
Abstract
On March 23, 2020, all insulin products were reclassified as biologics instead of drugs under the Biological Price Competition and Innovation (BPCI) Act of 2009. This allows biosimilar insulin products to be manufactured when the patent expires for the reference biologic, sometimes called the originator or brand name product. A biosimilar product may not be substituted for the reference biologic at the pharmacy counter unless the biosimilar undergoes further switch trials to earn the designation as an interchangeable biosimilar. Insulin glargine-yfgn 100 units/mL is the first biosimilar insulin to attain interchangeable status with the reference insulin glargine. In the INSTRIDE 1 and INSTRIDE 2 trials, insulin glargine-yfgn has proven noninferiority regarding blood glucose reduction and adverse effect profile versus reference insulin glargine; even in the INSTRIDE 3 trial in which treatment of diabetes was switched between insulin glargine-yfgn and reference insulin glargine throughout the trial without statistically significant changes to glucose levels or adverse effects. Insulin glargine-yfgn may be substituted at the pharmacy counter without consultation with the prescriber, in accordance with state laws. In suit with other biosimilars, insulin glargine-yfgn’s list price is significantly lower than other insulin glargine products. This increases market competition leading to decreases in costs of other insulin glargine products. Many patients who could not previously afford insulin therapy may now have significantly improved access to treatment. Providers will need education to increase awareness of these new biosimilars and interchangeable biosimilar insulin products, cost benefits, and substitution allowances.
Introduction
On March 23, 2020, after a 10-year transition period, all insulin products were reclassified from drugs to
Biologics—Large, complex molecules made from living tissues that may contain slight variations of a protein that cannot be copied exactly. 3
Follow-on biologics—Copies of biologic products approved under the Food, Drug, and Cosmetic Act 505(b)(2) pathway. 1 This pathway was used before all insulins were re-categorized as biologics in March of 2020. A follow-on biologic is a version of the reference biologic which is produced by a different company than the original reference biologic. Follow-on biologics are not biosimilars or generics and cannot be substituted for the original reference biologic at the pharmacy counter. In order to switch from a reference biologic to the respective follow-on biologic, the prescriber must write a new prescription specifically for the follow-on biologic. 3 Examples of follow-on biologic insulins are Basaglar® (follow-on insulin glargine U100; Eli Lilly and Company, Indianapolis, Indiana) and Admelog® (follow-on insulin lispro U100; Sanofi-Aventis, Bridgewater, NJ).
Biosimilars—A biosimilar is a successor to a biologic that has lost patent exclusivity and has been approved under Section 351(k) of the Public Health Service Act pathway. “Highly similar to US licensed reference biological product notwithstanding minor differences in clinically inactive components, and for which there are no meaningful differences in terms of safety, purity, and potency.”5,6 Biosimilars are not automatically interchangeable with the reference biologic at the pharmacy counter unless they have achieved interchangeable biosimilar status. In order to change from a reference biologic to the respective biosimilar, the prescriber must write a new prescription specifically for the biosimilar medication. 5 An example of a biosimilar insulin is Semglee® (insulin glargine U100—without the 4 letters “yfgn” after glargine); it had status as a biosimilar for several months before acquiring status as an interchangeable biosimilar. An example of a noninsulin biosimilar is Inflectra® (infliximab-dyyb; Pfizer, New York, New York) as a biosimilar to the reference biologic, Remicade® (infliximab; Janssen Biotech, Inc. Horsham, Pennsylvania).
Interchangeable biologics—Biosimilar medications that can be automatically substituted for the reference biologic at the pharmacy counter without consulting the prescriber, much like a generic medication.1,3-5 Interchangeable biosimilars must meet additional requirements under the BPCI Act of 2009, and be proven to produce the same clinical result as the reference biologic in any given patient. 1 These additional requirements include crossover/switch studies consisting of patients switching back and forth between the biosimilar and reference biologic medication.1,5 Semglee® (insulin glargine-yfgn; Viatris [formerly Mylan] Morgantown, West Virginia) has become the first insulin to achieve interchangeable biosimilar status.
Authorized generic—With FDA approval, a brand manufacturer can also sell its own “generic” version without the brand name on the label. An example is Insulin Aspart as the authorized generic of Novo Nordisk’s NovoLog®.
Insulin glargine 100 units/mL (U100), known by brand name as Lantus® (reference insulin glargine; Sanofi-Aventis, Bridgewater, New Jersey), was the first long-acting insulin analog introduced to the United States (US) market in 2000. Sanofi’s patent on Lantus® (henceforth, referred to as reference insulin glargine) expired in 2015, allowing (after several legal battles) other manufacturers to explore development of “copycat” products. As of this publication, only 3 such products have been produced: Basaglar® (follow-on insulin glargine U100), henceforth, referred to as follow-on insulin glargine, in late 2016, Admelog® (follow-on insulin lispro U100) in late 2017, and now Semglee® (insulin glargine-yfgn U100) in August 2020.
Semglee® (Insulin Glargine-yfgn 100 units/mL)
Semglee® (henceforth, referred to as insulin glargine-yfgn) was developed by Biocon Biologics and is distributed by Viatris (formerly Mylan). 7 Insulin glargine-yfgn is a long-acting recombinant human insulin analog approved by the FDA as a biosimilar of reference insulin glargine on June 11, 2020. As simply a biosimilar, Semglee®’s nonbranded name is insulin glargine U100. But as an interchangeable biosimilar, a suffix has been added to the nonproprietary name; in this case, Semglee® is referred to as “insulin glargine-yfgn U100.” Insulin glargine-yfgn demonstrated identical pharmacodynamic and pharmacokinetic characteristics to reference insulin glargine. 8 Insulin glargine-yfgn demonstrated noninferior glycemic efficacy to reference insulin glargine in treatment of both type 1 diabetes and type 2 diabetes regarding the primary endpoint of hemoglobin A1c (A1c) change from baseline in the INSTRIDE 1 9 and INSTRIDE 2 10 trials, respectively.
INSTRIDE 1 9 was a multicenter, open-label, randomized, 52-week trial to primarily determine noninferiority of insulin glargine-yfgn versus reference insulin glargine, each given once daily along with insulin lispro at mealtimes, regarding change from baseline A1c at 24 weeks in patients with type 1 diabetes. At 24 weeks, mean A1c change was 0.14% (standard error [SE] 0.054; 95% confidence interval [CI]: 0.033, 0.244) for insulin glargine-yfgn and 0.11% (SE: 0.054; 95% CI: 0.007, 0.220) reference insulin glargine. At 52 weeks, the mean A1c change was 0.21% (SE: 0.055; 95% CI: 0.100, 0.306) for insulin glargine-yfgn and 0.25% (SE: 0.056, 95% CI: 0.144, 0.363) for reference insulin glargine. Noninferiority was determined with minimal differences between groups with a 95% CI within the noninferiority margin of 0.4%. Its A1c-lowering abilities exhibited prolonged efficacy over 52 weeks, and the extent of this benefit did not significantly differ between insulin glargine-yfgn and reference insulin glargine (p > 0.3). There was no statistically significant difference in change in fasting plasma glucose levels between groups. The changes from baseline daily total basal insulin dose (p = 0.53) and daily mealtime insulin doses did not significantly differ between the 2 treatment groups.8-10 A slight increase in weight was noted in each group, but there was no difference between groups (p = 0.633). Adverse effect rates were similar between groups with hypoglycemia being the most common with 55.0% occurring with insulin glargine-yfgn and 61.2% with reference insulin glargine.
INSTRIDE 2 10 had a very similar design to INSTRIDE 1, but was conducted in patients with type 2 diabetes on oral medications to determine noninferiority of insulin glargine-yfgn versus reference insulin glargine regarding mean change in A1c from baseline over 24 weeks. The mean change in A1c was −0.60% (95% CI: −0.78, −0.41) for insulin glargine-yfgn and −0.66% (95% CI −0.84, −0.48) for reference insulin glargine. Noninferiority was determined with minimal differences between groups with a 95% CI within the noninferiority margin of 0.4%. No significant differences were detected in change in fasting plasma glucose (p = 0.071) or in A1c (p = 0.455). No difference was noted in daily basal insulin dose changes between groups (p = 0.757). An increase in weight was noted in each group, but without any significant difference between groups (p = 0.770). Adverse effects were similar between groups including hypoglycemia (p > 0.05).
Switching between insulin glargine-yfgn and reference insulin glargine did not impact glycemic efficacy in adults with type 1 diabetes in the INSTRIDE 3 trial. 11 Participants completing the reference insulin glargine arm of INSTRIDE 1 were randomized to receive reference insulin glargine or the treatment switching group who received insulin glargine-yfgn for weeks 0 to 12, then reference insulin glargine for weeks 12 to 24, then insulin glargine-yfgn weeks 24 to 36. The primary endpoint was change in A1c after 36 weeks to determine equivalence between groups. After 36 weeks, the mean change was −0.05 (0.032) for the insulin glargine-yfgn sequence group and −0.06 (0.034) for the reference insulin glargine sequence group, with an LS mean difference of 0.01 (95% CI: −0.085 to 0.101). This crossover/switch study exhibited no statistically significant difference in mean A1c change between groups with the 95% CI within +/-0.4% equivalence limits. No clinically significant differences were noted between groups regarding daily mealtime insulin doses, body weight, fasting plasma glucose, and self-monitoring blood glucose levels.
Insulin glargine-yfgn is well tolerated and has a safety and immunogenicity profile highly similar to reference insulin glargine in patients with type 1 and type 2 diabetes when given alone or in conjunction with rapid-acting mealtime insulin lispro. Like other insulins, the most frequently reported adverse effect was hypoglycemia. The frequency, number of episodes per 30 days, and incidence of overall nocturnal hypoglycemia did not significantly differ between the 2 treatment groups during the INSTRIDE 1 and INSTRIDE 2 trials. Most other reported adverse effects were mild to moderate and paralleled those of reference insulin glargine with respect to frequency and severity.8-11 Limitations of these trials include an open-label design (due to different packaging between insulin glargine-yfgn prefilled disposable pens and FDA-approved prefilled disposable reference insulin glargine pens) and study population heavy with males of Caucasian/European origins; neither of which are thought to have biased the results. These trials led to insulin glargine-yfgn’s approval in August 2020 as a biosimilar and in July 2021 as an interchangeable biosimilar to reference insulin glargine. The official launch of brand name interchangeable Semglee® to the US market began on November 16, 2021, with the simultaneous announcement and release of its authorized generic, Insulin Glargine-yfgn.
Indications
Brand name insulin glargine-yfgn and the authorized generic, Insulin Glargine-yfgn, are indicated to improve glycemic control in adults and pediatric patients with type 1 diabetes and in adults with type 2 diabetes. 7
Benefits
As the number of individuals diagnosed with diabetes continues to rise, there is an even greater need for affordable biosimilar insulins. 5 Diabetes places an economic burden on both patients and the healthcare system. 5 The prevalence of patients with uncontrolled diabetes can partly be attributed to the costly nature of insulin. 5 Biosimilar insulins are on the path to worldwide accessibility for all patients with diabetes. The new installation of biosimilar insulins to the market will create more competition, likely driving down the prices of insulin for all patients. Pharmacists routinely save patients money by substituting generic medications for their brand name counterparts. The ability of pharmacists to substitute interchangeable biosimilar insulins for brand name reference insulins is vital to reducing healthcare costs.
Payors prefer utilizing the least expensive options and achieve this through a tiered formulary system that directs prescribers toward biosimilars. CVS Caremark, a US pharmacy benefit management company, has already added follow-on insulin glargine to their formularies in place of reference insulin glargine. 1 Though the price difference between a biosimilar and reference insulin could be minimal for each prescription, the chronic nature of insulin use will likely eventually lead to exceptional savings for patients and payors. “Biosimilars marketed in the US typically have launched with initial list prices 15% to 35% lower than comparative list prices of the reference products,” the FDA wrote. 12 At the time of the writing of this publication (only 1-2 weeks from the status of interchangeability), the price of insulin glargine-yfgn was approximately one-third the price of reference insulin glargine, and follow-on insulin glargine was over two-thirds the price of reference insulin glargine (Table 1), both with the same safety and efficacy of the reference product. 13
Cost Comparison of Insulin Glargine U100 Products. 13
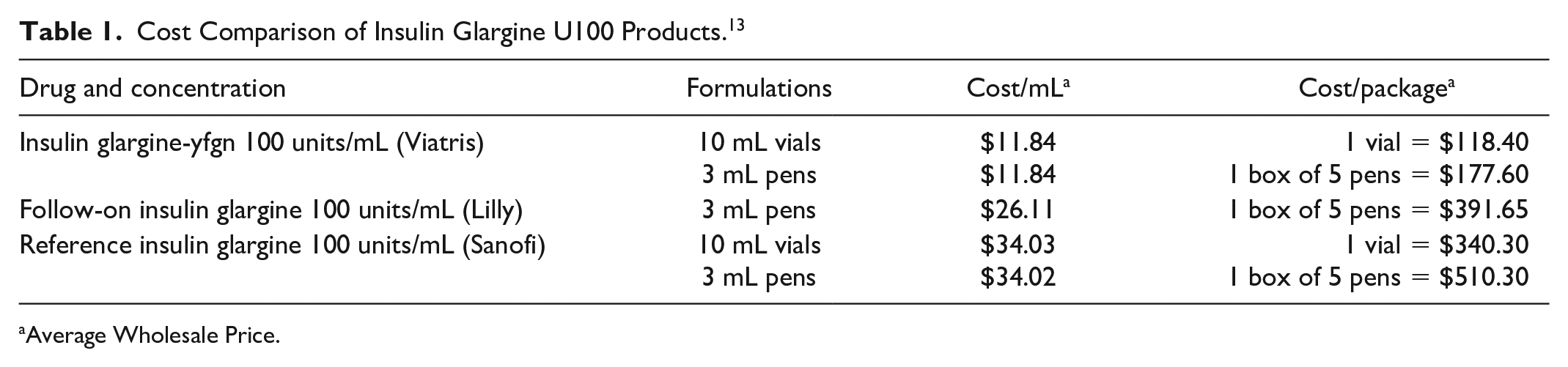
Average Wholesale Price.
Entering a new era of interchangeable biosimilar insulin could lead to a more competitive insulin market. U.S. insulin prices nearly tripled between 2002 and 2013 and increased by 15% to 17% per year between 2012 and 2016. 14 Between 2006 and 2013, out-of-pocket costs per insulin users with Medicare Part D increased by 10% per year, while spending for all prescription drugs increased by an average of only 2.8%. 14 The U.S. healthcare system could significantly cut costs by preferencing interchangeable biosimilar insulins over expensive reference biologics (insulin glargine-yfgn in place of reference insulin glargine) in a manner similar to generic substitutions for brand name products. To remain competitive, other insulin glargine products, and potentially other nonglargine basal-insulin products, will have to lower their prices to comparable levels of insulin glargine-yfgn. The next step will be the development of biosimilar interchangeable rapid-acting insulin for lower-cost complete insulin regimens. The positive impact of future insulin pricing means many more patients could gain access to much-needed insulin therapy.
Challenges
Traditional drugs are stable, small-molecule compounds with well-defined structures which can be reproduced identically by different synthetic pathways by different manufacturers. However, biologic products are unstable, large-molecule compounds with heterogeneous structures that are difficult to characterize. 1 The structures of biologic medications are dependent on the complex biological processes used to create them. Varying methods used by different manufacturers may affect specifics in structure or even spatial orientation of the molecule which could affect function, safety, and efficacy. Manufacturing protocols of the reference biologic remain proprietary information so that other manufacturers may not exactly duplicate the process, but must instead figure out a way to create the structure in a properly functional manner. 1 Small changes within the manufacturing process can affect the resulting structures of biologics, even within the same batch, known as microheterogeneity.1,2 Specific limits of variability have been set, and this variability must be clinically irrelevant and have no impact on safety or efficacy. Because it is not feasible for manufacturers to produce identical copies of the reference biologic, these copies may not be known as generics. 1 These are, therefore, more challenging to replicate versus true generics and fewer may be developed.
Biosimilars or follow-on biologics, unlike generic products, cannot be substituted at the pharmacy counter without consulting the prescriber. Until a biosimilar reaches interchangeable status, it relies on the prescriber writing a new prescription for the biosimilar product to be substituted in place of the reference product. Follow-on insulin glargine remains in this position as a follow-on biologic that may not be substituted for reference insulin glargine at the pharmacy counter. However, as an interchangeable biosimilar, insulin glargine-yfgn may be substituted for reference insulin glargine, if state law allows, at the pharmacy counter without prescriber authorization. Some may experience confusion and need clarification that insulin glargine-yfgn may only be substituted for reference insulin glargine at the pharmacist level and not for follow-on insulin glargine. The interchangeable designation to the reference insulin may imply superiority to other general biosimilar products. However, while interchangeable biosimilars have undergone switch studies with the reference insulin to prove no higher rates of adverse effects or decreased efficacy, they are not necessarily superior to other biosimilars. This distinction could create confusion regarding the preferred use of interchangeable biosimilars over general biosimilars. This may also prompt more manufacturers of general biosimilars to seek the interchangeable designation to maintain competitiveness.
As with most medications, patients and prescribers become partial to particular insulins or delivery devices they have become accustomed to using. Some may resist a therapeutic change and remain loyal to a specific brand of insulin even when less expensive biosimilars are an option. As more biosimilar insulins are approved, the available number of insulin products will increase as well. The sudden increase in different types of available insulins may bring confusion for providers and patients alike, prompting educational opportunities. Patients should be educated on the need to stop reference insulin glargine if switching to insulin glargine-yfgn. Providing appropriate education to both patients and providers regarding new biosimilar insulins will have a profound impact on biosimilar insulins becoming more widely prescribed. 1
Conclusion
Insulin glargine-yfgn is the first interchangeable biosimilar insulin to reference insulin glargine; both are insulin glargine U100. Based on evidence from clinical trials, insulin glargine-yfgn is expected to perform equivalently to reference insulin glargine regarding blood glucose control with a similar adverse effect profile. Insulin glargine-yfgn may, therefore, be substituted for reference insulin glargine without a prescription from a provider, as allowed per state law. Patients should be encouraged to inform their prescribers of such substitutions. As more analog insulin products’ patents expire, more biosimilar products may become available. The added market competition will promote lower insulin costs for patients and payors, as demonstrated with insulin glargine U100. Additionally, healthcare providers will need to be made aware of how these products relate to each other, how they must be prescribed, and the potential for substitution.
Footnotes
Correction (April 2023):
Article updated online to correct degree ‘PhD’ as ‘PharmD’ for the authors.
Abbreviations
BPCI, biological price competition and innovation; FDA, Food and Drug Administration; A1c, hemoglobin A1c; US, United States; U100, 100 units/mL
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.