
Abstract

Keywords
Background
More and more patients with type 1 diabetes mellitus (T1D) are switching from sensor-augmented insulin pump therapy to an artificial pancreas system (automated insulin delivery [AID]) for various reasons. As there are no suitable approved AID systems in Austria until 2021, do-it-yourself systems (open-source AID) are increasingly being used. The question arises, “How glycemic control changes after the switch?”
Methods
This monocentric retrospective data analysis from 2019 to 2021 compared sensor-augmented pump therapy with the open-source AID system using ambulatory glucose profiles (AGPs) from 25 patients with T1D. An AGP was collected from each of the 25 patients with the following data: mean glucose (mean gl [mg/dL]), glucose variability (GV [mg/dL]), coefficient of variations (CV [%]), time in hypoglycemia <54 mg/dL (%), time in hypoglycemia <70 mg/dL (%), time in target range 70-180 mg/dL (TIR [%]), time in hyperglycemia >180 mg/dL [%], time in hyperglycemia >250 mg/dL (%), sensor tracing time (%), and glucose management indicator (GMI [%]). As all patients used the Dexcom G6 continuous glucose monitoring (CGM) sensor system, the AGP data were exported from the data of the diabetes management application “Dexcom Clarity.” The CGM data were analyzed between the period 2019 and 2021. Four weeks with sensor-augmented insulin pump therapy before the conversion (AGP 1) and four weeks with the open-source AID system (AGP 2) were analyzed. The average and standard deviation (SD) of AGP 1 and 2 were generated from all patients and significance testing was performed using the t test (Table 1).
AGP Data With Sensor-Augmented Pump Therapy (AGP 1) and Open-Source AID (AGP2).
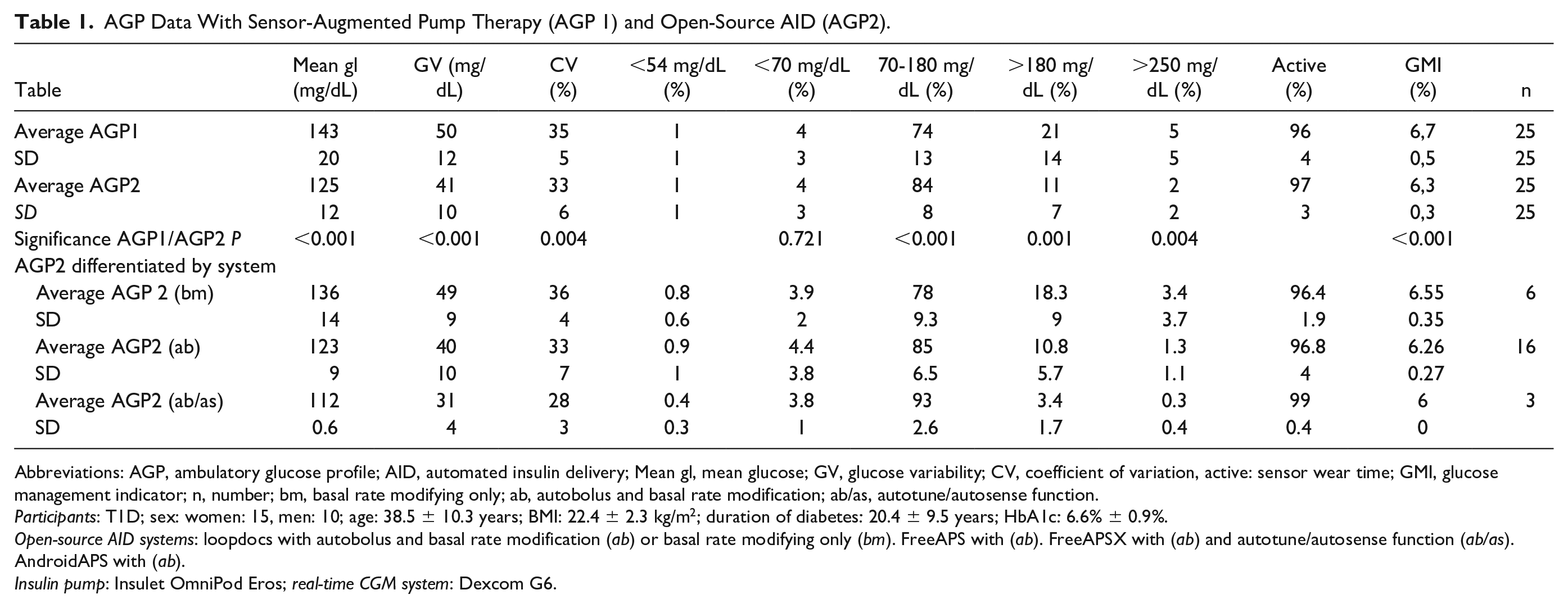
Abbreviations: AGP, ambulatory glucose profile; AID, automated insulin delivery; Mean gl, mean glucose; GV, glucose variability; CV, coefficient of variation, active: sensor wear time; GMI, glucose management indicator; n, number; bm, basal rate modifying only; ab, autobolus and basal rate modification; ab/as, autotune/autosense function.
Participants: T1D; sex: women: 15, men: 10; age: 38.5 ± 10.3 years; BMI: 22.4 ± 2.3 kg/m2; duration of diabetes: 20.4 ± 9.5 years; HbA1c: 6.6% ± 0.9%.
Open-source AID systems: loopdocs with autobolus and basal rate modification (ab) or basal rate modifying only (bm). FreeAPS with (ab). FreeAPSX with (ab) and autotune/autosense function (ab/as). AndroidAPS with (ab).
Insulin pump: Insulet OmniPod Eros; real-time CGM system: Dexcom G6.
Results
The comparison of AGP 1 and 2 (Table 1) shows a reduction of mean glucose from 143 mg/dL to 125 mg/dL (12%). Furthermore, glucose variability was reduced from 50 mg/dL to 41 mg/dL (22%) and CV decreased (6%). The TIR increased from 74% to 84% without changing the time in hypoglycemia. Time in hyperglycemia above 180 mg/dL and above 250 mg/dL decreased (47% and 60%). The glucose management indicator was reduced (6.7% to 6.3%, Δ0.4%). The respective SD of AGP2 parameters also showed a decrease between 2% and 60%, indicating smaller differences in AGP between patients with AID systems. In-between differences of the AID systems become apparent, analyzing AGP2 according to the systems function (ab), (bm), and (ab/as) (Table 1). The more advanced (ab/as) system was superior in relation to mean glucose (–17%), GV (–36%), and TIR (+19%) compared with the (bm) system. The time in the range with hypoglycemia below 54 mg/dL was reduced by 50% with the more advanced system (ab/as).
Conclusion
In conclusion, in this retrospective analysis of real-world data, an open-source AID system was able to obtain a significant improvement in glycemic control. The reduction of mean glucose and glucose variability is due to a significant decrease of values in hyperglycemia. In this retrospective data analysis, the open-source AID systems can be considered safe due to the lack of increase in hypoglycemia.
Matching the data of AGP1 and AGP2, the GMI can also be lowered, here as a substitute for the laboratory method of HbA1c value.
Looking at the AGP changes in relation to the different characteristics of the AID systems, there was an improvement in all AGP parameters with autobolus, autotuning and autosensing (ab/as) in this retrospective analysis.
As reported by Melmer et al, 1 in the herein conducted analysis the authors show an equivalent increase of 10% in TIR once switching from sensor-augmented pump therapy to an AID system. With an open-source AID system with basal rate adjustment, time in range improved by 6% in the literature. 2 Herein, we report 5% increase in TIR. With an autobolus open-source AID system, time in target can be increased by 11.3%, 3 which goes in line with the results of this data analysis.
Footnotes
Abbreviations
ab, autobolus and basal rate modification; ab/as, autotune/autosense function; AGP, ambulatory glucose profile; AID, automated insulin delivery; bm, basal rate modifying only; BMI, body mass index; CGM, continuous glucose monitoring; CV, coefficient of variations; GMI, glucose management indicator; GV, glucose variability; HbA1c, hemoglobin A1c; mean gl, mean glucose; SD, standard deviation; T1D, type 1 diabetes mellitus; TIR, time in range.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.