
Abstract





[P01] Critical Factors for Limb Salvage in Patients with Critical Limb Ischemia
Department of Plastic and Reconstructive Surgery, Critical Limb Ischemia Center, Kitaharima Medical Center, Ono, Japan
To determine critical factors for limb salvage and wound healing in patients with critical limb ischemia (CLI).
We retrospectively investigated a consecutive series of 85 patients with foot ulcers treated by revascularization and wound treatment by our multidisciplinary team between October 2013 and February 2019.
The mean age of the patients was 72.2±12.1 years. Sixty-six patients had diabetes, and 49 patients had end-stage renal failure. Out of 105 foot ulcers, 83 healed (42 required minor amputation), whereas 14 did not heal (13 required major amputation), and 8 patients died. The healing time of the ulcers was 76.6±72.4 days. Furthermore, 63 ulcers were associated with osteomyelitis and had a healing time of 89±85.7 days, whereas the other 42 ulcers without osteomyelitis had a healing time of 61.2±48 days (p<0.05). Between the healing and major amputation groups, the albumin levels, ambulatory status, autoimmune diseases, steroid use, C-reactive protein levels (CRP), osteomyelitis, post-revascularization skin perfusion pressure value, duration of antibiotics, and number of bacterial types were statistically different (p<0.05). A multivariate logistic regression analysis showed that CRP, steroid use, duration of antibiotic, and vascular status after revascularization were significantly associated with wound healing (p<0.05).
Patients with severely infected ulcers on admission and steroid users were more likely to have major amputations. Successful revascularization is important in wound healing, but the vascular status on admission is not associated with it. Wound management by wound specialists is key to successful wound healing in patients with CLI.
[P02] Clinical efficacy of New generation vascular and tissue regenerative cell (MNC-QQ) therapy for Non-healing Ischemic Ulcer
Juntendo University School of Medicine, Department of Plastic and Reconstructive Surgery, Tokyo, Japan
Recently, we have reported the novelty of serum free ex vivo expansion system (QQc) of peripheral blood mononuclear cells (PbMNC) as non-invasive and effective vascular and tissue regenerative cell therapy named MNC-QQ therapy. Herein, we report the safety and efficacy of this therapy on non-healing ischemic extremity wounds.
200ml of peripheral blood was drawn from patients with chronic (>3 months) ischemic extremity ulcers in an outpatient basis. Mononuclear cells were isolated and cultured in QQ culture for one week without passaging or media changes. Under local anesthesia, 2x107 cells were injected within 20 cm2 of the chronic wound and wound healing was monitored by photometrically. The adverse effects were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events. Wound closure, VAS scale, skin perfusion pressure (SPP), TcPo2, laser doppler, thermography and angiography were performed to evaluate efficacy post 2,4,8 and 12 weeks therapy.
A total of nine patients, ten limbs were enrolled. The age ranged from 64 to 74 years old. Eight males and one female. Seven patients had diabetes with renal failure and two with collagen disease as past medical history. Blood sugar levels were controlled for all patients, and HbA1C was below 8.0%. All of the wounds extended into bone or tendon and were located in the digits of the foot. Case one with adverse effect underwent infection from injection site with alternative ulcer which had later healed. All patients were ambulant without major amputation. There was no death, other serious adverse events, or major amputation seen within 12 weeks following transplantation. Increased vascular perfusion with decrease in VAS scale were seen in all patients. Interestingly, SPP significantly increase post therapy.
This clinical study indicates the safety and feasibility of MNC-QQc cell therapy in patients with ischemic nonhealing wounds. This methodology of transplanting highly vasculogenic EPCs from small amount of blood draw will be the world’s first non-invasive and effective peripheral blood vascular stem cell therapy for diabetic limb salvage.
[P03] Improvement in outcomes since commencement of multidisciplinary inpatient and outpatient pathways of care: Institutional Review of a 1500 bed teaching hospital in Singapore
Tan Tock Seng Hospital, Singapore, Singapore
Singapore has a high burden of diabetic foot disease with four LEAs performed everyday. We reviewed our institutional experience over the last 10 years and assessed the impact of the implementation of a multidisciplinary team approach to management, on the outcomes of patients with diabetic foot ulcers (DFUs).
A retrospective study of diabetic limb salvage attempts at a tertiary 1,500-bed university hospital from 2008 to 2018. A new inpatient diabetic foot ulcer pathway was implemented in 2014, to standardize the care of these patients. Since 2017, we introduced a multidisciplinary outpatient clinic called the Lower Extremity Amputation Prevention Programme (LEAPP), to allow for rapid access for patients with DFU. We compared the inpatient outcomes before and after implementation of the DM foot pathway. We compared waiting times and LEA rates in patients referred with DFUs to vascular clinics before and after the start of the LEAPP service.
There were an average of 760 admissions with DFU per year. The patient profiles remained similar. A third of the patients had end stage renal disease and contralateral amputation.
Since the implementation of the multidisciplinary inpatient pathway, we saw a drop in major LEAs from 125 per year to 87 per year. Minor LEAs showed a smaller drop from 709 per year to 565 per year. There was a five fold increase in revascularization rates. Up to 80% of limb salvage attempts were by angioplasty and the remainder were surgical revascularization. Limb salvage rate improved from 83% to 88%, with an improvement in 30 day mortality from 3.3% to 1.5%. Since the commencement of the LEAPP clinic, we saw a reduction in waiting times from 38 days to 5 days. There was a reduction in major LEAs from 9% to 3% and minor LEAs from 14% to 3%
Within our institution, we saw an improvement in patient outcomes since the institution of a multidisciplinary inpatient pathway and the commencement of a multidisciplinary diabetic foot clinic. Our results are in keeping with published data on the efficacy of multidisciplinary teams in the prevention of LEAs in patients with DFUs.
[P04] Tissue Tension with Complementary Negative Pressure Therapy for Enhanced Wound Closure after Debridement in Diabetic Foot Patients
Laniado Hospital, Netanya, Israel
Patients with infected diabetic foot in many cases are treated aggressively with extended soft tissue debridement, leading to soft tissue defects on the plantar surface. We tried to decrease treatment duration with gradual closure of wound edges and negative pressure with continues wound lavage and oxygen insufflation, preventing infection exacerbation.
In our study 8 patients had open wounds on the plantar surface of the foot after extended debridement. All patients had sufficient blood supply.
The “Top Closure Device” was put on the wound edges and tension sutures were used to gradually close the wound over several days. The wound was further closed with a negative pressure device (“V-Care”) providing wound irrigation with antimicrobial solution and insufflation of oxygen for anaerobic microbes. The procedure was usually performed after previous treatment when the wound surface turned to be clean from necrosis and abundance of suppuration. Blood tests and microbiological examination were performed.
Complete wound closure with forming of scar mechanically sufficient for ambulation was achieved in all 8 patients.
Based on our modest experience we propose wound edges tensioning combined with negative pressure irrigation therapy for quick wound closure of the diabetic foot and other extended wounds offering a superior alternative to application of VAC therapy alone.
[P05] Retrospective Analysis of Partial Calcanectomy for the Treatment of Chronic Calcaneal Ulceration
Saint Marys Medical Center Pmsr/Rra Podiatry Residency, San Francisco, United States
This retrospective study evaluates the results and outcomes for 29 patients who underwent partial calcanectomy for infected ulceration of the heel. This research seeks the appropriate indicators for offering the patient the best functional result at the most distal level while avoiding excessive procedures.
Twenty-nine patients (31 feet) underwent unilateral or bilateral partial calcanectomy at three centers of a multidisciplinary academic medical system between January 2012 and December 2017. A database of demographics, vascular risk factors, outcomes, complications, and other comorbidities was constructed. Twenty-nine patients were included in the final analysis. All patients had chronic, infected ulcerations of the calcaneus and had failed conservative treatment. The primary outcome of this study is the rate of amputation-free survival of 1 year. This positive outcome signifies that the patient did not suffer mortality or a subsequent major lower extremity amputation within one year of surgery.
This study had an average follow up of 28.3 months. Twenty (69%) patients had amputation-free survival of one year post partial calcanectomy. Three (10.3%) patients died, five (17.2%) had a more proximal amputation and one (3.4%) had both negative outcomes within 1 year of surgery. (After 1 year: no additional deaths; one proximal amputation). One death was due to infection of the surgical site; three were unrelated to the surgery. Two patients underwent proximal amputation due to vascular insufficiency, and two because of unresolved infection related to the surgery. One patient, who initially healed, later had amputation due to recurrent ulceration. In one case, lateral leg wounds led to proximal amputation. Twenty-four of thirty-one feet healed their partial calcanectomy at Mean 242 days. Ambulatory status in the twenty-three patients who did not require major amputation within 1 year showed that twenty-one patients improved or did not change and two worsened.

Partial calcanectomy is a viable and preferable alternative to proximal limb amputations in many patients. Further investigation is warranted to determine which factors identify patients who will benefit from partial calcanectomy from patients who should receive a major lower extremity amputation as their primary procedure.
[P07] Incidence of peripheral vascular disease and need for revascularization in ischemic diabetic charcot foot
King’s College Hospital, London, United Kingdom
To assess the prevalence of peripheral vascular Disease (PVD), critical leg ischemia (CLI) and need for revascularization in the Diabetic Charcot population.
Retrospective analysis of all patients attending the Diabetic Charcot’s clinic in 2013. All patients with proven Charcot disease were analyzed. Primary end points were incidence of PVD, CLI and need for revascularization.
One hundred and ninety-eight consecutive patients attended the diabetic Charcot foot clinic. 69 (35%) patients had radiological confirmed Charcot joint on X-ray, CT-spc or MRI and were included in the analysis. 66 (96%) presented with tissue loss and 3(4%) with rest pain. All 69 went on to have arterial duplex scans and 44 (64%) patients were found to have PVD in the femoral-popliteal segment 9%, infra-popliteal in 46% and over both levels in 45%.
34 (77%) out of the 44 patients with PVD required revascularization. 19 (43%) endovascular to the femoral-popliteal segment, 32% to infra-popliteal in 26% and in both in 42%
Another 15 (34%) had bypass revascularization. Femoral- popliteal, distal bypasses and ultra-distal bypasses in 20%, 53% and 27% respectively.
22 out of the 69 (32%) patients had undergone orthopedic procedures
Prevalence of PVD and CLI in the Diabetic Charcot population is significantly high. These are the most challenging group of patients and multi-disciplinary team approach is crucial. Complex early revascularization might be required.
[P08] Introduction to Morbidity and Mortality Rates after Chopart Amputation
Saint Marys Medical Center, Saint Marys Medical Center Pmsr/Rra Podiatry Residency, San Francisco, United States
This retrospective study evaluates the perioperative course of 31 patients who underwent chopart amputation for chronic non-healing ulcerations of the foot. The purpose of this research is to contribute demographics, clinical and surgical risk factors, and surgical outcomes and complications of the chopart amputation.
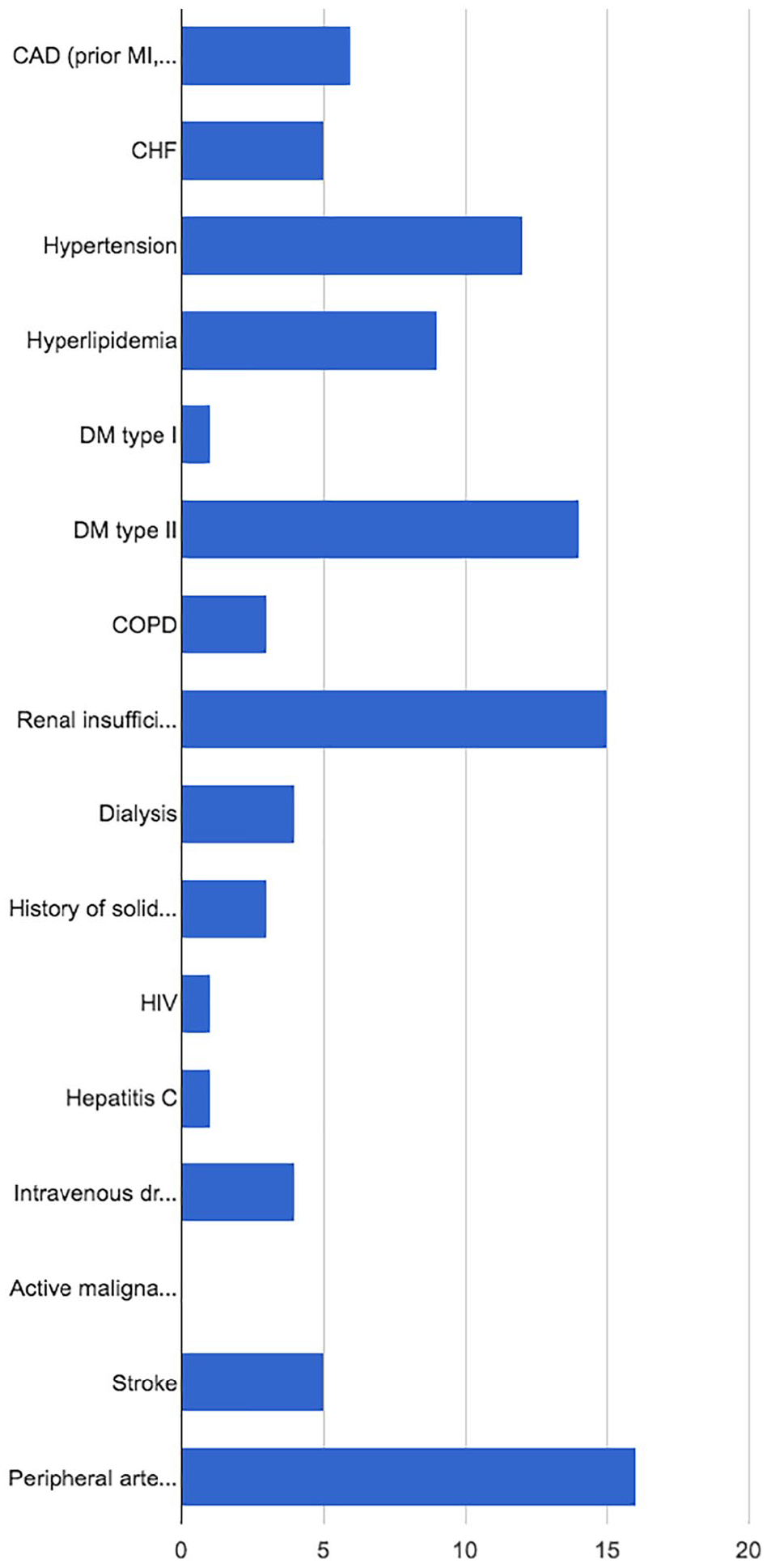
Thirty-one patients who underwent chopart amputations at any one of three centers of multidisciplinary academic medical systems (UCSF, SFGH, and SFVA) between 2012 and 2018 with minimum 12-month follow up were reviewed. We are currently constructing a database of patients’ sex, age, race, comorbid conditions including vascular status, renal status, coronary artery disease, hypertension, smoking status and ambulatory status. All patients were treated for chronic non-healing ulcerations of the foot after failing local wound care. Primary outcome variables are amputation free survival (defined as 365 days after surgery without amputation or death), proximal amputation and 3 and 5-year mortality.
The Figure displays the demographics of the patients who underwent chopart amputations. Overall, amputation free survival for the study population was 58.1% (18/31). Average time to healing is 73.86 days. Mortality occurred in 4/31 (12.9%) of the chopart amputees. None occurred after an amputation free survival (1,150 days, 734 days, 1,146 days and 1570 days) nor were they related to their chopart amputation. Ultimately, 11/31 (35.4%) went on to BKA and none to AKA. Mean follow up for this study population was 541.31 days.
In conclusion, our results contribute to current podiatric literature on chopart amputations. In our academic centers’ experience, this procedure is a viable alternative in limb salvage for a high risk low demand patient. Our future research will analyze variations in the outcomes according to demographics, clinical and surgical risk factors.
[P09] Outcomes After Midfoot Ostectomy for Treatment of Chronic Ulcers in a Charcot Foot
California School of Podiatric Medicine, Samuel Merritt University, Oakland, United States
Charcot neuroarthropathy often causes medial arch collapse and plantar osseous deformities leading to ulcerations. A plantar midfoot exostectomy creates a plantrigrade foot and aids in ulcer healing. The objective of our case series is to determine the efficacy of plantar midfoot exostectomies in the treatment of plantar midfoot ulcerations.
A retrospective review of 21 plantar midfoot exostectomies on 20 patients was conducted at 2 academic medical centers between 2014-2018. Inclusion criteria included Charcot Eichenholtz stage III at the midfoot, with an active plantar ulceration due to a bony exostosis. Exclusion criteria included patients with follow-up of <7 months. All exostectomies were performed with an incision at the wound with primary closure of the incision, and wound healing with secondary intention. Post-operatively, patients were given strict NWB instructions in a CROW boot, post-op shoe, or TCC. Outcomes measured included adjunctive procedures, time to heal, ulcer recurrence, and revision rate.
Twelve out of 20 patients were male (60.0%), the mean age was 55.75, and mean BMI was 33.3. All patients had diabetes mellitus and 4/20 (20.0%) had peripheral vascular disease. Plantar cuboid exostectomy was performed in 17/21 (80.9%) feet, while the rest were performed at the plantar medial cuneiform. Adjunctive tendo-Achilles lengthening or gastrocnemius recession was performed in 6/21 (28.5%) feet. Compliance with non-weight bearing protocol and offloading modality varied among patients. Surgical wounds dehisced in 6/21 (28.5%) feet. Plantar ulcerations healed on an average of 8.8 months in 17/21 (80.9%) feet. Among these, ulcers recurred in 10/17 (58.8%) feet at an average of 7.54 months after healing, with new wounds in 2/21 (9.5%) feet. Revision exostectomies were performed in 4/21 (19.0%) feet. At final follow-up of an average of 2.2 years, 10/21 (47.6%) wounds were closed, while the rest remain open.
While Charcot planing is a less invasive operative treatment for plantar midfoot ulcerations, we conclude that there is a high re-ulceration rate, which may be due to inconsistent post-healing offloading protocol and compliance.
[P10] Positive Intra-Operative Culture Does Not Impede STSG Integration in the Diabetic Host
Medstar Georgetown University Hospital, Washington DC, United States
Split thickness skin grafting (STSG) is an effective closure modality in treating diabetic foot ulcers. Bacterial colonization has traditionally been seen as a relative contraindication to the application of STSG. The study was designed to evaluate this theory and identify discrete predictors of graft success.
Following approval by the Georgetown University IRB, a search of the available electronic medical record from 2014-2016 was carried out utilizing the associated CPT code for application of STSG and cross referenced with ICD9 codes correlating with diabetic foot ulcer. All patients 18 years or older with diabetes mellitus and a lower extremity wound were included. Patients with an ulceration resulting from radiation, trauma, or autoimmune disease were not including.
A total of 108 patients were identified. 103 (95.4%) had hypertension, 75 (69.4%) had hyperlipidemia, 29 (26.9%) had congestive heart failure, and 22 (20.4%) had venous stasis. Complete epithelialization was obtained for 29 (22%) patients at day 30, 48 (36%) patients at day 60, 63 (48%) patients at day 90, and 77 (58%) patients at 365 days of follow up. On average, 4 serial debridement’s were carried out prior to STSG placement. The average heeling time was 13 weeks. At 71 weeks, 60% of wounds had shown complete heeling. The results identified no significant difference in graft uptake between positive pre and post debridement cultures, positive or negative culture growth in the pre debridement setting, and positive or negative growth in the post debridement setting.
It has previously been reported that bacterial colonization with common organisms can decrease STSG integration. This is especially true of a compromised host. The study results highlighted no significant difference in STSG integration with or without positive intraoperative cultures. Further, these findings were consistent over time.
[P11] Application of Novel Grading Scale to Quantify Small Vessel Disease in Cutaneous Tissue Surrounding Wounds
The Heart Hospital Baylor Plano, Plano, United States
Non-healing wounds of the lower extremities primarily result from severe underlying arterial vasculopathology. Clinical diagnosis and intervention currently focus on macro-arteriopathy, but small vessel disease (SVD) also contributes to this condition. This study uses a novel grading scale to objectively measure microvascular arteriopathy in skin surrounding non-healing wounds.
During an IRB-approved clinical study, skin biopsies were obtained from patients undergoing amputation procedures for non-healing wounds containing dry gangrene, wet gangrene, and no gangrene. Biopsies were stained with haemotoxylin and eosin and scored with a novel SVD grading scale. This scale ranged from 0-21 and was developed by a team of experienced vascular surgeons and pathologists and included factors indicative of microangiopathic changes of the skin. Factors included fibrin deposition, stasis changes, inflammation, thrombosis, and necrosis. An inverse proportional least squares model was used to determine a relationship between SVD severity and distance from wound edges.
A total of 92 biopsies were obtained from 16 patients undergoing 19 amputations (mean 4.8±2.1 biopsies per amputation). Amputations included 9 toes, 4 trans-metatarsal, and 5 below-the-knee amputations and were all performed due to non-healing wounds. Biopsy distance from wound edges ranged from 0.1 cm to greater than 10 cm and SVD scores ranged from 0 to 15. An inverse proportional relationship between SVD score and biopsy distance was observed, where the coefficient of biopsy distance was significant (Furthermore, general SVD score tended to be greater than zero regardless of biopsy distance suggesting a baseline level of SVD in patients with systemic disease (p=0.09). Figure 1 shows SVD scores to be generally low (0 to 3) until approximately 1.0 cm from wound edges where a sharp rise in SVD score occurs (up to 15).
SVD contributes substantially to delayed healing and other wound complications. This study demonstrates a unique relationship of increasing SVD with decreasing distance from wound edges. Using this information, a margin of clinically significant SVD surrounding chronic wounds can be determined and used to guide treatment planning.
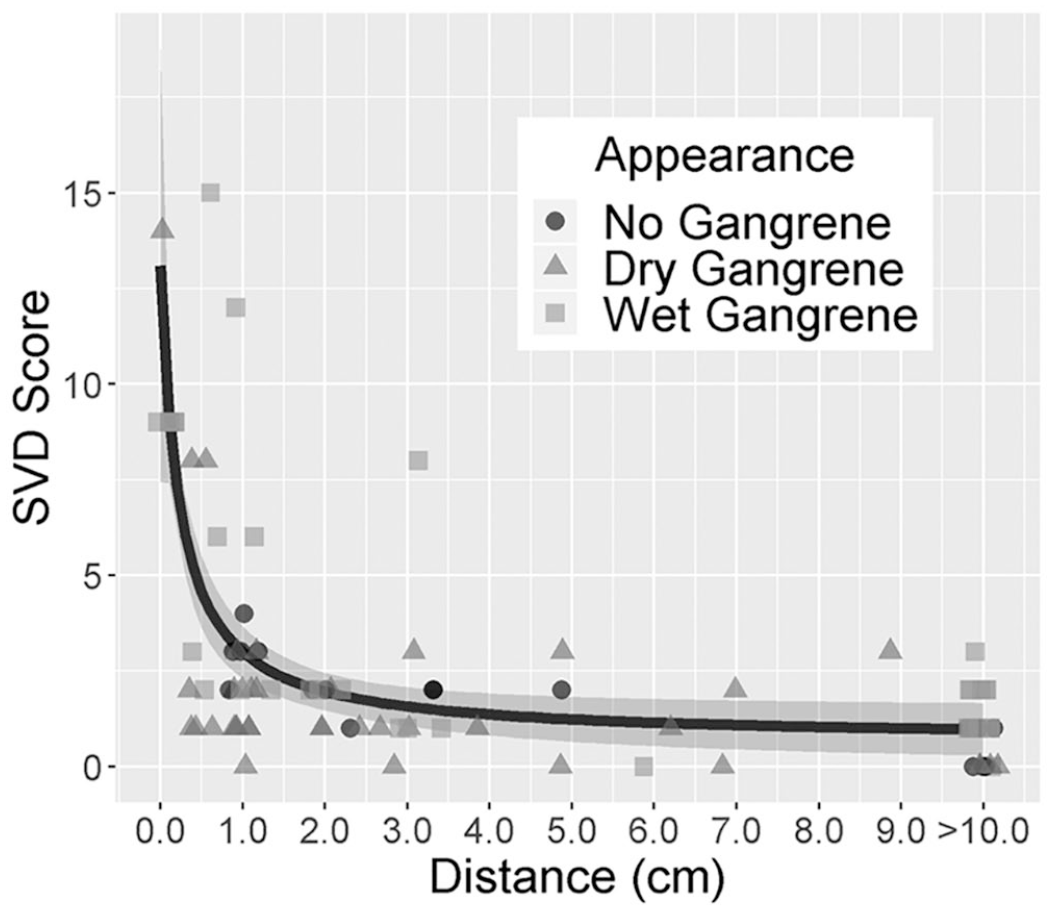
Relationship Between SVD Score and Distance (cm) from Wound Edge
[P12] WIFi Classification System as a Predictor of Healing: A Case Series
California School of Podiatric Medicine, Samuel Merritt University, Oakland, United States
The Society for Vascular Surgery’s Wound, Ischemia and Foot Infection (WIFi) scoring system is a relatively new classification for which evidence of long-term prognostic value is needed.1-12 The present study hopes to add mid-term outcomes of patients staged with WIFi before and after surgical intervention to the growing literature.
Single-center, retrospective case series of 12 consecutive patients with concurrent lower extremity ulceration and chronic-limb threatening ischemia (CLTI). All patients were hospitalized for either lower extremity infection and/or critical limb ischemia. Demographic, clinical, and WIFi stratification was obtained for each patient at the time of admission and first and final follow-up (Table 1). Binary scoring was utilized to simplify correlation of WIFi and success of therapy. Strength of prognostic value of the classification was defined as positive correlation between improvement in WIFi and increased limb salvage - maintenance of a limb distal to transtibial amputation.
Failure was defined as a loss of limb (any amputation at the level of or proximal to a transtibial amputation), independence with activities of daily living (ADL), or mortality. 12 patients were classified by WIFi at the time of hospitalization for CLTI, wound infection. Final follow-up duration was a mean of 13.23 months. Comorbidities of note include diabetes mellitus (DM) and end-stage renal disease (ESRD). WIFi risk of amputation is intended to be prognostic at 1 year.1-12 WIFi had similar prognostic value in patients with a glycated hemoglobin >8%, on dialysis, or both. An improvement in WIFi clinical stage (i.e. stage 3 to 2) was demonstrated in 8/12 patients, in which limb salvage at 1 year was 8 of these patients. Only 1 of 3 patients with a WIFi clinical stage of 3 or 4 survived amputation by 1 year.
Improvement in WIFi classification system post-surgical intervention lead to moderate improvements in patient outcome in this limited cohort. A lower amputation risk according to WIFi stratification was predictive of morbidity and mortality. Limitations of the present study include: sample size, retrospective nature, intergroup differences, and loss of follow-up.
[P13] Crural-crural/pedal bypasses an option to consider in selected patients with critical leg ischemia
King’s College Hospital, London, United Kingdom
The efficacy of distal and pedal bypasses origination from femoral and popliteal artery has been well documented throughout the literature. The aim is of this study is to assess using crural arteries as inflow for crural and pedal bypasses.
Retrospectively analysis all patients underwent Crural-Crural/Pedal bypasses (2015- 2019). Primary end points were 30 day mortality, limb salvage and patency rates.
Total of 14 cases presented with CLI. 12 males & 2 females Mean age 68 years (48 -87). 2 presented with acute on chronic leg ischemia, 5 presented with tissue loss and 7 with gangrene. 2 needed immediate post bypass Hybrid II angioplasty ending with rupture to the plantar anastomosis and were excluded from further analysis. The incidence of Diabetes mellitus, chronic kidney disease and Ischemic heart disease were 93%, 36% and 50% respectively. 11 (92%) cases had Hybrid I angioplasty t.
5 (45%)cases were done under Local anesthetic. 6 (50%) grafts completed full year and 4 33(%) between 6-11 months. 2 (17%) grafts occluded at 44 and 125 days, by which patients were intact and needed no further revascularization. 5 (45%) Cases had salvage angioplasty, 1 for inflow and runoff, 2 for the runoff only and 2 graft stenosis.
30-days mortality was 0%. Limb Salvage rate was 100%. Primary and secondary patency rates at 1 year were 47% and 100%.
Crural-Crural/pedal bypass is a feasible and reliable option in selected patients. Medium term results showed good outcome with good patency and high limb salvage rates. In high risk patients this procedure can be performed under LA. Graft surveillance is essential in detecting threatened grafts.
[P14] Combined hybrid remote endarterectomy and distal bypass in critical leg ischemia
King’s College Hospital, London, United Kingdom
Combined Hybrid Endovascular and surgical revascularization has proved its efficacy in managing complex PVD in critical leg ischemia (CLI). However, extensive infra-inguinal occlusive disease still remains a challenging task for such modality. We report new Hybrid Remote technique for such challenging cases.
A retrospective analysis of all patients who underwent lower limb Hybrid Remote Endarterectomy and distal bypass for CLI between 2012 and 2014. All grafts were recruited in duplex surveillance scan program for 1 year. The main outcome measures were major amputation rate, 30 days mortality rate, primary and secondary patency rates at 12 months. Kaplan-Meier analysis to assess and compare patency rates.
Total of 8 patients underwent Combined Hybrid Remote Endarterectomy and distal bypass for CLI over 2 year period. All cases presented with tissue loss and or gangrene. The median age was 73 years. The incidence of diabetes mellitus was 69%. All patients underwent full remote endarterectomy to the superficial femoral (SFA) and/or popliteal arteries combined with a distal bypass: popliteal-posterior tibial bypass in 3 cases, popliteal to anterior tibial in 2 case, popliteal to popliteal to peroneal in 2 cases, popliteal to tibioperoneal trunk in 1 case. Vein conduit was used in all cases.
No mortality was recorded at 30-days. Primary, secondary patency and Limb Salvage rates at 1 year were 47%, 100% and 100% respectively.
7 grafts required salvage angioplasty to restenosis at the SFA (6 cases and popliteal ( 1 case) endarterectomy sites and 3 to the bypass vein graft segment at year 1. Another 2 grafts required salvage angioplasty at year 2 and year 3 follow up.
Our cases have shown that Hybrid Remote Endarterectomy combined with distal bypass is a feasible option in selected cases with extensive infra-inguinal occlusive disease. Strict graft surveillance is mandatory is essential and early salvage angioplasty mostly needed to the superficial femoral endartrectomy segment.

[P15] The Power of a Standardized Approach to Wound Care: Venous Leg Ulcers
Sanford Health, Fargo, United States
It is estimated that approximately 2.5 million people suffer from chronic venous insufficiency (CVI) in the US, and of those, 20% develop venous ulcers. Cumulative annual costs of treating venous leg ulcer (VLU)s in the United States is estimated to be over $25001
In order to combat the impact of VLUs on patients’ lives and the economy, a standardized checklist approach to wound care has been proposed. This includes early assessment and diagnosis, adequate wound bed preparation, edema control, and the use of advanced cellular tissue products.2
Here, the authors have applied the standardized approach methodology to improve healing rates in patients with VLUs. The patients in this case series underwent early diagnosis based on venous insufficiency, ultrasounds, adequate wound bed preparation with the use of serial sharp debridement procedures, edema control with compression therapy, and the application of advanced cellular tissue products.
At follow-up, the patients demonstrated complete wound healing.
The authors believe that this checklist approach to VLUs can streamline clinical processes, standardize care and improve patient outcomes.
Davies AH. The Seriousness of Chronic Venous Disease: A Review of Real-World Evidence. Adv Ther. 2019 Mar;36(Suppl 1):5-12.
Snyder RJ, Jensen J, Applewhite AJ, Couch K, Joseph WS, Lantis Ii JC, Serena TE. A Standardized Approach to Evaluating Lower Extremity Chronic Wounds Using a Checklist. Wounds. 2019 May;31(5 Suppl):S29-S44.Thomas F. O’Donnell Jr. et al, Management of venous leg ulcers: Clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum, Journal of Vascular Surgery, Vol 60, No 2S.
[P15A] Impact Of Frailty On Major Adverse Events In Patients with Chronic Limb Threatening Ischemia: A Prospective Analysis
Keck Medicine of University of Southern California, Los Angeles
Frailty is a known predictor of morbidity in people undergoing surgery. Available tools for measuring frailty depend on gate-based assessment which is a major limitation for evaluation of patients with chronic limb threatening ischemia (CLTI). The aim of the current study is to estimate the role of a novel upper extremity frailty (UEF) index as a predicting tool for Major Adverse Events (MAE) in CLTI patients.
UEF index was prospectively measured for all consecutive patients with CLTI referred to vascular surgery service of two University Teaching Hospitals from September 2018 to June, 2019. Major Adverse Events (MAE), including Major Cardiovascular Adverse Events (MACE) and Major Adverse Limb Events (MALE) were documented in the postoperative period of thirty days. Impact of frailty status on outcome variables was assessed using univariate and multivariate methods.
Of 104 CLTI recruited patients, 77 patients (51 male, 26 female, mean age 69.1 ± 11.8 years) underwent revascularization (31 open, 46 endovascular). Twenty-six of them ( 33.8% ) were frail (UEF Index > 0.28 ), with an average UEF index of 0.22 ± 0.13. MACE, MALE and MAE respectively occurred in 3 (3.9%), 12 (15.6%) and 15 (19.5%) patients. Frail patients had a significantly higher rates of MAE (35.8% vs 9.8%, p=0.003), MALE (34.6% vs 5.9%, p=0.002) in revascularized group (Fig 1), as well as significantly higher rate MAE in all CLTI patients ( 30.8% vs 4.6%, p=0.001) (Fig 2).
Frailty defined by UEF Index is an independent predictor for MAE for CLTI patients undergoing revascularization, as well as all CLTI patients.


[P16] Effect on topical microbial load and community composition with two versus six-week topical Cadexomer iodine for treating chronic biofilm infections in Diabetic Foot Ulcers
South Western Sydney Limb Preservation and Wound Research, South West Sydney Local Health District, Sydney, Australia
Biofilms are known to possess multiple tolerance mechanisms to antimicrobial treatments. Despite this their use is widespread amongst clinicians managing chronic wound infections, however there is scant evidence available on their effectiveness in vivo.
As Cadexomer Iodine has previously demonstrated the ability to reduce the microbial load in diabetic foot ulcers (DFU) over 7 days of use, its effect on wound metrics and optimal duration was investigated. This pilot prospective cohort study enrolled patients with non-healing DFUs with suspected chronic biofilm infections over an 18-month period. Patients were randomized to receive either two or six weeks of treatment with second daily topical Cadexomer Iodine dressing application. Tissue punch biopsies were obtained pre-and-post treatment. DNA sequencing and real-time qPCR was used to determine the total microbial load, community composition and diversity of bacteria in tissue specimen’s pre-and-post treatment.
Scanning electron microscopy confirmed biofilm in all 18 enrolled patients with DFUs who had suspected chronic biofilm infections. Cadexomer Iodine resulted in 14 of 18 (78%) samples achieving a mean 0.5 log10 reduction in microbial load. Regardless of treatment duration there was no statistical difference in the reduction of total microbial loads in DFUs treated for two weeks. All DFUs showed an initial reduction in wound size with application of Cadexomer Iodine. There was no difference in the rate of wound healing for the two groups at 6 weeks. Cadexomer Iodine demonstrated an effect on microbial community composition and diversity with patient specific shifts in microbial community. This compositional change, usually a reduction, occurred to the relative abundance of key potentially pathogenic genera.
Longer treatment durations don’t appear to continue to reduce total microbial loads in DFUs after the initial effect. The initial wound reduction may be reflective of the effect of Cadexomer Iodine on biofilm. A disruption to the chronic infective process may the host to restore the normal reparative process of wound healing.
[P17] Veterans Affairs Hospitals Case Series: Chronic Diabetes-related Wounds Treated with Autologous Homologous Skin Construct
Veterans Affairs New Jersey Health Care System, New Jersey, United States
Nearly 25% of Veterans Affairs (VA) patients have diabetes and over 2/3 of amputations in VA patients are due to complications from diabetic foot ulcers. An autologous homologous skin construct (AHSC) was used to treat five chronic lower extremity wounds that had failed standard treatments in the VA hospital setting.
The study is a retrospective cohort analysis of VA patients with diabetes and complex lower extremity wounds that had failed standard treatments and were ultimately treated with AHSC. For each patient, a full-thickness skin harvest was taken from a healthy donor site and sutured closed. The harvest was then sent to a manufacturing facility to be processed into AHSC, and was returned for deployment within 48-hours. After debridement, AHSC was applied over the wound bed and covered with silicone. The dressing was secured, bolstered and changed weekly for three weeks. Standard wound care dressings were used until closure.
Three subjects with 5 separate chronic lower extremity wounds ranged in age from 67-73 years. Wound size ranged between 14-135cm2. Wound etiologies included open hallux amputation sites (Wounds 1 and 2), open wounds following hardware infection of the ankle (Wounds 3 and 4), and surgical dehiscence and pressure ulceration of a below knee amputation (Wound 5). Wound 1 closed by day 120 and remained closed at day 139. Wound 2 demonstrated granulation with progressive epithelialization by day 15, however the patient required a transmetatarsal amputation due to osteomyelitis of the adjacent second metatarsal unrelated to AHSC treatment. Wounds 3 and 4 demonstrated healing with neodermal island formation, fibrinous exudate, and progressing epithelialization. Wound 5 stump dehiscence wound showed progressive epithelialization and formation of dermal islands, and bridging epidermis across the wound bed by day 27.
A single application of AHSC accelerated healing in hard-to-treat lower extremity wounds in diabetic patients. This novel therapy may serve an important role in treating lower extremity wounds in the Veterans Affairs hospital setting, and potentially prevent additional wound care and amputations.

[P18] Infrared Eyes (iREyes)-Thermal Indexing to Quantify Wound Healing
Eden Medical, Inc., Howard Lake, United States
Diabetic foot wounds are common, complex and costly. Foot areas that are likely to ulcerate are associated with increased local skin temperature due to inflammation. Inflammation is characterized by the cardinal signs including redness, swelling, and heat.
To develop a low-cost mobile health (mHealth) infrared imaging system that acquires both thermal and visible spectrum imagery to quantify diabetic foot ulcer healing via thermal indexing and reduces patient risk due to skin breakdown.
A Phase 1 Small Business Innovative Research (SBIR) study involved 17 test diabetic ulcer subjects including 11 males and 6 females. Eleven of the seventeen subjects (64.71% of test population) had multiple clinical visits with wound index correlation showing an indication of wound healing process or delayed wound healing. Two of the subjects healed completely during the course. Two types of wound healing patterns were observed during the study: a negative-to-positive index and a positive-to-negative index with both patterns trending to a final value of zero as healing occurred. The negative-to-positive index pattern typically involved isotherms in the woundbed that would start to be warm at the beginning of the healing process, and continue to be warm. The positive-to-negative index would have isotherms that were cold and switch to being warm later in the healing process. The positive-to-negative index may be an indicator of an ischemic condition.
The outcomes indicate quantifying healing using thermal indexing is useful. A Phase 2 study is funded to quantify healing via regional foot index analysis and ulcer reoccurrence risk through temperature asymmetry threshold analysis. The combination of indexing and asymmetry analysis may represent a breakthrough over current practice.
[P19] Autologous Homologous Skin Construct for the Healing of a Chronic Stump Wound and Repair of Sinus Tract in Diabetic Patient
Plastic Surgical Associates of Fort Collins, 1701 East Prospect Road, Fort Collins, United States
Amputated extremities can develop severe chronic wounds, especially if the patients have diabetes. Amputated stumps frequently incur complications and may require extensive additional care and potentially revision amputations. Autologous homologous skin construct (AHSC) was deployed to heal a chronic stump wound refractory to multiple conventional therapies including split-thickness skin grafting.
The patient’s wound developed due to prosthetic use. A full-thickness skin harvest was taken from the abdomen, closed primarily and donor skin was sent to a manufacturing facility, processed into AHSC and returned to the clinician after 48-hours. The wound was deroofed revealing a sinus tract, which was injected with methylene blue and excised. The wound was debrided and AHSC was spread evenly in the wound-bed, covered with a silicone dressing, stapled in place and bolstered with a layer of Xeroform (Cardinal Health, Ohio, United States) for additional pressure/contact. Dressing was changed weekly for 30 days, continuing Xeroform or emollient with compression to day 80.
The donor harvest was acquired and closed without complication. Upon gross examination 7 days post AHSC therapy, dermal islands appeared to be present in the wound and excised sinus tract. By day 17, the wound was experiencing progressive granulation and epithelialization as dermal islands continued to proliferate and adhere to the wound bed. Also, the sinus tract was no longer visible. 30 days post-AHSC therapy, dermal islands had coalesced and hair follicles appeared at the edges of the healed wound. At day 41 post-AHSC, the wound continued to normalize with the edges appearing smooth. The patient’s wound closed 80 days post-AHSC application, allowing the patient to slowly increase ambulation and weight bearing activity in their prosthetic. At a durability follow-up visit, 104 days post AHSC therapy, the sinus tract had not recurred and the wound site was completely healed with neo-generated skin normalized to surrounding healthy tissue.
A single application of AHSC was able to close and heal the recurrent stump wound, including the excised sinus tract and surrounding debrided tissue within 80 days. This novel therapy may be an effective patient management strategy to treat chronic stump wounds in diabetic amputee patient populations.

[P20] Autologous Platelet Gel: a help in chronic deep diabetic foot ulcers treatment
Fondation Hôtel-Dieu, Site Harfleur, Le Creusot, France
Randomized Controlled Trial to evaluate the safety and efficacy of autologous platelet rich plasma (PRP) gel for stimulating wound healing in chronic deep diabetic foot ulcers (3 A stage according to UT classification). N=86 diabetic patients were randomized.
Good standard of care was used when appropriate: debridement, infection and comorbidities management, off-loading.
Gel is obtained from patients blood by getting a Platelet-Rich, Leucocyte-Poor Plasma using Regenkit (RegenLab, Mont-sur-Lausanne, Switzerland).
Outpatient protocol: 2 weeks run-in period; if no reduction of wound surface>20% randomization (treatment gel application or control standard treatment) with following visits as needed; if necessary new application for PRP group. End of Treatment Visit(EoTV) at 6 weeks+/−3days, Evaluation Visits EV1 at 9 and EV2 at 12 weeks.
For PRP group no dressing change only protective compress change at home once weekly, for control group dressing change once daily.
With PRP gel / with standard treatment
Patients Characteristics: n=46/40, age (years): 68,1±10,9/69,6±11.4; all with neuropathy ; macroangiopathy n=27/23 ; amputation history n=10/3 ; antiaggregant treatment n=27/27 and anticoagulant treatments n=9/3.
Wounds Characteristics: depth(mm) 15,2±9,6/16,09±11,2; surface(mm2) 0,64±0,39/1,85±4,15; location : toe n= 23/18, metatarsal 17/18, plantar vault 1/1, heel 3/1, other 2/2;duration (months) 6,67±6/6,77±5,7.
Off-loading: unremovable below knee cast n=2/0, removable below knee bi-valve polyester cast n=7/11, wheelchair with insole in appropriate shoes (n=2/3) or with cast (n=1/0), walking boot (n=9/6), plastazote pressure redistributing insole in appropriate shoes n=25/16, no (n=0/2).
Complete healing at EoTV: 26(76,5%)/8(23,5%)(p=0,001); at EV2: 34(72,3%)/13(27,6%). Average healing time (days): 41,28±12,61/47,75±14,42(p=0,029).
Gel treatment 1 single application n=27, 2 applications n=17, 3 applications n=2.
Acceptability: very satisfying at EoTV: 67%/33%; at EV2: 65%/44%
Side effects: 14/21 at V1: 8/5; V2: 3/5; V3: 1/0; EoTV: 0/3; EV1:2/5; EV2: 0/3; mostly related to off-loading and intercurrent factors.
This study confirms the interest of Regenlab Autologous Platelet Gel in the outcome treatment of diabetic chronic severe foot ulcer.
Its application increases the number of healed wounds, shortens the healing time. It is well tolerated and simple to make.
[P21] A randomized, multiple-dose study of subcutaneous UTTR1147A (IL-22Fc) in patients with neuropathic, non-healing diabetic foot ulcers (DFUs)
Genentech, 1 Dna Way, South San Francisco, United States
UTTR1147A is a novel human interleukin (IL)-22-IgG4 Fc fusion protein that promotes epithelial proliferation and wound healing. This phase 1b trial evaluated safety, tolerability, pharmacokinetics, and preliminary healing activity of subcutaneous (SC) UTTR1147A in patients with neuropathic, non-healing, uninfected DFUs.
Eligible patients received standard-of-care (SOC) treatment (International Working Group on the Diabetic Foot [IWGDF] 2015), including non-removable offloading during a 2-week run-in to ensure that DFUs were non-healing. Patients with non-healing ulcers received peri ulcer SC injections of placebo or 1000-µg, 2500-µg, or 5000-µg UTTR1147A every 3 weeks plus SOC treatment for 12 weeks. Sample size was determined by practical considerations rather than statistical power considerations. Primary measures of activity were percent change in ulcer surface area for index ulcer from baseline to Weeks 6 and 12. Safety analyses included all randomized patients who received at least one dose of study drug.
61 patients were enrolled, with mean baseline ulcer areas of 2.75 cm2 and 2.04 cm2 in UTTR1147A (n=41) and placebo (n=20) cohorts (range, 0.7 cm2–7.5 cm2), respectively. UTTR1147A appeared to be safe and well tolerated. Serious adverse events in 14 patients were comparable between placebo and treated subjects and deemed related to underlying disease. Most other adverse events were mild. Drug exposure was detected in serum and in wound fluid. No significant differences were observed among UTTR1147A cohorts and the placebo group for the proportion of patients with complete wound closure (6 weeks, 23.6% vs. 15%; 12 weeks, 43.2% vs. 36.8%) and median percentage reduction from baseline in ulcer area (6 weeks, -71.4% vs. -58.8%; 12 weeks, -95.9% vs. -96.7%).
UTTR1147A had a favorable safety profile in patients with neuropathic, non-healing, DFU. No clear treatment effects in wound healing over current SOC were observed. Following the IWGDF-prescribed SOC, including non-removable offloading, for non-healing neuropathic DFUs significantly reduced ulcer areas in all cohorts.
[P22] Piscine Acellular Graft Application in the Real World
3335 South Crater Rd, Suite 500, Petersburg, United States
Diabetes is a pandemic that is getting worse each year. By 2025, it’s projected that 333 million people will be afflicted. (1) Many of these patients will develop lower extremity wounds that will stall in the healing process. Advanced healing modalities will be needed to achieve final wound closure.
A piscine acellular graft product, which supports the body’s own ability to regenerate by recruiting the body’s own cells, was utilized in the below case series. The graft is derived from Icelandic codfish skin. The protein composition closely resembles that of human skin and porous microstructure provides a scaffold for efficient ingrowth of dermal tissue and capillaries. In addition, the graft is uniquely rich in the polyunsaturated Omega3 fatty acids, which are known for anti-inflammatory properties that assist in regeneration. (2,3) The below case series, level of evidence IV, documents the healing prowess of the graft as applied in the operating room and office. The patients presented initially as inpatient consults with non-healing wounds and multiple comorbidies. Each underwent a formal debridement with graft application in the operating room and subsequent graft applications in the office. The progress was documented photographically and with a percent area wound reduction (PAWR) calculation.
This is an in vivo case series that documents the wound healing of (2) patients under real world conditions. Each patient underwent vascular intervention prior to the first graft application. Both patients have diabetes mellitus with peripheral neuropathy, additionally, the first was a new hemodialysis patient with anemia of chronic disease. Both patients demonstrated a drastic decrease in PAWR as compared to their treatment prior to the piscine acellular graft applications. Clinical reduction in inflammation and peri-wound erythema was also documented.
It is believed the piscine acellular graft product was vital to the healing process with regard to the patients in this case series. Even in the arena of instances with non-compliance and minor setbacks commonly encountered in the real world, both patients went on to complete wound healing.
[P23] The Use of Maltodextrin/Ascorbic Acid dressing as a treatment of limb preservation, a Simple dressing
Unidad de Pie Diabetico, Caja de Seguro Social, Panama, Panama
The aim of this study is to describe and demonstrate the effectiviness of a limb preservation treatment protocol that utilizes sharp debridement, a maltodextrin/ascorbic acid dressing, gauze and off loading.
Case series that enrolled 21 patients with Wagner stage 3 or 4. Wound underwent initial surgical debridement upon presentation. All wound were dressed with maltodextrin dressing and secured with gauze as a secondary dressing. Appropiate offloanding was prescribed to each patient and dressing change occurred daily. Patients were followed up once a week for assessment and sharp debridement as indicated. Treatment continued until the wound resolved or the clinician resolved the wound with grafting. Wounds were assessed by digital planimetry to quantify wound healing. Results were analysed by calculation of K-M survival curves to determine probability of healing as a function of time.
Nineteen of 22 wound achieved complete hearing during the study. The remaining three wound were resolved with skin grafts; however these wounds achieved at least 70% healing. Survival analysis indicated a 50% probability of complete healing at 104 days and 50% probability of 70% healing was achieved al 56 days. Rapid granulation tissue formation was observed for all patients with the mean time to 80% coverage at 29.7 days.
The results of this study demonstrate that this protocol utilizing a maltodextrin based dressing evokes rapid wound healing in stage III and IV diabetic foot ulcers.
[P24] Impact of violet light on wound care
North East London NHS Foundation Trust, London, United Kingdom
To demonstrate the effectiveness of podiatry input in diabetic foot ulcers using a Moleculight i:X (( MolecuLight, Toronto, Canada) camera which uses violet light to identify potentially harmful levels of bacteria in a wound. The images allowed clinicians to quickly, safely and easily visualise bacteria and accurately measure wounds at the point of care.
The debridement of wounds on the lower limb is a core skill of the podiatrist. Debridement aims to remove devitalised tissue and enables full inspection of the wound bed and underlying structures. It also helps with drainage of exudate and allows samples to be taken for microbiological examination.
We took images using the Moleculight i:X of a series of diabetic foot ulcers pre and post sharp debridement to demonstrate the impact of debridement on the wound bed and surrounding tissues.
Images which showed potentially harmful levels of bacteria in the wound bed or peri-wound area were shown to be visibly improved following sharp debridement. The wound bed also appeared healthier with less fluorescing bacteria visible.
The Moleculight i:X images also provide more precise measurement of irregular wound dimensions and can guide more accurate tissue sampling for microbiological assessment.
The NICE guideline for diabetic foot problems - NG19, encourages the most cost-effective and clinically appropriate dressings; images from the Moleculight i:X can help to inform dressing selection, particularly in regard to expensive antimicrobial dressings such as silver.
Clinicians have found the resulting images very useful in explaining the presence of infection to patients or conversely, reassuring them that a wound is progressing in the right direction, patients report high levels of satisfaction with the use of Moleculight and find it a very helpful and interactive visual tool in clinic.
The Moleculight i:X has the potential to be a highly useful visual tool in demonstrating the value of podiatry input in the treatment of diabetic foot ulcers to other health care professionals who may at times be slow to refer these patients to specialist foot protection teams.
[P25] An accessible web application for determining baseline wound healing trajectory
Tissue Analytics Inc., Baltimore, United States
To build an accessible proof-of-concept platform based on published research that clinicians can leverage to predict time-to-heal for different types of wounds.
A browser-based web application was developed that processed basic user input including wound size, patient age and assessment date. The relationship between size of wound and velocity of repair is modeled by mathematical expressions developed by Noüy et. al. (1916, 1917), to create a baseline for healing expectations.
The interface demonstrates a pathway for the translation of research to practice that is easy for clinicians to use and minimally disruptive to clinical workflow. Using data from the first and second visits, clinicians can determine the likelihood of wound healing within an arbitrary time period.
Future work will incorporate more sophisticated mathematical models leveraging artificial intelligence and real-world datasets to increase prediction accuracy for different patient cohorts.
[P26] Anti-S. aureus, MEDI6389, accelerates wound healing in a polymicrobial dermonecrosis diabetic mouse model
Astrazeneca, Microbial Sciences, Gaithersburg, United States
Diabetic foot infections are often polymicrobial, and the presence of Staphylococcus aureus (SA) has been associated with delayed healing and worse clinical outcome. We developed a polymicrobial skin infection model in diabetic mice to test the hypothesis that targeting SA alone with monoclonal antibodies (mAbs) will accelerate wound healing.
Type 2 diabetic (db/db−/−) mice were intra-dermally infected with SA (1e6CFU), Pseudomonas aeruginosa (PA) (1e5CFU) and Streptococcus pyogenes (SP) (10CFU), and therapeutically immunized after infection with control IgG (c-IgG) or MEDI6389, a 3 mAb combination targeting alpha toxin, 4 secreted leukotoxins, and the cell surface adhesin clumping factor A (ClfA). By binding and neutralizing multiple virulence factors, MEDI6389 effectively blocks bacterial agglutination and SA-mediated cell killing, abrogates SA-mediated immune evasion and targets the bacteria for opsonophagocytic killing. Bacterial burden, pro-inflammatory mediators, lesion size and wound healing were monitored for 40 days.
Infection of diabetic mice with SA/PA/SP resulted in rapid bacterial proliferation, a prolonged pro-inflammatory response and large dermonecrotic lesions that were not healed 40 days post-infection. MEDI6389 showed a therapeutic window up to 8hrs after infection for significant reduction of lesion sizes compared to c-IgG and resulted in complete wound closure and reepithelization in 21 days vs. >45 days in c-IgG immunized mice. In contrast, monotherapy with any single mAb comprising MEDI6389 did not result in wound healing. Targeting a single pathogen with MEDI6389 not only accelerated SA clearance from the wound, but resulted in a significant reduction in both SP and PA CFU along with significant decreases in multiple pro-inflammatory mediators compared to c-IgG.
Collectively our data suggest that targeting SA with a specific multi-mechanistic mAb combination decreases disease severity and accelerates time to healing in a polymicrobial diabetic skin infection model. MEDI6389 therefore holds promise as an immunotherapeutic approach against DFU complications.
[P27] The Power of a Standardized Approach to Wound Care: Diabetic Foot Ulcers
Sanford Health, Fargo, United States
A diabetic foot ulcer (DFU) and the challenges that patients with diabetes face can be devastating. In fact, the five year mortality rate in diabetics with any lower extremity amputation has been reported at over 50%.1
A standardized checklist approach to diabetic wound care has been proposed to provide clinicians with a set of tools to support effective and evidence-based decision making to help them overcome some of the most common barriers to effective wound healing. This holistic approach is designed to meet providers’ and patients’ needs at every stage of the wound healing process, including accurate and early diagnosis, adequate wound bed preparation, the use of advanced cellular tissue products, and optimal offloading.2
Here, the authors present cases in which the standardized checklist wound care methodology has been applied to improve healing in patients with DFUs. The patients in this case series underwent adequate wound bed preparation with the use of serial sharp debridement procedures, the application of advanced cellular tissue products and adequate offloading.
Each of the patients showed complete healing and avoided amputation. The authors believe that this approach to DFUs can streamline clinical processes, standardize care and improve patient outcomes.
Thorud JC, Plemmons B, Buckley CJ, Shibuya N, Jupiter DC. Mortality After Nontraumatic Major Amputation Among Patients With Diabetes and Peripheral Vascular Disease: A Systematic Review. J Foot Ankle Surg. 2016 May-Jun;55(3):591-9.
Snyder RJ, Jensen J, Applewhite AJ, Couch K, Joseph WS, Lantis Ii JC, Serena TE. A Standardized Approach to Evaluating Lower Extremity Chronic Wounds Using a Checklist. Wounds. 2019 May;31(5 Suppl):S29-S44.
[P58] Pilot Study Assessing Novel Autologous Homologous Skin Construct Treatment of Non Healing Diabetic Foot Wounds
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
Diabetic foot ulcers (DFUs) are a significant burden on the worldwide health care system. These chronic lower extremity wounds are often refractory to standard of care and can result in lower extremity amputation. A novel autologous homologous skin construct (AHSC) using the patient’s dermal regenerative cellular populations was evaluated in a pilot study for the treatment of DFUs.
11 patients with DFUs refractory to at least a month of conservative care were treated with a single application of AHSC. A 1.5cm2 proximal calf harvest of full-thickness skin was collected in the clinic and sent to an FDA-registered facility where it was processed into AHSC and returned to the provider within 48-hours. AHSC was spread evenly across the wound, dressed with silicone, secured with steri-strips, and bolstered with an absorbent foam covered by a triple-layer compression wrap. Healing was documented with digital photography and planimetry during weekly dressing changes. Wound closure was verified 2 weeks following initial closure documentation. All wounds demonstrated graft take one week after ASHC application. 10/11 DFU patients (90.9%) had healed DFUs with a mean time to heal of 29.7 days [SD: 4.98; 95% CI: 19.9-39.4]. At 4 weeks, the mean PAR for all 11 wounds was 83.1% [SD:31.3% CI: 14.4-35.6]. 1 DFU patient developed a secondary infection not related to AHSC therapy requiring debridement and was withdrawn from the study 21 days after deployment. There were 2 AEs (18.1%), including 1 serious AE, neither was related to the study device or application procedure. All wounds remained closed at 2-week durability follow-up. All full thickness skin donor harvest sites remained closed with minimal morbidity. AHSC successfully closed DFUs refractory to dressing care with a single application in this pilot study warranting further evaluation with randomized controlled trials.
WIRB approved
[P59] Mechanism of Action of a Novel Advanced Wound Care Matrix
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
The authors recently described the safety and performance of a novel advanced wound care matrix (AWCM) in an IRB-approved retrospective study with 10 diabetic foot ulcer patients (1). This matrix consists of an upper compact layer and a lower porous layer, which mimic the structure of the basement membrane and dermis of human skin (2). Here we describe the investigation of possible mechanism of action underlying the clinical performance of this novel AWCM.
1.) Incubation of the AWCM with specific matrix metalloproteinases (MMP)-1, 2 and 9 which are most abundant in chronic wound exudates led to a reduction in the activity of MMP-1 by 55%, MMP-2 by 96% and MMP-9 by 66%, suggesting an activity modulation by the AWCM.
2.) Cell activity assays revealed an equally strong activity of healing-related growth factors (e.g. TGF-β1, bFGF and VEGF) at 0h and 72h after incubation and after subsequent washing of the AWCM, indicating that these growth factors were bound and preserved by the AWCM.
3.) Boyden Chamber Assays using human keratinocytes showed an equal number of migrated cells in wells incubated with the AWCM compared to growth supplement, which served as a positive control. Cell numbers in test and positive control were above the negative control. In addition, keratinocytes, fibroblasts and endothelial cells were successfully grown on the AWCM. Thus, the AWCM provided a favorable environment that enabled cell attachment and migration.
Based on these data we conclude that the novel bilayer AWCM supports the healing of diabetic foot ulcer by rebalancing MMPs and growth factors and by enabling cells to bind and migrate into the wound.
[P60] A Retrospective Case Series to Evaluate the Safety and Efficacy of a Novel Advanced Wound Care Matrix in the Management of Non-Healing Diabetic Foot Ulcers
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
Advanced Tissue Matrices have shown promise for treating diabetic wounds and other soft tissue defects. Recent advancements in technology have led to the introduction of a novel advanced wound matrix that features a bilayer structure and is specifically designed for the management of chronic wounds (1). The upper dense compact layer protects the wound and the healing process. This upper structure has a smooth texture with significant pull out strength properties to allow suturing (1). It supports growth factor binding and preservation and also provides a scaffold for migrating keratinocytes (2). The lower layer consists of a thick porous layer, which is able to absorb wound fluid (1). It modulates matrix metalloproteinase activity and provides optimal structure for cell migration and attachment (2).
The purpose of this case series was to report the efficacy and safety of this novel graft in treating diabetic foot ulcers. Ten consecutive patients with non-healing diabetic foot ulcers persisting longer than 4 weeks, Wagner one and two, received weekly application of the bilayer matrix along with standard wound care at a single wound center. These wounds were evaluated at weekly intervals for up to 12 weeks. After submission to the central IRB for approval the patients returned to obtain informed consent. The primary endpoint was complete wound closure at 12 weeks. The average wound size was 3.3cm2. At study conclusion, complete wound closure was achieved for 90% of the wounds, with 9/10 moving on to full closure. The average time to complete wound closure was 2.7 weeks. There were no serious adverse events related to the graft treatment group.
In conclusion, this case series suggests that this unique, bilayer advanced wound matrix may be an effective and safe method for treatment of diabetic foot ulcers. Larger pivotal studies are underway to confirm or refute these initially promising findings.
WIRB approved
[P61] A Prospective, Randomized, Controlled, Multi-Center Comparative Study of Two Application Regimens of Amniotic Membrane Wound Graft Application Versus Standard of Care in the Management of Non Healing Venous Leg Ulcers
SerenaGroup Inc
Venous leg ulcerations (VLUs) frequently represent a significant clinical challenge. Dehydrated human amnion and chorion allografts have shown great promise in the treatment of recalcitrant VLUs when compared to standard wound care (SOC) alone which includes debridement followed by multilayer compression therapy with a primary absorptive dressing. Adding placental grafts into the treatment regimen is often successful as they are rich in extracellular matrix proteins, growth factors, and cytokines, and as such can induce angiogenesis and dermal fibroblast proliferation which can lead to accelerated healing. Aseptically processed grafts may have a benefit over those that are terminally sterilized. The goal of this study was to compare aseptically processed dehydrated human amnion and chorion allograft (dHACA) applied weekly or biweekly combined with standard wound care versus standard of care alone in facilitating wound closure in non-healing VLUs. The research was reviewed and approved by the Western Institutional Review Board and registered on Clinical Trials.gov. Patients with non healing VLUs treated with SOC (appropriate debridement, primary absorptive dressing and multilayer compression) after a 2-week screening period were randomized to either receive SOC (20 patients) or wound-size-specific dHACA plus SOC applied weekly (20 patients) or wound-size-specific dHACA plus SOC applied bi-weekly (20 patients) for up to 12 weeks. Primary endpoint of this clinical trial was percent of patients healed and completely epithialized at 12 weeks. At study conclusion, both weekly and biweekly application of dHACA was statistically significantly better at healing VLUs then standard wound therapy and at a faster overall rate. In conclusion, aseptically processed dHACA should be considered as a viable option for the refractory venous leg wounds.
WIRB approved
[P62] A Prospective Multi-Center Study of a Weekly Application Regimen of Viable Human Amnion Membrane Allograft in the Management of Non Healing Diabetic Foot Ulcers
Feinberg School of Medicine, Northwestern University
Non Healing Diabetic Foot Ulcers (DFU’s) frequently represent a significant clinical challenge. Cryopreserved viable human amnion membrane (vHAMA) has shown great promise in the treatment of recalcitrant DFU’s as a supplement to standard of care. Adding these placental grafts into the treatment regimen is often successful as they are rich in extracellular matrix proteins, growth factors, and cytokines, and as such can induce angiogenesis and dermal fibroblast proliferation which can lead to accelerated healing. The purpose of this prospective study was to report the efficacy and safety of this novel graft in treating non healing diabetic foot ulcers. The research was reviewed and approved by the Western Institutional Review Board. Twenty patients with non healing DFUs treated with SOC (off-loading, appropriate debridement, and moist wound care) after a 2-week screening period were enrolled and received weekly application of vHAMA for up to 12 weeks. Primary endpoint of this clinical trial was percent of patients healed and completely epithialized at 12 weeks. At study conclusion, 85% of the patient receiving weekly application of vHAMA healed. In conclusion, aseptically processed vHAMA should be considered as a viable option for the refractory diabetic foot wound.
WIRB approved
[P28] Evaluation studies of a new Device - Neurotouch for screening Diabetic Peripheral Neuropathy
Foot Secure, Bangalore, India
Increased incidences and cost of diabetic peripheral neuropathy has necessitated large scale screening for DPN. However, existing devices does not support the same. A multi parameter screening device, NEUROTOUCH ((Yostra Labs, Karnataka, India) has been able to meet the requirement.
This study provides comparative analysis of NEUROTOUCH with the gold standard DPN diagnostic device.
Total of 1,344 subjects with diabetes were recruited from different hospitals in India based on inclusion and exclusion criteria for this comparative study. In order to eliminate inter measurer and intra-measurer variability, the paramedic staff were trained.
Monofilament test for tactile sensation, Vibration perception threshold (VPT), Hot and Cold perception (HCP), and IR thermometry for skin temperature were done using available standard devices in the hospital. Same parameters were measured using NEUROTOUCH device which has all the four tests in one device. Reports from NEUROTOUCH were generated using Bluetooth technology.
Statistical analysis of collected data with standard devices and NEUROTOUCH device was carried out. For VPT specificity and sensitivity of 95%, 80.7% was obtained. Infra-Red thermal skin measurements, when compared with the standard device, showed an interclass correlation of 0.89. For HCP threshold an interclass correlation of 0.68 and 0.69 was obtained respectively.
Tactile threshold measurements by conventional method is highly subjective with respect to results and does not give any quantifiable measurement.
NEUROTOUCH gives quantitative results in Grams of force applied by the filament tip, so statistical analysis of this parameter could not be done. As the tactile perception threshold is measured in grams by NEUROTOUCH the inter measurer and intra measurer variability was not seen.
NEUROTOUCH the device presents an innovative, compact and multimodality approach for screening peripheral neuropathy in type 2 Diabetes. It showed good sensitivity and specificity especially across all the four parameters when compared with gold standard devices. It is a single valuable device for detecting neuropathic abnormalities at point of care.
NEUROTOUCH DEVICE

[P29] EdenPump - A Self-powered Wearable Polymer Muscle Pump for Wound Care Treatment
Eden Medical, Inc., Howard Lake, United States
Diabetic foot ulcerations are one of the most common complications associated w/diabetes with a global annual incidence of 6.3%. The lifetime incidence of foot ulcers in diabetic patients is 19-34%. More than 50% of diabetic ulcers become infected and 20% of those w/moderate-severe infection result in amputation.
A body-worn US patented self-powered medical-grade pump has been developed as is a new advance in woundcare treatment for therapeutic agent delivery, infection management and promotion of wound healing. The pump has been successfully clinically tested in a smart dressing for ostomy therapy. The dime-sized pump has demonstrated dispensing up to 200 micro-liters of sealant without any electrical power. The pump features a hydrogel based muscle actuator which is disposable and a low-cost solution for wearable therapy for diabetic foot wounds.
A Phase 2 Small Business Innovative Research (SBIR) study involved 15 human subjects including 7 males and 8 females as an outpatient-based observational study. The pump was integrated in the dressing appliance to prevent leakage with a bio-friendly sealant. A total of 2,222 hours (92 days) of ostomy wear and leakage data was collected involving colostomy, ileostomy, and urostomy patients. A successful sealant delivery was achieved with ten subjects during the 10 day trial. Six of the ten subjects experienced an extended wear-time (i.e. 15 minutes to 7 hours 10 minutes) during the course of the study.
Conclusions:
Preventing leakage and extending wear time is achievable which can reduce skin breakdown and denuding. The pump can be used for antiseptic/antibiotic delivery, oncology, wound irrigation, pain treatment, tissue positioning/separation, and sealant dispensing. The pump construction features rapid prototyping 3-D printing fabrication, which offers low cost manufacturing and scalability.

[P30] Characteristics of Gait Initiation Phase in Older Adults with Diabetic Peripheral Neuropathy
Baylor College of Medicine, Icamp, Houston, United States
Impairment in steady-state gait in older adults with diabetic peripheral neuropathy (OADPN) is well-known, however little attention has been paid to gait initiation phase in which posture changes from upright standing to steady-state gait. We investigated kinematic characteristics of gait initiation phase in OADPN compared to healthy older adults (HOA).
We recruited 33 OADPN (25 women; age=72.7±5.5 years; body mass index (BMI)=31.16±5.71 kg/m2; maximum vibration perception threshold on either foot=37.09±8.64 V), and 38 HOA (12 women; 78.3±8.2 years; 27.11±4.21 kg/m2; no history of cardiovascular, neurological or orthopedic condition; no history of falling in the past 12 months). Subjects performed gait from an upright standing posture on level ground for minimum 10 meters at self-selected comfortable speed. We collected kinematic data using five wearable sensors (LEGSysTM, BioSensics LLC, Watertown, MA) attached on the shanks, thighs and lower back. We used previously validated algorithm to analyze kinematic parameters for gait initiation phase.
The number of steps and distance to reach steady-state gait from an upright standing posture was 77.3% and 64.8% greater for OADPN (3.9±2.1 steps and 2.06±1.42 m, respectively) than for HOA (2.2±0.8 steps and 1.25±0.53 m, respectively) (p<0.001 and p=0.004, respectively). Mean stride velocity during gait initiation phase was marginally less for OADPN (1.00±0.27 m/s) than for HOA (1.10±0.19 m/s) (p = 0.087). Gait cycle time (i.e., duration for one gait cycle) and double limb support (i.e., duration when both foot are in contact with the ground in one gait cycle) were 6.3% and 20.0% greater for OADPN (1.18±0.14 seconds; 27.65±7.62%, respectively) than for HOA (1.11±0.08 seconds; 23.04±4.93%, respectively) (p=0.020 and 0.003, respectively). Medio-lateral center-of-mass sway in gait initiation phase was 67.7% greater for OADPN (7.53±3.49°) than for HOA (4.49±1.69°) (p<0.001).
The results suggest that OADPN take more, slower and more unstable steps to reach steady-state gait from an upright standing posture compared to HOA. Given the risk of falls in gait initiation phase, the results also provide implications for needs to develop new interventions targeting gait initiation phase in OADPN.
[P31] The Effect of Daily Use of a Wearable Foot Compression Device on Motor Physiology in People with Diabetic Peripheral Neuropathy
Baylor College of Medicine, Icamp, Houston, United States
Individuals with diabetic peripheral neuropathy (DPN) have impaired motor performance. The aim of this study is to examine therapeutic effectiveness of mechanical stimulation through a wearable foot compression device equipped in a shoe insole on pathophysiology and motor performance in individuals with DPN.
Using a single-arm 4-week intervention study design, we examined effectiveness of daily use of shoes equipped with the foot compression device (FootBeat™, AVEX LLC, Colorado, USA) on improving vibration perception threshold (VPTmax), skin perfusion pressure (SPP), ankle brachial index (ABI), circumferences in the calf and ankle, and motor performances (postural sway with eyes open (EO) and eyes closed (EC) conditions, and gait performance during normal walking, dual-task walking and fast walking tasks). Thirty type 2 diabetic individuals with confirmed DPN (11 men; 68.1 ± 9.7 years; 33.4 ± 6.1 kg/m2) participated in this study.
VPTmax decreased post-treatment (27.4 ± 12.6 volts for pre-treatment and 23.3 ± 11.9 volts for post-treatment; p = 0.007). Center-of-mass sway in the medio-lateral direction decreased for both EO and EC conditions post-treatment (0.94 ± 0.43 cm for pre-treatment and 0.76 ± 0.32 cm for post-treatment, p = 0.020; 1.10 ± 0.45 cm for pre-treatment and 0.83 ± 0.37 cm for post-treatment, p = 0.033, respectively). Stride velocity increased for normal walking, dual-task walking and fast walking tasks post-treatment (0.87 ± 0.21 m/s for pre-treatment and 0.96 ± 0.23 m/s for post-treatment, p = 0.017; 0.75 ± 0.18 m/s for pre-treatment and 0.91 ± 0.23 m/s for post-treatment, p = 0.001; 1.10 ± 0.33 m/s for pre-treatment and 1.20 ± 0.27 m/s for post-treatment, p = 0.043, respectively). There was no significant changes in SPP, ABI and circumferences in the calf and ankle.
Our findings suggest the wearable foot compression device may be effective for treating neuropathic symptoms and motor performances in individuals with DPN.
This work was funded by AVEX LLC.
[P32] SnapshotNIR, a handheld imaging system for noninvasive measurement of transcutaneous hemoglobin oxygenation
Kent Imaging, Calgary, Canada
To demonstrate the utility of the handheld SnapshotNIR hemoglobin saturation imaging system ((Perry Baromedical, Florida, USA) across the wound care continuum.
A series of case studies will be presented that demonstrate the versatile role SnapshotNIR (hemoglobin saturation imaging can play in the various facets of lower limb and chronic wound assessment.
Instrumental methods to determine the adequacy of local oxygen delivery either measure regional blood flow or perfusion, local hemoglobin oxygen saturation, or dissolved oxygen pressure of the underlying tissue. While distinct measurements, these parameters are often highly correlated. Bowen et al (SM Vasc Med. 2016; 1(2): 1006) recently demonstrated the correlation between SnapshotNIR hemoglobin saturation and transcutaneous oxygen pressure in patients with chronic wounds. Data from Jones et al (PRS in-press 2019) demonstrated the non-inferiority of SnapshotNIR oxygenation and SPY laser fluorescence perfusion imaging in predicting murine flap necrosis. These comparative studies suggest that SnapshotNIR hemoglobin saturation, at the very least, compliment traditional oxygen pressure measurements or peripheral circulation perfusion measurements. We demonstrate that SnapshotNIR has added convenience over the current state-of-the-art methods and is suitable for use across the continuum of care, from initial assessment to continued wound management.
SnapshotNIR measurements can detect local deficits in oxygen delivery to tissue, non-invasively, in near real-time, with no consumables. This simple, battery-powered imaging device surveys large areas of tissue quickly making it suitable for the operating room or clinic settings where space and infrastructure are at a premium.
[P33] Gait, Balance, and Frailty: A Comparison Between Hemodialysis Patients with and Without Obesity
Baylor College of Medicine, Houston, United States
Obesity is a common epidemic among patients with diabetes undergoing hemodialysis (HD). It is well known that obesity is associated with gait and balance function decline in general population. On the other hand, in patients with frailty symptom, due to muscle loss, the weight may reduce as well as motor function. In this study, we hypothesized that HD patients with obesity may have better gait and balance than HD patient without obesity.
Seventy-four HD patients with diabetes were recruited. Based on the BMI cutoff of 30kg/m2 or larger, 39 subjects were classified as obesity (age=64.6±7.6years, BMI=36.9±5.9kg/m2) and 35 subjects were classified as non-obesity (age=64.6±9.6years, BMI=25.4±2.4kg/m2). Gait and balance parameters were quantified using validated wearable platforms. Physical frailty status was assessed by Fried Frailty Criteria.
Subjects in the obese group had 12% faster stride velocity, 6% longer stride length, and 12% shorter gait cycle time than subjects in the non-obese group. They also had 28% better ankle stability and 35% better hip stability, as well as 37% less center of mass sway. The prevalence of frailty was 10% lower in the obese group.
Overall, aligned with our initial hypotheses, HD patients in the obese group had better gait and balance compared to the non-obese group, however these trends didn’t achieve statistically significant level in our sample. We speculate that the observed poorer motor performance in the non-obese group may link to loss of muscle mass caused by prolonged immobility imposed by HD therapy. This hypothesis is supported by higher prevalence of physical frailty observed among the non-obese group. If this is confirmed in a larger sample, results may suggest that tracking BMI and determining involuntary weight loss can provide timely intervention to avoid progression toward frailty and its associated consequences in patients undergoing hemodialysis.
[P34] Albuminuria associated with a history of foot ulcer in patients with type 2 diabetes: An opportunity for early detection of complications in ambulatory podiatric clinics
Western University of Health Sciences, Westernu Health Center, Pomona, United States
Albuminuria can be predictive of morbidity and mortality in patients with type 2 diabetes (T2D), particularly in those hospitalized with diabetic foot ulcers (DFU). The purpose of this study was to assess albuminuria prevalence using point-of-care (POC) testing in a cross-section of patients presenting to an ambulatory podiatric clinic.
Enrolled subjects gave informed consent and completed a brief questionnaire that encompassed their past medical, surgical, and social history; demographic information; tobacco use history; exercise frequency; and reason for their podiatric clinic appointment. A voided urine specimen was obtained and analyzed using the semi-quantitative Clinitek microalbumin 2 reagent strips to determine the urine albumin-creatinine ratio (UACR). Data were analyzed using the SAS software for Windows version 9.3 (Cary, NC). Chi-square analyses were conducted to determine the association between clinical variables. P-value <0.05 was considered statistically significant.
85 patients (45 males; 40 females) were included in final analysis. Patients had multiple complaints of various foot symptoms: 78.3% pain, 32.5% infection, 41% numbness, 43.9% tingling, 23% weakness, 48.2% swelling, and 30.1% cold feet. None reported active DFU. Mean age 53.7 years, 58.8% (n=50) Hispanic, 41 patients (48%) had T2D, 32 (38%) had hypertension, and 28 (33%) history of DFU.
UACR results categorized into three groups: 1. normal (<30mg/g); 2. microalbuminuria (30-300mg/g); or 3. macroalbuminuria (>300mg/g). Seventeen (20%) had microalbuminuria, 8 (9%) had macroalbuminuria, and 60 (70.6%) had UACR<30mg/g. Subjects with history of DFU, 35.7% had microalbuminuria and 17.9% had macroalbuminuria. In contrast, those without a history of DFU, 12.3% had microalbuminuria and 5.3% had macroalbuminuria (p=0.0028).
Subjects subdivided into four groups: A) T2D without history of FU- [foot ulcers]; B) T2D with history of FU; C) No T2D and No FU; and D) History of FU without diabetes.
Patients with T2D and history of FU were twice likely to have albuminuria compared to those without history of DFU and five times more likely than those with neither T2D nor history of FU. Using POC-UACR testing in podiatric clinic offers opportunity for screening and monitoring albuminuria at risk patients.
[P35] Effectiveness of daily use of bilateral customized ankle-foot orthoses to reduce foot pain in older adults
Baylor College of Medicine, Houston, United States
Foot pain is prevalent in older adults and is associated with fall risk and disability. This study aims to examine whether daily use of the bilateral custom-made AFOs can reduce foot pain.
Ambulatory older adults (n=44, age=74.7±6.4, 70% female, 64% history of fall) were randomly assigned (ratio=1:1) to an Intervention Group (IG) which received AFOs and fitted walking shoes, and a Control Group (CG) which received fitted walking shoes. Participants in both groups were encouraged to wear the prescribed footwear at all times, especially during walking and standing. Visual analog scale (VAS) was used to assess the pain of each foot at baseline, 6-month, and 12-month visits. The outcome measure was the maximum of foot pain score obtained from the right and left feet at each visit.
In the IG, there was significant change in foot pain across baseline, 6-month and 12-month assessments (p = 0.030). Compared with baseline, the participants in the IG had significantly less foot pain at 6-month (−40.5%, p = 0.011), and at 12-month (−73.0%, p = 0.010) assessments. In contrast, no significant change in foot pain was found across baseline, 6-month and 12-month assessments (p = 0.682) in the CG. Although there was also reduction in foot pain observed at 6-month (−44.5%) and 12-month (−26.1%) assessments, none of them achieve statistical significance (p > 0.05).
This study suggested that daily use of bilateral custom-made AFOs is effective to reduce foot pain possibly by lowering plantar pressure. The reduction of foot pain due to custom-made AFOs could potentially increase adherence and acceptability of AFO use, leading to improvements in physical activity levels and quality of life.
[P36] Using plantar electrical stimulation during routine dialysis process to improve gait and balance in people with diabetes undergoing hemodialysis
Baylor College of Medicine, Icamp, Houston, United States
People with diabetes undergoing hemodialysis (HD) are suffering from deteriorated gait and balance. Many of these patients receive routine HD treatments every week, providing an optimal opportunity for intervention. This study examined the feasibility and effectiveness of a plantar electrical stimulation during routine HD process to improve gait and balance.
Twenty-six participants with diabetes receiving HD were recruited and randomized into an intervention group (IG: n=13, age=59.5±10.4years, BMI=29.7±6.0kg/m2, female=39%) or a control group (CG: n=13, age=63.2±6.1years, BMI=30.9±6.0kg/m2, female=54%). The IG received 1-hour electrical stimulation on plantar regions during routine HD process (3 sessions/week) for 12 weeks. The CG was provided with an identical but non-functional device for the same period. Participants were blinded to the group allocation. Gait and balance were examined using validated wearable platforms at baseline, midline (6-week), and conclusion of the program. This study however focused on changes in gait and balance at 6-week.
All participants in the IG completed all electrical stimulation sessions indicating the feasibility. Compare to the baseline, the CG didn’t have noticeable change in gait performance at 6-week (p>0.050, Cohen’s effect size d=0.12-0.25). However, improvement trends were observed in the IG for all gait parameters with the largest effect observed in double support (13% improvement, d=0.66). At 6-week, the CG showed trends of deterioration in balance control (19-95% deterioration, d=0.22-0.45) while the IG showed trends of improvement with the largest effect observed in Center of Mass Sway (27% improvement, d=0.31).
This study provides early results of plantar electrical stimulation during routine dialysis. It is still ongoing and is expected to recruit 100 participants. If results can hold in a larger sample size, it may recommend routine plantar electrical stimulation therapy to improve mobility and potentially prevent falls in hemodialysis patients.
[P37] Framework for designing diabetic sandals for the Indian patient
Northeastern University, 360 Huntington Ave, Boston, United States
India is the diabetes capital of the world with over 80 million diabetics (IDF). Current preventive diabetic footwear results in non-adherence as patients lament the quality, style and effectiveness of the footwear. We have studied how to design and make diabetic sandals using indigenous materials for the Indian consumer.
The first phase of research involved personal interviews with 250 diabetic males between the age of 45-55 years spread across the country to understand the characteristics of ideal sandals for them after the consideration of geographical, cultural and climatic factors. The second phase involved consulation with leading diabetologists and podiatrists to identify special concerns for the needs of diabetic feet in India. Then, by collaboration with footwear designers and component manufacturers in Italy, we designed a range of footwear that combines the needs of the caregiver and patient to thereby improve adherence.
73.2% of patients preferred sandals (incl. chappals) over shoes and the sweet spot in pricing was found to be $30-$35. Historical popularity of the paduka and then the Hawaii chappal, results in a strong preference for thongs and toerings. To counter pressure point created due to the thong, a layer of foam surrounded by leather was added. 68.4% of patients preferred open-toed sandals which are often susceptible to injury. Hence, we added a protective leather welt in the front of the sole. Caregivers complained about the lack of physical activity so we have added metatarsal pads in the footbed which provides a massaging effect and encourages walking. Patients donot throw sandals until they are visibly damaged and continue using the current MCP sandals even after insoles have bottomed out resulting in injuries. We used a high-durability crystallized PU memory foam insole (25 Shore A hardness.)

Infographic with features
There is an increase in adherence of preventive diabetic footwear among Indian diabetic patients when given designs they are familiar with whilst also keeping costs between $30-$35. The framework for these designs are made by meeting the requirements laid down by caregivers.
[P38] Diabetic foot ulcer outcomes in two hospitals in Bahrain
Royal College of Surgeons in Ireland, Medical University of Bahrain, Dublin, Ireland
One third of DFUs will result in either a minor or major amputation with a 50% recurrence rate within 5 years2, 3 and following amputation for a complicated DFU, the mortality rate is significantly higher at 59% after 3 years4. There is however, little data available on the outcome of diabetic foot ulcers in the literature and more research is needed6, 7.The aim of this study was to gain insight of DFU outcomes in two hospitals in Bahrain.
This is record review of patients with DFUs attending two hospitals in Bahrain between January 1st, 2017 and January 1st, 2018. The ulcer outcomes were defined as healed, unhealed, amputated or unknown outcome8.
A total of 338 patients between the ages of 26 and 92 were included the study. 247(73%) were males out of which 62.37% were of Bahraini nationality and 91(26.9%) were females with the majority (68.13%) being Bahraini nationals. The mean age of patients with DFUs was 60.93 (SD:12.489). With analysis of outcomes, the largest group of 115 patients (34%) had an unknown outcome and when excluded, 43% of ulcers were healed, 42.2% were unhealed and 14.8% were resolved by amputation. Females were more likely than male patients to end up with a healed ulcer (OR: 1.42) and were also significantly less likely to have a limb amputated in order to resolve an ulcer (OR:0.37).
The findings in this study demonstrates the demographic characteristics of ulcer outcomes in patients with DFUs in Bahrain.
RCSI Bahrain Dilmun Project
[P39] Use of Integra Dermal regeneration Template for Limb Salvage in Diabetic Patients with no-option Critical Limb Ischemia
Caja Costarricense del Seguro Social, Hospital San Juan de Dios, Vascular Surgery, San Jose, Costa Rica
Evaluate the use and efficacy of the dermal substitute Integra® Dermal Regeneration Template (Integra LifeSciences, New Jersey, United States) for treatment and limb salvage in diabetic patients with no-option critical limb ischemia.
Retrospective single center study Diabetic Foot Unit of Maria Cecilia Hospital, for critical limb ischemia patients. The primary end-point was one year amputation rate and limb salvage. The secondary end-point was Healing Time.
Between October 2014 and October 2017, 1024 patients with Critical Limb Ischemia (CLI) were admitted. A total of 1981 lower limb angiographies were carried out. In all the patients either an endovascular or surgical procedure was performed. In 84 patients (8.2%) there was a failure in distal revascularization with a persistent CLI after the procedure. This group was considered the no-option CLI population, with a mean Transcutaneous Oximetry (TCOM) < 20mmHg. Despite the persistent CLI, 25 patients of this cohort obtained the complete wound healing, 12 patients were treated Integra®, the others were treated with any dermal substitute. No major amputation was carried out at 1 year follow up in Integra ® group vs 15% in the control group. Integra ® group healed within a mean time of 83,5 days and the non Integra® group healed within a mean of 139 days (p-value 0.028).
A conservative foot surgery in diabetic patients with no-option CLI may achieve limb salvage and may improve amputation rates, besides a failed or suboptimal revascularization. The use of Integra ® in patients with diabetic Foot Ulcers (DFU) and no-option CLI may be an useful option in limb salvage program.
[P40] Seasonality in Foot Inflammation Detected by a Telemedicine Once-Daily Temperature Monitoring Mat
Podimetrics, Inc., Somerville, United States
Existing research on seasonality of diabetic foot complications is limited to two retrospective studies of complications in temperate climates (Armstrong, 1997; Leung, 2007). These studies reported peak outcomes in warm weather months. We aimed to characterize the seasonal pattern of foot inflammation in an arid desert climate.
We analyzed foot temperature data from a once-daily telemedicine temperature monitoring mat in a cohort of 542 patients living in the American Southwest. Patients were prescribed the mat from high risk foot clinics for the purpose of monitoring for early detection and prevention of diabetic foot ulcers. More than 425,000 foot temperature readings, or “scans,” were collected over a three year period. We assessed the percentage of scans on any given day that had signs of inflammation, which we defined as a temperature differences between the left and right foot exceeding 4.0°F.
Per Figure 1, a patient scan was most likely to have inflammation from late November through March and least likely to be detected from June to September. The mean temperature in this region during these periods is 70.2°F and 104°F, respectively. These results differ from but are not necessarily inconsistent with those from Armstrong 1997 and Leung 2007. Indeed, warm weather months in New York and Hong Kong are similar climatologically to the winter months in the American Southwest. One potential explanation that reconciles previously-published data with ours is that pedal inflammation preceding non-acute diabetic foot outcomes is due to repetitive microtrauma, which increases with activity during months with “nice” weather. One strength of this study is we report seasonal inflammation. This lends further evidence that seasonality in diabetic foot outcomes is due to increases in activity and repetitive microtrauma as opposed to acute injury or some non-physiological mechanism.

The potential implications of this research are many. If the likelihood of poor outcomes is highest during “nice” weather, providers should provision high quality preventive care before and during these periods of elevated risk. Evidence-based practices include routine exams, frequent foot and footwear inspection, and once-daily foot temperature monitoring.
[P42] Renal foot services - moving away from the Cinderella story?
Barts Health NHS Trust, Whipps Cross Hospital, London, United Kingdom
Diabetic foot disease is considered the Cinderella of diabetic complications. Patients on haemodialysis form a further ill-served subset, at greater risk of foot ulceration and amputations. These patients fail to access podiatry services despite spending a large amount of time in a clinical setting, resulting in increased morbidity and mortality.
A survey revealed that of 90 random patients on haemodialysis, 56 had diabetes. 10 had pre-existing foot problems, and only 6 reported regular podiatry input. Key reasons for this included lack of capacity within the podiatry service to deliver regular input unless ulceration was established, and missed appointments by patients who were accessing healthcare services up to 12 hours each week.
A screening program was developed by diabetes, podiatry and renal team staff. This involved a comprehensive training program with a multidisciplinary model involving the lead podiatrist and dialysis nurses working together to assess and screen patients.
Five haemodialysis nurses across 4 units volunteered to be ‘foot champions’ on their respective units, and underwent structured training and assessments delivered by the lead podiatrist.
Patients are given a high risk foot leaflet and have their feet screened on a monthly basis to check the following: open wounds, palpable temperature difference, pain or swelling, new / worsening discolouration, corns / callus.
Anyone identified as requiring podiatry review is referred via a fast-track pathway to podiatry.
After two months, we have already received 8 new referrals for active foot disease; of which 1 has required input from the diabetic foot multi-disciplinary team.
Patients on the haemodialysis unit report high levels of satisfaction with the new service, and are confident that they now have a point of contact on the unit should they develop any concerns regarding their foot health going forward.
Patients on dialysis have high risk of foot ulceration and should receive regular podiatry input every 8 – 12 weeks.
Without additional resources, we have established a robust pathway for haemodialysis patients to access foot screening. We aim to extend this model across our entire haemodialysis population of over 1200 patients.
[P43] Plain radiographic utilization for diabetic foot ulcer management
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
Imaging surveillance patterns on diabetic foot ulcers are not as well understood. This survey aimed to reveal the current practice pattern in the podiatric community.
We designed a prospective, voluntary, online survey which would be disseminated by the American Podiatric Medical Association (APMA). Our sampling strategy consisted of all actively practicing podiatrists who were members of the APMA. We then analyzed de-identified and aggregated survey results. Dartmouth College Committee for the Protection of Human Subjects (CPHS) exempted the study for non-human research (CPHS#STUDY00031013).
Overall response rate was 5%. For a new diabetic foot ulcer consult, 65.2% participates “always” ordered a plain radiograph, 11.3% ordered a plain radiograph if they felt it could have been infected in the past, 21.2% would order a plain radiograph if the ulcer looked infected at the time of the consult and 2.3% reported they would use other imaging modalities. MRI was the alternative modality that was most commonly described. If an established diabetic patient returned with a new foot ulcer, 45% “always” ordered a plain radiograph and 37.6% would only order a plain radiograph when the ulcer appeared infected. If an established diabetic patient presented with a new ulcer that could have been infected, 14.2% ordered a plain radiograph. 3.2% reported that they would order other imaging modalities for an established diabetic patient with a new foot ulcer. Again, MRI was the choice of alternative imaging modality.
Our findings demonstrated the variation of plain radiograph use when a diabetic foot ulcer was not infected. Presence of infection narrowed the variability of the treatment plan.
[P44] Predominance of Polymicrobial Infections and Complicated Disease Etiology in Chronic Wounds as Evidenced by Metagenomic NGS Assay
Cosmosid, Aarhus, Denmark
Today’s standard of care for chronic wound diagnosis is based on slow, low-throughput assays targeting one pathogen at a time or trying to culture them. For at-risk patients with vascular, diabetic or pressure ulcers, these assays are limited, require a priori knowledge, and often fail to identify causative agents within a clinically relevant time frame, leading to extreme outcomes. Chronic wounds can contain many infectious agents including fungi, viruses and anaerobes, posing challenges for proper identification and timely appropriate treatment.
CosmosID has introduced CosmosDx (CosmosID, Rockville, Maryland, USA), the first commercially available shotgun metagenomic diagnostic test for chronic wounds. With this test, clinicians receive a detailed report of all microbes and potential pathogens present along with community resistome profiles within 48 hours of sample submission.
We present preliminary results of an ongoing study of >1400 patients, representing the largest clinical cohort subjected to shotgun metagenomic testing to date.
Specimens were collected using eNAT swabs (Copan, Brescia, Italy). We optimized a multi-step sample-to-sequencing process into a highly sensitive, reproducible, bias-free integrated workflow that is tolerant towards low DNA input and overwhelming host background. This Next-Generation Sequencing (NGS) assay offers improved detection of known (previously recognized) pathogens including fungi, viruses and anaerobes as well as their associated microbiomes with fast turnaround time (36-48 hours).
Preliminary results from a subset of 630 patient samples show an increased diagnosis rate as evidenced by very few (n=14, 2.60%) samples with negative results. A single pathogen was identified in only 50 samples (9.29%), whereas 88.10% (n=474) of the samples demonstrated evidence of mixed and/or poly-microbial infection. More than 500 bacterial species and 150 genera were identified, and a large number of microorganisms previously not recognized as wound pathogens were detected in a majority of the samples, including more than 20 species of fungi.
These findings indicate that mixed and/or polymicrobial infections (88.10% of the samples) might be the rule for chronic wounds rather than the exception. The newly identified organisms present in a majority of the samples suggest that chronic wounds are more complex than previously thought. Additionally, the detection of the community resistome can aid therapeutic decisions.
[P45] Healing rates of foot surgery performed by a podiatric surgeon on people with diabetes
Bolton Diabetes Centre, Bolton NHS Foundation Trust, Lancs, United Kingdom
Determine the median healing time for foot surgery performed by a Podiatric Surgeon working within a tertiary vascular service
Outcomes of patients referred to a Podiatric Surgeon between January 2017 and December 2018 were audited. Demographic, vascular intervention, infection status and HbA1c were recorded. Good control was defined as HbA1c between 48-58 mmol/mol. Infection was defined as cellulitis; osteomyelitis diagnosed using plain images or MRI plus monitoring of inflammatory markers.
Vascular intervention was defined as any endovascular or surgical revascularisation. Surgery was divided between amputations, corrective procedures and Charcot revision. Amputations were defined by type i.e. single toe, ray and trans-metatarsal. Healing was defined as 100% closure and healing rates were reported as median time to healing.
109 patients were referred to the Podiatric surgeon and 70 procedures were performed. Of the patients who did not go on for surgery 7.5% had passed away, 7.5% were unfit f, 20% refused and 65% were watchful wait.
The procedures performed included amputation of 14 toes (20%), 27 ray amputations (38.5%), 20 trans-metatarsal amputation (28.5%), charcot revisions (4%) and corrective surgery (9%). Osteomyelitis preceded in 85% of patients who went on to have amputations. 41% of patients had vascular intervention before surgery –60% of patients who had surgery were American Society of Anesthesiologists(ASA) grade 3 whilst the remaining 40% were grade 4
The mean age was 64 years of which 89(81.7%) were male. 91 patients (69%) had type 2 diabetes. The average HbA1c was 63.7mmol/mol
The median time for healing was 36 days. Infection requiring antibiotics was 14.3% at 30 days and 14% requiring further surgery within 6 months
A new service provided by a Podiatric Surgeon to complex vascular patients has provided much faster access to dedicated Podiatric surgical lists and excellent results post operatively. Further discussion will be to consider reasons for infection and correlation between poor diabetes control and previous vascular intervention on the healing rates.
[P46] Analysis of proximal ‘clean’ bone margins in diabetic foot osteomyelitis by conventional culture, DNA sequencing and microscopy
South Western Sydney Limb Preservation and Wound Research, South West Sydney Local Health District, Sydney, Australia
Diabetic foot infections are a common cause of hospitalisation, with osteomyelitis contributing to the risk of lower limb amputation. The International Working Group on the Diabetic Foot suggests diagnosis of osteomyelitis through isolation of bacteria from bone sample, or histological findings to guide antibiotic therapy.
Conventional culture, DNA sequencing and microscopy approaches were employed to detect pathogens from infected and proximal bone margins (presumed to be clean) associated with Diabetic Foot Osteomyelitis (DFO). Intraoperative bone specimens of 14 consecutive subjects with suspected DFO were collected over a six-month study period from Liverpool Hospital, Vascular Surgery Department. Infected bone and a proximal bone margin presumed to be “clean/non-infected” were collected. Bone material was subjected to conventional culture, DNA sequencing and microscopy.
In total, eight of 14 (57%) proximal bone margins had no growth by conventional culture but were identified in all proximal bone specimens by DNA sequencing. Proximal bone margins all had lower median total microbial counts than infected bone specimens, but differences were not statistically significant (clean = median of 5.6 Log10, +/− 0.28 versus infected = median 5.8 Log10, +/−0.6, p = .22). The most commonly sequenced microorganisms were Streptococcus sp., Staphylococcus sp., Peptrostreptococcus sp., and Stenotrophomonas sp. Pathogens identified by sequencing in infected specimens were also identified in proximal margins and the microbiomes were similar (ANOSIM = .02, p = 0.59). Using a combination of SEM and/or PNA-FISH, we visualised the presence of microorganisms in infected bone specimens and corresponding proximal margins of seven patients (50%). Both biofilm and planktonic bacteria were visualised in infected and clean margins.
We identify that bacteria can still reside in what seems to be proximal “clean” margins. The significance of culture-negative – sequence-positive findings and the implications on clinical outcomes requires further analysis from a larger sample size that incorporates differences in surgical and post-operative approaches, correlating any outcomes back to culture-sequence findings.
Scanning electron microscopy image from infected and clean bone specimens.

[P47] Methodological approaches for assessing the cost of diabetic foot ulcers: a systematic literature review
Royal College of Surgeons in Ireland, Medical University of Bahrain, Dublin, Ireland
Diabetic foot ulcers ( DFUs) are a serious complication of diabetes and impose considerable costs on healthcare services, patients, their families and society. Due to these related high costs, studies that explore and measure costs of DFUs are important for prevention and best care practice. Although the framework of cost studies is well established, there may be substantial variations in study populations, type of foot lesion, study designs, costing methodologies and type of costs taken into consideration. This review aimed to evaluate the methodological approaches in assessing costs of DFUs and to explore contributions of different countries to the literature.
A systematic search was conducted in PubMed, Embase, Scopus, Web of Science and CINAHL to identify DFUs cost studies in English. Additionally, bibliographies were inspected to identify other relevant studies. Following the PRISMA guidance, the review analysed study design, analytical perspective, data collection, and analytical methodologies adopted in the included studies.
Twenty-seven studies of the costs related to DFUs were identified. Most studies were conducted in Western countries. The reviewed studies used different study designs, data collection strategies and data sources, which in turn make a systematic comparison of cost estimates unrealistic. Detailed descriptions of applied costing methods and other methodological aspects were often limited or absent. Many studies limited their cost analysis to the healthcare payer’s perspective and disregarded costs to patients, their families and the wider society.
The costs of DFUs have been assessed using a wide range of methodological approaches and are often restricted to the healthcare payer’s perspective. Therefore, cost analyses may underestimate the true societal cost of DFUs. Moreover, there is a need for encouraging further research in the developing world.
[P48] Frequency of skin fungal infections in patients suffering from diabetes mellitus type 2 (dm2) monitored in a diabetic foot outpatient clinic
Tzaneio Prefecture General Hospital of Piraeus, Diabetic Foot Clinic, Pireas, Greece-Footcenter private podology center, Argiroupoli, Attiki, Greece
Diabetic Foot Ulcer (DFU) is a frequent complication of Diabetes Mellitus type 2 (DM2). Diabetic neuropathy, peripheral vasculopathy as well as DM induced immunosupression formulate a pathogenetic backround making these patients prone to localised fungal skin infections (FSI). This study investigates the prevalence of FSI and especially onychomycosis in patients with DM2
A study group of 103 patients (67% men, 65,8±11,0 yo, HbA1c 7,0±1,2%) suffering from DM for 15,7±9,1 years was formed. These patients have been referred to the Diabetic Foot Clinic of Tzaneio General Hospital. We assessed the patients’ clinical and laboratory profile to specify the type of infection they were diagnosed with. Data were processed by SPSS.
It is a case series retrospective study approved by the hospital’s ethics committee. As the first study on this topic in our area, it increased the level of awareness of the health professionals that work or are trained near to us.
The prevalence of candida onychomycosis, onychogryphosis, ingrown nail was respectively 75,5%, 27,1% and18,4%. Onychomycoses were correlated with neuropathy (relative risk1,03, 95% ~1,01-1,10), with BMI (RR: 1,12, 95% ~1,10-1,25), retinopathy, (RR: 1,05, 95% ~1,01-1,30) absence of carers/cohabitants (RR: 1,02, 95% ~ 1,01-1,10). Onychogryphosis was correlated with recurrent lesions, (RR: 1,01, 95% ~1,01-1,10), neuropathy (RR: 1,06, 95% ~1,04-1,46). Ingrown nail was correlated with a low level of self care and hygiene (RR: 1,03, 95% ~1,01-1,10) and neuropathy (RR: 1,04, 95% ~1,01-1,10).
This study indicates that patients with DM2 usually suffer from candida onychomycosis. Neuropathy, (increased) BMI and retinopathy appear as the principal risk factors. Health professionals involved in DFU care ought to be aware of these conditions in detail and in correlation to the aforementioned systematic risk factors.
The most prevalent fungal nail infections among our patients


[P49] Creating an inpatient multidisciplinary team to care for patients with diabetic foot infections
Duke University Hospital, Hospital Medicine Program, Durham, United States
Patients with diabetic foot infections represent a medically and socially complex group where multidisciplinary care is essential. Our academic medical center prioritized creation of an integrated, multidisciplinary inpatient team to care for patients with diabetic foot infections more effectively and efficiently.
A multidisciplinary core team developed resources and care pathways in several priority areas:
guidance for emergency room staff in form of criteria for consults and suggested empiric antibiotics;
routine early involvement of vascular surgery team with use of objective testing;
admission order set including guidance for subspecialty consultations, antibiotic choice, and early involvement of physical therapy;
increased operating room availability to facilitate needed operative interventions;
localization of patients on one general medicine team to facilitate communication and coordination among teams; and
enhanced educational resources for patients and nursing for wound care and amputations.
Initiatives were rolled out sequentially in early 2018. With the creation of a dedicated internal medicine rounding team, the number of medicine attending physicians decreased from 17 different attending physicians in the 6 months preceding our initiative to 10 distinct attending physicians. Patients discharged from the dedicated rounding team have lower length of stay than those discharged from other medicine teams. For the two cohorts (patients with wounds only and those undergoing any amputation), we have seen improvements in length of stay and readmission rates when our admission order set was utilized as outlined in Table 1. We are analyzing data on utilization of consults and impact on patient care (i.e., blood glucose control for patients with endocrinology consultation).
Post-implementation data when admission order set completed versus not completed.


Forging a multidisciplinary inpatient rounding team can lead to more consistent providers for patients and reduce length of stay as well as lower readmission rates for patients with diabetic foot infections.
[P50] Refocusing DFOCUS: An Update to the Diabetic Foot Online Clinic Utilization Score (DFOCUS) to Predict Clinic Volume
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
The goal of this presentation is to demonstrate a useful tool for clinicians and administrative personnel to predict the clinical volume of diabetic patients to help allocate resources appropriately.
The Diabetic Foot Online Clinical Utilization Score (DFOCUS) was reviewed and updated with current epidemiological data. The online open calculator was developed based on the prevalence of diabetic patients and diabetic foot ulcer. The risk stratification score was also included to further calculate the number of diabetic patients based on the risk of developing a diabetic foot ulcer. Re-ulceration was also estimated in the calculator for patients in remission.
DFOCUS v. 1 was launched in 2014. Since that time, it has received some 27,500 page visits and related queries from more than 130 nations. In October of 2018 the online open calculator was successfully launched with updated epidemiological data data from the International Working Group on the Diabetic Foot and related sources.
The DFOCUS is an online open calculator to help clinicians and administrative personnel identify and allocate resources for high risk patients with diabetes. The launch of DFOCUS v.2 suggests that updates can be done instantly as new epidemiological data becomes available.
[P51] Sole Searching: Administrative Delay for Prescriptive Shoes as a Cause of Re-ulceration in Early Diabetic Foot Remission
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
The goal of this presentation is to illustrate how administrative delays in dispensing diabetic shoes may cause new or re-open diabetic foot ulcerations amongst patients in remission.
A series of patients who were in the diabetic foot remission clinic at Keck Hospital of University of Southern California but ulcerated while waiting for prescribed diabetic shoes were identified and presented. A detailed process analysis of diabetic shoe dispensary at a university teaching institution was conducted to identify the process defect and root cause.
Based on the process analysis and presented cases, multiple process modifications were implemented. The most immediate modification was changing the vendors that could provide high quality diabetic shoes efficiently. The team also established a new and close relationship with the Department of Family Medicine to expedite primary physicians sign-off as part of the diabetic shoe qualification. Patients who had no primary care physician and/or had lost follow up with primary care physician could have an immediate referral. Patient data that was necessary for diabetic shoe approval was also collected during the initial consult.
The presented case series demonstrated the impact of the process to dispense prescriptive diabetic shoes among high risk patients. The authors advocated to recognize defects in the healthcare system as potential risk factors for diabetic foot re-ulceration among patients in remission.
[P52] Toe, Flow and Go: A Novel Program for Diabetic Foot and Peripheral Arterial Disease Limb Preservation
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
The purpose of this manuscript is to describe and outline the components necessary in creating a successful interdisciplinary limb preservation program.
The four building blocks: Hot Foot Line, Wound Healing Clinic, Remission Clinic and Screening Clinic were described. These building blocks for a limb preservation program were designed based on population size and patient acuity. Specific quality measures for each clinic were also discussed in detailed to improve overall outcome of the program as well as the patients.
The outcomes of each building block were measured by different outcome measures. For the ‘hot foot line’, in-hospital and regional amputation rate for both major and minor amputations can be monitored as well as inpatient length of stay. The wound-healing clinic can be monitored for high:low amputation ratio, time to healing, number of curative procedures, and hospitalization rates. Remission clinic data included ulcer-free days, functional activity level, or frailty level. Screening clinics can be used to gather prospective data on long-term outcomes following initial risk assessment.
The “Toe, Flow & Go” model leverages specialists in Podiatric Surgery (Toe), Vascular Surgery (Flow) and Physical Therapy (Go) to create a successful limb preservation program. This interdisciplinary team combined with the program components outlined above helps our patients with diabetes and peripheral artery disease move through their world better.
[P53] Prevalence of vitamin and mineral deficiencies in diabetic patients with foot wounds
University of Adelaide, Adelaide, Australia
Nutrition and wound healing are closely linked. Nutritional deficiencies, including deficiencies of vitamins and micronutrients, may impede normal progression through the specific stages of wound healing. The purpose of this study was to analyse serum vitamin and mineral levels in diabetic patients with foot wounds
Plasma levels of Vitamin A, C, D, E, copper, zinc and ferritin were measured at initial assessment of diabetic patients with foot wounds seen at multidisciplinary foot clinics or admitted to our hospital in Australia. The association between the nutrients most commonly cited as important for wound healing, vitamin C, vitamin A and Zinc, and clinical factors including smoking status, duration of diabetes, HbA1c levels, BMI and burden of diabetic foot disease as assessed by WIfI score was analysed using using Kruskal-Wallis test (for Vitamin C) or Wilcoxon test (for Zinc and vitamin A).
131 patients were included in the study. Seventy-seven patients had a biochemical deficiency of at least one micronutrient. The most prevalent vitamin deficiency identified was vitamin D with 56% of patients presenting with levels below the normal range. Suboptimal levels of vitamin C affected 73% of patients, comprising marginal levels in 22.2% and deficient levels in 50.8%. Zinc deficiency, vitamin A deficiency and low ferritin levels were present in 26.9%, 10.9% and 5.9% of patients respectively. None of the patients had low levels of copper or vitamin E.
There was no correlation between BMI, duration of diabetes, HbA1c or smoking status and nutritional deficiency. Increased severity of diabetic foot disease was associated with lower vitamin C levels (p = 0.02).
Vitamins and micronutrients are required in small amounts, yet critical to cellular metabolism. These results show that in diabetic population with foot wounds, the prevalence of vitamin and micronutrient deficiency is high. Special concerns for the high prevalence of vitamin C and zinc deficiency, given their key roles in wound healing.
[P54] WoundVue Camera: A novel device to assess diabetic foot ulcers
University of Adelaide, Adelaide, Australia
The initial wound measurement and regular monitoring of diabetic foot ulcers is critical to assess treatment response. There is no standardised, universally accepted, assessment method to characterise diabetic foot ulcers. To address this need, a novel imaging system has been developed. Our project aims to assess treliabilty and practicality of the WoundVue camera technology (LBT INNOVATIONS, Adelaide, Australia)
The WoundVue camera is a prototype device. The system consists of two infrared cameras which image the wound from a vantage point and an infrared projector. The process of triangulation combines the range of all points in the image, thus obtaining a three-dimensional reconstruction of the wound. Fifty-seven diabetic foot wounds from patients seen in MDF clinic were photographed from two slightly different angles and distances using the WoundVue camera. Wound area, volume and maximum depth were measured for assessment of reliability. 31 of these wounds also had area calculated using the Visitrack™ (Smith&Nephew, London, United Kingdom) and correlation between area obtained using both systems was assessed.
WoundVue images test-retest analysis showed excellent agreement for area [ICC 0.995 (95% CI 0.991 – 0.997)], volume [ICC 0.988 (95%CI 0.979 – 0.993)] and maximum depth [ICC 0.984 (95% CI 0.975 – 0.990)] measurements. Good agreement was found for area measurement using the WoundVue camera and Visitrack™ system [ICC 0.874 (95% CI 0.754 – 0.937)]
The WoundVue system is capable of recreating a 3D model of diabetic foot wounds and produces accurate and reproducible data. Digital images are ideal for monitoring wounds over time and the WoundVue camera has the potential to be a valuable adjunct in diabetic foot wound care.
[P55] Evaluation and perspectives of podiatric interventions performed in multidisciplinary context on lower extremity amputations
Université du Québec À Trois-Rivières, Québec, Canada
Multidisciplinary team (MDT) has been shown to reduce diabetic foot ulcerations (DFUs) and amputations, but there is heterogeneity between team members and interventions. Podiatrists have been suggested as “gatekeepers” for the management of DFUs. The purpose of our study is to review the effect of podiatric interventions in MDTs on DFUs and amputations.
We conducted a systematic review of literature published up to 1st may 2018, through searches on databases and grey literature. Two investigators independently assessed the titles and abstracts and articles were included following inclusion criteria: respect of design, language, participants, interventions and outcomes. They independently extracted data from a pre-designed sheet and assessed potential risk of bias with JBI critical appraisal tools. Inconsistencies between reviewers were resolved reaching consensus with a third reviewer. 367 articles were reviewed for title and abstract and 16 articles met eligibility criteria but only 9 studies which fulfilled inclusion criteria had allow to meta-analysis.
All included studies for meta-analysis reported favorable data for people with diabetes in an MDT management that included podiatry. For total LEAs as primary outcome, the random effect model was applied and a significant result was found in favor of MDT with podiatry (RR: 0.69, 95% CI 0.54 – 0.89, I2 = 64%, P = 0.002). For major LEAs (level defined as above knee amputation and/or below knee amputation), results were also in favor of MDT with podiatry and still significant (RR: 0.45, 95% CI 0.23 – 0.90, I2 = 67%, P < 0.02). The result was not significant for minor LEAs (level defined as amputations at any level of the foot) (RR: 0.93, 95% CI 0.59 – 1.40, I2 = 55%, P = 0.76). Visual inspection of the funnel plot for the included cohort studies for total LEAs has demonstrated no strong evidence of publication bias of studies in favor of the interventions.
Our research is the first to specifically address the relevant role of podiatric interventions in an MDT approach for DFU management and highlights the necessity for stronger design and intervention descriptions in team approach for daily practices. Further studies should take this perspective.
[P56] Extracorporeal shockwave therapy (ESWT)-PACE technology: Micro-Vascular Stimulation Post-Amputation applied to Incision Lines Promotes Healing and Reduces Edema - Avoiding Extended Wound Care or the need for further Surgical Intervention
3360 Martin Farm Rd, The Mayer Institute, Suwanee, United States
Treating post-amputation surgical incisions with ESTW/PACE is effective and will optimize the healing potential by enhancing the revascularization of the micro-circulatory system, reducing edema, and speeding the annealing process at the incision line, avoiding the need for extended local wound care, repeated surgical intervention
20 Subjects selected from the existing practice population of a busy Wound Care Center of Excellence. that required either a 1st or 5th Ray Amputation, a 1st or 5th digit amputation or a 2nd, 3rd, and 4th MTH resection to qualify for inclusion. Those with critical limb ischemia were excluded.
The appropriate surgical procedure was performed. Post-amputation clinical evaluations, best practice wound management and treatment with ESWT/PACE was performed at 1 week and 3-weeks or until the it was determined that the incisions were healed. Target wounds were measured; data and pictures were recorded.
The treatment of ESWT/PACE was well tolerated, patients were universally compliant. We observed and all most uniform tissue response in the 3-weeks post-surgery. The incision lines came together substantially quicker than what we observed after our similar operations without ESWT/PACE. With this hastening of the kneeling process at the incision line, came a marked reduction in postoperative edema. These are patients that normally exhibited tremendous edema for a prolonged period of time. The combination of faster incision line closure and reduction in edema tended to return our patients back to a more normal life cracker and with a more durably healed diabetic foot.
Adequately controlling oedema and re-establishing perfusion can assist with healing. Our results demonstrated that ESWT-PACE technology is effective in increasing the healing rate by augmenting micor-revascularization and secondarily reducing edema by improving the venous return. The device was easy to apply by clinicians in the Wound Care Center of Excellence. During the ESWT/PACE treatment there was no treatment-related toxicity. 1 patient who underwent 5th ray amputation developed flap failure because of trauma from the buckle of the removable cast walker he was wearing postoperatively.
[P57] Pilot Study Assessing Novel Autologous Homologous Skin Construct Treatment of Venous Stasis Leg Ulcers
Usc Department of Vascular Surgery, Keck School of Medicine of University of Southern California, Los Angeles, United States
Venous stasis leg ulcers (VLUs) are a significant burden on the worldwide health care system and are often refractory to standard of care. A novel autologous homologous skin construct (AHSC) using the patient’s dermal regenerative cellular populations was developed to close difficult to treat wounds and assessed in a pilot study setting. 10 VLUs all being refractory to at least a month of conservative care were were treated with a single application of AHSC. A 1.5cm2 proximal calf harvest of full-thickness skin was collected in the clinic and sent to an FDA-registered facility where it was processed into AHSC and returned to the provider within 48-hours. AHSC was spread evenly across the wound, dressed with silicone, secured with steri-strips, and bolstered with an absorbent foam covered by a triple-layer compression wrap. Healing was documented with digital photography and planimetry during weekly dressing changes. Wound closure was verified 2 weeks following initial closure documentation. 10/10 wounds (100%) had complete graft take one week after ASHC application. All VLU wounds demonstrated granulation and progressive epithelialization shorty after AHSC deployment. 9 of 10 wounds (90%) closed within 12 weeks of a single application of AHSC. A 12.2 cm2 wound that had been open for 11 months and failed a prior split-thickness skin graft closed in 13.4 weeks after AHSC therapy. All wounds remained closed at 2-week durability follow-up. All full-thickness skin donor harvest sites remained closed with minimal morbidity.AHSC successfully closed VLUs refractory to dressing care with a single application in this pilot study warranting further evaluation with randomized controlled trials.
WIRB approved