
Abstract
Background:
Diabetes-related foot disease (DFD) management requires input from multiple healthcare professionals, and has worse outcomes for people living in remote localities by comparison to urban areas. Remotely delivered healthcare may reduce this disparity. This overview summarizes current evidence on the effectiveness, stakeholder perceptions, and cost-effectiveness of remotely delivered healthcare for DFD.
Methods:
A search of 5 databases was conducted to identify systematic reviews published between January 2000 and June 2020. Eligible reviews were those evaluating remotely delivered monitoring or management of patients at risk of or with active DFD, or clinicians managing these patients. Risk of bias was assessed using the AMSTAR-2 tool.
Results:
Eight reviews were eligible for inclusion, including 88 primary studies and 8509 participants, of which 36 studies involving 4357 participants evaluated remotely delivered monitoring or management of DFD. Only one review had a low risk of bias, with most reviews demonstrating limited search strategies and poor reporting of participants. Evidence on effectiveness was mixed, with meta-analyses demonstrating long-term ulcer healing and mortality were not significantly different between telehealth and standard care groups, although the lower-limb amputation rate was significantly decreased in one meta-analysis. Perceptions of telehealth by patients and clinicians were generally positive, whilst acknowledging limitations relating to access and use. Cost-effectiveness data were limited, with poor reporting preventing clear conclusions.
Conclusions:
Remotely delivered healthcare of DFD is well received by patients and clinicians, but its effectiveness is unclear. High quality trials are needed to evaluate the risks and benefits of remotely delivered DFD management.
Introduction
Diabetes-related foot disease (DFD) encompasses a range of foot complications, such as ulcers, gangrene and infection, and predisposes affected individuals to amputation and reduce life expectancy.1,2 An estimated 20% of the approximately 430 million people with diabetes globally are expected to develop DFD, 1 making it a leading cause of hospital admission 3 and one of the top 10 causes of global disability.1,4 Prevention and treatment of DFD requires a range of interventions, including comprehensive patient education, use of offloading footwear, risk factor control and treatment of pre-ulcerative lesions and active ulcers, and regular foot care, delivered by a multidisciplinary group of health professionals. 5
DFD is traditionally managed through hospital or clinic appointments with multiple health professionals such as podiatrists, vascular surgeons and wound care nurses.5,6 The frequency of these appointments varies depending on the severity of DFD but can occur multiple times per week. 6 These consultations required with a range of specialists creates substantial burden on the patient and healthcare system and can complicate management.3,7 Additionally, outcomes from DFD are substantially worse for people residing in more geographically remote areas where, for example, amputation rates are up to 10 times higher than in urban regions. 8
Recent research has assessed the role of telehealth and related technologies in foot assessment, medical management, offloading footwear design and education for DFD treatment.9-15 Remote delivery of healthcare can provide a more accessible and convenient way for patients to receive management through reducing the need for face-to-face consultations and potentially reduce geographic inequality in outcomes. To be successful remotely delivered healthcare should be acceptable to relevant stakeholders, such as patients and clinicians, and be cost-effective. Currently, the role of telehealth in DFD management is controversial. 13 Its assessment is complicated by the heterogeneity in telehealth management programs which have been used. These have varied in the route of delivery, frequency of contact, and target population.13-15 Published studies have focused either on only selected components of DFD healthcare, such as wound care only, or focused on specific aspects of telemedicine, such as one route of delivery or on stakeholders’ perceptions of such interventions alone.9,12,13 It is therefore essential to investigate and understand the composite range of methods of remotely delivered DFD healthcare that have been tested, and the stakeholders’ perceptions and cost-effectiveness of such interventions.
This overview aimed to collate evidence from existing systematic reviews on remotely delivered monitoring and management of DFD, report and evaluate evidence on their effectiveness, stakeholder perceptions and cost effectiveness.
Methods
This study was designed as an overview of systematic reviews. This is an emerging research method that summarizes broader fields of evidence than traditional systematic reviews, and can summarize different interventions for the same condition or population.16-18 The diversity of telehealth interventions examined in primary research to date suited the use of an overview rather than a systematic review. This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 19 and was registered with PROSPERO (CRD42020197394).
Search Strategy and Study Selection
PubMed, MEDLINE, CINAHL, Embase, and Cochrane Library were searched for eligible English-language articles published between January 2000 and June 2020 to capture contemporary research on technology-driven healthcare. Each database was searched independently by a single author using an agreed search string, and the findings reviewed by a second author. The date of the last search was 29th June 2020. A broad search string was developed combining 3 groups of terms using Boolean operators: (1) “review” (eg, systematic), (2) “remote” (eg, telehealth), and (3) “disease and treatment” (eg, diabetic foot). The search strategy and example string are shown in Online Appendix 1. Reference and citation lists were manually searched to identify additional eligible reviews.
Eligible articles were published systematic reviews that included primary studies investigating the effect of telehealth management in adults with or at risk of DFD, or clinicians managing DFD. Reviews reporting telehealth management of DFD or monitoring of the foot in people at risk of developing DFD were eligible if participants were described as at high risk of developing DFD or had DFD. Each review identified from the search was screened by at least 2 authors. Title screening identified reviews on telehealth for managing DFD or a relevant risk factor, confirmed by abstract and full-text screening.
Evaluation of Bias
The Assessing the Methodological Quality of Systematic Reviews (AMSTAR)-2 tool was used to assess risk of bias. 20 This 16-item checklist appraises systematic reviews of randomized and non-randomized studies of healthcare interventions. The checklist items cover several critical and non-critical aspects of review quality, including a-priori design, search strategy, study selection and data extraction, reporting of included and excluded studies, quality assessment, methods for data synthesis and formulation of conclusions. Each item was scored as “yes” (1 point), “no” or “unsure” (0 points). Cut-off scores for overall risk of bias were chosen in line with previous overviews,21,22 as ≥80% = low risk, 50%-79% = moderate risk, 25%-49% = high risk, and <25% = critically high risk. Two authors independently assessed risk of bias of each review, with the first and last author resolving disagreements.
Data Extraction and Analysis
A standardized form was developed (Online Appendix 2) to extract the following data from each review: title, authors, year published, date assessed, search strategy, number of primary studies, participants included, participant characteristics and intervention setting, type, frequency and duration of remotely delivered and standard healthcare intervention(s), primary and secondary review outcomes, review limitations and additional relevant information. Two authors independently extracted and cross-checked data from each review, with the last author resolving disagreements between the 2 relevant authors. Extracted data were summarized narratively, taking into consideration review scope, population, interventions, comparator groups, outcomes (PICO) and methodological quality. An excel database was created using citation cross-referencing between individual reviews by a single author (AD) to identify each primary study to ensure no data were included twice. Evidence on effectiveness were grouped in relation to the method of remote monitoring and management and population (eg, clinician or patient). Meta-analyses were planned but significant heterogeneity across the reviews precluded this.
Results
Of 6153 search results, 419 underwent full-text screening. Most were excluded due to not being a systematic review or not evaluating DFD-related telehealth interventions. Figure 1 illustrates the PRISMA flow diagram. Eight systematic reviews focusing on remote monitoring for people at risk of DFD or remote management of people with DFD were included.23-30 These reviews, 4 of which included meta-analysis,23,25,27,30 are summarized in Table 1.
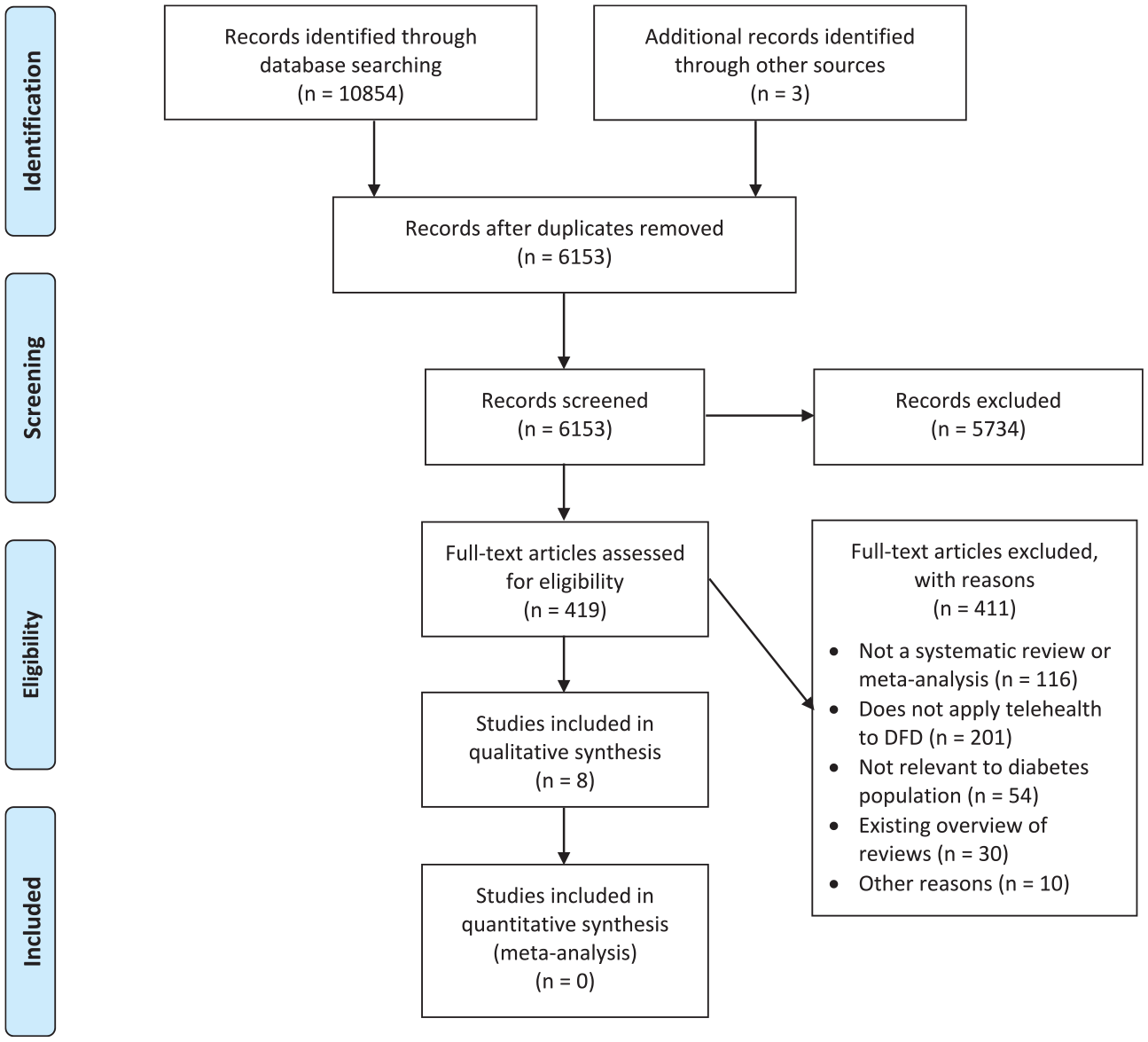
PRISMA Flow Diagram Illustrating Screening and Selection Process.
Characteristics of Reviews and Analyses Included in This Overview of Reviews.
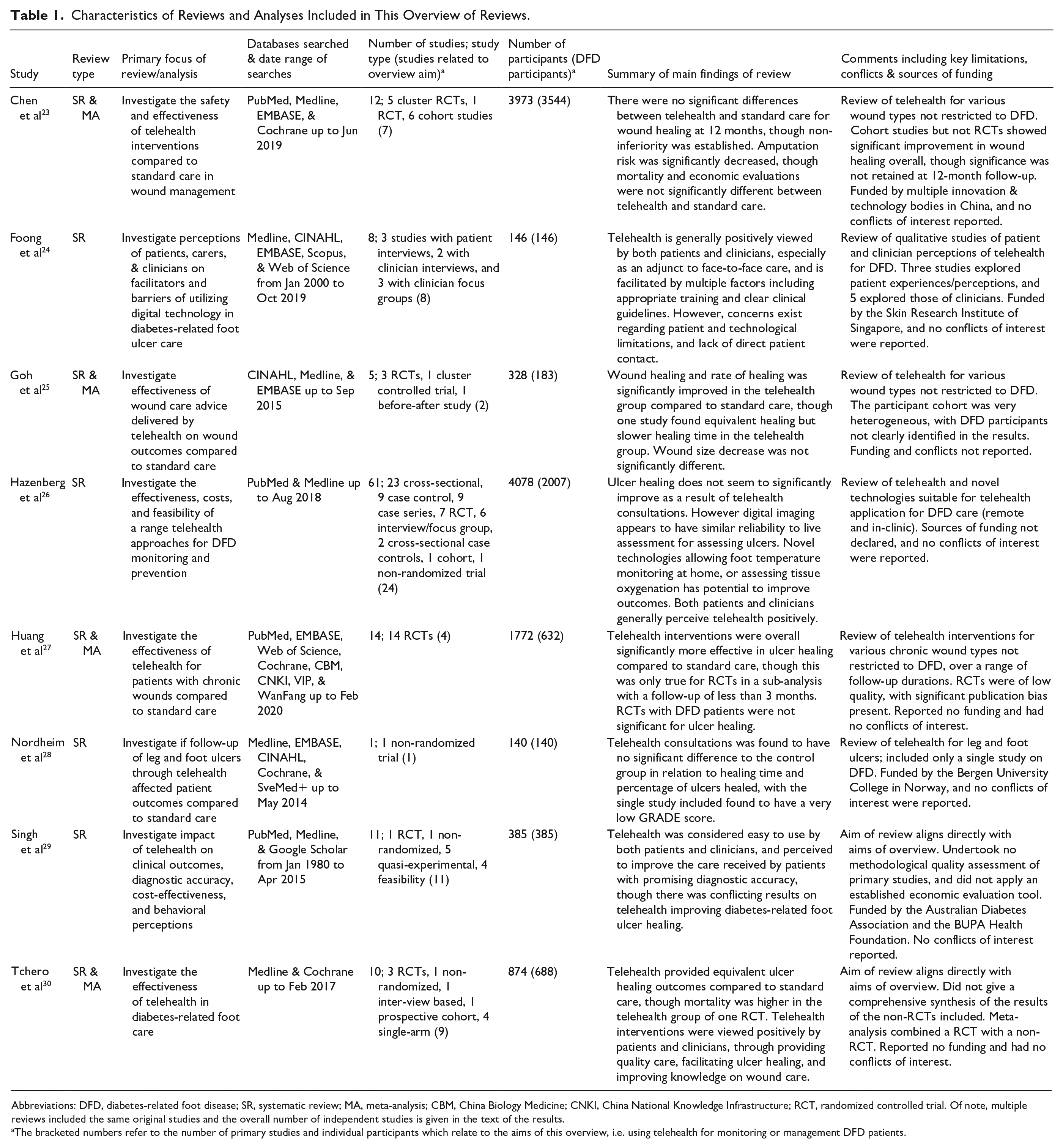
Abbreviations: DFD, diabetes-related foot disease; SR, systematic review; MA, meta-analysis; CBM, China Biology Medicine; CNKI, China National Knowledge Infrastructure; RCT, randomized controlled trial. Of note, multiple reviews included the same original studies and the overall number of independent studies is given in the text of the results.
The bracketed numbers refer to the number of primary studies and individual participants which relate to the aims of this overview, i.e. using telehealth for monitoring or management DFD patients.
Review and Participant Characteristics
The reviews were published between 2014 and 2020 and included 88 independent primary studies of 8509 participants, which are listed in Online Appendix 3. Not all primary studies assessed the use of telehealth for DFD; 37 studies described foot monitoring performed in community or hospital clinics, or technology development, and 15 did not involve management of DFD. The remaining 36 primary studies of 4357 participants aligned with the aims of this overview. Four reviews focused on studies using telehealth for DFD,24,28-30 one of which included only qualitative studies investigating patient and clinician perspectives of telehealth for DFD. 24 Three reviews focused on telehealth management of a range of wound types23,25,27 and one focused on telehealth management of DFD, but included studies that were delivered in a standard clinic environment, as well as those delivered remotely. 26
Risk of Bias
Four reviews had a high risk of bias,25,26,29,30 3 a moderate risk of bias23,24,27 and 1 a low risk of bias. 28 Table 2 summarizes the risk of bias outcomes and limitations of the reviews. Common limitations identified included: no clear a-priori design, lack of a comprehensive literature search (eg, not screening reference lists), not justifying reasons for excluded articles, not providing adequate detail on included studies (especially participant details) and not reporting the sources of funding. This variation in risk of bias and the presence of critical methodological limitations across many of the reviews necessitates caution in the interpretation of the findings, particularly the applicability of the findings to a broader population.
Methodological Quality of Systematic Reviews Based on the AMSTAR-2 Criteria.
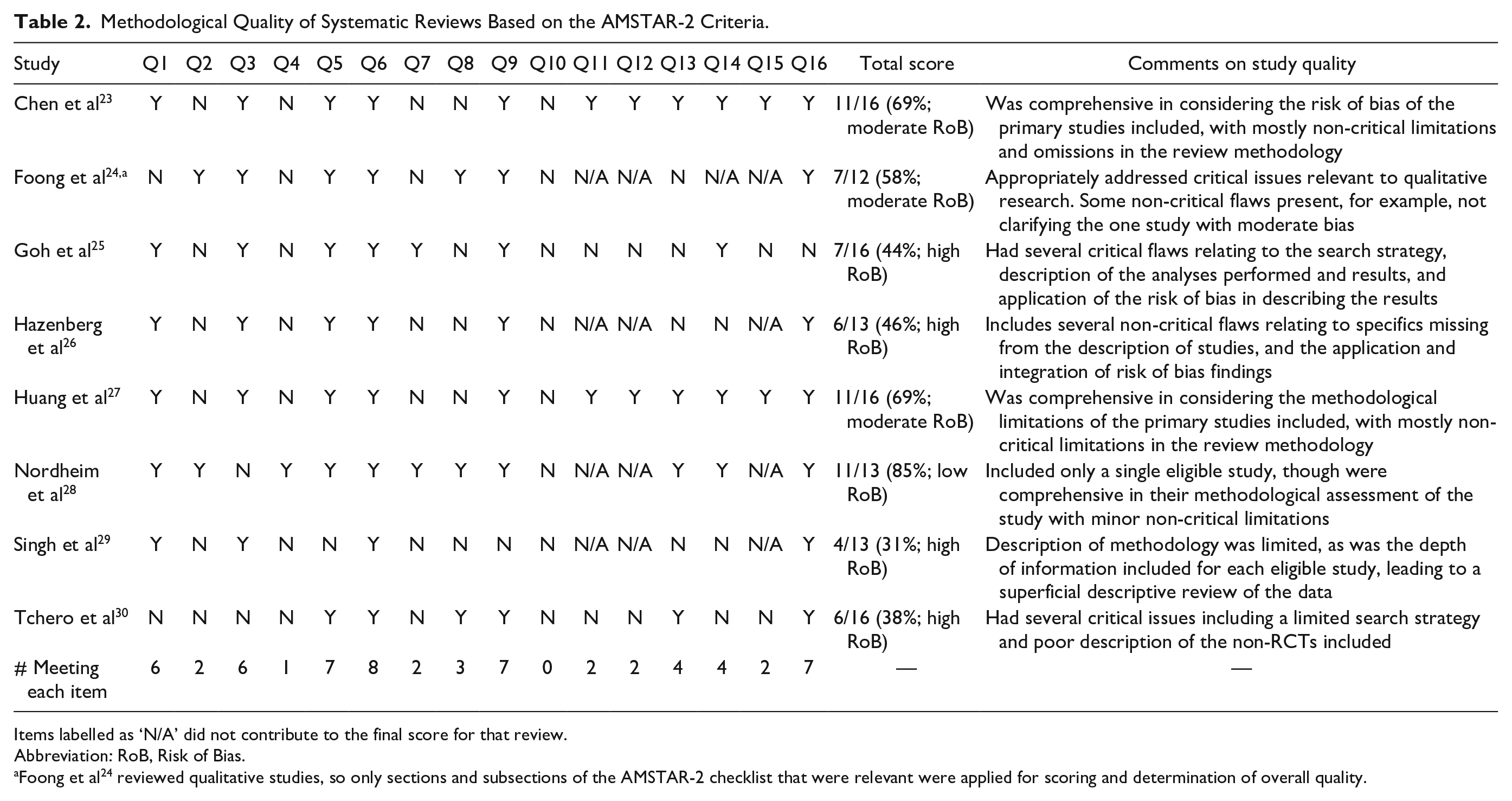
Items labelled as ‘N/A’ did not contribute to the final score for that review.
Abbreviation: RoB, Risk of Bias.
Foong et al 24 reviewed qualitative studies, so only sections and subsections of the AMSTAR-2 checklist that were relevant were applied for scoring and determination of overall quality.
Effectiveness of Telehealth in Managing DFD
A range of DFD interventions within the reviews were classified as “telehealth” or “telemedicine,” with most reviews reporting on the effectiveness of videoconferencing management and the accuracy, feasibility and use of digital images to assist in providing healthcare. One review also described the effectiveness of novel technologies that had potential telehealth applications. 26
Videoconferencing and digital photography in the management of DFD
A few primary studies were included across at least half of the reviews,31-33 each of which reported a lack of high quality evidence and consensus on the effectiveness of video consultations for improving ulcer healing and reducing the time to ulcer healing and amputation rates.23,25-30 A meta-analysis of 2 studies evaluating nurse-led algorithm-based telehealth consultations in 1 review reported no significant difference between telehealth and standard care in achieving DFD ulcer healing (odds ratio [OR] 0.86; 95% confidence interval [CI] 0.57-1.33, P = 0.53, I2 = 0%). 30 Two other meta-analyses of studies using specialist nurses or wound care experts reported that telehealth management significantly improved the healing of a heterogeneous group of wounds, including diabetes-related foot ulcers compared to standard care (5 studies [2 DFD-specific]: HR = 1.40, 95% CI 1.10-1.79, P = 0.01, I2 = 60.6% 23 ; 12 studies [3 DFD-specific]: RR 1.44, 95% CI 1.16-1.80, P = 0.001, I2 = 76%). 27 These findings were not, however, confirmed when the analyses were limited to randomized controlled trials, 27 or studies with follow-up of greater than 3 months 27 or for wound healing at 12 months or longer (all P > 0.05). 23
These 2 meta-analyses also reported no significant difference in mortality between telehealth and standard healthcare (RR 1.03, 95% CI 0.47-2.24, P = 0.94 23 ; OR 0.82, 95% CI 0.46-1.46, P = 0.51), 27 though reported a significant reduction in the frequency of amputation after 12 months in the telehealth group compared to the standard healthcare groups (RR 0.52, 95% CI 0.34-0.80, P = 0.003 27 ; and RR 0.45, 95% CI 0.29-0.71, P = 0.001). 23 The other reviews also reported faster ulcer healing rates using a telephone-based advisory system 30 or home nurses to assist in telemonitoring 25 and non-inferiority for time to healing and amputation rate 26 and reduced diabetes-related foot ulcer size compared to outpatient clinic visits. 23
Of 17 studies in these reviews that investigated the use of digital imaging, 10 assessed the accuracy or feasibility of imaging within the clinic or hospital setting, whilst the other 7 assessed the use of digital photography performed in the patient’s home that was then sent to clinicians for review. Photographing feet or ulcers as described in these 7 studies was reported to be useful for DFD management due to its convenience and allowing for more frequent monitoring.26,29,30 However, the effect of this digital photography on ulcer healing, amputation, or mortality was not reported. The included reviews reported a high degree of intra and inter-observer agreement between photographs and live assessment of ulcers.26,29,30 These findings were dependent on the camera used, with mobile phones reported to have lower inter-observer reliability compared to tablets. 26 Overall, telehealth management was reported to be effective when supplementing rather than replacing face-to-face consultations,23,24,30 with one review stating this approach increased ulcer healing rate and reduced amputations. 30 Other reviews stated that this approach had other benefits, such as reducing the time needed to gather patient data during face-to-face consultations, reducing the duration of subsequent consultations, 30 and reducing the mean number of hospital appointments required. 23
Novel technologies in the management of DFD
One review evaluated technologies for DFD management with potential telehealth applications. 26 Three of four randomized controlled trials reported that daily home infrared foot temperature monitoring and offloading of identified hot spots significantly reduced the risk of recurrent diabetes-associated foot ulcers compared to standard healthcare. Thermometric mats had high sensitivity in predicting future foot ulcers in the home setting and smart socks demonstrated moderate agreement with cameras in assessing foot temperature. 26 Dermal thermography was able to identify significant temperature differences between healthy feet and feet with an ulcer or Charcot arthropathy. 26 Hyperspectral imaging assessing tissue oxygenation was reported to have unclear efficacy in predicting ulcer healing and future ulcer development before tissue breakdown occurred. 26
Stakeholder Perceptions of Telehealth for Managing DFD
Five reviews evaluated 18 primary studies with a minor or major qualitative component, gathering clinician and patient experiences and perceptions of using telehealth technologies, through surveys, interviews or focus groups.23,24,26,29,30
Clinician perceptions
Telehealth monitoring and management was reported to be positively viewed and considered easy to use,26,29,30 to facilitate improved wound management skills (particularly for nurses),24,26,29,30 allow remote prescribing26,29,30 and improve treatment time, 29 all leading to improved patient outcomes.26,29,30 Telehealth was also perceived effective for communication between multidisciplinary teams24,29 and between clinicians and patients, leading to holistic and individualized care. 24 Nurses reported that increased responsibility improved their confidence and job satisfaction.24,26 Telehealth-based communication also improved efficiency of healthcare when using electronic documentation and interactive web-based platforms, reduced unnecessary phone calls and enabled a smoother workflow. 24
Telehealth was, however, considered time-consuming24,26,30 and might reduce clinical skills by removing direct patient contact, 24 particularly if certain clinicians (such as podiatrists) were not involved in the telehealth process. 24 Other reported drawbacks included the potential for less patient engagement in treatment, invasion of privacy 24 and dependence on clinician training and access to technologies. 24 In one review a lack of systematic training led to frustration amongst clinicians and intentions to resign from their position. 24 Telehealth was also reported by clinicians to have limitations for patients, including difficulty in using the technology for monitoring and consultations, for example, inability to take accurate photographs of feet.24,26 Finally, effective telehealth services were reported to require ‘buy-in’ at all leadership levels in addition to clear guidelines and protocols for telehealth conduct.24,26
Patient perceptions
Similar to clinicians, patients also reported positive perceptions of telehealth. They found it feasible and easy to use, felt safe when receiving information from clinicians and appreciated reduced travel time required for consultations,24,26,29,30 although one review reported no difference in patient satisfaction compared to usual care. 23 Patients also perceived the quality of care received from telehealth to be high and felt their treating clinicians sufficiently skilled to deliver this healthcare.26,30 Patients reported telehealth consultations led to empowerment through improved access to clinicians and engagement in their own healthcare. 24 Telehealth facilitated discussion with their managing clinicians 24 and usefully supplemented standard healthcare visits,24,30 particularly amongst older patients. 24 While taking photographs was seen as beneficial for ulcer assessment, patients had concerns regarding their ability to use mobile phones and applications correctly, despite acknowledging the benefit of providing the images to clinicians. 24
Cost-Effectiveness
Only 3 reviews reported the cost-effectiveness of telehealth from 6 primary studies,23,26,30 the results of which were conflicting. One review reported that one study found significantly reduced treatment costs using digital imaging and remote consultation compared to standard healthcare. 30 Another review reported no significant difference in average treatment costs between telehealth and standard healthcare. 26 The other review reported on 4 primary studies, 2 of which reported reduced cost, 1 statistically equivalent costs and 1 higher mean costs for telehealth versus standard healthcare. 23 The heterogeneity in the telehealth management tested and a lack of detailed reporting made it difficult to draw conclusions from these reports.
Discussion
This is the first overview to compile evidence on the efficacy, stakeholder perceptions and cost-effectiveness of telehealth in the remote monitoring and management of DFD; a common but under-recognized complication of diabetes. 3 DFD patients have unique monitoring and management requirements that distinguish them from people with diabetes without DFD. This overview found the efficacy of telehealth in achieving sustained ulcer healing and reduced mortality was not clearly demonstrated, whereas amputation rates were reportedly significantly reduced. Cost-effectiveness data were minimal, leading to inconclusive outcomes.34,35 Despite this, stakeholders had positive views on telehealth, believing it facilitated improved communication between parties and ultimately improved healthcare.
Telehealth is an ambiguous term and encompasses a range of potential healthcare interventions. 36 This overview found that video-consultations and digitally sharing photographs to or between clinicians have been frequently trialed and may reduce amputation rates although more clear evidence is needed before concluding this. 37 These findings alongside stakeholder views on telehealth indicate its potential value in supplementing rather than replacing traditional face-to-face care. However, effective telehealth may be costly, making it necessary to consider if the resources required outweigh those used in current systems. The cost-effectiveness of DFD telehealth management has not been clearly established,34,35 although it might be for those living in remote areas, 38 who have higher rates of diabetes, and are under-reported in research. 39 Previous research focused on risk factor control in people with diabetes has suggested that telehealth management improves control of glycated hemoglobin, cholesterol and blood pressure for people in rural and medically underserved populations. 40
Overall, the effects of telehealth on long-term outcomes were unclear, with interpretation of the identified reviews limited by the heterogeneity of the telehealth management tested, the populations included, and the length of follow-up. Patient characteristics including age, 41 ethnicity, 42 and rurality of residence40,43 can contribute to the benefit and feasibility of telehealth. Many studies have highlighted the difficulty experienced by the elderly in using mobile and other technologies, 44 although the proportion of mobile and computer owners is increasing amongst this demographic, as well as evidence of their adaptability to new health-related technologies. 45 Cultural differences are also recognized as a predictor of telehealth appropriateness and uptake, as well as the lack of sufficient representation of ethnic minorities within telehealth trials. 42
Daily foot checks and offloading footwear form the cornerstone of DFD prevention, 6 though uptake and adherence to these are reported to be poor.46,47 Home-based foot monitoring with capacity for the recording and transmission of data has become more feasible with technological advancements relating to sensors and wearable devices.13,48 Psychological interventions and behavioral support were not included in this overview and though it is theorized they could improve patient understanding and engagement in managing DFD, the level and quality of evidence is low. 49 Overall, this overview highlights the lack of high quality research testing the efficacy of telehealth in improving the outcomes of people with DFD. The variety of interventions and wound types assessed were key barriers in determining the benefit of telehealth in remote DFD monitoring and management. Carefully designed randomized controlled trials are needed to rigorously test the value of remotely delivered DFD monitoring and management.
Several strengths and limitations should be noted. The overview was conducted according to established guidelines and the authors ensured searching, screening and data extraction were conducted independently by multiple authors. The inclusion of quantitative and qualitative data also strengthens the value of the finding of reviews evaluating telehealth. Heterogeneity present in the primary studies was an inherent limitation, as was the methodological quality of the identified reviews. This made it difficult to draw conclusions, but demonstrates the possibilities and flexibility of telehealth if applied. The lack of cost-effectiveness data also obscured the potential financial benefits (or limitations) of telehealth. Finally, as overviews only include systematic reviews, relevant primary studies not captured by any of these reviews or that were published after these reviews, were not incorporated in this overview.
Conclusions
DFD places a large burden on individuals and health systems due to the requirements for repeated multidisciplinary consultations. Remotely delivered monitoring and management may facilitate improved healthcare particularly for patients living in rural or remote locations. This overview found that though telehealth is well regarded by both patients and clinicians, there is a lack of high quality evidence or consensus on its long term effectiveness in improving DFD outcomes. High quality trials are needed to determine the value of telehealth in managing DFD.
Supplemental Material
sj-docx-1-dst-10.1177_19322968211012456 – Supplemental material for Remotely Delivered Monitoring and Management of Diabetes-Related Foot Disease: An Overview of Systematic Reviews
Supplemental material, sj-docx-1-dst-10.1177_19322968211012456 for Remotely Delivered Monitoring and Management of Diabetes-Related Foot Disease: An Overview of Systematic Reviews by Aaron Drovandi, Shannon Wong, Leonard Seng, Benjamin Crowley, Chanika Alahakoon, Jasmin Banwait, Malindu E. Fernando and Jonathan Golledge in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-2-dst-10.1177_19322968211012456 – Supplemental material for Remotely Delivered Monitoring and Management of Diabetes-Related Foot Disease: An Overview of Systematic Reviews
Supplemental material, sj-docx-2-dst-10.1177_19322968211012456 for Remotely Delivered Monitoring and Management of Diabetes-Related Foot Disease: An Overview of Systematic Reviews by Aaron Drovandi, Shannon Wong, Leonard Seng, Benjamin Crowley, Chanika Alahakoon, Jasmin Banwait, Malindu E. Fernando and Jonathan Golledge in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-3-dst-10.1177_19322968211012456 – Supplemental material for Remotely Delivered Monitoring and Management of Diabetes-Related Foot Disease: An Overview of Systematic Reviews
Supplemental material, sj-docx-3-dst-10.1177_19322968211012456 for Remotely Delivered Monitoring and Management of Diabetes-Related Foot Disease: An Overview of Systematic Reviews by Aaron Drovandi, Shannon Wong, Leonard Seng, Benjamin Crowley, Chanika Alahakoon, Jasmin Banwait, Malindu E. Fernando and Jonathan Golledge in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
AMSTAR, assessment of multiple systematic reviews; CI, confidence interval; DFD, diabetes-related foot disease; HR, hazard ratio; OR, odds ratio; PICO, patient intervention comparison outcomes; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RR, risk ratio.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from James Cook University (Strategic Research Investment Fund) and the Queensland Government supported this work. JG holds a Practitioner Fellowships from the National Health and Medical Research Council (1117061) and a Senior Clinical Research Fellowship from the Queensland Government, Australia. The funders played no role in study design, conduct, data collection, analysis and interpretation, and did not assist in preparation or review of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.