
Abstract

Big data analysis and artificial intelligence (AI) algorithms change how medical care is driven. They provide more accurate diagnoses, better follow-up of medical conditions, risk classification and prediction, and workflow optimization. 1 In ophthalmology, multimodal examinations are essential for diagnosis and follow-up. 1 Efficient and predictable management could be provided with big data and AI. 2
To achieve optimal AI development, dataset formation is critical. Reliable datasets with many entries, multiple ethnicities, and secure and trustworthy labels are fundamental. Nevertheless, labeling process standardization and homogenization remain challenges. 2
Diabetic retinopathy (DR) is a significant cause of preventable blindness in working-age adults worldwide, responsible for more than 24,000 annual cases of blindness. 3 There is increased risk in patients with chronic diabetes mellitus, especially those with poor disease control. 4 AI technology provides unprecedented diagnostic accuracy, triage intelligence, risk stratification, and workflow optimization with accuracy equivalent to health-care professionals 5 and more cost-effectiveness in DR detection. 3 Standardizing and homogenizing the classification of DR in ophthalmological datasets is challenging.
We compared applied DR scales in publicly available DR retinal fundus photos datasets. (Table 1)
Publicly Available DR Datasets.
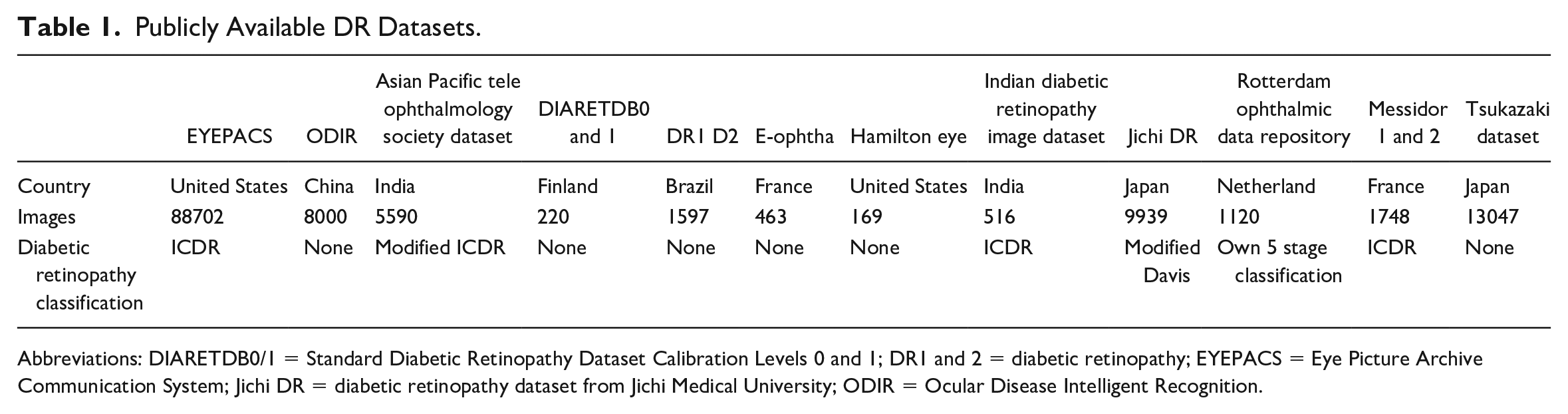
Abbreviations: DIARETDB0/1 = Standard Diabetic Retinopathy Dataset Calibration Levels 0 and 1; DR1 and 2 = diabetic retinopathy; EYEPACS = Eye Picture Archive Communication System; Jichi DR = diabetic retinopathy dataset from Jichi Medical University; ODIR = Ocular Disease Intelligent Recognition.
A significant quality-labeling by retina specialists could improve algorithm performance, 2 and reliable datasets are fundamental to AI development; however, labeling process standardization and homogenization remain challenges. 2 In some datasets, the DR classification is not explicit (eg, ROD Rep). There was no DR classification method in datasets such as Tsukazaki, HEI- MED, E-ophtha, DR1, DR2, DIARETDB0/1, and ODIR.
The most often-applied classification in open-access ophthalmological datasets is ICDR (73.64%), which stratifies DR in four stages and is based on the classic ETDRS classification. We proposed the Scottish Diabetic Retinopathy (SDR) as appropriate for diagnosis thought retinal images, with one single macular centered retinal exam. SDR grading is more sensitive for grading moderate and severe cases than ICDR classification. In DR datasets, the SDR grading is an adequate classification due to greater sensitivity in detecting moderate and severe DR using a single macula-centered image.
When choosing the classification method applied in the dataset, the image field of view and the number of images must be considered. Classical ETDRS and ICDR classifications tend to underestimate DR classification in retinal photographic images due to limited image view areas compared to retinal fundus examinations. Scottish Diabetic Retinopathy Grading (SDRG) is the only classification based on a single fovea-centered retinal photograph. For this reason, it is a valuable alternative to be considered in DR dataset classifications.
It is fundamental to standardize DR grading in datasets to develop algorithms and ensure proper patient referral. AI can provide a more accurate diagnosis 1 and be more cost-effective than human assessment. 6
The various DR labeling systems generate a fundamental problem for AI datasets. Possible solutions are retinal-finding identifications in supervised learning or standardization of a DR classification. Reliable labeling methods also need to be considered in datasets, with more trustworthy labeling, including multiple-specialist analysis.
Footnotes
Abbreviations
AI, artificial intelligence; DR, diabetic retinopathy; SDR, Scottish Diabetic Retinopathy.
Permissions
The data used in this current study are available upon request to the corresponding author
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M B Gonçalves is a researcher supported by Lemann Foundation, Instituto da Visão -IPEPO, São Paulo, Brazil and CAPES Foundation, Ministry of Education of Brazil, Brasília, DF, Brazil. D A Ferraz has been supported by CAPES Foundation, Ministry of Education of Brazil, Brasilia, DF, Brazil. The authors Luis F Nakayama, Helen N V Santos, Fernando K Malerbi, Paulo H Morales, Mauricio Maia, Caio V S Regatier, and Rubens Belfort Jr, disclosure that they have not received funding for this project and article.
UNIFESP Ethics Institutional Review Board number
CAAE 33842220.7.0000.5505 / n:0698/2020