
Abstract

Previous research has shown that insulin, as a peptide hormone, is susceptible to structural changes and loss of effectiveness when exposed to environmental temperatures outside the recommended storage range.1-4 It was also shown that it is often improperly stored by people with diabetes (PwD) to a clinically relevant percentage of storage time, 5 although the effect on glycemic levels remains not yet quantified.
To assess awareness and knowledge regarding proper storage and transport of insulin, we conducted a cross-sectional online survey (Charité ethics approval: EA 2/042/20). Participants were recruited via professional medical organizations, international patient advocacy networks, and social media. Of the 200 participants based in 16 different countries in Europe, North America, Asia, and the Western Pacific region, 74% were PwD, including type 1, 2, and other; 26% were healthcare professionals (HCPs); and 19% were caregivers of children with diabetes. As participants could belong to more than one group, 26 participants were HCPs living with diabetes and 10 were HCPs and caregivers of children with diabetes at the same time. An analysis was made by means of a spreadsheet analysis. Because we made some interesting findings, we would like to provide a brief summary of the results.
Only 54% of the participants could indicate the correct temperature ranges for both storage of unopened insulin in a refrigerator (2°C-8°C) and when opened and in use (2°C-30°C). Of PwD and caregivers, 76% take precautions to protect their insulin in-use from heat or cold, and 50% assume that insulin loses partial effectiveness when exposed to temperatures outside the recommended range. However, we found participants to overestimate the individual protection measures taken, as only 35% regularly monitor storage temperatures, and only 67% use a “cooling bag/dedicated cooler” to protect their insulin during travel.
One-third of all HCPs report having never received education on insulin storage as part of their professional training, without significant differences between those working in diabetes care and other areas of healthcare.
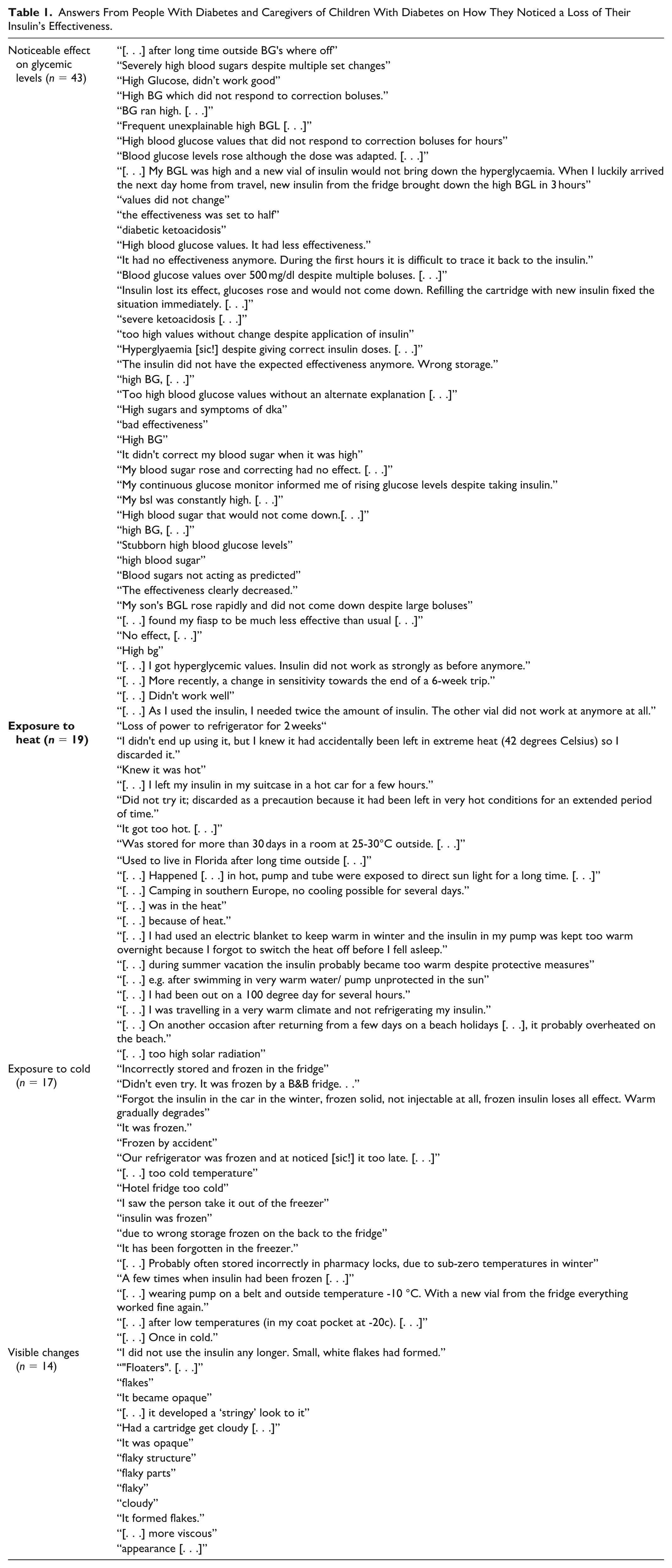
Although all groups (45% of HCPs, 51% of caregivers, 33% of PwD) have experienced incidents with a loss of insulin effectiveness as a suspected cause for glycemic instability, or even emergency situations, those cases were not sufficiently documented and remain underreported. Noticed effects were mostly glucose fluctuations outside their target range and ineffective correction doses (46%) and exposure to heat (20%). Of the PwD and caregivers who suspected a correlation of insulin storage and efficacy, only 30% ever discarded their insulin and renewed their prescription to replace it. The suspected causes for out-of-range temperatures included, for example, having left insulin in a car in summer or winter and the use of heat blankets at night (Table 1). Of the HCPs that witnessed such incidents with their patients, 43% suspected exposure to heat or cold, the use of expired (17%), or otherwise incorrectly stored insulin (26%). However, only 42% of them documented such incidents and the suspected cause in the patient record, and only 8% included the information in their medical report or discharge letter. Only one participant consulted the insulin manufacturer.
Answers From People With Diabetes and Caregivers of Children With Diabetes on How They Noticed a Loss of Their Insulin’s Effectiveness.
Given the importance of precise insulin dosing and the financial burden on PwD and caregivers due to increasing insulin prices and out-of-pocket expenses, there is an urgent need for more transparency of publicly available information on insulin stability and the impact of potentially harmful environmental factors as well as sufficient recommendations for daily practice. Based on published research to date, it was not possible to precisely quantify the potential decline of insulin potency caused by environmental temperature. However, this lack of knowledge and awareness can put PwD at risk of variations of glucose levels with an increased risk for severe consequences such as diabetic ketoacidosis. Participants appear to employ a variety of individual protection measures, which are often not appropriate, that is, reported measures like wrapping their insulin in a wet cloth or storing insulin on ice packs or ice cubes.
Because of the considerable number of participants who were not informed about the correct storage conditions and the potential structural changes, there is a need for better education of HCPs, PwD, and caregivers to prevent incidents in the future, reduce unnecessary waste of insulin, and allow safe and efficient diabetes management. Furthermore, research is needed to investigate this anecdotal correlation of temperature and insulin stability reported by the users, as those cases seem to rarely be documented.
Footnotes
Acknowledgements
The authors would like to thank Amin Zayani for his advice on the topic of insulin storage.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.