
Abstract
Background:
The use of flash-glucose monitoring system FreeStyle Libre (FSL) has demonstrated benefits in metabolic control and quality of life in different populations with diabetes mellitus (DM), being funded in many countries. Due to this, DM subjects on hemodialysis (HD) are using FSL despite the accuracy in this population being unclear. The aims of the present study are to assess the accuracy of FSL in DM subjects on HD, its relationship to hydration status, and patient satisfaction.
Material and Methods:
A prospective study in 16 patients with DM in a chronic HD program was conducted. Interstitial glucose values from FSL during a 14-day period were compared to capillary glucose measurements obtained at the same time. Hydration status was measured via bioimpedance spectroscopy. Satisfaction with FSL was obtained from an ad hoc satisfaction questionnaire.
Results:
A total of 766 paired interstitial and capillary glucose levels were analyzed. A correlation coefficient of 0.936 was determined and a mean absolute relative difference (MARD) value of 23%, increasing to 29% during HD. MARD was not related to hydration status. Interstitial glucose values were lower during HD (100.1 ± 17 mg/dL) than within the 12 hours after (125.1 ± 39 mg/dL; P = .012) and the days without HD (134.2 ± 32 mg/dL; P = .001). Subjects showed high satisfaction with FSL.
Conclusion:
The accuracy of FSL in DM patients on HD is lower than in other populations, especially during HD sessions and is not related with the hydration status. Despite this, the degree of patient satisfaction with FSL is very high.
Introduction
Diabetes mellitus (DM) is the main cause of chronic kidney disease (CKD) in developed countries 1 and the most powerful predictor of end-stage renal disease (ESRD). 2 The prevalence of both pathologies is progressively increasing.1,3
Maintaining consistent glycemic control is essential in the management of CKD. However, the management of DM is difficult due to the physiological changes caused by the disease itself, the hemodialysis (HD) treatment, and the wide variability in daily intrapatient glucose values. 4
The flash-glucose sensing FreeStyle Libre (FSL) provides a broader picture of the daily glucose profile, rather than the limited information provided by self-monitoring capillary blood glucose (SMBG), while simultaneously reducing the frequency of finger pricks. Not only real-time glucose values, but also glucose trends are given, allowing patients to take actions to prevent hyper- and hypoglycemia. This system has demonstrated a reduction in time in hypoglycemia, in particular nocturnal episodes related to patients with type 2 DM 5 and type 1 DM (T1DM), 6 and an improvement of glycemic control in some specific populations. FSL has been also tested in some groups with specific characteristics, such as pregnant women with DM with good accuracy. 7 Because of the proven benefits of FSL use, this device has been widely accepted by patients with DM and is currently funded in most of the developed world, mostly for T1DM, including Spain. Due to this, subjects with DM in HD are using FSL; however, to our knowledge this is the first study performed in Caucasian population and the largest study that evaluates the accuracy of FSL in patients with DM undergoing HD, in which rapid hemodynamic changes and volume and solute variations could reduce the accuracy of the measurement of interstitial glucose concentrations. Besides, body composition, specifically, the degree of water content may affect the accuracy of this device, as it measures glucose in interstitial fluid.
The aim of the present study was to assess the accuracy of FSL in patients with DM and ESRD in chronic HD, the possible effect of hydration status on the accuracy, and the degree of satisfaction with the system as perceived by the patients.
Material and Methods
A prospective study was designed including patients with DM in a chronic HD program, followed in the Department of Nephrology of Fundación Puigvert, during a period of four months (December 2018-April 2019). All patients underwent HD sessions with standard bicarbonate dialysate containing 100 mg/dL of glucose and the duration of the HD sessions was 3.5-4 hours. We prioritized patients in receipt of insulin treatment. Exclusion criteria were defined as patients being less than 18 years old, being in treatment with glucocorticoids, pregnant, patients where it was not possible to insert or use the device or not giving consent.
A total of 16 patients met the inclusion criteria, did not meet any of the exclusion criteria, and signed the informed consent form. As such, Ethics Committee of Fundación Puigvert approval was obtained. Clinical, anthropometrical, and DM-related data were collected from the patient’s medical records. Data on the current treatment for DM was directly acquired from patients. The hydration status of each participant was obtained before the first session of the study (in supine position and after five minutes rest) using a Bioimpedance (Body Composition Monitor by Fresenius Medical Care, version software 3.2).
In the first clinical visit, the FSL was inserted into each participating patient (in the contralateral arm of the fistula) and they were educated in its use. The correct use of the device was verified in HD sessions. The insertion was performed by trained healthcare staff and patients wore the system for up to 14 days. Throughout this period, patients were asked to measure the interstitial glucose values and the capillary glucose values (using the FSL reader for both measurements) at the same time (always with less than five minutes between one and the other measurement), six times a day (before main meals and two hours after). Patients were also asked to record, in an ad hoc data collection sheet, the results of both measurements, trend arrows, if it was a preprandial or postprandial measurement, time, dose of insulin in case of insulin therapy and other possible situations with a possible influence on glucose values (exercise, illness, stress. . .).
During the HD sessions, both glucose measurements and data were collected every hour by the patient or by trained nurses. After 14 days, the FSL was removed and the data were downloaded to the FSL Software. Patients were also asked to complete an ad hoc satisfaction questionnaire, indicating from 0 to 5 the degree of agreement with the questions asked, where zero signified totally disagree and 5 signified totally agree.
Results were expressed as frequencies and percentages of qualitative variables and as the mean and standard deviations of quantitative variables. Normality of data distribution was evaluated using the Kolmogorov–Smirnov test. Student’s t-test, or Mann–Whitney test and Pearson correlation were used to analyze quantitative variables, and chi-squared was used for qualitative variables. Mean absolute relative difference (MARD) was also used to evaluate analytical accuracy of the system. Downloaded glucose values from FSL were compared with all temporary matched (±5 minutes) capillary blood glucose values. All matched measurements were evaluated regardless the glucose trend. All statistical tests were considered significant at P <.05. Statistical analysis was performed using the SAS statistical package (version 9.3).
Results
A total of 16 patients were included in the present study. Baseline characteristics are listed in Table 1.
Baseline Features of the Subjects with DM Included in the Study.
BMI, body mass index; HbA1c, hemoglobin A1c; HD, hemodialysis; OAD, oral antidiabetic drugs; T1DM, type 1 diabetes; T2DM, type 2 diabetes.
Mean ± SD.
Two of the patients withdrew prematurely from the study (on the fourth and seventh day, respectively); one as a result of a kidney transplantation and the second as the FSL had to be removed for a radiological exploration (magnetic resonance image).
Mean interstitial glucose value during the entire period was 118.5 ± 29 mg/dL, being significantly lower during the HD sessions than within the 12 hours after HD (100.1 ± 17 mg/dL vs 125.1 ± 39 mg/dL, respectively; P = .012) and the days without HD (134.2 ± 32 mg/dL; P = .001). No differences were found between the mean interstitial glucose within the 12 hours after HD and the days without HD (P = .352).
All patients, except for one, experienced slight overhydration.
A total of 766 paired capillary blood glucose and sensor interstitial glucose values were used for the correlation analysis. The correlation coefficient for all paired values was r = 0.936; P = .000 (−33.2 ± 19.6 mg/dL), markedly lower during HD (r = 0.894; P = .000). Interstitial glucose values were lower than capillary glucose values, as shown in Figure 1.
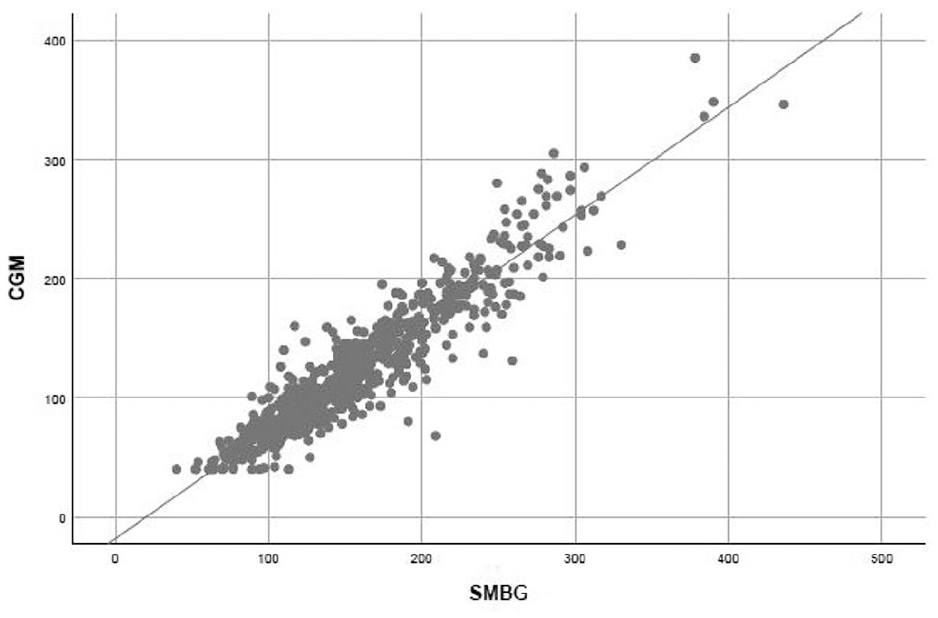
Scatter plot showing the correlation between interstitial glucose values obtained from FreeStyle Libre in mg/dL (CGM) and capillary glucose values in mg/dL (SMBG). r = 0.936 (P = .000).
The global calculated MARD was 23%. Figure 2(a) and (b) shows the global MARD and the MARD in the different analysis windows and for different glucose value. MARD was higher during HD sessions than in the other analysis windows (Figure 2(a)) and was also higher for glucose values on target (70-180 mg/dL) or below target (<70 mg/dL) (Figure 2(b)). MARD was slightly better for glucose values above glucose target (>180 mg/dL) (Figure 2(b)). We made a subanalysis of the paired values with two minutes or less measurement lapse (91.25% of total values), where a global MARD value of 23% was obtained.
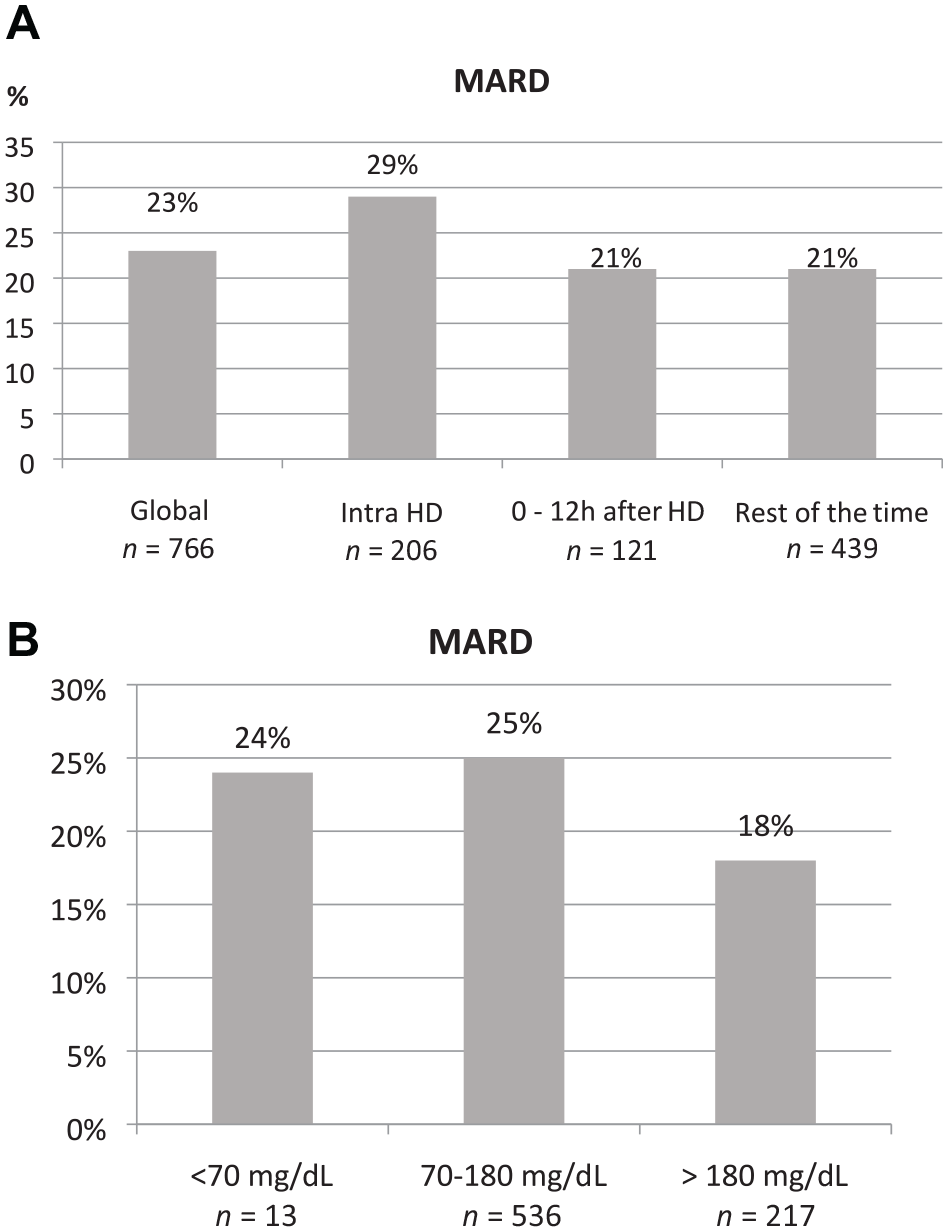
(a) Global calculated MARD and in the different analysis windows. n = number of paired values used for calculation. (b) MARD values obtained for euglycemia, hyperglycemia, and hypoglycemia. n = number of paired values used for calculation.
No statistically significant correlation was found between the interstitial glucose values obtained from FSL and the hydration status measured by bioimpedance spectroscopy (r: 0.416, P = .178), age (r: −0.201, P = .456), DM duration (r: 0.031, P = .910), or body mass index (r: −0.202, P = .453).
A total of 14 patients fulfilled the satisfaction questionnaire. Most of the subjects were highly satisfied with the FSL, considering its use very easy and useful for DM management. Main results of the questionnaire are shown in Figure 3.
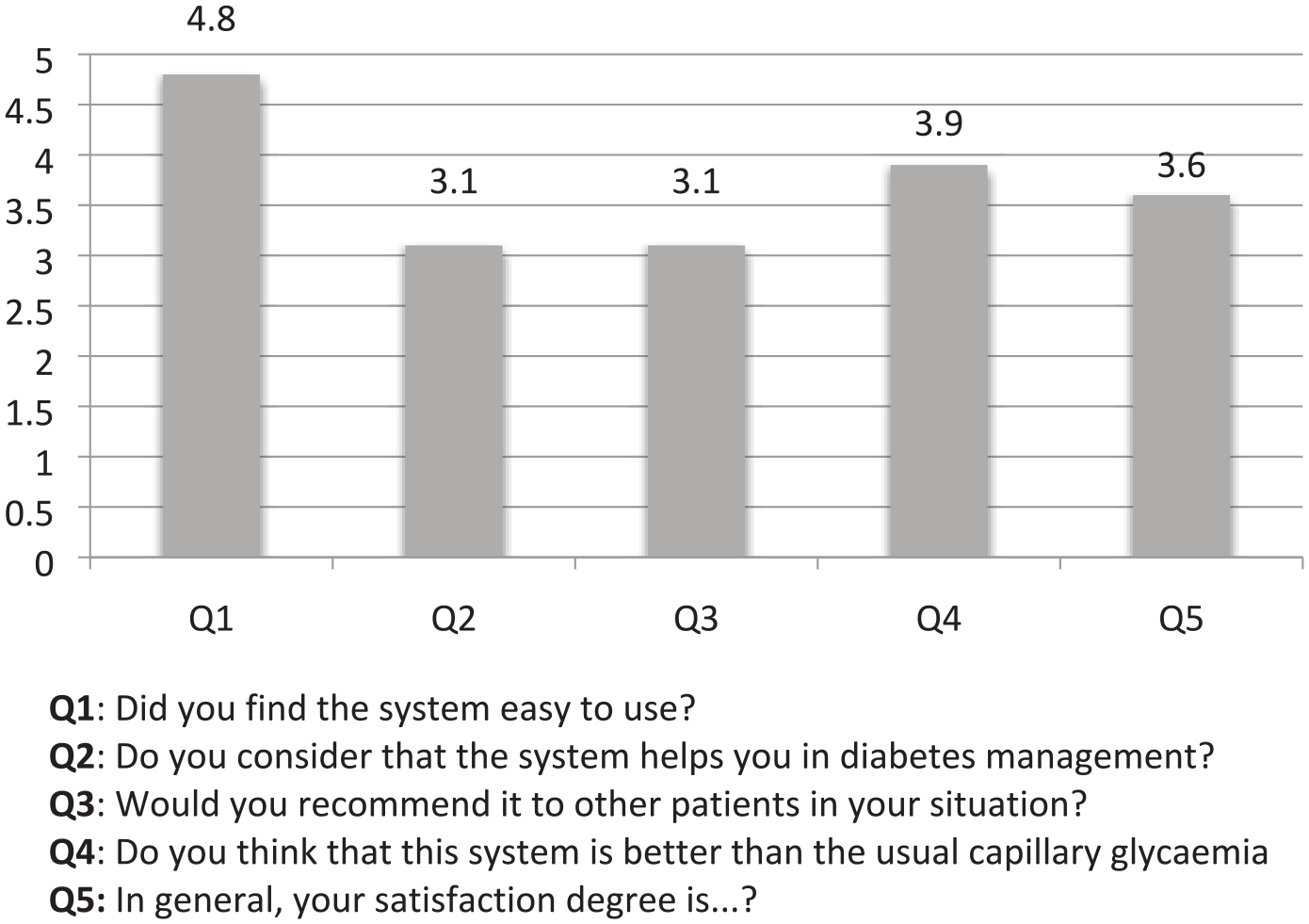
Results obtained from the satisfaction questionnaire.
Discussion
The present study is the first that evaluates the accuracy of the FSL system in Caucasian subjects with DM and ESRD on HD, as well as the degree of satisfaction with its use. In the population analyzed, the correlation found between the capillary blood glucose levels and the interstitial glucose levels was high. However, the global calculated MARD was worse than previously reported in other populations with DM, and also the MARD separately analyzed in three different analysis windows: during HD sessions, between 0 and 12 hours after HD and from 12 hours after HD until the new HD. The degree of satisfaction reported by the patients with FSL use was very high.
Lower interstitial glucose concentrations were found during HD compared to the other two analysis windows. In our knowledge, only four studies have evaluated glucose concentrations and glycemic variability in patients on HD using continuous, or flash glucose monitoring systems, with nonconcordant findings. In the study performed by Mirani et al, 8 they found a higher mean glucose value on the day of HD and also higher glycemic variability. However, the study by Kazempour-Ardebili, 9 and a recent study with the flash glucose monitoring system, 10 showed lower glucose levels on days when HD occurred. Jung et al did not find any differences in glycemic control 11 between HD and non-HD days. These discordant published patterns may be explained due to the small number of patients involved, the different types of DM treatments, and a potentially lower accuracy of the FSL system during HD.
The global correlation found between capillary blood glucose and interstitial glucose in present study (r > 0.9) is similar to that previously reported when evaluating other populations, such as pregnant women 7 or patients with T1DM. 12 However, when calculating the MARD, we found worse values in these patients compared to the populations mentioned before (23%). Furthermore, this accuracy is still lower during the HD sessions with an increased MARD of 29%. To our knowledge, there is just one study 13 that analyzes the accuracy of a flash glucose monitoring system in patients undergoing HD. This study was performed in Asian population, with a smaller number of paired samples (104) and using the Free-Style Libre Pro, also found a poorer MARD (overall MARD: 19.5%) with FSL Pro compared to SMBG and continuous glucose monitoring (CGM) system. In line with our study, they also found lower levels with the FSL Pro system and better MARD for glucose values >180 mg/dL.
We have no evidence to explain our findings. One hypothesis could be that the hypervolemia observed in patients with ESRD on HD induces diluted glucose levels in the interstitial space, with the consequent lower reading. This would explain the worsening of MARD in HD since patients begin sessions in a state of maximum hydration. In the present study, hydration status measured by bioimpedance spectroscopy was not related with the correlations obtained between both glucose measurements, but all patients, except one, were slightly overhydrated, which may potentially explain the difference observed in this population compared to others. However, in the study performed by Yajima et al, 13 they found a lower MARD in CGM system, which measures the interstitial glucose as well; however, this was measured in the abdomen and not the arm. Another factor that can influence the MARD value could be rapid changes in glucose levels during HD. 9 Further studies are needed to confirm this MARD in this subgroup of DM patients and to explain mechanisms that could affect the accuracy of the system.
The main limitation of this study is the small number of patients included. Nonetheless, the main strengths of this study are its prospective nature and, that despite the small number of patients, the large volume of glycemic data collected from each patient provides statistical weight to the correlation analysis.
In conclusion, despite being well valued, the flash-glucose sensing FSL in patients with DM and ESRD in HD seems to be less accurate than in the general population with DM. According to our findings and until more studies are done to clarify this, patients in HD should be advised about the accuracy of the FSL to enable better clinical decisions and we recommend to perform a capillary blood glucose measurement to make therapy decisions.
Footnotes
Acknowledgements
We thank Abbott Laboratories for their support in this work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Genua reports nonfinancial support from Sanofi, Novonordisk, Lilly, MSD, and Esteve, outside the submitted work. Dr Sánchez-Hernandez reports personal fees for speaking/consulting from Almirall S.A. and Abbott Laboratories, S.A, outside the submitted work. MJ Martínez reports personal fees from Roche, Abbott, Menarini, and MSD. I. Pujol, J. Places, C. González, Dr Martinez, and JM Díaz have nothing to disclose. Dr Chico reports nonfinancial support from Roche, Medtronic, Abbott, Novalab, Sanofi, Novonordisk, Astra, Lilly, Boehringer, MSD, and Esteve, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.