
Abstract
Introduction:
Despite advances in the management of type 1 diabetes (T1D), there is an increasing incidence of skin reactions related to diabetes devices such as patch pumps and glucose sensors. Aim of the present study was to assess the prevalence of dermatological complications in pediatric patients with T1D using technological devices.
Methods:
Online survey regarding skin reactions related to the use of patch pumps and/or glucose sensors was administered to families of children and adolescents (0-17 years) with T1D. Data were collected on demographic characteristics, duration of diabetes, and clinical features of dermatological complications if present.
Results:
Our study population consisted of 139 patients (female 51.8%) aged 11.1 ± 3.3 years. More than half (51.1%) experienced skin reactions due to patch pumps or glucose sensors. Dermatological complications were mainly caused by continuous glucose monitoring (56.3% of total). Timing of appearance of dermatological reactions varied from a few days to several months after the introduction of the device. The application of hypoallergenic barrier bandages was the most frequently adopted measure to solve the issue.
Conclusions:
Our study confirmed high frequency of dermatological complications among pediatric patients with type 1 diabetes. Well-designed studies are awaited to provide clear recommendations to minimize the burden of skin issues related to technological devices.
Introduction
In the past two decades, technology has acquired a crucial role in the management of type 1 diabetes (T1D). It is estimated that about 75% of children and adolescents with T1D use medical devices such as continuous subcutaneous insulin infusion (CSII) pump or continuous glucose monitoring (CGM) systems. 1 CSII allows to simulate the physiological insulin secretion with its circadian variations. 2 Among others, a subtype of CSII is now recognized which is applied directly on the skin at the infusion site without external tube, also known as “patch pump”. 3 CGM system allows to monitor the current glucose value in real time. Two types of CGM systems are currently available: real-time CGM (rtCGM) and intermittently scanned CGM (iCGM), also called flash glucose monitoring (FGM). 4 To maintain clear distinction throughout this article, we will refer to these devices as CGM and FGM.
The impact of technology on adherence and glycemic control has been well demonstrated. Benefits due to the advance of technology include improved glycemic outcomes, fewer episodes of severe hypoglycemia, and reduction in the rate of diabetic ketoacidosis.5,6
Despite these benefits in the management of T1D, an alarmingly increasing rate of skin reactions related to the use of technological devices has been emerging. 7 The recurrent application and the long wearing time (up to 14 days) of the adhesives used to ensure pumps and sensors to the skin are related to a high risk to have dermatological complications, which are barriers to continuous use. Case reports on skin reactions caused by devices used for the management of T1D have been increasingly described in the literature, as well as observational studies and intervention trials that discuss cutaneous complications due to patch pump or CGM/FGM have been recently conducted.8-11 The most reported skin reactions due to technological diabetes devices are scarring, lipodystrophies (including both lipohypertrophy and more rarely lipoatrophy), irritant contact dermatitis, and allergic contact dermatitis. These are usually characterized by intense itching and represent tricky dermatological issues since they are related to a certain risk of developing a secondary bacterial infection.
Methods
We conducted a cross-sectional survey based on an online questionnaire filled out by patients’ parents between June and December 2019.
Survey participants were patients with T1D who use technological diabetes devices followed-up at Pediatric Diabetes Center in Turin and Messina. Patients’ parents gave their written informed consent through the online form before completing the questionnaire. Inclusion criteria were represented by the duration of T1D for at least 3 months and the use of technological devices for more than 1 month. Exclusion criteria were the inability to complete the questionnaire. Out of 180 patients who were randomly recruited and invited to take part in the study, 139 (77.2%) agreed to participate. The questionnaire included questions on the following items: demographic characteristics; diabetes duration; type of insulin treatment; duration of the use of patch pump, FGM, or CGM; occurrence, timing, and severity of dermatological complications if present; and measures taken in the event of skin reactions. Particularly, we focused on skin reactions typically characterized by erythematous lesions.
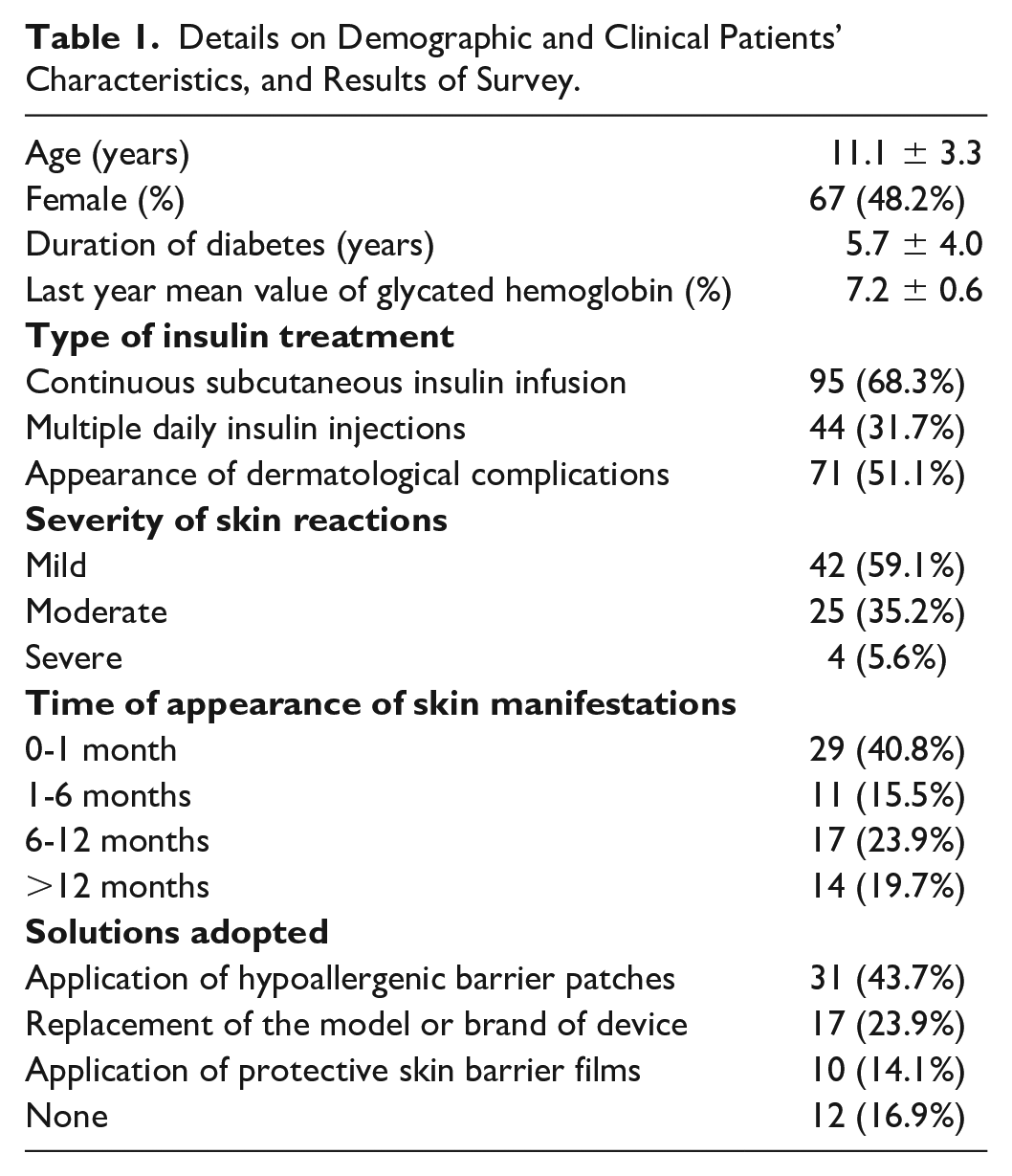
The severity of dermatological complications was divided into three classes: a mild reaction (faint homogenous erythema without infiltration), a moderate reaction (defined if erythematous lesions with infiltration and small vesicles were present), and a severe reaction (characterized by intense erythema with coalescing vesicles and bullous skin lesions). To facilitate the definition of severity, participants were asked to characterize the type of skin reaction in comparison with photographs of various skin conditions due to pumps or glucose sensors (Figure 1). The photographs used as examples of different skin conditions were taken from our clinical experience. Demographic and clinical patients’ characteristics and the results of questionnaire were statistically analyzed. The numerical data were expressed as mean and standard deviation and the categorical variables as absolute frequencies and percentages (Table 1). In order to compare patients with and without skin reactions, we applied unpaired t-test for numerical parameters and ChiSquare test for categorical variables. A P-value <.050 was considered to be statistically significant.

The three photographs characterizing the severity of skin lesions.
Details on Demographic and Clinical Patients’ Characteristics, and Results of Survey.
Results
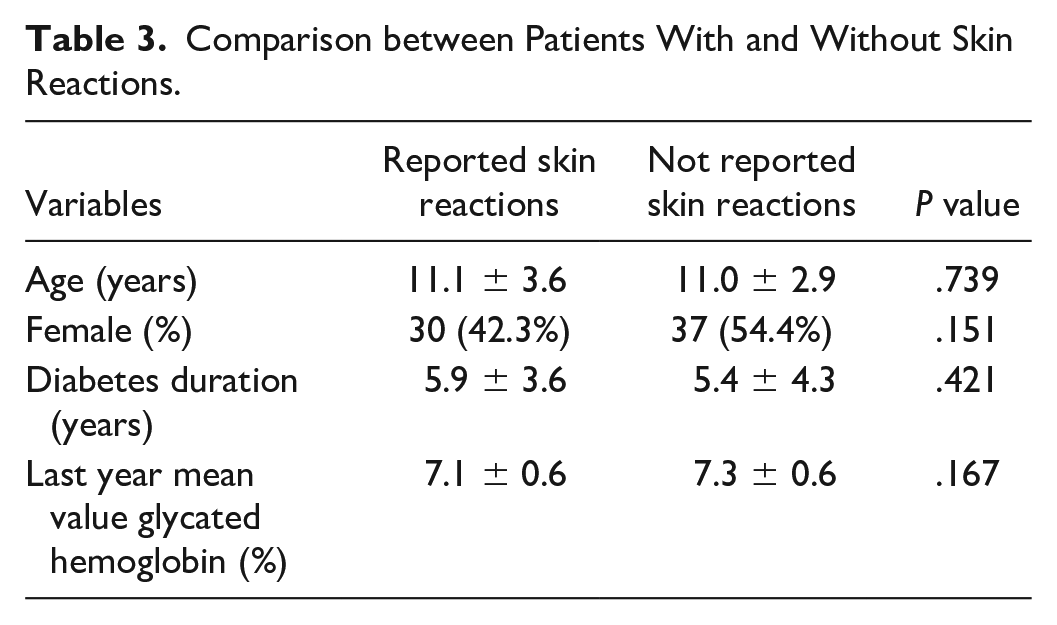
Mean age of our study population was 11.1 years (range 4-17 years) with a homogenous distribution between male and female (48.2% and 51.8%, respectively). Mean duration of T1D was 5.7 years. Almost all patients presented a suboptimal glycemic control as demonstrated by the last year mean value of glycated hemoglobin (7.2 ± 0.6%, 55 ± 7 mmol/mol). Over half of patients (51.1%) experienced dermatological complications due to patch pumps or glucose sensors. Of these, 59.1% referred to mild reactions, 35.2% reported moderate reactions, and 5.6% of patients had severe skin reactions. Dermatological issues were mainly present in subjects wearing CGM (56.3% of total cases). FGM and patch pump users reported a skin lesion rate of 35.3% and 8.4%, respectively (Figure 2). The distribution of CSII, CGM, and FGM users, as well as the correct percentages of skin reactions due to the different technological devices among our study participants, is shown in Table 2. The timing of appearance of dermatological reactions varied from a few days to several months after the introduction of these devices. The majority of patients solved the problem by applying hypoallergenic barrier patches and bandages (43.7% of the total cases). In accordance with the diabetes specialist’s decision, 23.9% of patients replaced the model or brand of the “culprit” device. Ten subjects (14.1%) used barrier films for skin protection, while 12 patients (16.9%) adopted no solutions considering the problem as not very influential. One patient was forced to discontinue any type of continuous or flash monitoring system due to the persistence of skin lesions, and she was switched back to self-monitoring blood glucose. Finally, there were no significant differences in age, gender, duration of T1D, and last year mean value of glycated hemoglobin between patients with reported skin reactions and other study participants (Table 3).
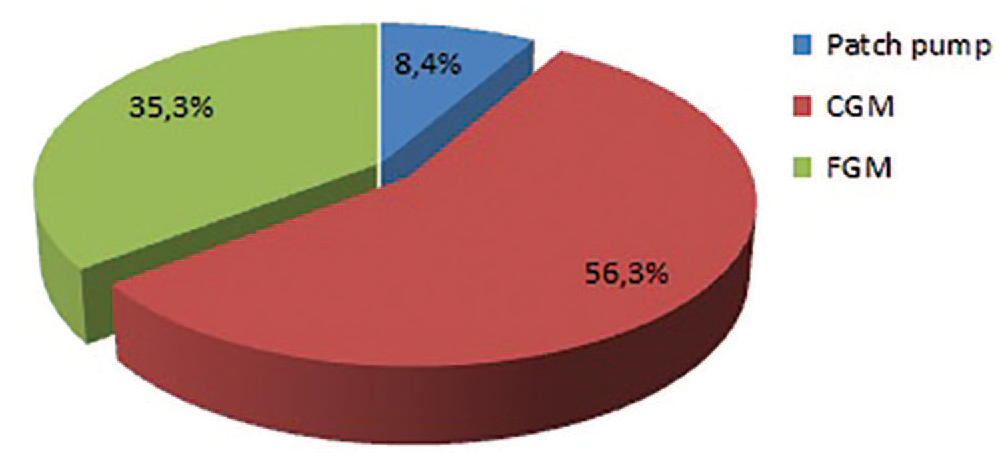
Distribution of different diabetes device responsible for dermatological complications among patients who reported skin issues.
Relationship between Skin Reactions and the Total Number of Patients Wearing Different Technological Devices among Our Study Participants.
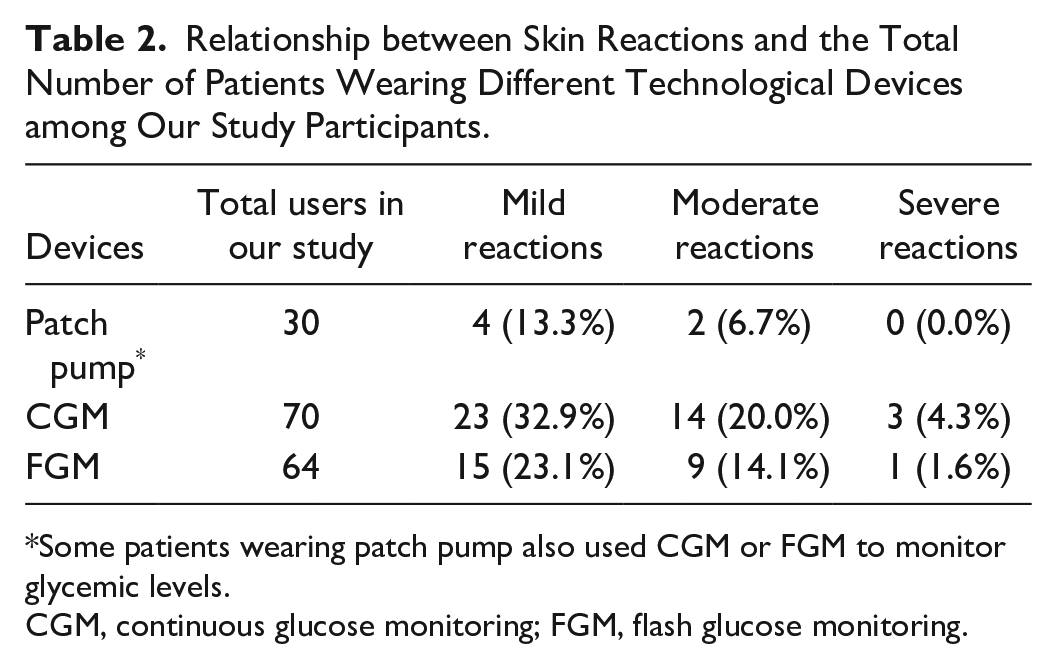
Some patients wearing patch pump also used CGM or FGM to monitor glycemic levels.
CGM, continuous glucose monitoring; FGM, flash glucose monitoring.
Comparison between Patients With and Without Skin Reactions.
Discussion
More than half of the pediatric patients wearing technological devices for the management of T1D experience dermatological complications. Our findings are in accordance with the results reported by other recent studies. Berg et al demonstrated a rate of 63% of cutaneous complications among CSII users and a rate of 46% of skin reactions among children who regularly used glucose sensors. 12 Another study showed that 43% of patients experienced skin complications related to insulin infusion sets. 13 These data are similar to those founded by Al Hayek who reported that 48.2% of adolescents on CSII therapy had dermatological unwanted effects. 14 Allergic contact dermatitis (ACD) is the most insidious among skin-related complications. ACD is a delayed-type allergic hypersensitivity reaction, which is caused by a T cell-mediated immune reaction to usually harmless allergens. Clinical manifestations of ACD include erythema, edema, vesicles, oozing, and intense pruritus. 15 Although it is considered that ACD is less frequent than other milder dermatological conditions, there is a strong impression that the real prevalence of this condition in children and adolescents with T1D is higher than commonly expected. 16 One of the main causes of the increasing prevalence of ACD is the exposition of a potent allergen. The longer insertion time than in the past may allow the allergen to forward sensitization.17,18 One of the worst consequences related to ACD is pruritus, which may also cause “bad school performance” with tiredness and impaired concentration due to itching during nights. The influence of pruritus on the determination of the patient’s tolerance for skin lesions is well known. Some patients even use antihistamines to relieve the itching sensation with the potential risk of adverse sedating effects. 19
Several factors may promote the appearance of skin reactions in T1D pediatric patients. One of these is the compromised integrity of the skin that may be related to pre-existing skin diseases such as atopic dermatitis. Repeated taping of the same sites may be the leading cause of cutaneous damage due to the trauma of repeated insertions. Careless removal of adhesive tapes, if made with excessive force and energy, may increase the risk of tissue damage. Another crucial aspect is represented by the components contained in the adhesives of patch pumps and glucose sensors. Unfortunately, the exact composition and preparation of adhesives used by various manufacturers are rarely available, since single elements quantity may vary in the ratio in each device. However, several threatening compounds included in diabetes devices have been identified. Among these, isobornyl acrylate (IBOA), N,N-dimethylacrylamide (DMAA), and colophonium seem to be the most harmful agents. IBOA is a photopolymerizable acrylate monomer, and it is used, in its liquid form, in coatings, sealants, glues, adhesives, paints, and inks and also as a plasticizer in various plastic materials. 20 In 2016, the presence of IBOA was discovered in a popular glucose sensor. Several studies have since confirmed the role of IBOA as the culprit sensitizer causing ACD in patients using the same glucose sensor.21,22 DMAA is frequently used as a monomeric diluent in ultraviolet curing adhesives. Small amounts of DMAA were recently identified in the adhesive patch of the FGM sensor. 23 Colophonium is a natural substance derived from pine trees, and it is used in both unmodified and modified forms as a fast-acting adhesive for industrial, medical, or other commercial uses. 24 Colophonium was found in both glucose sensors and patch pumps. Positive patch test reactions to colophonium were observed in numerous patients wearing diabetes devices containing this substance.9,21,25
To manage the emerging issue of skin reactions in young patients with T1D, several preventive measures have been put forward. Recently, Messer et al proposed a practical comprehensive guidance to preserve the skin integrity of patients who chronically use diabetes devices. The authors shared tips on the correct device placement, prophylactic skincare, accurate removal techniques, and promoting skin healing. In addition, they suggested the application of various barrier agents to minimize the risk of hypersensitivity reactions. 26 This preventive solution appears to be the most frequent choice among pediatric patients with T1D, as demonstrated by our results. The majority of individuals apply hypoallergenic (hydrocolloid and/or silicone-based) plasters for blocking adhesives from sensors and pumps from the contact with the skin. 27 For some patients, liquid barriers may offer sufficient protection from adhesive agents. Based on our experience, we consider that these skin protective devices are very useful and, in most cases, allow to solve dermatological complications so that patients may continue to use the potentially harmful device. These barrier films are mostly only useful in milder irritations but not in ACD. They are not able to prevent a potent allergen from migrating into the skin. Furthermore, they can be irritative to skin itself. 28
Another solution that is increasingly being adopted is the off-label use of fluticasone propionate nasal spray. This nasal steroid is commonly used by patients with allergic rhinitis. Benefits of applying fluticasone propionate spray to the skin were recently reported by Paret et al who described their real-life experience with 12 patients suffering from local skin irritation due to CGM. The authors demonstrated that spraying two puffs of the steroid on the skin area prior to adhesion of glucose sensor significantly reduced the degree of cutaneous irritation. 29 However, there are no studies on the long-term use of nasal steroids applied topically, and their use is widely debated.
Finally, the recognition and avoidance of the sensitizing agent contained in the adhesives used to secure patch pumps and sensors to the skin remain the landmark of the management in the event of ACD. 16
Conclusions
Our survey confirms the high frequency of dermatological complications in patients with type 1 diabetes. Skin reactions due to technological devices represent a clinical condition that diabetes specialists must learn to know and manage in a proper way. The physicians should also constantly report the occurrence of skin adverse reactions to device manufacturers. There is a compelling unmet need for companies to supply detailed information about allergens and irritants contained in their devices.
The persistence of dermatological concerns increases the risk of diabetes-related emotional distress. Although several preventive measures are available so far, there are no clear and universal recommendations on the most suitable management plan. We remark the need for well-designed studies to minimize the burden of diabetes devices and to optimize the quality of life for people with diabetes.
Footnotes
Authors’ Contributions
SP and DT collected the data, drafted, and wrote the paper; GS and MFM helped write the paper; FL contributed to discussion and reviewed the paper; IR conceived the study and reviewed the paper. The paper has been read and approved by all the authors, and each author considers that the paper represents their honest work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.