
Abstract
Background:
To summarize new evidence regarding the methodological aspects of blood glucose control in the intensive care unit (ICU).
Methods:
We reviewed the literature on blood glucose control in the ICU up to August 2019 through Ovid Medline and Pubmed.
Results:
Since the publication of the Leuven studies, the benefits of glycemic control have been recognized. However, the methodology of blood glucose control, notably the blood glucose measurement accuracy and the insulin titration protocol, plays an important but underestimated role. This may partially explain the negative results of the large, pragmatic multicenter trials and made everyone realize that tight glycemic control with less-frequent glucose measurements on less accurate blood glucose meters is neither feasible nor advisable in daily practice. Blood gas analyzers remain the gold standard. New generation point-of-care blood glucose meters may be an alternative when using whole blood of critically ill patients in combination with a clinically validated insulin dosing algorithm.
Conclusion:
When implementing blood glucose management in an ICU one needs to take into account the interaction between aimed glycemic target and blood glucose measurement methodology.
Blood Glucose Control: The Clinical Trials
It has been known for a long time that blood glucose levels correlate well with the outcome of critically ill patients, following a J-shaped relationship (Figure 1). 1 Both hyperglycemia and hypoglycemia are associated with increased mortality and morbidity.2-5 Similar relationships between blood glucose levels and the outcome are found in patients suffering from acute myocardial infarction and stroke. However, it is important to realize that this relationship is affected by long-term exposure to blood glucose levels before the acute phase of critical illness. Therefore, the latter relationship is blunted and shifted toward higher glycemic levels in patients with established diabetes, certainly in the ones with poorly controlled diabetes. This also explains the stronger correlation between new-onset hyperglycemia in acute critical illness and poor outcomes in patients, who were not known to have diabetes mellitus. 6 However, a significant number of these patients may have undiagnosed diabetes mellitus. 7
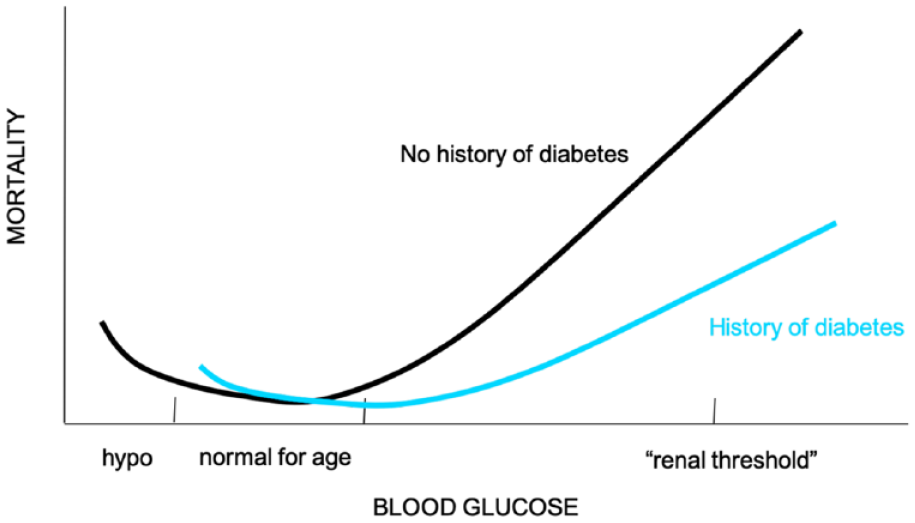
J-shaped curve showing negative effects for both hypoglycemia and hyperglycemia.
Before the landmark studies by Greet Van den Berghe in the early 2000s, blood glucose control (BGC) in the intensive care unit (ICU) was mainly reserved for patients with diabetes. Higher blood glucose levels up to 215 mg/dL were generally not acted upon by physicians. 1 In patients without diabetes, higher blood glucose levels were generally tolerated without intervention, under the premise that hyperglycemia would eventually resolve since the patient did not have diabetes mellitus.
In 2001, their first randomized controlled trial (RCT), tight glycemic control (TGC), in comparison with conventional BGC, reduced mortality and morbidity in critically ill patients, mainly admitted after surgery. This study applied a TGC, targeting blood glucose levels between 80 and 110 mg/dL. In the conventional group, blood glucose levels up to 215 mg/dL were accepted, and insulin administration was ceased when glycemia fell below 180 mg/dL. TGC was achieved by a nurse-driven protocol. A blood gas analyzer was used to make frequent measurements of glucose concentrations in arterial blood. Insulin was only administered intravenously via a central line. Basically, all patients admitted to the ICU were included in the trial, leading to a high level of expertise among the nursing staff.
In 2003, Krinsley et al showed similar benefits in a well-controlled study in medical critically ill patients. 8 However, the single-center RCT by the Leuven group on TGC in the medical ICU only showed effect in prolonged critically ill patients (ICU stay over 3 days), using the same TGC protocol as in the surgical ICU RCT. 3 It appeared that single-center studies using a very standardized protocol in all admitted patients, in combination with a high level of expertise of ICU staff, showed benefit of TGC in comparison with very loose glycemic control.
Several large multicenter trials, such as the normoglycemia in intensive care evaluation and survival using glucose algorithm regulation (NICE-SUGAR) study (n = 6104), Glucontrol study (n = 1101), VISEP (n = 537) and the studies by Arabi (n = 523) and De La Rosa (n = 504), did not succeed in reproducing the same benefits with TGC.9-13 These studies were not only pragmatic, reflecting the daily setting of critical care, but also allowing more variability in the execution of the study protocol. Another crucial difference with the original Leuven studies on TGC is that the large multicenter trials compared TGC with intermediate BGC (<145 mg/dL), instead of no control (<215 mg/dL) (Table 1).
Key Differences between Leuven Studies and NICE-SUGAR Study.
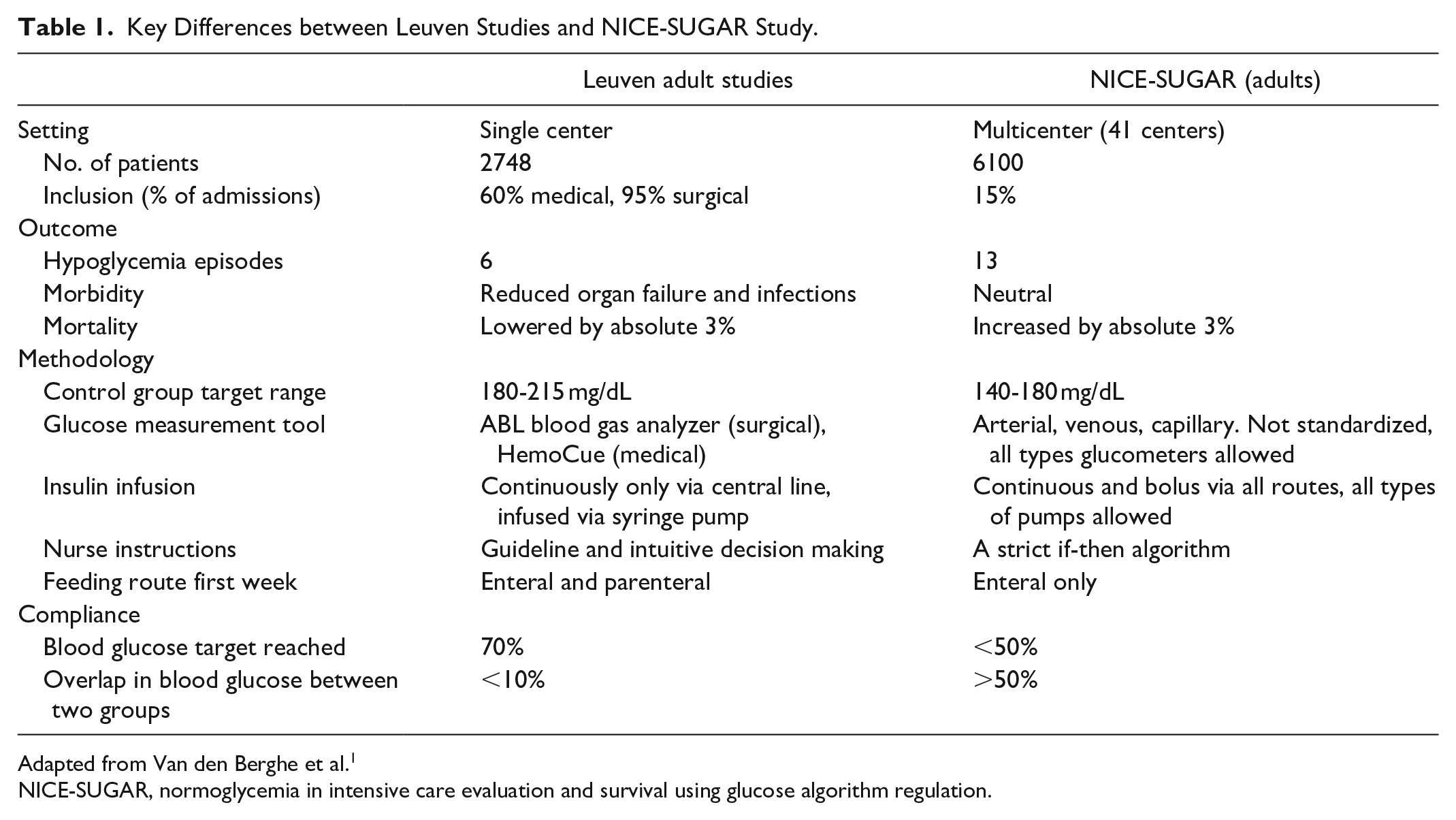
Adapted from Van den Berghe et al. 1
NICE-SUGAR, normoglycemia in intensive care evaluation and survival using glucose algorithm regulation.
This discrepancy between the Leuven single-center studies with high internal validity (strict study protocol) and the large multicenter studies with low internal validity, but higher external validity or generalizability, led to important controversy on the benefit of TGC.14-16 All meta-analyses and systematic reviews conclude that TGC does not reduce mortality, but increases the incidence of hypoglycemia strongly.17,18 Insulin-induced hypoglycemia may thus be the culprit in mitigating the benefits of TGC.
The Balancing Act: Controlling Hyperglycemia While Avoiding Hypoglycemia
After the publication of these contradicting clinical trials and the ensuing controversy, a unifying approach emerged, going from intensive insulin therapy over TGC to the current practice of blood glucose management (BGM). There is now a wide consensus on the negative effects of both long episodes of hyperglycemia and even short episodes of severe hypoglycemia.19,20 In the framework of current BGM, the goal is therefore to avoid exposure to hyperglycemia (>180 mg/dL) and severe hypoglycemia (<40 mg/dL), thus accepting a wider range of blood glucose levels that do not require insulin administration. The importance of adequate glucose control is stressed by several international guidelines, such as the American Diabetes Association (preprandial 90-130 mg/dL, postprandial <180 mg/dL) and the Society for Critical Care Medicine (70-150 mg/dL at any given point).21,22 More importantly, we believe that the emphasis should shift from a preoccupation with target ranges to the selection of the patient populations which may benefit the most of BGM and even more important to the methodological aspects of BGM.
The basics of any BGC or BGM remain rock steady. To know the blood glucose level and to act upon, it needs to be measured, frequently. The blood glucose measurement has to be accurate as its value is used in a BGC algorithm to initiate or adjust insulin administration. This algorithm may be a skilled bedside nurse or a sophisticated computer program. The resulting insulin administration needs to be reliable by avoiding unnoticed interruptions or boluses. Everyone involved in BGC needs to be aware of the interfering factors in BGC such as steroids and parenteral as well as enteral nutrition.
Measurement of Blood Glucose Levels
Different methods of blood glucose measurement in critically ill patients are used in daily practice, ranging from point-of-care (POC) glucose measurements with capillary or arterial blood, arterial whole blood in blood gas analyzers, to plasma or serum from venous or arterial blood measured in the central lab.23-25 Blood glucose measurements in plasma in remote central laboratory facilities of the hospital may be impractical, inefficient, and unsafe to implement TGC due to the inevitable time delay between sampling and availability of the blood glucose result to the clinical staff. 26 Methodologies for blood glucose measurements at the patient’s bedside or in the ICU itself are therefore preferred from a logistical point-of-view. 27 Additionally, the tendency to decrease the number of arterial and central lines, in order to decrease the incidence of bloodstream infections, makes frequent blood sampling in the ICU more difficult. To tackle this issue of blood sampling, the pragmatic studies mainly used capillary glucose measurements in their BGM protocols.9-11
However, POC blood glucose meters were developed for the management of out-of-hospital patients with diabetes to help them control their own glycemia. Because of the advent of TGC protocols after the publication of the Leuven studies, the POC blood glucose meters became more often used in the setting of critically ill patients. 28 Nevertheless, critically ill patients differ tremendously from out-of-hospital patients with diabetes. 29 Critically ill patients are exposed to factors that may affect blood glucose measurements: anemia, peripheral edema, vasoconstrictive drugs, and interfering drugs such as icodextrin.30-35 This had been underestimated and may have had a major influence on the results of the pragmatic trials. Not surprisingly, many studies revealed that the accuracy of these POC devices was not sufficient for the tight ranges aimed for in the TGC protocol.36-38 A simple study by Duncan Young, presented at the 29th International Symposium on Intensive Care and Emergency Medicine (ISICEM) in 2009, showed a 95% confidence interval (CI) of 37.8 mg/dL, exceeding the 30 mg/dL TGC range of 80-110 mg/dL, when using POC blood glucose meters (Table 2). Blood gas analyzers had the most accurate results with a 95% CI of 14.4 mg/dL, followed by laboratory values with a 95% CI of 21.6 mg/dL. Mixing methods had the worst accuracy with a 95% CI of 50.4 mg/dL, greatly exceeding the TGC range of 30 mg/dL. This study underpins the relationship between aimed target range width and required accuracy. When the 95% CI of a blood glucose meter exceeds the target range width, one needs to question the bluntness of the diagnostic tool.
95% Confidence Intervals (CI) for Different Glucose Measurement Methods.
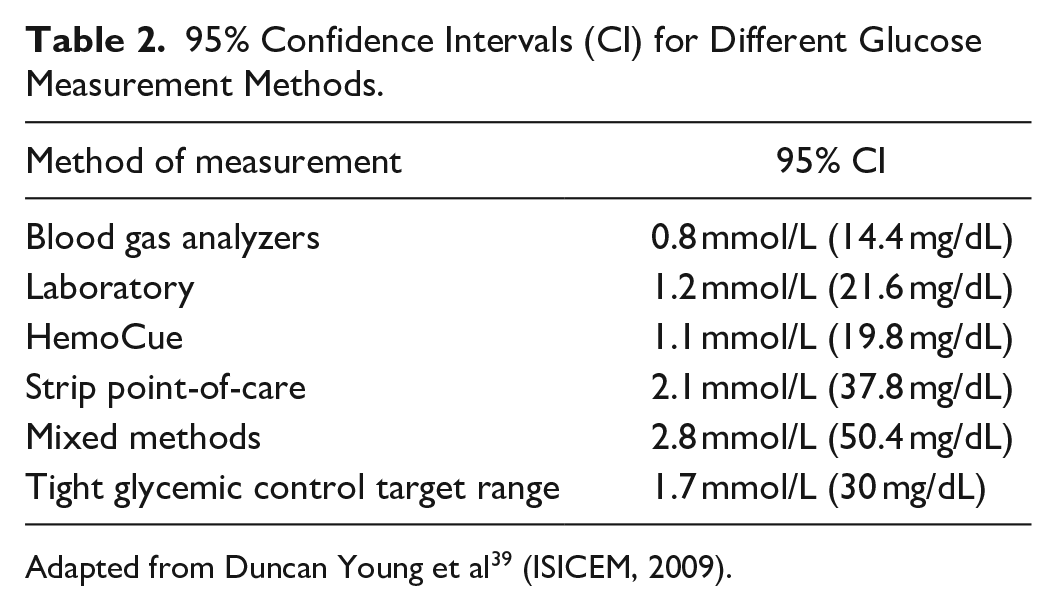
Adapted from Duncan Young et al 39 (ISICEM, 2009).
One has to take into account not only the target range width but also the absolute blood glucose value. Are we measuring in the hypoglycemic, normoglycemic, or hyperglycemic range? ISO15197:2003 standards for blood glucose meters prescribe a maximal deviation of 20% in 95% of measurements when blood glucose levels are above 75 mg/dL and a deviation of 15 mg/dL when below 75 mg/dL. Confirmation of compliance with these standards is executed by the manufacturers and does not necessarily apply in a hospital setting, let alone the critically ill patient population. Logically, most feared is the overestimation of blood glucose levels in the lower glycemic range, leading to unjustified increased dosing of insulin, and eventually to increasing numbers of true hypoglycemic episodes.
Vlasselaers et al investigated the accuracy of two older generation POC devices, HemoCue (HemoCue AB, Angelhölm, Sweden) and AccuCheck (Roche Diabetes Care Inc, United States) vs an arterial blood gas analyzer (ABL, Radiometer Medical, Brønshøj, Denmark) using arterial whole blood samples for all devices. 26 Initial analysis showed a very good correlation between the POC blood glucose meter and blood gas analyzer (r2 = 0.97 for AccuCheck and 0.94 for HemoCue). But dividing the measurements into different glycemic ranges resulted in a dramatic drop of the correlation coefficient in the TGC (r2 = 0.66 for AccuCheck and 0.56 for HemoCue) and hypoglycemic ranges (r2 = 0.73 for AccuCheck and 0.78 for HemoCue). However, the lower correlation coefficients are at least partially explained by the narrower ranges of values, leading to decreased statistical power.
Another study with older generation POC blood glucose meters showed that less than 60% of the results by capillary (fingerstick) measurement fell within a 20% error range from the central laboratory reference method. 40 In the hypoglycemic range, the agreement was even as low as 26%. The use of arterial blood in the glucose meter resulted in better agreement with central laboratory measurement, especially in the hypoglycemic range (70% and 55%, respectively). Arterial blood gas analysis yielded the best agreement with 75% and 65% for the total and hypoglycemic ranges. Interestingly, they found a consistent overestimation with capillary measurements for all glycemic ranges. This implies that the use of POC devices with capillary blood can potentially lead to an increased number of hypoglycemic events, certainly when aiming for strict normoglycemia. Some POC devices tend to systematically overestimate blood gas values, while others underestimate levels in the low glycemic range and overestimate levels in the high glycemic range, which is a slightly better safety profile in the context of TGC. 41
As a first step to address these problems, corrective measures were introduced to compensate for the anemia. An increase in hematocrit is known to give lower glucose readings and vice versa.30,31,42 This potentially masks hypoglycemia in anemic patients by measuring falsely elevated glucose levels. In 2009, Meynaar et al investigated the use of a correction factor (×1.086) after measuring glucose levels in arterial blood with POC blood glucose meter. 43 They compared against the standard central laboratory reference measurement, classically tested on serum. Using the ISO 15 197 limits, they found that in 9% of cases, glucose levels exceeded the acceptable range as compared with the central laboratory. By applying the correction factor, the difference improved to 6%. Capillary measurement, as classically used in POC devices, was not tested in this study.
chemistry techniques such as blood gas analyzers or central laboratory methods are considered less susceptible than biosensor technology in POC tests. 40 Interference with these tests can be caused by patient, pharmacological, and physiological factors. Glucose levels in the interstitial fluid can be affected by tissue perfusion, temperature, and local humoral factors. 44 POC device measurements are based on enzymatic reactions and therefore sensitive to pH fluctuations, as occurs frequently in ICU patients. 45 ICU patients are also often administered many different drugs, of which some may influence glucose level measurements. Tang et al investigated 30 different drugs and their effect on glucose readings from six different POC devices.30,46 Interferences were found for ascorbic acid, acetaminophen, dopamine, and mannitol.
This body of research sparked the efforts by POC blood glucose meter manufacturers to improve their devices. Recent real-world studies, comparing newer generation POC glucose meters with central laboratory tests, showed that their accuracy is comparable in ICU and non-ICU settings, falling within the limits of CLSI quality standards. These newer generation POC glucose meters may be fit for BGC in critically ill patients.47-49 A single-center trial in critically ill patients tested the accuracy of three “new” POC blood glucose meters in the setting of TGC. The FDA:2014 accuracy criteria were used with a maximum total allowable error of 10% and a maximal coefficient of variation (CV) of 3.9%. Arterial whole blood was used for blood glucose measurements in the POC devices and the blood gas analyzer was the reference methodology. All “new” meters met the FDA criterion of maximal 10% total allowable error: blood gas analyzer 0.0%, Freestyle Precision (Abbott Diabetes Care) 9.4%, Pro StatStrip Connectivity (Nova Biomedical) 3.7%, AccuCheck Inform II (Roche Diagnostics) 2.2%. The 95% CI was approximately 20 mg/dL for all POC blood glucose meters, compared with 7 mg/dL for the blood gas analyzer. Since the study by Vlasselaers et al in 2008, which was done in a similar patient population and the same context of TGC, the 95% CI of the POC blood glucose meters was basically halved. With a 95% CI of 20 mg/dL, the POC blood glucose meters may now be better suited for (tight) blood glucose management with a target range width of 30 mg/dL (80-110 mg/dL target range). Icodextrin did not interfere in any of the tested blood glucose meters and neither hematocrit nor oxygen tension could explain glucose level differences.
Blood Glucose Management Protocol
Apart from correct and accurate glucose measurement, a second important aspect for adequate BGM is the implementation of a clinically validated protocol. 50 In general, the choice of protocol appears to have a greater influence on glucose control measures than the glucose measurement method. Sensor inaccuracy can have an exponential impact on insulin dosing errors depending on the algorithm that is used. Protocols that implement more frequent measurements— or even near-continuous measurements—are bound to reduce the margin of error. 51 Several BGM “systems” exist, from nurse-driven insulin administration based on intermittent measurements to fully autonomous computer-controlled looped systems, fed by near-continuous measurements.52-56 In the original Leuven studies, an intuitive paper-based algorithm was used by the ICU nurses. This was later converted into a computer-based algorithm to calculate the most optimal insulin or glucose dose to achieve normoglycemia.52,57,58 In order to clinically validate the newer computerized protocols, research groups take more and more advantage of simulation models and computer learning.59,60 Simulation models have also been used to assess the required accuracy level of blood glucose meters. Van Herpe et al found that the mean absolute relative difference (MARD), a newer indicator of blood glucose meter accuracy, should be less than 7.1% for intermittent glucose measurement in order to avoid acute life-threatening situations and to minimize potentially life-threatening situations to <0.01%. 51
Because of the heterogeneity in study protocols over the years, it is difficult to ascertain the best-standardized protocol for the ICU. 61 Simulation models can certainly aid in guiding future RCTs, but further research is required to clinically validate new protocols.
The Current Consensus
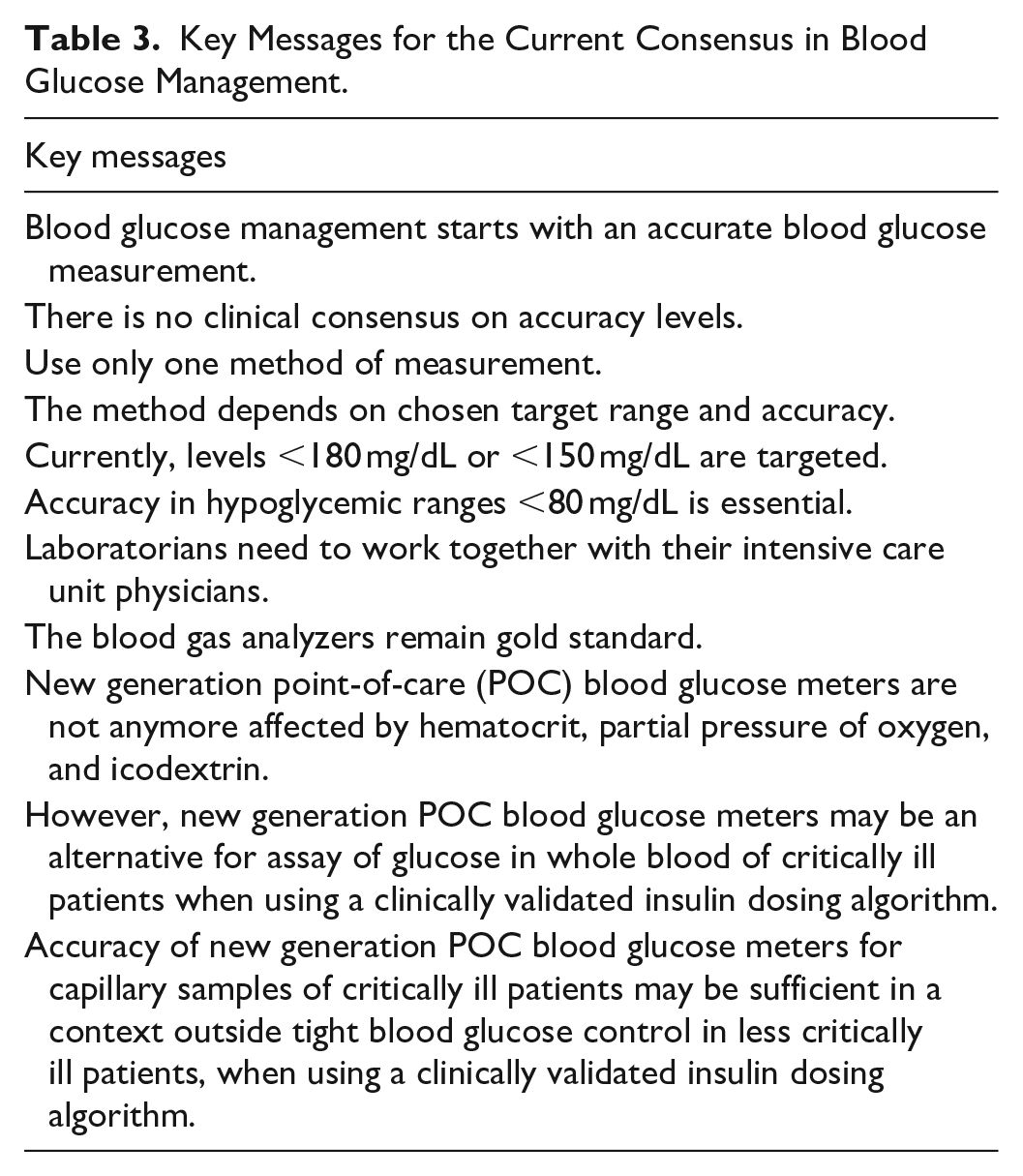
At this point, there is an international expert consensus among ICU staff to treat blood glucose values above 180 mg/dL in all ICU patients. The general aim is to keep blood glucose levels between 140 and 180 mg/dL, in order to have the necessary margin to avoid hypoglycemia. This can be achieved by frequent measurements, with a preference for arterial blood samples over capillary blood. Incorrect measurement is an important cause of hypoglycemia in critically ill patients. Using capillary blood in critically ill patients is less reliable because of peripheral edema. It often leads to an overestimation of blood glucose levels and should be avoided. The accuracy of blood glucose measurement devices should be checked periodically and preferentially, arterial blood gas analyzers are used. Arterial or venous blood samples are preferred. When hyperglycemia or hypoglycemia is detected, the use of a validated insulin dosing protocol leads to better BGC (Table 3).
Key Messages for the Current Consensus in Blood Glucose Management.
Conclusion
Ever since the publication of the landmark study by Van den Berghe et al, 1 the benefits of good glycemic control have been internationally recognized. Methods of glucose measurement as well as therapeutic protocols have been well investigated during this time. Studies have shown a discrepancy between risk/benefit in tightly standardized single-center trials and the more heterogeneously designed multicenter trials.
In order to optimize BGC, there is a continued need for accurate blood glucose measurement devices. On the other hand, the implementation of a protocol-based approach to hyperglycemia or hypoglycemia in any ICU patient remains an important standard of practice. The optimal target range is yet to be determined and depends greatly on the accuracy of newer glucose measurement devices and the adherence to protocol setup.
Future research is aimed at fully closed-loop systems, with continuous blood glucose measurement and computer-controlled intervention, also known as the “artificial pancreas”.62-68 A performant system could greatly reduce the significantly increased workload in the ICU. Of course, clinical validation of these systems would still be required to investigate the effect on clinical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.