
Abstract
Background:
Since 2016, German health insurance companies reimburse continuous glucose monitoring (CGM) systems for persons with insulin-dependent diabetes, leading to a tremendous increase of CGM use. This study assessed the use of CGM, the satisfaction with, and the data analysis behavior among young people.
Methods:
During a diabetes camp for young people from all over Germany, participants anonymously answered a questionnaire on their method of glucose monitoring, satisfaction and quality of CGM use, HbA1c, and diabetes distress (Problem Areas in Diabetes Scale [PAID]-5).
Results:
A total of 308 participants (age 21.4 ± 3.5 years; 73% female; diabetes duration 10.1 ± 5.9 years) completed the questionnaire. Approximately, 25% used self-monitoring of blood glucose (SMBG), 46% intermittent-scanning continuous glucose monitoring (iscCGM), and 30% real-time continuous glucose monitoring (rtCGM). Mean HbA1c was slightly, but not significantly, higher among SMBG users compared with CGM users (8.0% ± 1.9% vs. 7.7% ± 1.4%; P = .791). Diabetes distress was not associated with the method of glucose monitoring (SMBG 5.6 vs. iscCGM 6.2 vs. rtCGM 6.5; P = .386). Overall, satisfaction with CGM use was very high; 98% of the CGM users reported better well-being with CGM compared with previous SMBG use. Only 19% of CGM users reported regular data analyses; their HbA1c was lower compared with other CGM users (7.2% ± 1.2% vs. 7.7% ± 1.4%; P = .039).
Conclusions:
In this large sample of young people, 75% were using a CGM system. Treatment satisfaction was very high, but CGM use was not associated with reduced diabetes distress or better glycemic control. However, young people who regularly analyzed their CGM data reported lower HbA1c levels.
Introduction
The use of modern technologies for diabetes management is increasing tremendously in Germany ever since the approval of free access to continuous glucose monitoring (CGM) systems in 2016 for all individuals with insulin therapy. Furthermore, 53% of children and adolescents with diabetes use sensor-augmented pump therapy and about 80% tried it at least for one day. 1 The positive impact of CGM use has been reported on clinical outcomes such as HbA1c,2-8 glycemic variability, 9 time in range, 10 and hypoglycemia-related endpoints.6,7,11-13
While glycemic control is the main goal of diabetes management, treatment satisfaction is also important when assessing the impact of CGM use on living with diabetes. A high level of satisfaction with CGM use was shown in various clinical trials13-15 and qualitative studies,16,17 especially in patients with a high risk of hypoglycemia. However, most of these studies focused on adults with diabetes or parents of children with diabetes. Surveys of adolescents and young adults are still rare.
This is disconcerting as young people are a patient group with poorer metabolic control18,19 and with special needs and interests. Adolescents and young adults face unique challenges such as taking responsibility for their health, separating from their parents, and planning their future life. Moreover, they seek new experiences with a spontaneous and autonomous lifestyle, which is often difficult to combine with the efforts of the diabetes management, which requires constant self-reflection and self-controlling behavior. 20
The challenging demands of diabetes and its management could result in high diabetes distress and risk for psychological disorders. A recent meta-analysis reported that approximately 30% of children and adolescents with diabetes had symptoms of depression and anxiety. 21 Furthermore, 30% of adolescents with diabetes reported significant diabetes distress. 22 Although these mental health issues were mostly subclinical, they were associated with short- and long-term poor adherence to treatment, poor glycemic control, and low health-related quality of life.21-23
Continuous glucose monitoring systems may be considered as a helpful tool and may reduce diabetes distress in young people,24,25 but can also have adverse effects26,27 because of sleep disturbances or feeling of permanent control. The benefit of CGM use is also influenced by several factors such as age, 2 level of education, 28 and continuity of sensor use.6,29 However, these factors have not been previously examined in the youth population. Therefore, the aim of this cross-sectional study was (1) to assess how young people use CGM systems in their daily lives, (2) to determine treatment satisfaction of CGM users, (3) to investigate metabolic control and diabetes distress in CGM users compared to self-monitoring of blood glucose (SMBG) users, and (4) finally, to assess HbA1c levels in those who regularly analyze CGM data compared with other users.
Methods
The study was a cross-sectional study conducted in a nationwide diabetes youth camp in Germany (Camp D) in 2018. Participation in the four-day camp was open to all interested young people with diabetes from the age of 16. The purpose of the camp was to encourage young people with diabetes to lead a self-determined and active life through shared activities, such as sports and camping. Health care professionals and peers with diabetes also provided a wide range of workshops about different topics of daily life with diabetes. The camp was publicized on social media, support groups, diabetes centers, and diabetes practices. The event was organized by a pharmaceutical company and supported by nationwide patient organizations, the state of Schleswig-Holstein, and many volunteer diabetes professionals.
Participants and Procedures
All 371 young participants of the 2018 camp were invited to visit the study center at the event site and participate anonymously in the study. They were informed about the study beforehand in the invitation letter to the camp. For the young people under 18 years of age, a consent form for participation was enclosed, which was to be signed by their parents. The questionnaire was handed out in paper form. Participant placed the completed questionnaire in a sealed box. All participants older than 18 years gave verbal and written consent.
The study was approved by the ethics committee of Hannover Medical School, Germany (Nr. 7940_BO_K_2018) and in accordance with the Declaration of Helsinki. This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. 30
Questionnaire
Sociodemographic data
The questionnaire assessed demographic information (age, sex, country of birth, and highest level of education) and clinical data (type of diabetes, diabetes duration, type of insulin therapy, method of glucose monitoring, last HbA1c, and number of severe hypoglycemia during the last 12 months, also see Table 1).
Sample Characteristics, Clinical Data, and Diabetes Distress by Method of Glucose Monitoring.
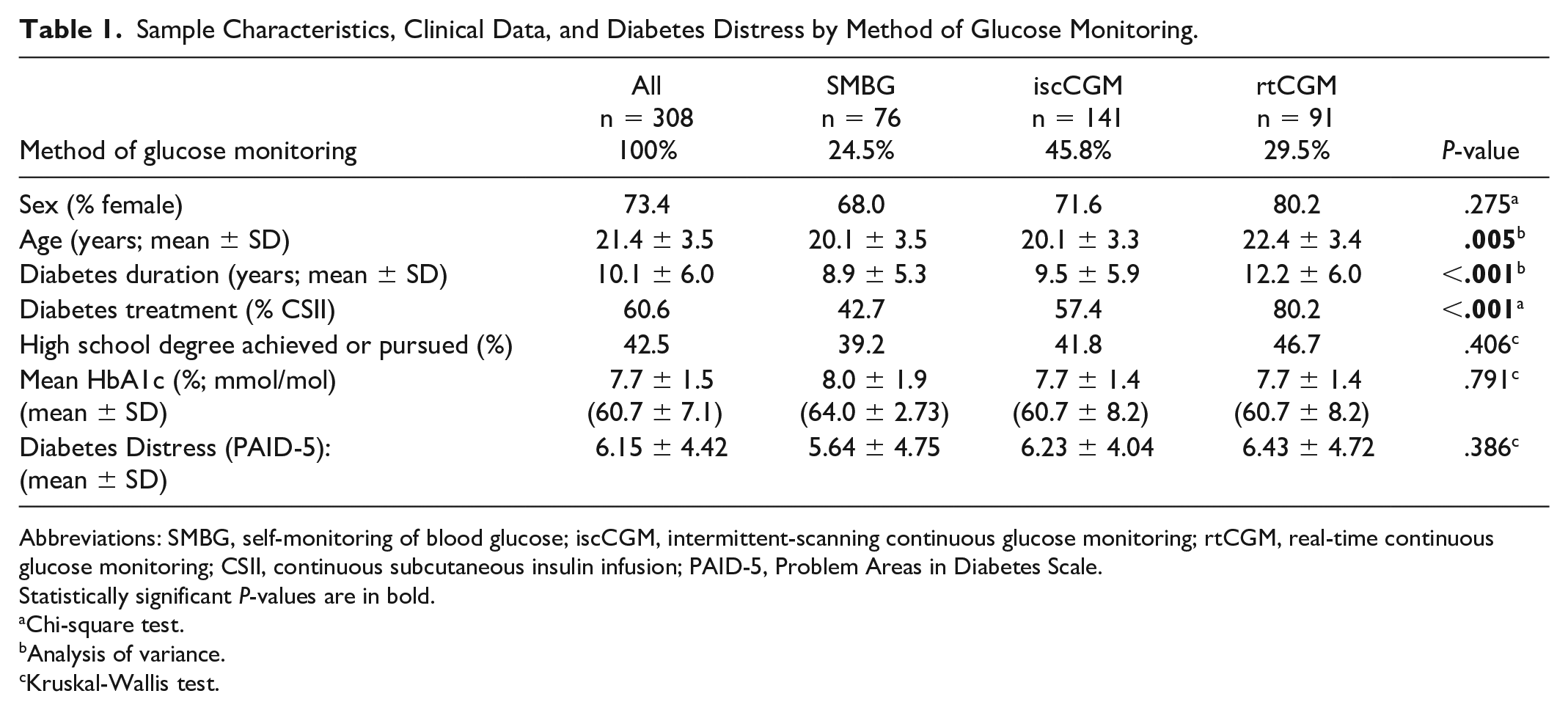
Abbreviations: SMBG, self-monitoring of blood glucose; iscCGM, intermittent-scanning continuous glucose monitoring; rtCGM, real-time continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; PAID-5, Problem Areas in Diabetes Scale.
Statistically significant P-values are in bold.
Chi-square test.
Analysis of variance.
Kruskal-Wallis test.
Method of glucose monitoring
One question was designed to ask for the method of glucose monitoring (CGM use or no CGM use) and one question for the monitoring system in use: intermittent scanning CGM system (iscCGM) versus real-time CGM system (rtCGM).
Diabetes distress
Diabetes distress was assessed using PAID-5,31,32 a short form of the Problem Areas in Diabetes Scale (PAID). 33 The five items included questions on feeling scared or depressed by living with diabetes, worrying about diabetes-related complications, diabetes taking too much physical and mental energy, and coping with complications. Answers were given on a 5-point Likert scale. Sum scores range from 0 to 20, with higher scores representing higher diabetes distress; and sum-scores >7 indicate diabetes distress that needs further examination. 32
Treatment satisfaction
Satisfaction with the use of CGM systems was assessed by a questionnaire developed and validated for the use of new technologies. 34 The questionnaire consists of 10 items focusing on satisfaction and comfort (eg., impact on overall well-being, feeling of security). Furthermore, the questionnaire includes items on trust in the system and gain of important new information due to CGM use (see all items in Table 2). The items were answered on a 5-point Likert scale, with higher scores indicating a higher degree of satisfaction. The questions on CGM use were only answered by those using any CGM system.
Satisfaction with CGM use by iscCGM users and rtCGM users.
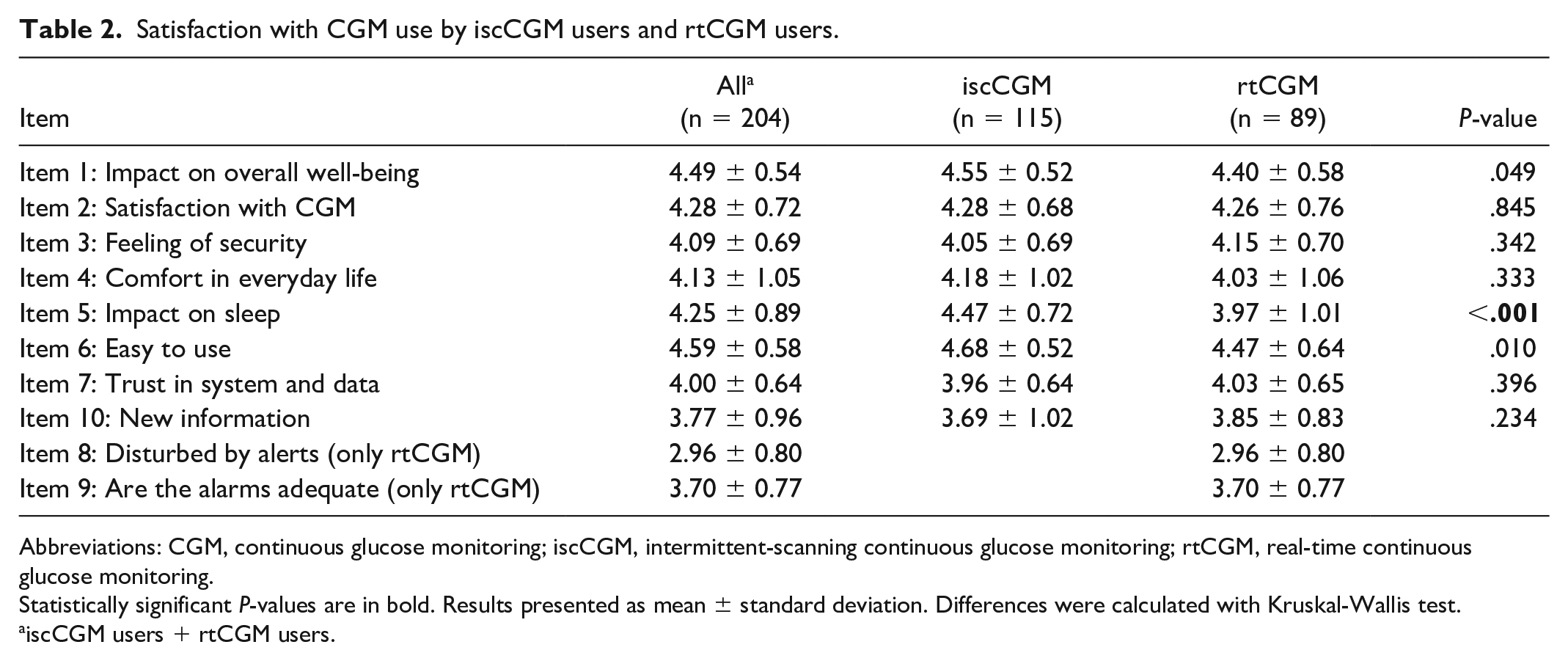
Abbreviations: CGM, continuous glucose monitoring; iscCGM, intermittent-scanning continuous glucose monitoring; rtCGM, real-time continuous glucose monitoring.
Statistically significant P-values are in bold. Results presented as mean ± standard deviation. Differences were calculated with Kruskal-Wallis test.
iscCGM users + rtCGM users.
Data analysis behavior
Quality of CGM use was assessed by asking participants about their CGM data analysis strategy in everyday life. For response categories were given: regularly on my own, sometimes on my own, merely at my diabetologist, or no data analyses.
Statistical Analyses
All analyses were performed using the statistical software package IBM SPSS Version 25 (SPSS Inc., Chicago, Illinois, United States). Descriptive statistics are presented as frequencies, mean values (M) and standard deviations (SD). Differences between groups regarding categorical variables were analyzed with a chi-square test, and bivariate analyses were performed using a Mann-Whitney U test or Kruskal-Wallis test for non-categorical variables that did not meet the assumptions of the parametric test. To test whether variables’ distribution departs significantly from normality, Shapiro-Wilk test was performed. A two-sided level of P < .05 was considered significant. Bonferroni correction was used to counteract the problem of multiple comparisons for the nine individual comparisons concerning satisfaction with CGM use. Multiple linear regression was used to estimate the influence of diabetes duration, age, diabetes distress, sex, and method of glucose monitoring on HbA1c. Confounders were added simultaneously to the model and modeled as linear, except for sex (female/male), and method of glucose monitoring (SMBG/rtCGM/iscCGM).
Results
Sample
Of the 371 visitors of the camp, 308 young people agreed to participate in the study (83% response rate). The demographic and clinical characteristics of the young people are shown in Table 1. The mean age of the young people was 21.4 ± 3.5 years, 73% female. Male participants were slightly younger than females (20.50 ± 3.11 years vs. 21.7 ± 3.51 years; P = .007). Forty-three percent of the participants already had or were pursuing a high school degree. This rate is similar to the German background population data in 2018 (40%). 35 The majority of participants (94%) were born in Germany, and of which 83% reported both parents were of German origin. Compared with the German background population data, the proportion of young people with a migration background was lower in this sample (32% and 17%, respectively). 36
A total of 61% used an insulin pump (continuous subcutaneous insulin infusion [CSII]) and the other 39% used multiple daily injections.
Method of Glucose Monitoring
In addition, 24% used SMBG, while 46% used iscCGM and 30% used an rtCGM (see Table 1). Insulin pumps were used more frequently by rtCGM users (80% rtCGM vs 57% of iscCGM users and 43% of SMBG users, P < .001).
Mean age was significantly different between SMBG, rtCGM, and iscCGM users (P = .005), indicating that rtCGM users were slightly older than the others. Diabetes duration was also different between the three groups (P < .001), and those using rtCGM seem to have longer mean diabetes duration.
Glycemic Control
Self-reported mean HbA1c was 7.7% ± 1.5% (60.7 ± 7.1 mmol/mol). The therapy target of HbA1c <7.5% (58 mmol/mol) was reached by 55% according to the guideline recommendations 2018. 37
Multiple linear regression with HbA1c as the dependent parameter showed that age (P < .001), diabetes duration (P = .033), and diabetes distress (P < .001) were significant predictors, such that higher distress, younger age, and longer diabetes duration predicted a higher HbA1c level. However, these parameters explain a small amount of the HbA1c variance (corrected r2 = 0.094). No significant influence was found for sex (P = .063) and method of glucose monitoring (P = .207).
Severe hypoglycemia during the last 12 months was reported by 6% of the participants.
Diabetes Distress
The mean diabetes distress assessed by PAID-5 questionnaire was 6.15 ± 4.42. Female participants reported a higher level of distress than their male counterparts (6.72 ± 4.45 vs. 4.57 ± 3.94, respectively, P < .001). There were no significant differences in diabetes distress based on the type of glucose monitoring (SMBG 5.64 ± 4.75 vs. iscCGM 6.23 ± 4.04 vs. rtCGM 6.43 ± 4.72, P = .386).
Overall, 35% of the young people had a sum score of eight or higher indicating an elevated level of diabetes distress. The proportion of highly distressed participants was independent of the type of glucose monitoring (P = .823).
Satisfaction With CGM Use and Analysis Behavior
Of 232 young people using a CGM system, 204 answered the questions regarding the CGM use and their satisfaction with the system (88% response rate, 75% female).
Overall, the participants were highly satisfied with their system, and 98% reported better well-being with CGM compared with previous SMBG use. Data on the satisfaction with CGM use are shown in Table 2. The only small but significant difference between those using a rtCGM system and those with an iscCGM system relates to disturbances by alarms during night time (impact on sleep rtCGM 3.97 ± 1.01 vs. iscCGM 4.47 ± 0.72; P < .001).
Regular self-reliant analyses of CGM data were reported by 19% of the participants. Further 31% answered that they sometimes analyzed their CGM data, 38% analyzed their data only at their diabetes out-patient unit, and 12% never analyzed the data. Mean HbA1c was significantly lower in those analyzing CGM data regularly on their own compared with the other groups combined (7.2% ± 1.2% [55.19 ± 10.38 mmol/mol] vs. 7.7% ± 1.4% [60.66 ± 8.2 mmol/mol], respectively; P = .039). There were no differences in terms of sex (P = .821), diabetes duration (P = .130), school degree (P = .431), and diabetes distress (P = .153) between the regular analyzers and the other groups combined. Only the age was significantly higher in those analyzing data regularly (23.2 ± 3.4 years vs. 21.3 ± 3.4 years; P = .02).
Discussion
Around 20 months after reimbursement of CGM systems for patients with insulin-dependent diabetes in Germany, a large group of young people answered a questionnaire on their experience with this technology, their satisfaction with their CGM systems, and their habits concerning data analyses.
In this sample, the rate of female participants is very high compared to the German background population with Type 1 diabetes, where gender ratio is balanced. 38 This may reflect the higher interest of young women in self-help activities. In addition, the number of young people from a migrant background is low.
Compared to the slowly growing number of young people using an insulin pump in Germany, CGM rapidly became the standard in this age group.1,38 Almost three-quarters of the participants used CGM systems, which is higher than in the representative diabetes population, where around 50% used CGM in this age group. 38 CSII was used by around 60% of the participants, which is slightly higher compared to the background population. 38
The willingness to use CGM systems is promoted by the coverage of costs by the health insurance companies in Germany, which is supported by the tremendous increase in CGM use since 2016. 38 But other factors also play a role: our data suggest that increasing age and diabetes duration were reflected in a higher rate of technology use, which may be because it is common to start glucose monitoring with SMBG and change to CGM under certain circumstances, for instance a hypoglycemia unawareness. 39 These data go along with data from the T1D Exchange registry (T1DX) and the German/Austrian diabetes patient registry (DPV) that show a drop in CGM use among adolescents. 40 Reasons may be concerns of body image, feeling of permanent control, or first experiences of sexual intimacy. 41
With the implementation of CGM systems, improvements concerning metabolic control, treatment satisfaction, and quality of life were expected.2,42 However, the real-world data in this study showed no significant cross-sectional difference in HbA1c between those using a CGM system and those using blood glucose self-monitoring. These data are in line with longitudinal real-world data from DPV data for Germany/Austria and T1D Exchange for the United States. 43 There was also no significant difference in HbA1c between iscCGM users and rtCGM users. Our data, however, indicated a benefit of CGM systems on metabolic control as long as young people analyze their CGM data by themselves on a regular basis. Considering this, it is worrying to find that only one-fifth of the young people analyzed their data regularly and about 50% did not analyze their data self-reliantly.
Our findings do not show lower HbA1c values in CGM users compared with SMBG users, whereas data from the T1D Exchange Registry and the German diabetes registry do show better glycemic control in CGM users. In our sample, glycemic control is better than in the representative background population with Type 1 diabetes, 44 and differences between CGM users and SMBG users may not be detected. 40
It is likely that the time of transition where young people start to take more responsibility for diabetes care is especially vulnerable. Thus, young people may need more support to benefit from this technological progress. Recent studies have shown that this support can be provided by patient education and training. For example, the evaluation of the “structured training and treatment program for self-reliant rtCGM use” (German acronym: SPECTRUM) showed that the success of CGM use is influenced by user training in adults and adolescents.45,46 Not only did the SPECTRUM evaluation show an improvement in CGM-specific knowledge, practical skills, and comfort with CGM use, but also a slight improvement in HbA1c. 45 This shows that structured training can improve personal skills with technology use, and glycemic control, which is consistent with the findings in our sample that show lower HbA1c in those analyzing data regularly.
Independent of the metabolic control, almost all users were highly satisfied with their CGM system. They felt more secure, better informed about their metabolism, and less burdened. Continuous glucose monitoring can be used in many ways, for example, for short-term decisions that prevent time out of range, especially hypoglycemia, 47 but also for therapy optimization. The aspect that young people feel better informed, although regular data analyses are rare among them in this sample, may be due to the fact that they feel informed on a short-term basis in daily life for specific situations, but that structured analyses that reveal weaknesses in their long-term treatment may not be the focus of interest.
Negative aspects concerning satisfaction were related to disturbances by alarms, mainly during sleep. The results of our real-world data of a large sample of young people are similar to those of samples of older persons with diabetes that assessed satisfaction with CGM use under clinical conditions over time. 48 Both the clinical data among adults and adolescents and the real-world data suggest a high level of satisfaction and comfort with CGM use.
However, the use of CGM systems and the high level of satisfaction with them do not seem to go along with reduced diabetes distress. We found no significant association of CGM use and the level of diabetes distress. This leads to the idea that technology use does not increase distress in this age group, but also does not lead to a relief. However, it is possible that the PAID-5 questionnaire did not sufficiently capture the challenges that CGM users face in daily life (eg, permanent control, sleep disturbances).
Even though distress was low in our study sample, about one-third of the participants reported elevated diabetes-specific distress that needs further examination. Along with findings in a meta-analysis from Buchberger et al. 21 and Hagger et al., 22 our findings suggest that a large group of young people need more practical and psychological support. Technology may reduce some of the burdens, as treatment satisfaction is high, but it cannot address every aspect of living with diabetes such as future concerns and fear of severe complications. Some of the burdens may also be increased by technology use. For example, the large amount of permanently available CGM data may overwhelm the user, and permanent control may be experienced as a burden, especially in an age group that seeks independence. Further research is needed to examine interpersonal factors that may improve psychological well-being and clinical outcome through technology use. These studies would be essential for developing individually tailored treatment options to optimize young people’s technology use.
The current study has some important limitations. First, the cross-sectional observational study does not allow any conclusions on causal relationships to be made between different outcomes. Second, the camp participants are not a representative sample of young individuals with insulin-dependent diabetes. The majority were female, number of participants with migration background was low, diabetes fairly well controlled, and the participants of Camp D have registered themselves for this event. Thus, they may represent a sample with high interest in their diabetes management. Third, the participants self-reported their last HbA1c values measured at their last out-patient visit. Verification of these self-reported data was not possible due to the anonymous nature of the data collection process. Provided data are from summer 2018: due to fast development of diabetes technologies, new challenges and advantages may occur, for example, hybrid closed-loop systems, 49 which require further research.
Conclusions
A rapid and high acceptance of the new diabetes technologies was documented in an age group that is faced with many unique challenges in their disease management. A hint towards better metabolic control among the young camp participants is seen in those who actively and regularly analyze their data.
Even in this selected sample that may represent individuals with better glycemic control and high motivation toward disease management, the number of those analyzing data regularly is low. We assume that it is important to increase the number of those analyzing data regularly. Further research is needed in order to see which path leads us there, for example, whether training programs or psychological interventions have an impact on regular data analysis.
Footnotes
Acknowledgements
The authors thank all participants of this study.
Abbreviations
CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; DPV, diabetes patient registry; HbA1c, hemoglobin A1c; iscCGM, intermittent-scanning continuous glucose monitoring; PAID, Problem Areas in Diabetes Scale; rtCGM, real-time continuous glucose monitoring; SMBG, self-monitoring of blood glucose.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.H. has no conflict of interest; K.L. received honoraria from Chiesi, DexCom, Lilly, Medtronic, Menarini Berlin Chemie, MSD, NovoNordisk, Roche Diabetes Care, and Sanofi; M.J. and G.E. have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from “Förderstiftung MHHplus.”