
Abstract

The alarming spread of the SARS-CoV-2 virus makes it necessary to find the right measures to prevent and combat the coronavirus disease (COVID)-19 pandemic. 1 Researchers have identified angiotensin converting enzyme II (ACE2) as the likely receptor with which SARS-CoV-2 infects human cells.2,3 Recent findings suggest that ACE2 is highly expressed in the oral cavity 3 and detectable virus concentrations were found in saliva.4,5 Hence, the virus may predominantly enter the body via the oral mucosa. Gum disease (periodontitis) is known to cause ulceration of the gingival epithelium and weaken the protective function of the buccal mucosa. It can be postulated that this exposed ulcerated surface increases the risk of invasion by SARS-CoV-2.
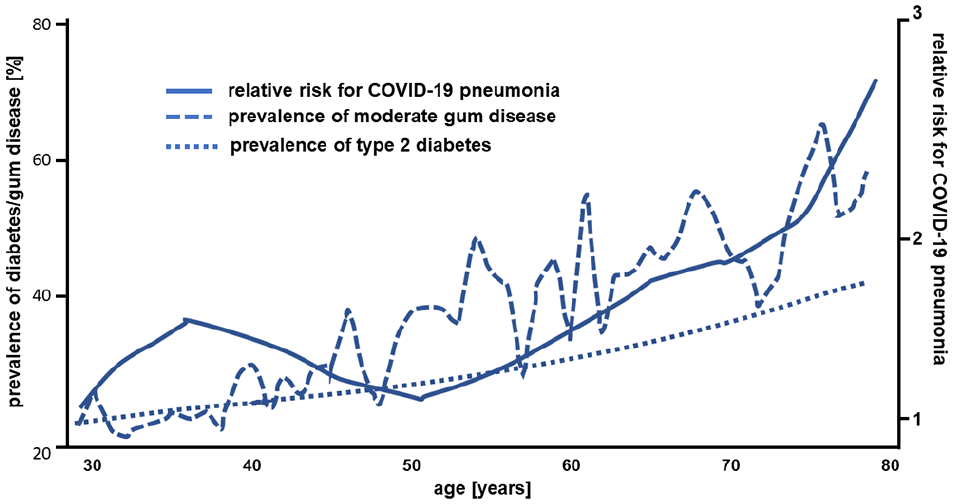
The current population-based analyses of the severe COVID-19 courses in China 6 show a clear correlation with higher age, which is similar to the correlation between age and the prevalence of periodontitis, and also similar to the well-known correlation between age and diabetes prevalence (Figure 1).7,8 A further indication is the current COVID-19 mortality statistics in which European countries without regular and state-supported oral hygiene consultations and treatments (such as Belgium, Italy, and Spain), with comparable infrastructure and living standards, have significantly higher mortality rates per one million inhabitants (state on April 2, 2020: 606, 490, and 436, respectively) than countries with well-established oral hygiene programs (such as Germany: 71, Austria: 61, or Norway: 38 9 ).
Diabetes is a risk factor for gum disease and it is necessary to pay attention to possible oral complications in the early stages. The International Federation of Diabetes (IDF) 10 recommends that regular diabetes screenings should be supplemented by an annual oral cavity assessment for gum disease, including bleeding while brushing or inspection for swelling. Hyperglycemia causes damage to the connective tissue in the oral cavity with reduced synthesis of gum fibroblasts, resulting in the loss of periodontal fibers and alveolar bone. 11 In addition, impairment of the phagocytic activity of mononuclear and polymorphonuclear cells has been observed, leading to the development of aggressive pathogenic subgingival flora. Periodontal infection can therefore induce systemic inflammation, which in turn builds up or reinforces chronic insulin resistance. A vicious circle of hyperglycemia, periodontitis and connective tissue degradation, inflammation (oral and systemic), and insulin resistance develops, which is virtually uncontrollable for all disorders without effective intervention. 11
A recently published long-term study provided impressive evidence for the value of oral care in the primary prevention of pneumonia in people with diabetes. The investigators analyzed this association in 98 800 people in Taiwan over a period of 12 years. The authors concluded that patients who received intensive periodontal treatment had an average 66% lower risk of pneumonia. Patients with diabetes had a 78% increased risk of developing pneumonia compared to the control group. 12 These findings indicate that the multimorbid patient with diabetes and periodontitis as a comorbidity has a frighteningly high risk of pneumonia even without SARS-CoV-2 infection.
The association between diabetes and increased COVID-19 mortality may be related to the aspects described above but also to additional systemic effects of periodontitis. Periodontal disease affects blood sugar levels and impairs the innate immune system. Periodontitis also increases systemic inflammation, as host-derived mediators of periodontal disease and tissue destruction (eg, cytokines and metalloproteinases) are released from the inflamed periodontal tissue into the circulatory system. 13 It is known that patients with diabetes have an increased risk of mortality from concomitant oral diseases, while patients with periodontitis have a demonstrably higher risk of diabetes. 14 In this context, biomarkers such as activated matrix metalloproteinase 8 (available as a laboratory or saliva rapid test) offer the possibility of identifying patients at risk for diabetes and thus making it accessible for targeted prevention.15,16
A well-functioning gingival epithelial barrier can help to prevent pathogenic viruses and bacteria in the oral cavity from entering the bloodstream. This means that regular daily tooth brushing with additional application of disinfectant mouthwash up to the posterior pharynx, especially in patients with diabetes, could potentially help to reduce the potential systemic consequences of a SARS-CoV-2 virus infections. The dentist and the diabetes specialist should advise patients with diabetes to have regular check-ups and dental hygiene treatments.17,18 This targeted prevention strategy, with additional recommendations for monitoring and maintaining oral health, can be a quick and simple approach to protection against the current coronavirus pandemic. COVID-19 does not stop at borders; it is a global challenge, and solutions to this pandemic will require an interdisciplinary alliance of experts in all fields, including dentistry, periodontology, and diabetology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.