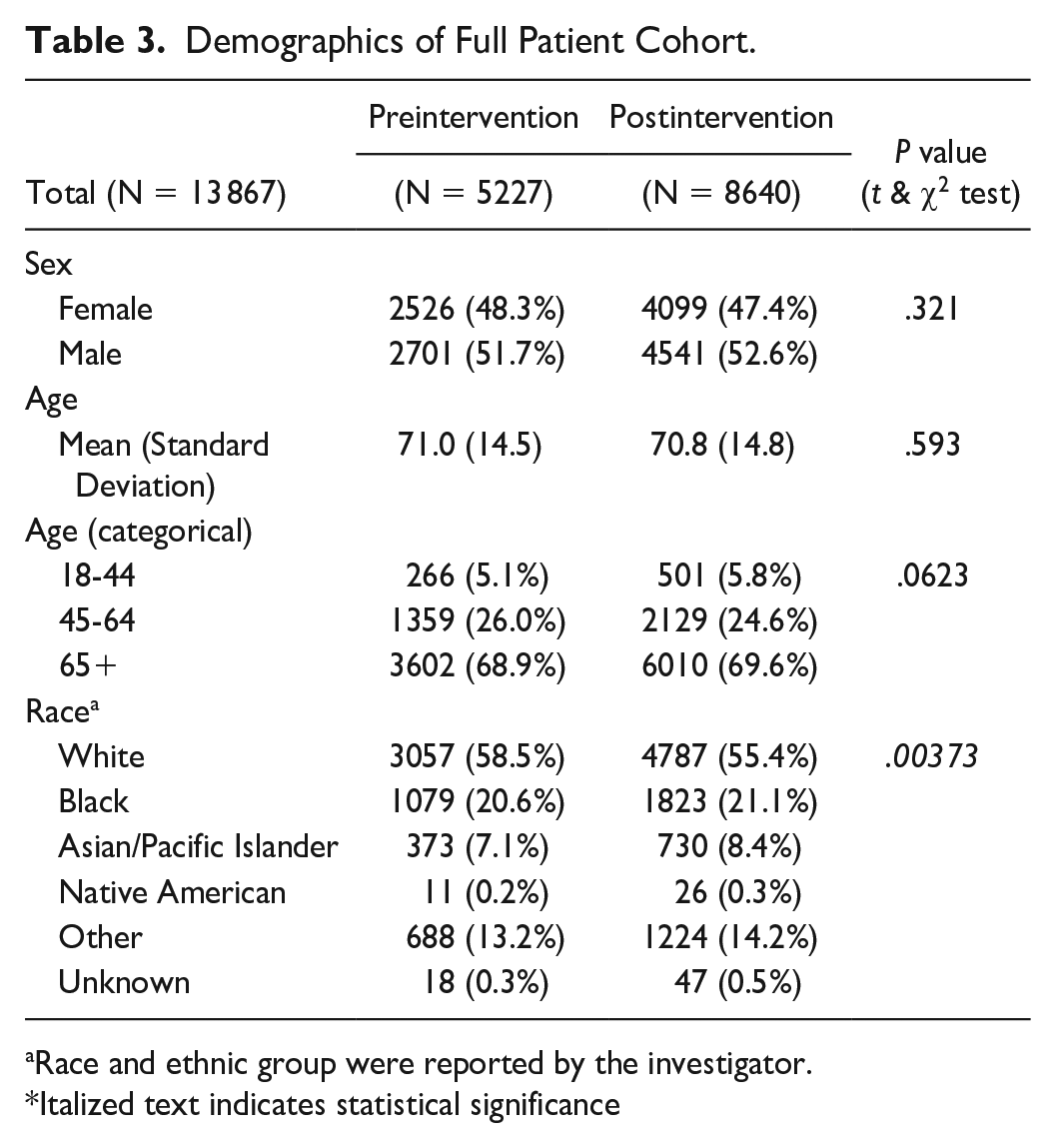
Race and ethnic group were reported by the investigator.
Italized text indicates statistical significance
Preintervention, only 61.2% of patients on average had an A1c measured during hospitalization (Table 4). Following the delivery of the intervention bundle, the frequency of A1c measurements increased to 74.5% in the postintervention period (P < .001). The rate of testing continued to increase over time until it plateaued at nearly 80% at the end of the study period (Figure 2). This improvement in the frequency of A1c measurement was sustained for more than two years following the initial intervention.
Admission Characteristics.
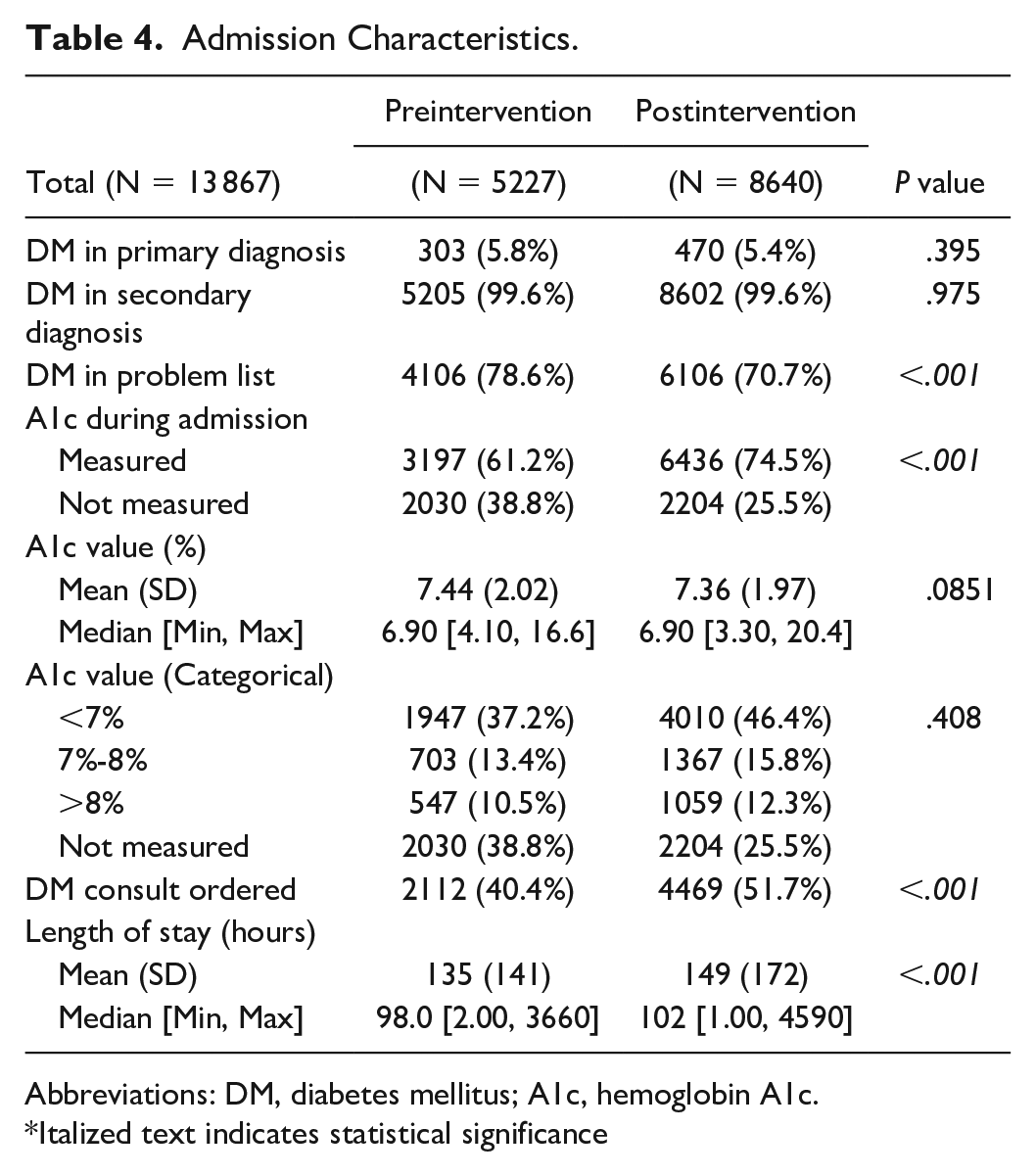
Abbreviations: DM, diabetes mellitus; A1c, hemoglobin A1c.
Italized text indicates statistical significance
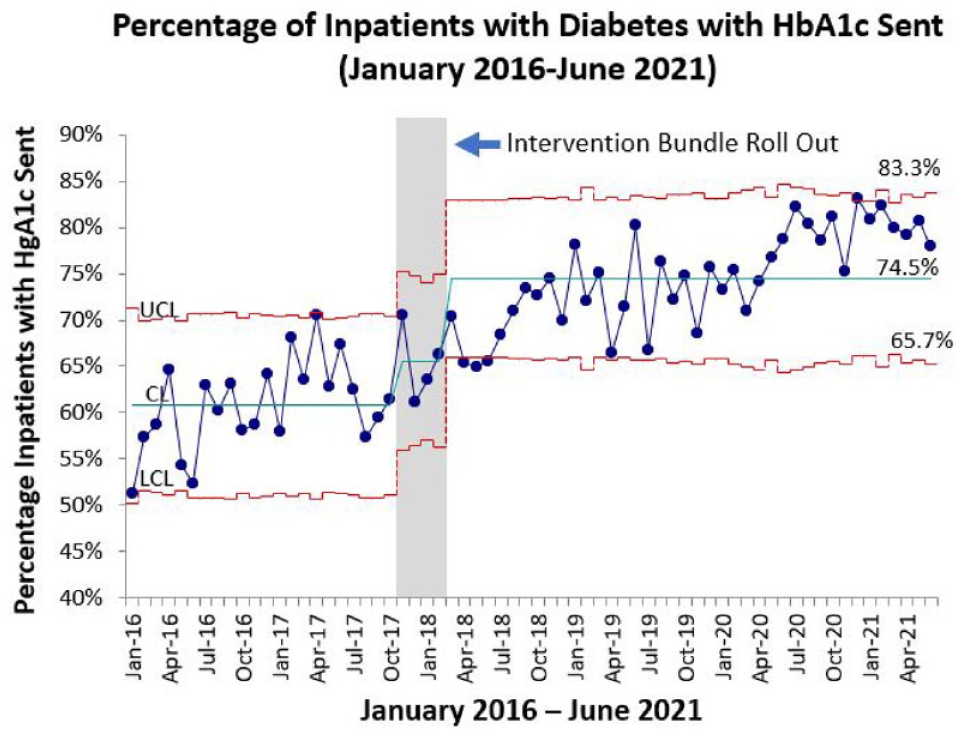
Control chart demonstrating the percentage of inpatients with diabetes who had A1c checked during hospitalization before and after the deployment of the intervention bundle. In the total cohort, preintervention only 61.2% of patients who met the criteria had an A1c measured. This increased to 74.5% of patients following rollout of the intervention bundle (P < .001). The green line is the center line (CL) and is equivalent to the mean. The red lines on either side of the mean are the upper and lower control limits (UCL and LCL); approximately 3 standard deviations on either side of the mean.
Interestingly, we also noted greater engagement with the diabetes consult service, with the percentage of patients with diabetes consults increasing from 40.4% preintervention to 51.7% postintervention (P < 0.001). The length of stay was also greater in the postintervention period (on average 135 hours preintervention compared to 149 hours postintervention, P < 0.001).
Discussion
Our study’s intervention bundle achieved a significant increase in the frequency of A1c testing for patients with diabetes admitted to a community hospital. Implementation of Lean Six Sigma to discover the root causes of the problem and standardize the processes and training allowed for efficient A1c ordering and reporting. Most striking was the sustained increase in the percentage of patients who had their A1c checked more than two years after the initial intervention bundle was implemented.
This differs from the only previous study identified that had been able to achieve a statistically significant increase in inpatient A1c measurements. 13 Dulipsingh et al had been able to achieve this through physician education and also noted a reduction in hypoglycemic and hyperglycemic events. 13 These improvements were, however, not sustained on follow-up, and the study included only 144 patients during their two-month intervention and three-month follow-up, whereas ours included 13 867 over several years. Our study differs in our detailed, multifaceted approach to quality improvement with Lean Six Sigma, proving that for improvement to be sustained, several synergistic measures need to be adopted simultaneously.
This project was also unique in its setting in a community hospital, rather than in a large academic center, from where most previous studies evaluating quality-improvement methodologies have been published. Indeed, most patients in the United States receive care in the community hospital setting as opposed to large academic centers according to the Association of American Medical Colleges. 14 We also noted greater attention to diabetes management, reflected by the increase in proportion of patients who were seen by the inpatient diabetes management service. Unexpectedly, we also noted an increase in the length of stay after the intervention. Although this may be a result of additional time required for glycemic management above and beyond the time the patient needs to recover from their primary illness, the more likely explanation for this is that a good portion of the postintervention period spanned the time following the onset of the COVID-19 pandemic. As a result of elective procedures being canceled and overall greater disease burden of patients, healthcare resources were stretched, presumably leading to an increase in length of stay.
Lean Six Sigma has been utilized across the healthcare sector to reduce time, costs, and patient errors. Most of the studies looking at the impact of Lean Six Sigma have centered around cardiology, surgical, and radiological subspecialties. 10 To our knowledge, only two previous studies have looked specifically at improving diabetes management: one targeting outpatient collaboration between primary care providers and specialists 15 and the other focused on inpatient insulin delivery. 16 We observed that this multifaceted, holistic approach involving provider education, changes in the laboratory protocol, and updates to the EHR interface allowed for not only a significant increase in the frequency with which A1c measured but also perhaps, more importantly, a sustained change. The sustainability is likely a reflection of the permanency of the system-wide changes made to streamline electronic ordering and laboratory turnover. However, this approach is more intensive than other quality-improvement endeavors and requires more investment from leadership.
A limitation of this project is that it was restricted to one institution, and therefore, the generalizability of the results remains unclear. For example, most patients in our study population were above the age of 65 years. However, our study demonstrates the feasibility of implementing quality-improvement interventions in the community hospital setting using Lean Six Sigma. Another limitation is the inability to determine if the change reflects the strength of any one intervention over another in the bundle. For example, the value added by provider education to the overall result remains difficult to calculate independent of the changes to laboratory protocols and the EHR. It is also difficult to say whether the change was impacted by other confounding variables such as staff turnover. On the other hand, our study does reflect how a sustainable change often requires multiple simultaneous approaches for the resolution of all root causes of a problem, underpinning the value of the Lean Six Sigma method.
While the goal of this quality-improvement project was to increase the frequency of A1c measurements, there was no statistically significant reduction of A1c levels over time. The authors believe that this metric may not apply to this particular study as patients are typically hospitalized for a short time and any change in A1c is still largely dependent on factors affecting outpatient glycemic control that were not directly targeted in this study. Additional research is needed to determine whether such systemwide changes can impact outpatient diabetes management as well.
The timeliness of A1c measurement (earlier in the admission vs later) was not assessed, and the apparent increase in length of stay we observed may have been offset if measures had been taken to engage the diabetes management team earlier in admission for patients with a known history of diabetes. This remains an area for future research. In addition, data on the ethnicity of patients were not available at the time of that analysis.
The guidance for measuring A1c in the hospital is still largely based on the consensus opinion, and the impact of increasing A1c measurement on inpatient glycemic control or outcomes after discharge has not been directly studied. A1c measurements have their limitations as they can be falsely low or high in the setting of acute illness (eg, recent blood loss), making it difficult to advocate for this “one-size-fits-all” approach. Nevertheless, inpatient A1c measurements have been shown to predict inpatient dysglycemia but may also predict poor clinical response in hospitalized patients such as increased need for renal replacement therapy in intensive care unit patients.2 -4 Various algorithms can incorporate recent A1c measurements into decision-making to guide best insulin-initiation strategies at admission 5 and formulate a comprehensive diabetes management plan at discharge encompassing adjustments to outpatient medications and appropriate timing of follow-up.6,7
Lack of awareness of guidelines for glycemic management in the hospital in general, and the utility of A1c specifically, is a significant barrier to achieving glycemic targets. Studies show therapeutic inertia, that is, failure to initiate or intensify therapy when it is clinically indicated, leads to suboptimal glycemic management of hospitalized patients.17 -20 Hyperglycemia in hospitalized patients is not only associated with increased morbidity and mortality but also with increased risk of hospital complications and cost.21 -25 Fear of hypoglycemia is frequently mentioned in the literature as a barrier to treatment intensification, 26 but having knowledge of the patients’ previous glycemic control by measuring A1c could help remedy this.
Finally, authors speculate that implementation of similar initiatives may also lead to the detection of patients with a previously unknown diagnosis of diabetes, thus adding to the improvement of diabetes care.
Conclusions
This novel approach was successful in improving adherence to the guideline-based measurement of A1c in hospitalized patients. This is the first quality-improvement project in a community hospital utilizing the Lean Six Sigma process for this purpose and may represent a valuable methodology for community hospitals to improve inpatient diabetes care.
Footnotes
Acknowledgements
Authors thank the members of the Glucose Steering Committee at Suburban hospital and the Johns Hopkins Biostatistics, Epidemiology, and Data Management (BEAD) Core.
Abbreviations
ADA, American Diabetes Association; A1c, hemoglobin A1c; DMAIC, define, measure, analyze, improve, and control; EHR, electronic health record; SIPOC, suppliers, inputs, processes, outputs, customers.
Declaration of Conflicting Interests
A.P.D. reports research funding from DexCom, Inc. M.Z. reports consulting for EMD Serono. These organizations had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The quality-improvement study has been acknowledged by the Johns Hopkins Institutional Review Board.