
Abstract

Although Electronic Health Records hold great promise for improving clinical care and workflow, in most cases, it functions as a data repository rather than as dynamic patient care tool and take away too much “doctors time.1-4” Electronic Health Records have shown to improve quality metrics in Diabetes clinics. 1 We determined the impact of implementing a new physician workflow tool called “Reya Digital Assistant” (Cura Technologies Inc., Menlo Park, CA, United States). It is a new generation of clinical software which creates highly intuitive digital clinical assistant applications on various specialties. It provides details about the patients in the right context helping physicians make better clinical judgement. The software also has an advantage of tracking record of history of patient medications, clinical and laboratory data, co-morbidities, and complications which support the treating physician to overcome or delay the new onset of disease-related complications (Figure 1).
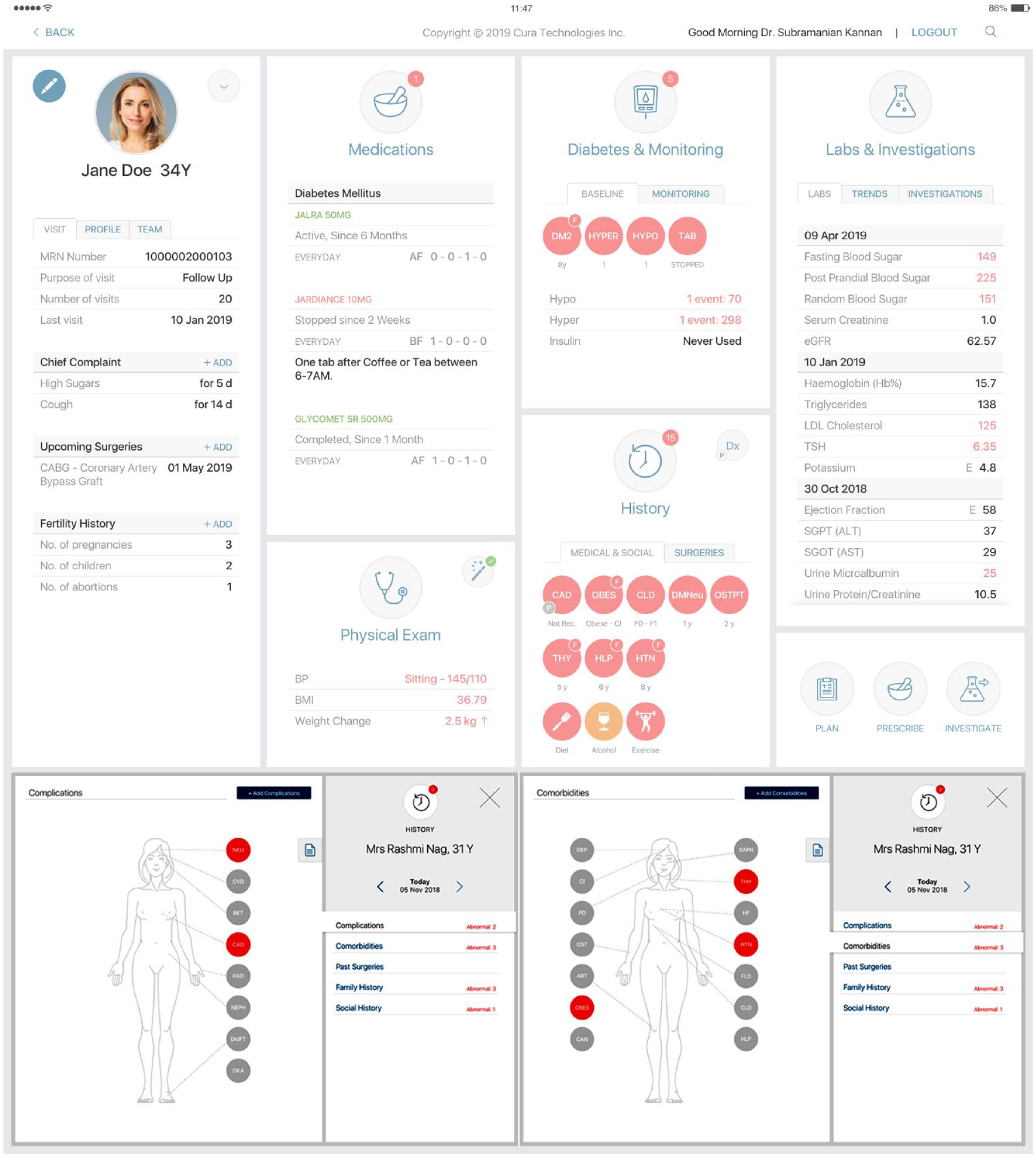
Dashboard view of the Diabetes Clinical & Laboratory data, complications, and co-morbidities documented in the Cura Digital Clinical Assistant at each patient visit.
We reviewed patients (>18 years) data of the clinic obtained from the digital clinical assistant between January 2017 and December 2018. The initial visit for the patient was considered when their data first entered into the system, and latest follow-up was considered as last visit of the particular patient. A total of 42 095 patients (24 491 males; 58.2%) records were reviewed and the mean age was 50.65 ± 15.4 years. The mean duration of diabetes was 8.3 ± 6.5 years, 89.2% being diagnosed with type 2 diabetes and 5.9% patients had newly diagnosed diabetes, and the mean duration of follow-up was 5.35 ± 4.48 months. A 49% increase in new clinic visits was measured with the same clinical workflow, clinical protocols, and clinic staffing levels, and there was threefold increase in repeat visits when comparing footfalls in 2017 and 2018. There was a significant reduction in fasting blood glucose values (147.99 ± 58.64 vs 137.67 ± 44.53 mmHg; P < .05) and HbA1c values (8.04 ± 1.87 vs 7.72 ± 1.5; P < .05) in the latest visits compared to initial visit of patients who have completed atleast six months follow-up. The number of patients with HbA1c <8% was 54% at initial clinical visit which increased to 63% (P < .01) at their latest clinic visit, while the number of patients with LDL-c < 100 mg/dL improved from 38.2% to 61.8% in 2018 (P < .01) and patients with BP < 140/90 mmHg increased from 28.4% to 30.3% (P = .876). Improved documentation of weight and BP at every clinic visit (>80%) was also noted with adoption of the digital clinical assistant. This is an exploratory model involving preliminary data and more definitive patient level cohort data with adjustment for confounders are needed. Patient or physician satisfaction rates were not qualitatively captured. But the fact remains that despite adoption of a new technology with the same clinical staffing and resources, we were able to improve the clinic throughput with almost doubling of new patient visits and a threefold increase in repeat visits coupled with a significant increase in the number of patients who achieve quality metrics (HbA1c < 8% and LDL-c < 100) and nonsignificant increase in patient who achieved BP < 140/90.
Footnotes
Acknowledgements
We thank the Cura team for helping us develop the software in collaboration with the medical team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article