
Abstract
Background:
Despite increases in continuous glucose monitor (CGM) and insulin pump use in adults with diabetes, there is room for expansion. Technology adoption may be influenced by the training environment and fellowship education. However, little is known about adult endocrinology trainee comfort with, understanding of, or methods by which trainees receive education about diabetes technology.
Methods:
Mixed methods, sequential explanatory evaluation using survey and semi-structured interviews of endocrinology trainees and fellowship leadership in Accreditation Council for Graduate Medical Education (ACGME)-accredited adult endocrinology fellowship programs to assess trainee and leadership comfort with, perceived knowledge of, and current methods for diabetes technology education.
Results:
Seventy-seven respondents completed the survey. The majority of training programs have curricula for training on insulin pumps (74%) and CGM (75.3%); 52% of fellows felt curricula are adequate. First- and second-year fellows were more comfortable with CGM than insulin pump use. Only half of third-year fellows felt comfortable with starting insulin pump therapy or recommending insulin dose adjustments based on CGM rate of change arrows. Qualitative interviews identified the importance of both direct instruction and experiential learning in diabetes technology education.
Conclusions:
Almost half of trainees feel that curricula for learning to use and manage insulin pumps and CGM are inadequate and feel uncomfortable with critical aspects of technology use, demonstrating the need for increased attention to trainee education in the use of diabetes technology. Based on a better understanding of current and preferred methods for instruction, this study provides direction for future development of initiatives to improve fellow education in this field.
Introduction
The prevalence of diabetes, including type 1 diabetes (T1D), is increasing.1,2 Use of diabetes technologies, specifically continuous glucose monitors (CGMs) and insulin pumps, is associated with improved health outcomes for people with diabetes.3-9 For this reason, consideration of diabetes technology use is now considered standard of care. 10 However, data from the T1D Exchange have demonstrated overall low rates of CGM use and slow growth in pump use over time. 11
With increasing evidence to support the benefits of diabetes technology, there is need for further expansion of its use. However, technology adoption may be influenced by the social contexts in which training occurs. 12 A study assessing pediatric endocrinology training on insulin pumps and CGMs reported that fellows were similarly comfortable with both types of technologies, but only around half of the respondents felt that they had adequate training. 13 However, little is known about adult endocrinology trainee and fellowship program leadership perception of training on diabetes technology or the current methods by which adult endocrinology trainees receive diabetes technology education. Evaluation and attention to training in diabetes technology is needed to adequately prepare fellows and facilitate increased use in clinical practice. Given the importance of fellowship training in developing skills for independent practice, we sought to assess current adult endocrinology trainee and program leadership comfort with, and perceived knowledge of diabetes technology, as well as current methods for teaching and learning about diabetes technology.
Methods
Ethical Approval
This study was reviewed and determined exempt by the Boston University Medical Center Institutional Review Board. Consent was obtained prior to completion of the survey and interviews.
Study Design
We conducted a mixed methods, sequential explanatory study comprising a cross-sectional survey followed by qualitative semi-structured interviews of adult endocrinology fellowship trainees and program leadership (program directors and associate program directors).
Setting and Participants
The survey was sent via e-mail to adult endocrinology program directors and/or program coordinators identified via the Accreditation Council for Graduate Medical Education (ACGME) listing for the 148 ACGME-accredited Endocrinology, Diabetes, and Metabolism fellowship training programs in the United States. Program directors or coordinators were asked to distribute the survey to their trainees and leadership for completion. The survey was administered anonymously and data were collected using Qualtrics (Qualtrics, Provo, UT), sponsored by the Boston University Clinical and Translational Science Institute. The survey was administered during August and September 2019 when trainees were early in their respective years of training.
The survey was adapted from a survey administered to pediatric endocrinologists and trainees. 13 The survey included 43 five-point Likert scale-based questions, eight yes/no questions, five free response questions, and nine demographic questions. Questions assessed comfort with and perceived knowledge of diabetes technology, as well as questions about educational resources. There were 27 questions on the use of insulin pumps and 17 questions on CGMs. Questions explored both technical and conceptual aspects of their use. The survey was reviewed for validity by an adult endocrinologist with a focused interest in the use of diabetes technology. An invitation to participate in a semi-structured interview to allow for enrichment and further understanding of the data was included in the survey. This invitation was not linked to participant responses to maintain confidentiality, and thus, generated a convenience sample of participants for qualitative interviews.
One-on-one, semi-structured interviews were conducted either in-person or over the phone using an interview guide that was created by the authors. The guide was created using a conceptual framework for technology education 14 and adult learning theories. 15 We sought to explore participants’ experiences and attitudes toward diabetes technology education. The interview guide was reviewed by an adult endocrinologist with experience in graduate medical education and interest in diabetes technology. Interviews were conducted by K.L.F. and K.L.M. during February and March 2020. Interviews were audio-recorded, professionally transcribed, reviewed for accuracy, and anonymized prior to analysis.
In an attempt to minimize the nonresponse rate, we recruited participants through e-mail invitation to program directors and/or coordinators with two e-mail reminders to participate over the two-month survey period. The survey was administered anonymously to reduce confidentiality concerns, and additionally, participants were incentivized to complete the survey and participate in the semi-structured interviews through entry into lotteries for $50 gift cards.
Data Analysis
Quantitative data from the cross-sectional survey were analyzed using SAS® OnDemand for Academics (SAS Institute, Cary, NC). All results are expressed as means and standard deviations for continuous variables and as relative percentages for categorical variables. Likert scale data were dichotomized with responses of “always” and “most of the time” categorized as “more than half the time,” and responses of “about half the time,” “sometimes,” and “never” categorized as “half or less of the time.” Fisher exact tests were used to assess differences between groups by fellowship year and between fellows and program leadership.
Thematic analysis of interviews was conducted in an inductive and deductive approach using procedures of grounded theory.16,17 An initial code book was developed from knowledge frameworks and learning theories.15,18 Team members (K.L.F., K.L.M.) independently reviewed and coded the first two transcripts. The team (K.L.F., L.B.D., K.L.M.) then met to discuss initial and additional codes and reach consensus on coding guidelines and a revised code book. Team members (K.L.F., K.L.M.) then applied the revised coding framework to interview transcripts and met to reach consensus on dominant themes.
Results
Demographics
Table 1 contains the demographic information for the 79 respondents who started the survey; 77 respondents completed the survey. There are 148 endocrinology fellowships in the United States with roughly 305 fellowship positions filled each year. 19 The survey response rate could not be calculated as the number of recipients is not known since it was sent to leadership for distribution, not all fellowships have an associate program director, and fellowship length varies between two and three years. Of the respondents, 63.2% were fellows and 35.4% were leadership. Forty-nine percent were from the Northeast, with the remaining distributed throughout the United States. Training program size was variable, the majority having between four and nine fellows.
Demographics.
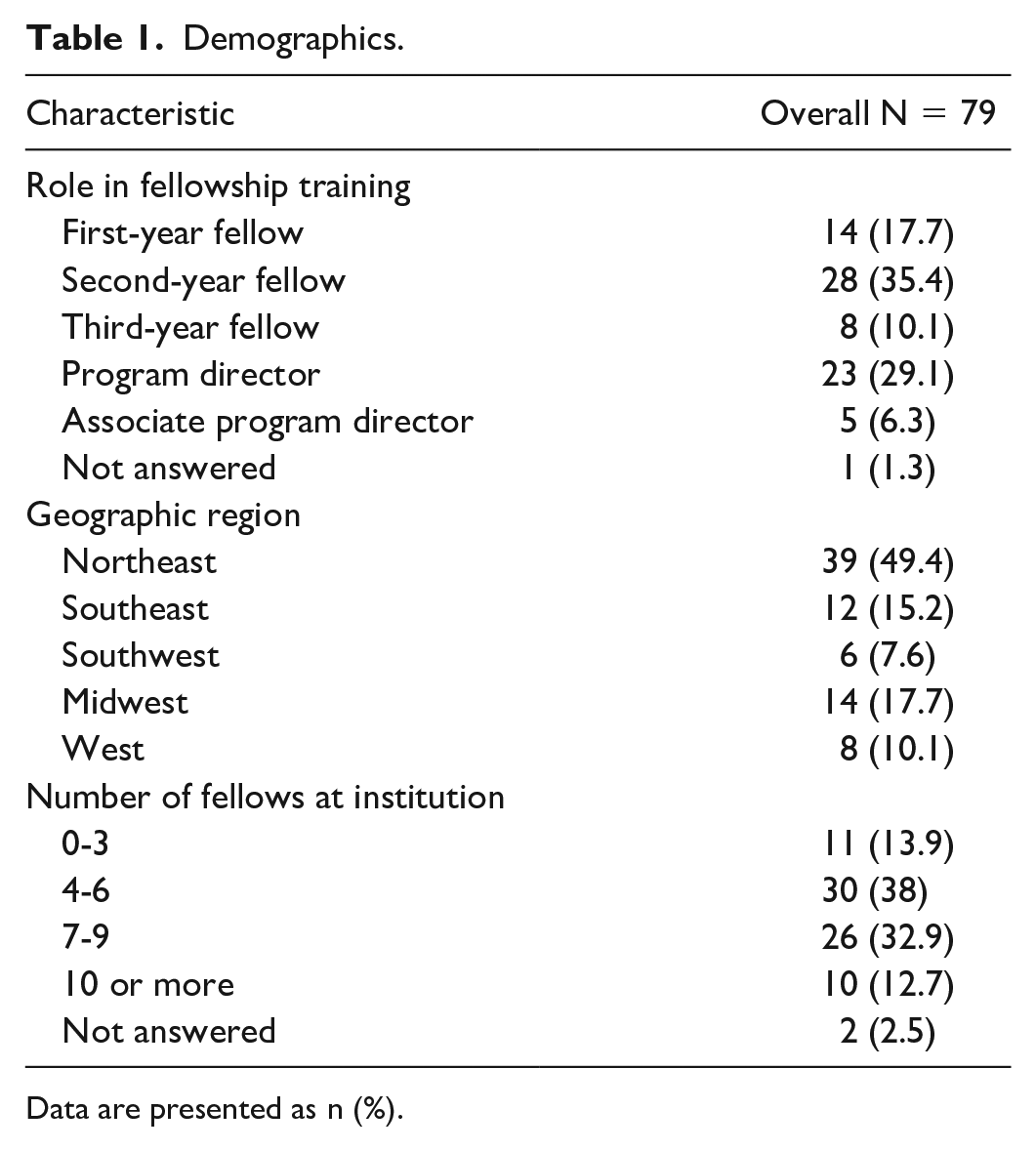
Data are presented as n (%).
Diabetes Technology Educational Practices
Of respondents, 74% and 75.3% reported having curricula for insulin pumps and CGM, respectively (Table 2). While not statistically significant, differences between fellow and leadership perception of educational practices were observed. When comparing fellow responses to leadership, a slightly greater percentage of leadership perceived there to be curricula in place. For insulin pumps, 70% of fellows reported a curriculum in place compared to 81.5% of program leadership (P = .41) and for CGM, 72% of fellows reported a curriculum compared to 81.5% of program leadership (P = .41). Despite most programs having diabetes technology curricula, only 54.5% of respondents felt that the curricula were adequate, with a similar percentage of leadership reporting this compared to fellows (59.3% vs 52%, P = 1.00). More fellows were interested in additional educational opportunities to learn about diabetes technology compared to leadership (82% vs 66.7%, P = .29). Response rates for questions about adequacy of diabetes technology curricula were lower than for other questions. Nearly all respondents felt that formal education (94.8%) and clinical exposure to diabetes technology (96.1%) were very to extremely important. The primary source for diabetes technology education was identified as endocrinology faculty members, followed by certified diabetes care and education specialists (CDCES) (48% and 35.1%, respectively) (Table 3).
Curriculum for Diabetes Technology and Adequacy.
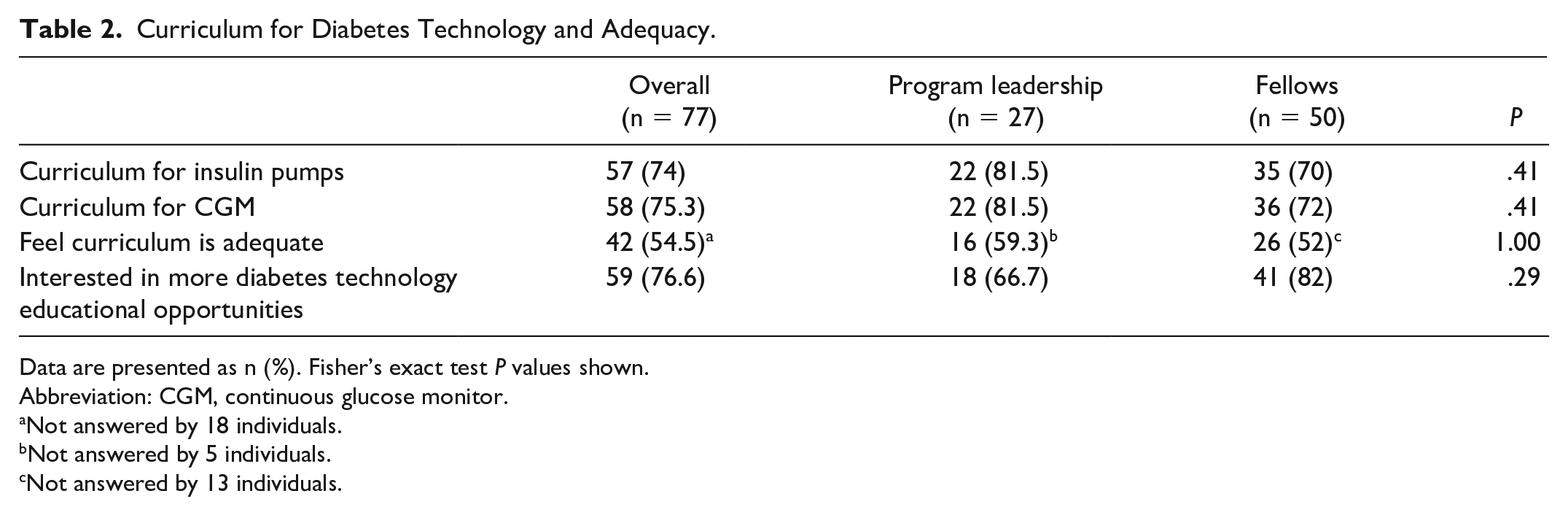
Data are presented as n (%). Fisher’s exact test P values shown.
Abbreviation: CGM, continuous glucose monitor.
Not answered by 18 individuals.
Not answered by 5 individuals.
Not answered by 13 individuals.
Source of Majority of Diabetes Technology Education.

Data are presented as n (%).
Abbreviation: CDCES, certified diabetes care and education specialists.
Comfort
Fellows were asked questions about their comfort with different aspects of insulin pumps and CGMs. Figure 1 demonstrates comfort stratified by year in fellowship. Comfort with nearly all aspects of diabetes technology use increased with more years in training. Comfort was lowest for starting insulin pump therapy. The largest increase in comfort seen was with starting patients on CGM, with only 46.2% of first-year fellows and 100% of third-year fellows feeling comfortable with this. Fellows were more comfortable with CGMs than insulin pumps at all stages in training.
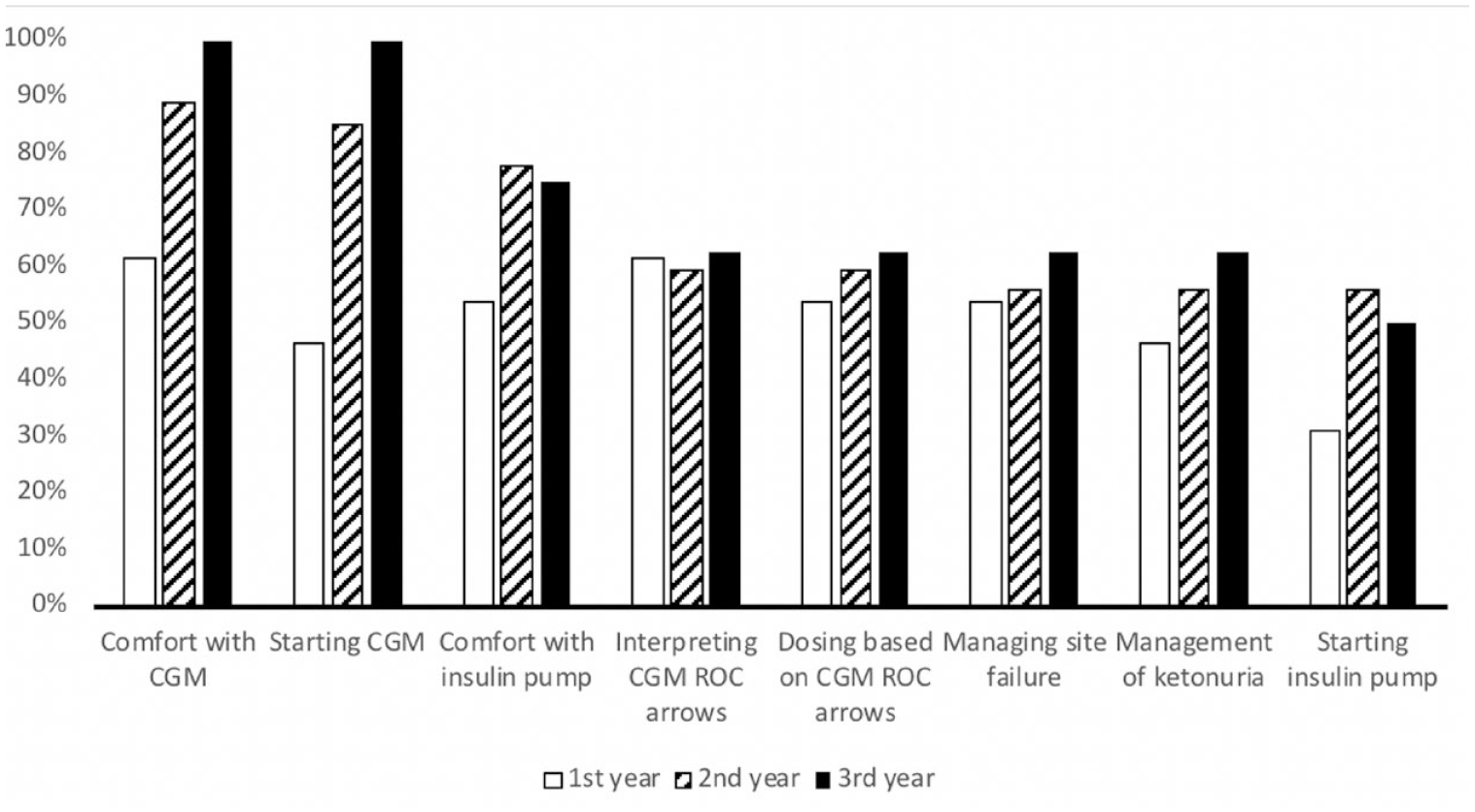
Comfort with diabetes technology by fellowship year.
Self-Perceived Knowledge
Self-perception of knowledge of diabetes technology was also evaluated (Tables 4 and 5). Similar to comfort, self-perceived knowledge about technology increased with more years of training for both insulin pumps and CGMs. With increasing years of training, a greater percentage of fellows in each year felt that they were able to counsel patients on the benefits of diabetes technology more than half the time, with higher rates for CGM than for insulin pump among first-year (76.9% vs 71.4%) and second-year fellows (88.9% vs 74%). Slightly lower rates were observed for counseling on the limitations of insulin pumps as compared to potential benefits among first-year (64.3% vs 71.4%) and second-year fellows (70.4% vs 74%).
Self-Perceived Knowledge About Insulin Pumps by Fellowship Year.
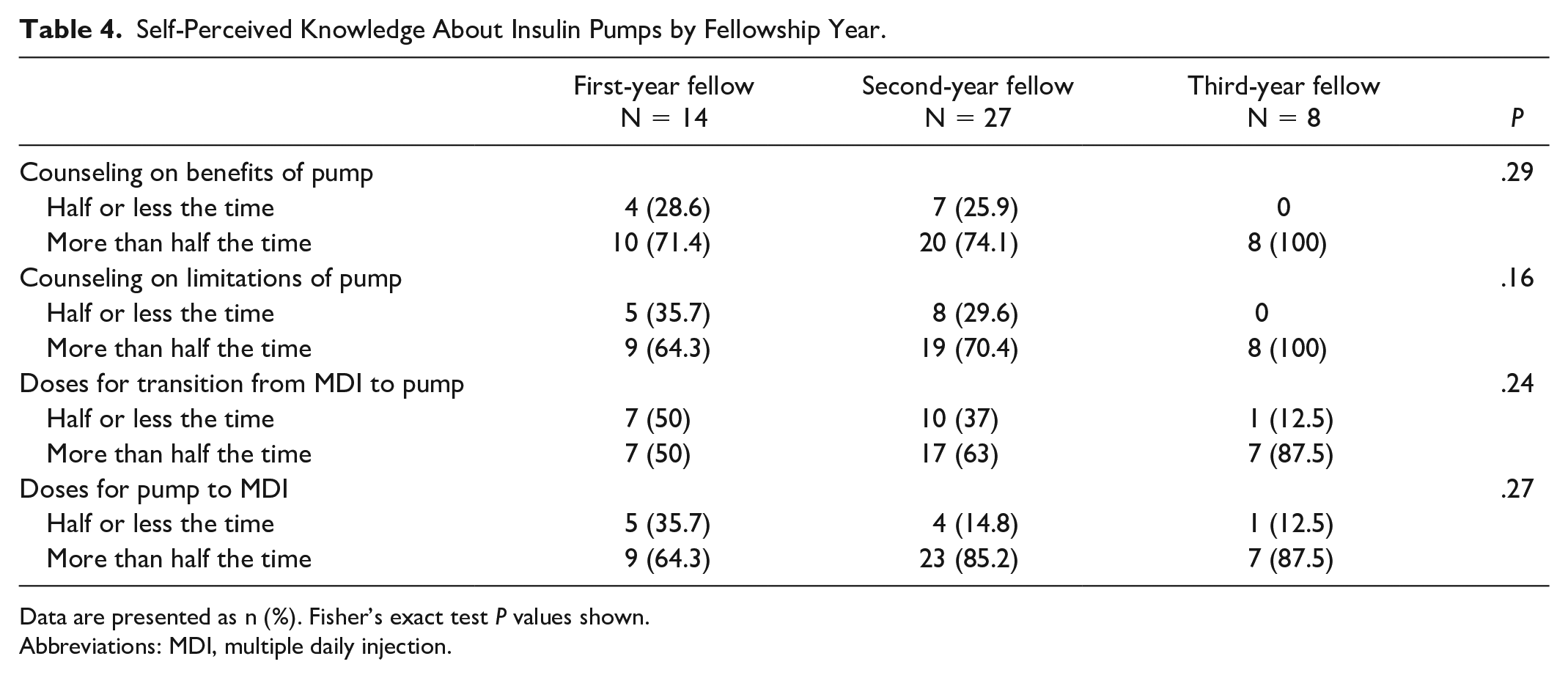
Data are presented as n (%). Fisher’s exact test P values shown.
Abbreviations: MDI, multiple daily injection.
Self-Perceived Knowledge About CGM by Fellowship Year.
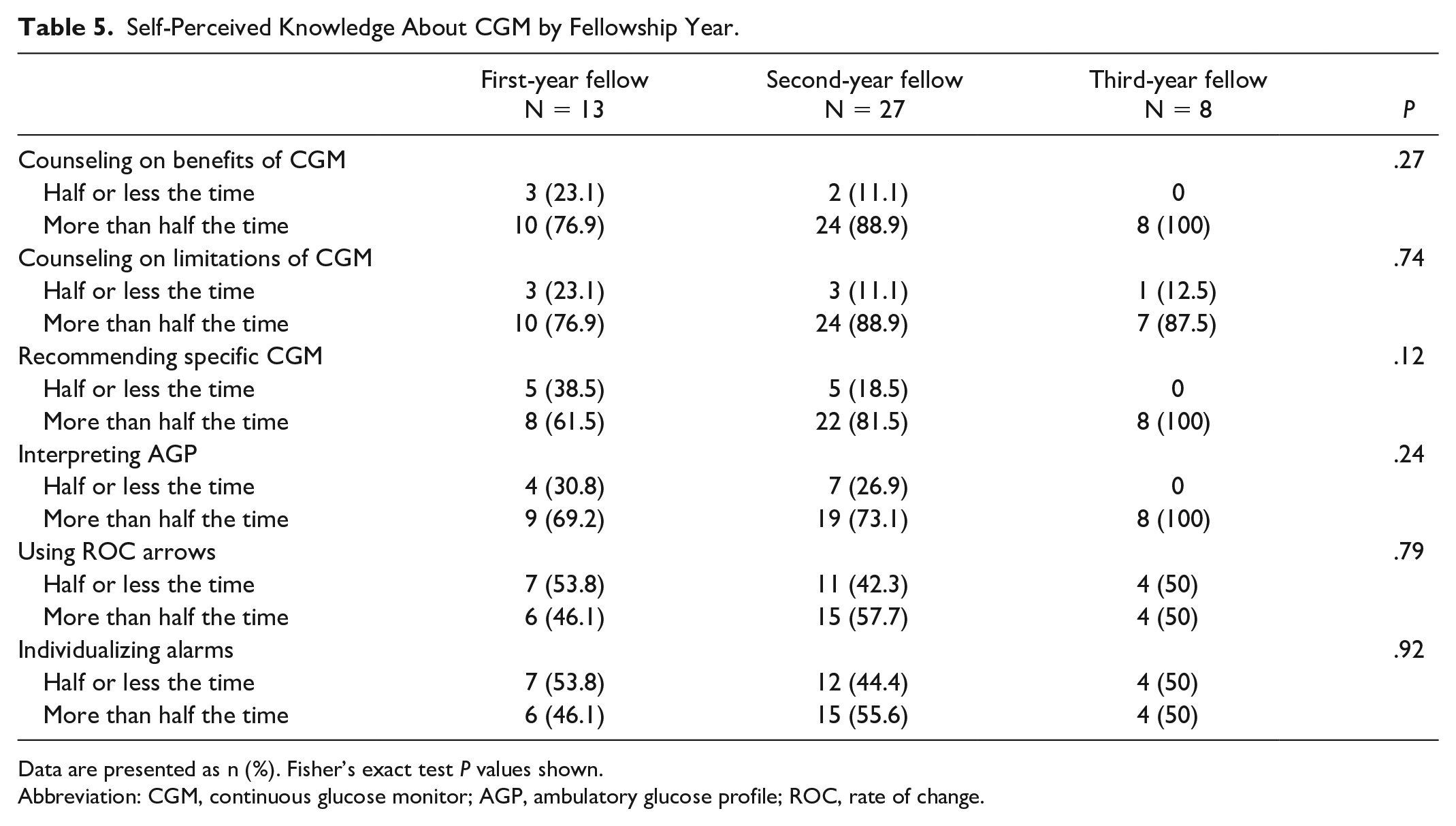
Data are presented as n (%). Fisher’s exact test P values shown.
Abbreviation: CGM, continuous glucose monitor; AGP, ambulatory glucose profile; ROC, rate of change.
Self-perception of knowledge about adjusting insulin dosing based on pump and CGM data also increased with more years of fellowship training. For insulin pump use, fewer than half of first-year fellows reported that they felt able to adjust basal rates, insulin to carbohydrate ratios (ICR), and sensitivity factors more than half the time. In the third year of fellowship, more than 70% of fellows reported feeling able to adjust pump insulin dosing more than half the time. Using glucose data from CGMs, less than half of first-year fellows felt able to adjust ICR or sensitivity factor more than half of the time, while 61.5% felt able to adjust basal rates more than half of the time, all of which increased by the third year of training. The only knowledge areas that did not universally improve with more years of training were understanding of rate of change arrows and alarm individualization for CGMs. Self-reported understanding of both of these more than half of the time remained near 50% across all three years of training.
Self-perceived knowledge of using diabetes technology in specific settings or specific features of technology was more varied but generally lower for first- and second-year fellows (Figure 2). A greater percentage of first-year fellows felt that they understood how to use diabetes technology in the setting of exercise and acute illness than second-year fellows (42.9% vs 40.7% for both), while all third-year fellows felt that they understood how to use technology in these settings.
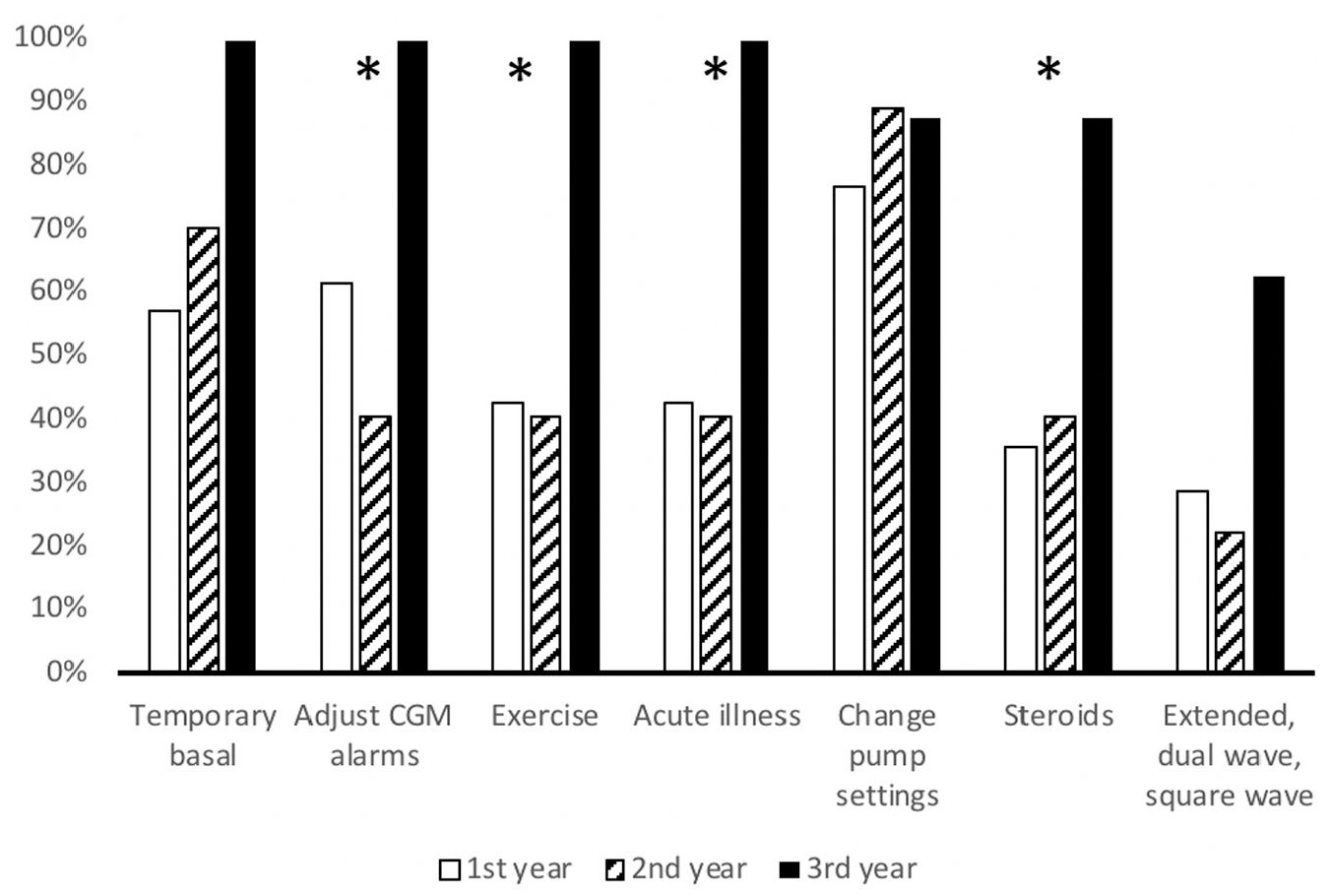
Self-perceived knowledge of specific technology features and settings.
Qualitative Analysis
Eleven semi-structured interviews were conducted, two with program directors (one in the Northeast and one in the Southwest) and nine fellows. Fellows were evenly distributed across years in training (three each in the first, second, and third years), 77.8% were women, 66.6% were at programs in the Northeast, with one fellow each from the West, South, and Midwest. All were training at programs in urban settings.
We identified the following six themes (Table 6): (1) direct instruction and experiential learning are common methods of instruction and were felt to best be used sequentially, (2) fellows highly value opportunities for experiential learning, (3) diabetes technology curricula were felt to be informal or absent and fellowship programs lack standardized means for fellow competency assessment, (4) institutional and programmatic factors may facilitate or serve as barriers to diabetes technology education, (5) fellows lack prior training related to diabetes technology, which influences their comfort and knowledge, and (6) volume of experience is important in development of comfort using diabetes technology in clinical practice.
Qualitative Themes and Illustrative Quotes.
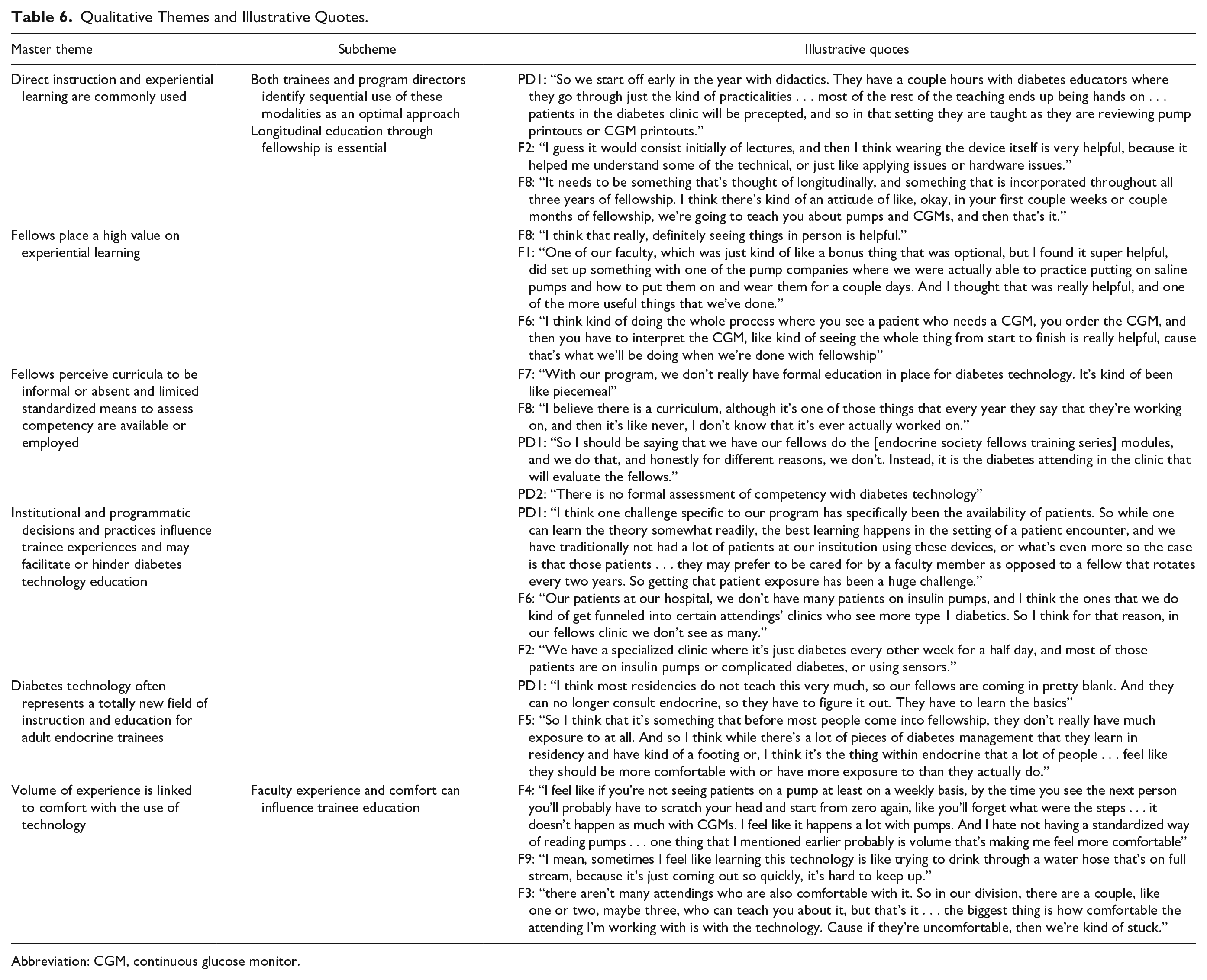
Abbreviation: CGM, continuous glucose monitor.
Both trainees and program directors identified direct instruction and experiential learning as common methods for education on diabetes technology. Experiential learning refers to the process wherein learners gain knowledge from participation in and reflection on experience. 20 Frequently, this refers to clinical experiences for postgraduate medical trainees. Sequential use of these modalities was identified as an optimal approach, and the importance of longitudinal education throughout fellowship was recognized by trainees. Fellows highly valued experiential learning, including the ability to wear devices themselves, as they felt this is what is required to prepare them for independent practice and better be able to navigate the technical aspects of managing patients using insulin pumps in particular.
Consistent with the quantitative data, trainees felt that curricula for diabetes technology were frequently informal or absent and therefore insufficient. Both trainees and program directors identified that a standardized way of assessing competency is lacking and that assessment for independent practice was made through evaluation of work in the clinic, where there may be limited exposure to technology.
As experiential learning is highly valued by trainees, a theme emerged identifying institutional factors and programmatic practices influencing trainee experience and serving as facilitators of and barriers to diabetes technology education. These factors, including patient population and insurance coverage, as well as “funneling” of patients using diabetes technology to specific faculty, largely impacted availability of patients from which trainees could learn in clinical settings.
Limited exposure to diabetes technology prior to fellowship was identified by both trainees and program leadership as influencing both knowledge and comfort. Diabetes technology is unique among other aspects of diabetes management as there is often limited exposure prior to endocrine fellowship training and trainees are required to rapidly learn both basic and complex knowledge and skills for clinical management of people living with diabetes using devices.
Fellows reported that comfort with technology use was directly related to volume of exposure. While conceptual knowledge was easier to retain, understanding technical aspects and interpreting downloaded data were difficult when specific devices were not seen frequently. Importantly, the impact of faculty comfort in use of diabetes technology was also identified as influencing trainee comfort with technology use.
Discussion
In our survey of endocrinology fellows and program leadership, while the majority of respondents reported having training in use of diabetes technology, only around half felt that training was adequate during fellowship. Although knowledge of technology and comfort with its use improved with more years of experience, gaps in knowledge remained. These findings were supported by our qualitative analysis, with increasing exposure leading to increased comfort and need for both direct and experiential learning emerging as dominant themes among both trainees and leadership, consistent with adult learning theories in medical education. 15
During endocrinology fellowship, trainees have two to three years to master a multitude of topics. While there is exposure to many areas of endocrinology during internal medicine residency, diabetes technology is not widely incorporated prior to fellowship. This creates a steep learning curve and makes it essential for fellows to gain experience using technology during fellowship, as they have only a short period of time to acquire knowledge before practicing independently. This is further complicated by the rapid pace of change of technology and potential lack of training or routine use of technology in faculty clinical practices. Additionally, not all faculty participate in fellowship curriculum development, which may create gaps if diabetes technology is not recognized as an area of importance or if faculty with this expertise are not involved in the fellowship program.
Most third-year fellow respondents felt comfortable with many aspects of technology use and perceived themselves to have reasonably high levels of knowledge about use of CGM and insulin pumps, answering that they were able to manage clinical scenarios or use specific features more than half the time. As our survey was distributed early on in the academic year, this suggests that fellows learn many aspects of the use of diabetes technology during the first and second year of training. However, comfort with important aspects of insulin pump use, including starting insulin pump therapy and managing infusion set failure and ketonuria, remained low even among third-year fellows, suggesting critical gaps in fellow education and areas for additional focus. Despite growing evidence for benefit of automated insulin delivery systems,21,22 low rates of trainee comfort with insulin pump technology and limited experience in fellowship training may hamper broad clinical adoption of this technology.
While fellows place a high value on experiential learning, access to clinical experiences to gain knowledge and develop expertise in the use of diabetes technology are not ubiquitous. This is particularly the case in adult endocrinology clinics at academic medical centers, which often care for a high proportion of publicly insured patients who have historically had variable insurance coverage for diabetes devices.23,24 Lack of access to CGMs and insulin pumps for patients or preferentially scheduling patients who already use these devices with faculty members rather than fellows may be detrimental to fellow education and the ability to increase trainee comfort with diabetes technology. Programmatic efforts to increase trainee exposure to patients using diabetes technology are needed to ameliorate this. While CGM use has historically been lower than insulin pump use in T1D Exchange data, 11 recent increases in the use of CGM may explain our finding that fellows and program directors both reported increased knowledge and comfort with CGMs compared to insulin pumps. It is yet to be seen if increased fellow comfort with CGM will translate to increased rates of CGM use in adults with diabetes.
Nearly half of respondents reported that education surrounding diabetes technology is provided by endocrinology faculty members, followed byCDCES. In our qualitative analysis, both fellows and program directors reported the need for direct instruction about diabetes technology, as well as experiential learning, and the sentiment that these are best used sequentially. Educational interventions based on the situated learning and guided participation model,20,25 in which trainees gain knowledge and skills through a series of workshops and clinical experiences in an apprentice-like fashion, 26 may be most beneficial to trainees and should be evaluated in future research to improve training in the field.
Fewer respondents answered questions about the adequacy of their program’s diabetes technology curricula than answered other questions. This may suggest fear of speaking negatively against one’s training program and should be further explored.
Strengths of our study include the mixed methods design with responses from both leadership and fellows in training from all regions of the United States and across all years of training. However, there are several potential limitations. The survey was sent to fellowship leadership and coordinators to distribute to fellows, so not all fellows may have received the survey and the sample size was small. Due to our method for survey distribution, it is difficult to calculate a true response rate, particularly as duration of training varies across different institutions. It is also possible that the responses may be skewed based on the distribution of the survey and raises the possibility of nonresponse bias in our results. Programs who felt it was important to address diabetes technology in their curricula may have been more likely to distribute the survey. Responses could also be reflective of programs with greater deficits surrounding a diabetes technology curriculum, which may have resulted in more fellows identifying deficits and desire for increased training, or conversely reflective of programs with an emphasis on diabetes technology education, thereby underestimating deficits. Respondents were also asked to voluntarily participate in the semi-structured interview process, so this group may have been self-selected as having more interest in diabetes technology education and may not be representative of all fellows or program leadership. Additionally, as interviews took place as the COVID-19 pandemic began in the United States, we were unable to complete interviews with all participants who initially showed interest in participation. This resulted in a smaller than desired sample size and as a result, we cannot confirm that we achieved thematic saturation. However, the findings from the survey and interviews were congruent and the use of triangulation in our study suggests the validity of our findings.
Conclusion
Despite near universal acknowledgment of the importance of formal education and clinical exposure to diabetes technology for adult endocrinology trainees, almost half of trainees feel that curricula for insulin pumps and CGMs are inadequate and feel uncomfortable with critical aspects of technology use, even after completion of two years of training. Our study identifies current methods by which adult endocrinology fellows are trained in the use of diabetes technology, preferred methods for instruction, highlights the need for additional attention and curricular development in this field, and provides direction for future development of education initiatives to improve fellow education.
Footnotes
Acknowledgements
The authors would like to thank Brynn Marks, MD, for graciously sharing her pediatric endocrinology diabetes technology survey tool and Poorani Goundan, MD, for reviewing our survey and interview guide for validity.
Abbreviations
ACGME, Accreditation Council for Graduate Medical Education; AGP, ambulatory glucose profile; CDCES, certified diabetes care and education specialist; CGM, continuous glucose monitoring device; MDI, multiple daily injection; ROC, rate of change; T1D, type 1 diabetes.
Authorship Confirmation Statement
All persons who meet authorship criteria are listed as authors and all authors certify that they have participated sufficiently. KLF, KLM, and LBD conceived in the design of the study. KLF and KLM acquired the data and completed data analysis, and KLF, KLM, and DWS interpreted the data. KLF and KLM drafted the manuscript. DWS and LBD revised the manuscript critically for important intellectual content. KLF, LBD, DWS, and KLM approved the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Boston University Department of Medicine Education Evaluation Core Pilot Grant